

Abstract
Aims
Femoroacetabular impingement (FAI) is a potential cause of hip osteoarthritis (OA). The purpose of this study was to investigate the expression profile of matrix metalloproteinases (MMPs) in the labral tissue with FAI pathology.
Methods
In this study, labral tissues were collected from four FAI patients arthroscopically and from three normal hips of deceased donors. Proteins extracted from the FAI and normal labrums were separately applied for MMP array to screen the expression of seven MMPs and three tissue inhibitors of metalloproteinases (TIMPs). The expression of individual MMPs and TIMPs was quantified by densitometry and compared between the FAI and normal labral groups. The expression of selected MMPs and TIMPs was validated and localized in the labrum with immunohistochemistry.
Results
On MMP arrays, most of the targeted MMPs and TIMPs were detected in the FAI and normal labral proteins. After data normalization, in comparison with the normal labral proteins, expression of MMP-1 and MMP-2 in the FAI group was increased and expression of TIMP-1 reduced. The histology of the FAI labrum showed disorderly cell distribution and altered composition of thick and thin collagen fibres. The labral cells expressing MMP-1 and MMP-2 were localized and their percentages were increased in the FAI labrum. Immunohistochemistry confirmed that the percentage of TIMP-1 positive cells was reduced in the FAI labrum.
Conclusion
This study established an expression profile of MMPs and TIMPs in the FAI labrum. The increased expression of MMP-1 and MMP-2 and reduced expression of TIMP-1 in the FAI labrum are indicative of a pathogenic role of FAI in hip OA development.
Cite this article: Bone Joint Res. 2020;9(4):173–181.
Keywords: Hip, Labrum, Matrix metalloproteinase, Femoroacetabular impingement, Osteoarthritis
Article focus
Molecular pathology of femoroacetabular impingement (FAI).
Labral matrix metalloproteinase (MMP) profile in FAI.
Pathogenic role of FAI for hip osteoarthritis (OA).
Key messages
Increased MMP-1 and MMP-2 in the FAI labrum.
Patterns of MMP-positive cells in the FAI labrum.
FAI labrum as a possible source of hip degeneration.
Strengths and limitations
Direct comparison between FAI and normal labrum; detailed biochemical (protein array) and histological (zonal) analyses of the FAI labrum.
Limited sample size.
Introduction
Femoroacetabular impingement (FAI) is defined as abnormal contact between the proximal femur and the acetabulum.1 The role of FAI in the pathogenesis of hip osteoarthritis (OA) is currently of great interest to orthopaedics and sports medicine. There are two subtypes of FAI: 1) pincer impingement, which features an over-covered acetabulum; and 2) cam impingement, where an aspherical femoral head (cam abnormality) presents.2 While a strong correlation between cam impingement and the onset of hip OA has been established, the linkage between pincer impingement and hip OA is still controversial.3 Among ongoing debates are the influence of FAI on the progression of hip OA and the necessity of surgical treatment of FAI.4
It is generally agreed upon that, in FAI, the anatomical anomaly at the proximal femur and acetabulum makes non-physiological contact, and exerts abnormal forces between the acetabular labrum and articular cartilage on the femoral head during hip motion.5 The repetitive collisions that occur during hip motion may lead to labral injury and chondral delamination, and trigger a degenerative cascade involving the hip joint.6 The fibrocartilaginous acetabular labrum is, therefore, the focal point of FAI pathology and the proposed initiator of hip OA. A common surgical pathology of FAI is a labral tear, which was first described by Altenberg7 more than 50 years ago. It is estimated that 87% to 90% of labral tears are associated with bony anomalies of the hip.8,9 The types of labral tears include labral detachment and intrasubstance tears. Pathologically, the torn labrum is degenerative, which includes disorganized matrix, cysts, hyper/hypocellularity, high vascularity, and ossification.10,11 Detailed cellular and molecular pathology of the FAI labrum is critical for evaluating its impact on the hip joint and developing new therapies, but has not been thoroughly investigated.
Matrix metalloproteinases (MMPs) are a family of secreted or membrane-associated calcium-dependent zinc-containing enzymes capable of digesting virtually all extracellular matrix proteins.12 While the enzymatic functions of MMPs are essential for developmental biology and maintaining tissue homeostasis, increased expression of certain MMPs is common in ageing, inflammation, and degeneration.13–15 To a specific degenerative condition, individual MMPs may play unique roles.16 The proteolytic activity of MMPs is counter-regulated by a group of tissue inhibitors of metalloproteinases (TIMPs), which have various biological functions but most impressively inhibit the function of a broad spectrum of MMPs.17 It is the balance between MMPs and TIMPs that maintains the homeostasis of the extracellular matrix under physiological conditions.18 The degenerative pathology in the FAI labrum, particularly the disorganized extracellular matrix, may be the result of unbalanced enzymatic activities between MMPs and TIMPs. A detailed expression pattern of MMPs and TIMPs is an essential molecular pathology of degeneration but has not been revealed in the FAI labrum.
The purpose of this study was to investigate the expression profile of MMPs and TIMPs in labral tissue with FAI pathology, in comparison with normal labral tissue, using a protein array. The hypothesis was that there are distinct expression patterns of specific MMPs and TIMPs in FAI labral tissue. In this study, the identified MMPs and TIMPs were further validated and localized in the torn labral tissue with immunohistochemistry, and analyzed in conjunction with collagen and elastic fibre organizations histologically.
Methods
Collection of labral tissues
Labral tissue samples were collected from four patients with symptomatic labral tears who underwent hip arthroscopy. The patients comprised three males and one female, and the mean age was 24.5 years (21 to 32). Under arthroscopy, labral tears were observed at the anterosuperior section of the acetabular rim. For this study, the torn labral tissues were biopsied arthroscopically at locations 2 to 3 o’clock, 1 to 2 o’clock, and 11 to 12 o’clock, according to the acetabular clock face positions described by Philippon et al.19 After the acetabular rim was trimmed with a 5.5 mm burr, the labral tear was repaired with suture anchors. The labral samples were stored in sterile containers at -80°C and shipped in dry ice overnight for laboratory analysis.
On the day of protein extraction, the surgical labral samples were thawed. A small portion of each FAI labral sample was fixed with 4% paraformaldehyde for histology. The rest of the labral samples were weighed and used for protein extraction.
For normal controls, three cadaveric hips were obtained from National Disease Research Interchange (Philadelphia, Pennsylvania, USA). The donors comprised one female and two males, and the mean age was 49 years (33 to 58). Donor exclusion criteria included histories of hip disease and injury, as well as cancer. The cadaveric hips were transported to the laboratory on ice within 18 hours after the donor was deceased, and stored at -80°C. On the day of protein extraction, the cadaveric hips were dissected and carefully inspected for signs of injury and arthritis. All three obtained hip joints were negative of intracapsular haematoma, excessive joint fluid, inflamed synovium, and cartilage wear. Labral tissue, in full thickness, was resected from the anterosuperior section (corresponding to 12 to 3 o’clock in the acetabular clock face position used for arthroscopic labral biopsy)19 of the acetabular rim. For each labral sample, a small portion was fixed in 4% paraformaldehyde and processed for histology. The rest of the dissected labrum was used for protein extraction.
Expression profile of MMPs and TIMPs
The labral tissue was homogenized in mammalian protein extraction reagent (mPER; Thermo Fisher Scientific, Waltham, Massachusetts, USA) using a tissue homogenizer. The resulting tissue lysate was centrifuged at 12,000 rpm for 20 minutes at 4°C and the supernatant was collected. The protein concentration was determined using a bicinchoninic acid (BCA) protein assay kit (Thermo Fisher Scientific).
The proteins extracted from the FAI and normal labral samples were pooled within the same group and applied separately on membrane-based Human MMP Antibody Array (Abcam, Cambridge, Massachusetts, USA). The Array has built-in antibodies targeting a total of ten MMPs and TIMPs: MMP-1, MMP-2, MMP-3, MMP-8, MMP-9, MMP-10, MMP-13, TIMP-1, TIMP-2, and TIMP-4. The capturing antibodies of MMPs and TIMPs are arranged in arrays on a membrane. The design of the antibody Array includes positive and negative controls for data normalization. The Array membrane with the FAI or normal labral proteins was incubated at 4°C overnight. Following incubations with biotinylated-detecting antibody and horseradish peroxidase-conjugated streptavidin, chemiluminescent detection reagent was added onto the membrane. The array membranes were imaged with a digital camera for chemiluminescent signals.
On the arrays of FAI and normal labral proteins, the expression of MMPs and TIMPs was quantified by densitometry (ImageJ; National Institutes of Health, Bethesda, Maryland, USA). On each array, the intensity of individual MMPs and TIMPs was normalized with the internal positive (set at 100%) and negative (set at 0%) controls. After normalization, the intensities of the same MMPs and TIMPs were compared between the FAI and normal labral groups. When the normalized intensity of a MMP or TIMP in the FAI labral proteins was 20% above the background (i.e. the negative controls on the Array) and at least onefold greater or less than the normal labral proteins, it was deemed as pathologically relevant. A group of selected MMPs and TIMPs were further validated for expression and localized in the labral tissue with immunohistochemistry.
Histology and immunohistochemistry
The FAI and normal labral samples for histology were embedded in optimal cutting temperature (OCT) medium (Sakura Finetek USA Inc, Torrance, California, USA) and frozen at -80°C, before being sectioned with a cryostat. Tissue sections were stained with haematoxylin and eosin (H&E), and Picrosirius Red for tissue structure and collagen fibre composition, respectively.
For immunohistochemistry of MMP-1, MMP-2, and TIMP-1, tissue sections of labral samples were blocked with 10% normal goat serum and hydrogen peroxide. Rabbit antihuman MMP-1, MMP-2, and TIMP-1 polyclonal antibodies (Abcam) were used at 1:200 dilution in 100 mM tris buffered saline with 0.025% Triton-X (Sigma-Aldrich, St. Louis, Missouri, USA). The primary antibodies were separately applied and incubated at 4ºC overnight in a moisture chamber. A biotinylated goat antirabbit secondary antibody and avidin-biotin complex reagents (Vector Laboratories, Burlingame, California, USA) were applied onto the slides sequentially. Peroxidase substrate 3,3'-diaminobenzidine solution was used to detect immunoreaction chromogenically. Nuclei were counterstained with haematoxylin. Tissue sections were viewed under a microscope and images were taken at standardized locations on each tissue section: at the diagonal centre of labral sections, as the central region of the labrum; and at the labral surface directly above the central region, as the labral surface region. The MMP-1, MMP-2, and TIMP-1 positive cells, as well as the total number of cells, on the images were counted and the percentages of positively stained cells were calculated.
Statistical analysis
The data are expressed as medians (interquartile ranges, IQRs). The percentages of MMP-1, MMP-2, and TIMP-1 positive cells in the superficial and central regions of the FAI and normal labral samples were compared with the Mann-Whitney U test (KaleidaGraph V4.5; Synergy Software, Reading, Pennsylvania, USA). The significance level was set at p < 0.05.
Results
Histology
The histology of the labrum was divided into superficial and central regions. The superficial region in the normal labrum included a layer of cells on the surface of the labrum and a narrow adjacent zone, where collagen fibre bundles and cells were oriented in parallel with the labral surface. While the outmost layer of the normal labrum consisted of mostly red (thick) collagen fibres, the adjacent area was made up of both red (thick) and green (thin) collagen fibres as demonstrated by polarizing microscopy (Figures 1a and 1c). Of the FAI labrum, the superficial region was expanded from the thickness of the corresponding region in normal labrum. In certain areas, cell distribution lost the layered pattern shown in the normal labrum. In general, however, cellularity seemed to be slightly increased. The collagen fibre alignment in the superficial region of the FAI labrum was still distinctive from the central region but, compared to the normal labrum, had uneven distribution of green (thin) collagen fibres and lost the outmost layer (Figures 1b and 1d).
Fig. 1.

Histology of the superficial region of the normal and femoroacetabular impingement (FAI) labrums. a) In the normal labrum, the superficial region includes a single layer of cells on the surface and an adjacent area (marked by arrows), where cells line in parallel with the surface. b) In the FAI labrum cells are lost from the surface layer, and the cells in the superficial region are distributed in a more random fashion. The entire superficial region in the FAI labrum is expanded (marked by arrows). There are mostly thick collagen fibres in the surface layer of the normal labrum. The collagen fibres in the adjacent area are composed of both thick and thin fibres. c) Collagen fibres in the superficial region of the normal labrum are oriented in parallel with the labrum surface. d) Collagen fibres in the superficial region of the FAI labrum are disoriented and more heterogenous in the makeup of collagen fibres. Haematoxylin and eosin (H&E) staining was used in a) and b); Picrosirius Red staining was used in c) and d). Bars represent 50 µm (original magnification 200×).
In the central region of the normal labrum, cellularity was low. There were a number of cyst-like voids, which varied in size and appeared to be interconnected (Figures 2a and 2c). Collagen fibre bundles consisted of mostly orange/red (thick) fibres. In the central region of the FAI labrum, the extracellular matrix was hypochromatic and cyst-like voids were deformed (Figures 2b and 2d). Cell density was low in general in the FAI central region, where cell distribution was not as even as in the normal control. Collagen bundles in the FAI central region were overtly green (thin) fibres and disorganized.
Fig. 2.

Histology of the central region of the normal and femoroacetabular impingement (FAI) labrums. a) In the normal labrum, cells are scattered in the central region. The extracellular matrix is featured with voids (indicated with arrows). b) In the FAI labrum, the central region is occupied with disrupted and disorganized matrix, with very few cells. c) The normal labrum is made up of mostly thick (orange/red) collagen fibres, whereas d) the FAI labrum has an increased content of thin (green) collagen fibres, which are also disorganized. Haematoxylin and eosin (H&E) staining was used in a) and b); Picrosirius Red staining was used in c) and d). Bars represent 50 µm (original magnification 200×).
MMP and TIMP expression by antibody array
On the MMP array, positive and negative controls were correctly identified in both FAI and normal groups. The targeted MMPs and TIMPs were detected in both FAI and normal labral proteins, except for MMP-10 in the normal labrum. For both FAI and normal labral tissues, the predominantly expressed ones were TIMP-1 and TIMP-2. The spots of individual MMPs varied in intensity and size on both FAI and normal labral arrays (Figures 3a and 3b). Densitometry showed that, after normalization, the expressions of MMP-1 and MMP-2 in the FAI labral samples were increased approximately onefold compared to the normal labral samples (Figure 3c). Another multifold increase in the FAI labral tissues was MMP-10. However, its overall expression level was low in the FAI labral proteins (< 20% after normalization) and barely detected in the normal labral proteins. MMP-13 was also increased in the FAI group but its difference with the normal group was less than onefold. Interestingly, MMP-8 was reduced in the FAI labral samples, compared with the normal controls. The normalized expression of TIMP-1 in the FAI labral samples was about 58% of that in the normal labral samples (median 0.45 (IQR 0.03) vs median 0.77 (IQR 0.03)).
Fig. 3.
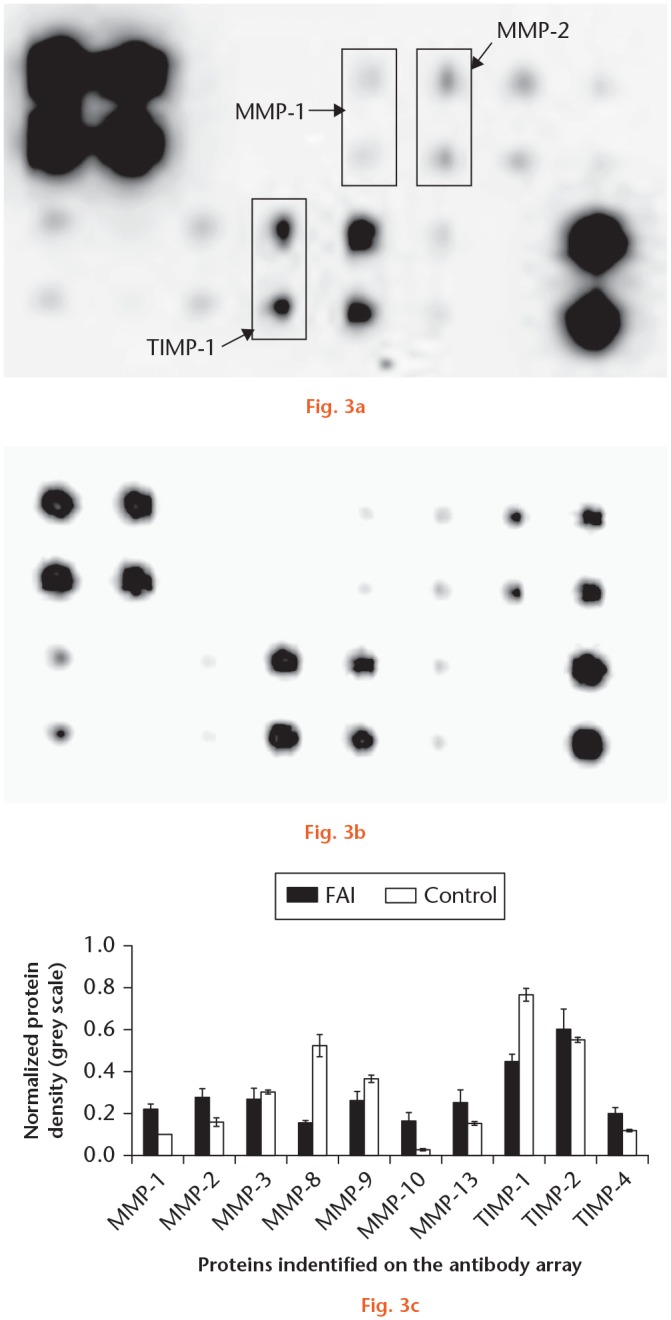
The expression of matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMPs) in normal and femoroacetabular impingement (FAI) labral proteins. The membranes of antibody array show varied dots of MMPs and TIMPs that expressed in a) FAI labral samples and b) control labral samples. c) The normalized data of densitometry show quantitatively the differences of MMP and TIMP expression in the normal and FAI labrums. There are notable increases of MMP-1 and MMP-2, and reduction of TIMP-1 in the FAI labral proteins.
Immunohistochemistry of MMP-1, MMP-2, and TIMP-1
In the superficial region of the normal labrum MMP-1 was nearly negative, except for light staining due to an ‘edge effect’ (Figure 4). There were a few MMP-2-positive cells in the normal labrum, but they were only slightly stained. MMP-1 and MMP-2 were detected in the superficial region in the FAI labrum, especially around degenerative lesions. Both MMP-1 and MMP-2 were stained intracellularly and MMP-2 was also detected extracellularly. With an increased cell density in the superficial region of the FAI labrum, the percentages of the cells that were positively stained for MMP-1 and MMP-2 were three- to four-fold greater than those in the same region in the normal labrum (p < 0.05). In contrast, TIMP-1 was intensely stained in the superficial region of the normal labrum, but its staining in the same region in the FAI tissues was light. The percentage of TIMP-1 positive cells in the superficial FAI labrum was about one-fifth of that in the normal labrum (p < 0.05).
Fig. 4.
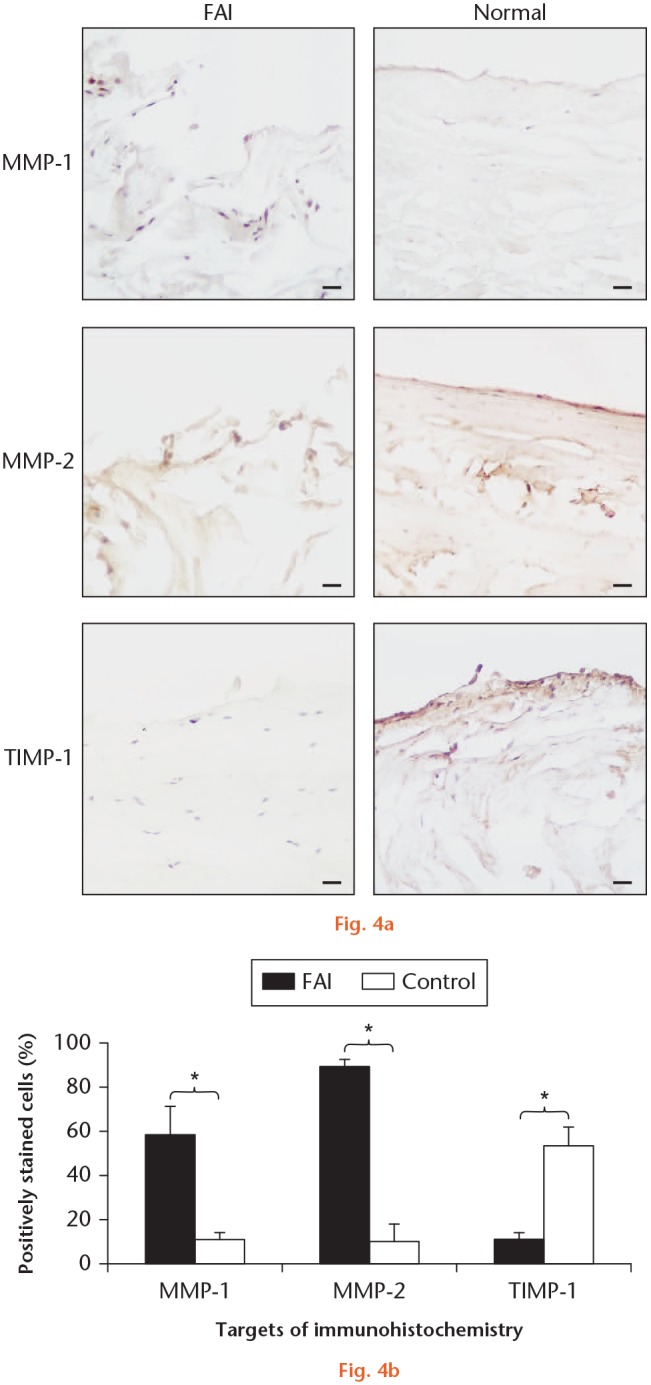
a) Immunohistochemistry of matrix metalloproteinase (MMP)-1, MMP-2, and tissue inhibitor of metalloproteinases (TIMP)-1 in the superficial region of the normal and femoroacetabular impingement (FAI) labrums. MMP-1 positive cells are detected mostly in the superficial layer of the FAI labrum but not in the normal labrum. MMP-2 is detected both intracellularly and extracellularly in the superficial region in the FAI labrum. TIMP-1 is extensively stained in the normal labrum but not in the FAI labrum. b) The percentages of MMP-1 and MMP-2 positive cells in the superficial region of the FAI labrum are significantly increased, compared with the normal labrum. The percentage of TIMP-1 positive cells in the superficial region of the FAI labrum, however, is reduced. Bars represent 50 µm (original magnification 200×). Nuclei are counter-stained with haematoxylin. *p < 0.05.
In the central area of the labrum, MMP-1 positive cells were scattered in the FAI samples, but they were even fewer in the normal controls (Figure 5). Compared with the normal labrum, MMP-2 positive cells were increased in the central area of the FAI labrum. MMP-2 staining in the FAI samples was predominantly extracellular. TIMP-1 was detected in the central region of the normal labrum both intracellularly and extracellularly, but it was nearly negative in the central area of the FAI labrum. In the central region, the percentages of the MMP-1 and MMP-2 positive cells in the FAI samples were more than ten-fold of those in the normal labrum (p < 0.05). The percentage of TIMP-1 positive cells in the central area of the FAI samples, however, was less than one-tenth of that in the same region in the normal labrum (p < 0.05).
Fig. 5.
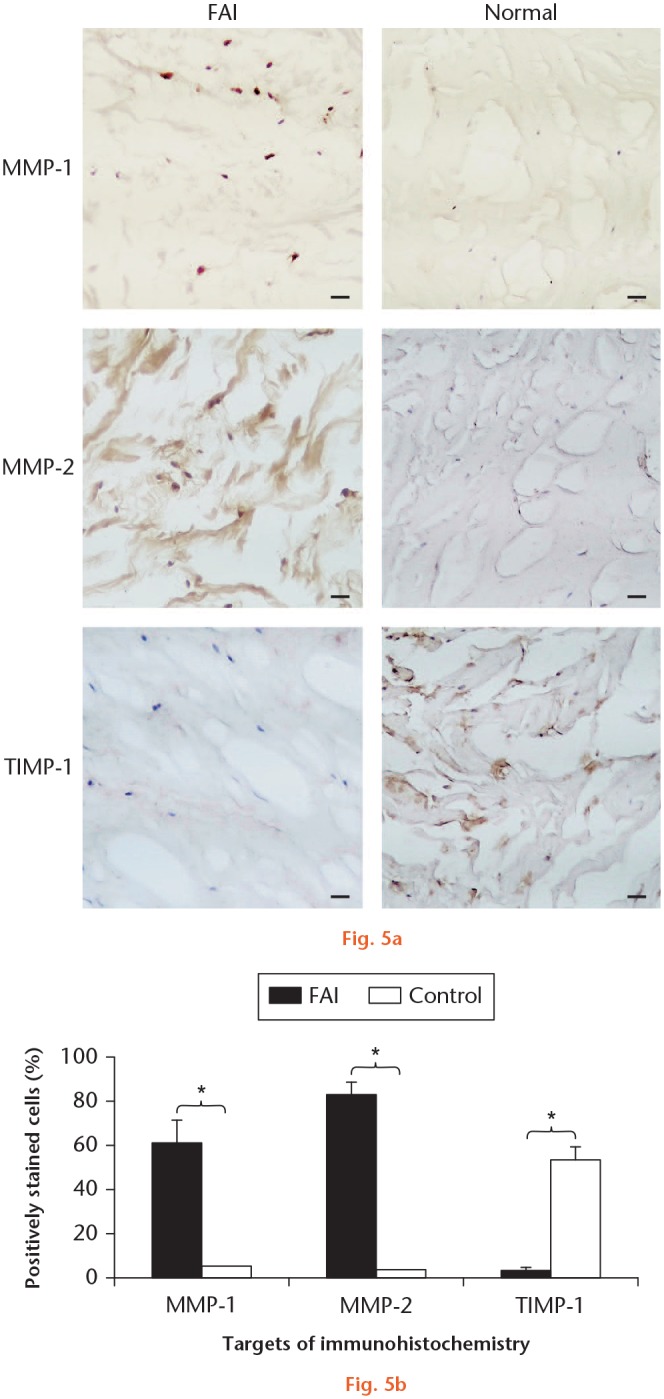
a) Immunohistochemistry of matrix metalloproteinase (MMP)-1, MMP-2, and tissue inhibitor of metalloproteinases (TIMP)-1 in the central region of the normal and femoroacetabular impingement (FAI) labrums. Both MMP-1 and MMP-2 are detected in the central region of the FAI labrum but not in the normal controls. While MMP-1 is mostly stained intracellularly in the FAI labrum, MMP-2 is detected both intracellularly and extracellularly. TIMP-1 is detected in the normal labrum but not in the FAI labrum. b) The percentages of MMP-1 and MMP-2 positive cells in the central region of the FAI labrum are significantly greater than those in the normal labrum. The percentage of TIMP-1 positive cells in the central region of the FAI labrum is significantly reduced compared with the normal labrum. Bars represent 50 µm (original magnification 200×). Nuclei are counter-stained with haematoxylin. *p < 0.05.
Discussion
Progression from FAI to labral tear and hip OA has been recognized clinically,20 but the underlying cellular and molecular mechanisms in the labrum are still to be understood. Structurally, from the edge to the centre the labrum varies in the patterns of collagen fibre organization and cell distribution.21 In this study, the labrum was divided into superficial and central regions for analysis, according to patterns of cell distribution and arrangements of fibre bundles in the normal labrum. The superficial region included a single layer of cells on the outmost surface and an adjacent area where cells and collagen fibres were organized in parallel to the surface.
In the FAI labrum, a noticeable pathology was the loss of cells from the outmost layer of the superficial region. Apoptosis in labral tissue was common in dysplastic OA hips (12/20), where the entire joint is degenerative.22 It was less common in the labrum of the hips with avascular necrosis of the femoral head, when the pathology was confined to the femoral head. In this study, the FAI labral samples were collected from non-OA hips. The cell loss from the outmost layer of the FAI labrum was likely a consequence of labral tear rather than a degenerative hip. Since the labrum is exposed to the hip joint, the cells in the outmost layer could be vulnerable to a pathological joint condition that was secondary to labral tear. In contrast to cell loss in the outmost layer, the cellularity in the adjacent area was slightly increased. This may suggest that the FAI labrum was responsive to the tear.
Cells in the labrum produce mostly type I collagen.23 The area beneath the outmost layer consisted of both thick (such as type I collagen) and thin (such as type III collagen) fibres, as the polarizing microscopy demonstrated.24 In the FAI labrum, collagen fibres in the superficial region were not only disorganized but also altered in the makeup of collagen types, which may be signs of altered cell phenotypes. Overall, the superficial region of the FAI labrum was still distinctive structurally, with densely packed collagen fibres, and slightly expanded in thickness.
Inside the labrum, the central region had a few cells and contained mostly thick collagen fibres. The pathology of the FAI labrum includes cystic and disordered matrix.10 In this study, the extracellular matrix of the FAI labrum was a mixture of thick and thin collagen fibres. The increasing heterogeneity of collagen types in the matrix of the FAI labrum was likely the result of simultaneous tissue degeneration and repair, and could be the molecular foundation of a compromised labral mechanics in FAI, such as dynamic shear.25–27 In this study, cyst-like matrix voids were prevalent in the FAI and normal labrums. Similar labral ‘pseudocysts’ presented in most of the osteoarthritic hips (69/77) and in the FAI labrum.10,22 Therefore, cystic lesions in the labrum are likely degenerative but not specific to FAI. To determine the biological significance of those cyst-like voids in the labral matrix may require a developmental study because the formation of those voids seems to be related to ageing, which associates with labral degeneration.28 It is possible that the donors’ ages, which were higher than those in the FAI group, were an influential factor for the appearance of cyst-like voids in the normal labrum. The cadaveric hips were normal by gross inspection but early degeneration in the hips could not be ruled out completely. Although cellularity was increased in some areas of the FAI labrum, no leucocyte infiltration presented. These cells in the FAI labrum had been identified as endothelial cells, macrophages, and mast cells, responding to tissue injury.29 It is noteworthy that some previous studies included FAI labrum at the stage of hip OA, or compared the FAI labrum with OA hip labrum.10,29,30
Dissection of ageing hips (aged between 61 and 98 years) revealed a high rate of degenerative labral tear (53/55 hips).11,28 A hallmark of tissue degeneration is an increased expression of MMPs.15 The MMP family includes collagenases, gelatinases, stromelysins, elastases, and aggrecanases. MMPs degrade a variety of extracellular macromolecules such as collagen, aggrecan, decorin, biglycan, fibromodulin, and versican.12 MMP antibody arrays, which screen the expression of multiple MMPs simultaneously, offered a global view of MMP expression in the FAI labral tissue. After data normalization, the MMP and TIMP expression profile of the FAI labrum was notably different from the normal labrum.
MMP-1 is the most ubiquitously expressed interstitial collagenase that specifically degrades type I collagen and other fibrillar collagens.31 The increased MMP-1 in the FAI labrum was more consequential as labrum consists of mostly thick (type I) collagen fibres. An increase of MMP-1 is a common phenomenon found in degenerative conditions such as intervertebral disc degeneration, degenerative meniscus tear, and OA.32–34 Immunohistochemistry demonstrated that a large portion of the cells in both superficial and central regions of FAI labrum expressed MMP-1, indicating the extensiveness of collagen degradation in FAI labrum. Interleukin-1 (IL-1), known to induce chondrocyte catabolism in OA,35 upregulates the expression of MMP-1 by labral cells.23 In both OA and FAI hips, IL-1 was expressed in the labrum, synovium, and cartilage.30 It is likely that MMP-1 expression in the labrum is regulated by intertwined signalling pathways.
While MMP-1 and other MMPs cleave collagen triple helix, MMP-2 further digests collagen monomers.36 The increase of MMP-2 in the FAI labrum could be in concert with MMP-1 activity to complete collagen degradation. Immunohistochemical localization showed that MMP-2 was distributed diffusely in the FAI labrum. MMP-2 is also increased in ageing tenocytes, which are associated with degenerative tendinopathy, and the chondrocytes in osteoarthritic cartilage.37,38 Together, the increased expression of MMP-1 and MMP-2 could effectively break down the extracellular matrix in the torn labrum.
A sum of MMP and TIMP enzymatic activities determines either proteogenesis or proteolysis in the extracellular matrix.18 On their protein arrays, both the FAI and normal labrums expressed a large amount of TIMP-1 and TIMP-2, which inhibit the proteolytic activities of MMPs and stabilize the tissue environment. A comparison between the normal and FAI labrums revealed a reduction by more than one-third of TIMP-1 in the FAI labrum. This could further promote proteolysis in the FAI labrum and is in line with other degenerative pathology, such as intervertebral disc degeneration in which TIMP-1 is downregulated.32 Furthermore, recent studies suggest that TIMP-1 may influence matrix accumulation indirectly, through regulation of macrophage function in tissue injury and inflammation.18,39
Both the increase of MMPs and decrease of TIMP-1 in the FAI labrum revealed by this study are equally important molecular insights into the FAI and labral tear pathology. Their pathological impacts, however, may extend beyond the labrum. As a source of proteolytic enzymes in the hip joint, the FAI labrum could be responsible for degradation of hip cartilage. Compared with labrum and synovium, the articular cartilage in the same FAI hips expressed more inflammatory cytokines such as IL-1, IL-8, MMP-13, and a disintegrin and metalloproteinase with thrombospondin motifs-4 (ADAMTS-4).30 Those cytokines and MMPs are known to trigger the onset of OA.40 While a torn labrum destabilizes the hip mechanically, depending on the size, shape, and location of the tear,41,42 releasing MMP-1 and MMP-2 into the joint could exert profound influences on the functions of the chondrocytes in hip articular cartilage. It is the malfunction of chondrocytes and cartilage degeneration that ultimately mark the development of OA in the hip.
In addition to the increased expression of MMP-1 and MMP-2 and reduced expression of TIMP-1, the MMP arrays hinted at other clues of FAI pathology. For example, MMP-8 in the FAI proteins was about one-third of that in the normal labral samples. MMP-8 is prominent in the development of periodontitis,43 but has not been widely quoted in musculoskeletal degeneration. MMP-8 was not selected for further validation because it is unlikely that a reduction of MMP-8 could reverse the predominantly proteolytic degeneration in the FAI labrum. One note about the limitation of this study is that the MMP-1, MMP-2, and TIMP-1-positive cells were counted in a semiquantitative manner, although rules for image locations and imaging parameters were followed consistently. For the FAI pathology, however, the trends, patterns, and localization of those positive cells are more important than their actual counts. The sample size of this study was limited by the accessibility to clinical and cadaveric resources, i.e. the quantity of labral biopsy and number of suitable donors. The goal of this study was an initial screening of MMP expression in the FAI labrum. The labral samples collected in this study were sufficient for carrying out MMP array and immunohistochemistry. Nevertheless, the molecular pathology of FAI revealed in this preliminary study is evidence of a strong linkage between FAI and hip OA. Clinically, this study suggests that the healing and repair of labral tears are integral to the strategy of FAI management and hip OA prevention.44,45
Acknowledgments
None declared
Footnotes
Author contributions: J. Schon: Designed the study, Performed the experiment, Collected and analyzed the data, Wrote the manuscript.
J. Chahla: Performed the experiment, Wrote the manuscript.
S. Paudel: Performed the experiment, Collected and analyzed the data.
L. Manandhar: Performed the experiment, Collected the data.
T. Feltham: Performed the experiment, Collected the data.
J. Huard: Wrote the manuscript.
M. Philippon: Designed the study, Collected and analyzed the data.
Z. Zhang: Designed the study, Analyzed the data, Wrote the manuscript.
Conflict of interest statement: None declared
Ethical review statement: The uses of labral tissues and cadaveric tissues for this study were approval by the Vail Valley Medical Center Institutional Review Board (#2015-10).
Follow us @BoneJointRes
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- 1. Agricola R, Waarsing JH, Arden NK, et al. Cam impingement of the hip: a risk factor for hip osteoarthritis. Nat Rev Rheumatol. 2013;9(10):630-634. [DOI] [PubMed] [Google Scholar]
- 2. Philippon MJ, Maxwell RB, Johnston TL, Schenker M, Briggs KK. Clinical presentation of femoroacetabular impingement. Knee Surg Sports Traumatol Arthrosc. 2007;15(8):1041-1047. [DOI] [PubMed] [Google Scholar]
- 3. Kowalczuk M, Yeung M, Simunovic N, Ayeni OR. Does Femoroacetabular impingement contribute to the development of hip osteoarthritis? A systematic review. Sports Med Arthrosc Rev. 2015;23(4):174-179. [DOI] [PubMed] [Google Scholar]
- 4. Wyles CC, Heidenreich MJ, Jeng J, Larson DR, Trousdale RT, Sierra RJ. The John Charnley Award: redefining the natural history of osteoarthritis in patients with hip dysplasia and impingement. Clin Orthop Relat Res. 2017;475(2):336-350. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Amanatullah DF, Antkowiak T, Pillay K, et al. Femoroacetabular impingement: current concepts in diagnosis and treatment. Orthopedics. 2015;38(3):185-199. [DOI] [PubMed] [Google Scholar]
- 6. Bedi A, Kelly BT. Femoroacetabular impingement. J Bone Joint Surg Am. 2013;95-A(1):82-92. [DOI] [PubMed] [Google Scholar]
- 7. Altenberg AR. Acetabular labrum tears: a cause of hip pain and degenerative arthritis. South Med J. 1977;70(2):174-175. [PubMed] [Google Scholar]
- 8. Wenger DE, Kendell KR, Miner MR, Trousdale RT. Acetabular labral tears rarely occur in the absence of bony abnormalities. Clin Orthop Relat Res. 2004;(426):145-150. [DOI] [PubMed] [Google Scholar]
- 9. Dolan MM, Heyworth BE, Bedi A, Duke G, Kelly BT. CT reveals a high incidence of osseous abnormalities in hips with labral tears. Clin Orthop Relat Res. 2011;469(3):831-838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ito K, Leunig M, Ganz R. Histopathologic features of the acetabular labrum in femoroacetabular impingement. Clin Orthop Relat Res. 2004;(429):262-271. [DOI] [PubMed] [Google Scholar]
- 11. Seldes RM, Tan V, Hunt J, Katz M, Winiarsky R, Fitzgerald RH., Jr Anatomy, histologic features, and vascularity of the adult acetabular labrum. Clin Orthop Relat Res. 2001;(382):232-240. [DOI] [PubMed] [Google Scholar]
- 12. Malemud CJ. Matrix metalloproteinases (MMPs) in health and disease: an overview. Front Biosci. 2006;11:1696-1701. [DOI] [PubMed] [Google Scholar]
- 13. Gargiulo S, Gamba P, Poli G, Leonarduzzi G. Metalloproteinases and metalloproteinase inhibitors in age-related diseases. Curr Pharm Des. 2014;20(18):2993-3018. [DOI] [PubMed] [Google Scholar]
- 14. de Bruyn M, Vandooren J, Ugarte-Berzal E, Arijs I, Vermeire S, Opdenakker G. The molecular biology of matrix metalloproteinases and tissue inhibitors of metalloproteinases in inflammatory bowel diseases. Crit Rev Biochem Mol Biol. 2016;51(5):295-358. [DOI] [PubMed] [Google Scholar]
- 15. Vo NV, Hartman RA, Yurube T, Jacobs LJ, Sowa GA, Kang JD. Expression and regulation of metalloproteinases and their inhibitors in intervertebral disc aging and degeneration. Spine J. 2013;13(3):331-341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Bluteau G, Conrozier T, Mathieu P, Vignon E, Herbage D, Mallein-Gerin F. Matrix metalloproteinase-1, -3, -13 and aggrecanase-1 and -2 are differentially expressed in experimental osteoarthritis. Biochim Biophys Acta. 2001;1526(2):147-158. [DOI] [PubMed] [Google Scholar]
- 17. Brew K, Nagase H. The tissue inhibitors of metalloproteinases (TIMPs): an ancient family with structural and functional diversity. Biochim Biophys Acta. 2010;1803(1):55-71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Arpino V, Brock M, Gill SE. The role of TIMPs in regulation of extracellular matrix proteolysis. Matrix Biol. 2015;44-46:247-254. [DOI] [PubMed] [Google Scholar]
- 19. Philippon MJ, Michalski MP, Campbell KJ, et al. An anatomical study of the acetabulum with clinical applications to hip arthroscopy. J Bone Joint Surg Am. 2014;96-A(20):1673-1682. [DOI] [PubMed] [Google Scholar]
- 20. Grant AD, Sala DA, Davidovitch RI. The labrum: structure, function, and injury with femoro-acetabular impingement. J Child Orthop. 2012;6(5):357-372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Petersen W, Petersen F, Tillmann B. Structure and vascularization of the acetabular labrum with regard to the pathogenesis and healing of labral lesions. Arch Orthop Trauma Surg. 2003;123(6):283-288. [DOI] [PubMed] [Google Scholar]
- 22. Domzalski ME, Synder M, Karauda A, Papierz W. Histological changes of the acetabular labrum in coxarthrosis: labral degeneration and repair. Hip Int. 2017;27(1):66-73. [DOI] [PubMed] [Google Scholar]
- 23. Dhollander AA, Lambrecht S, Verdonk PC, et al. First insights into human acetabular labrum cell metabolism. Osteoarthritis Cartilage. 2012;20(7):670-677. [DOI] [PubMed] [Google Scholar]
- 24. Aynardi M, Zahoor T, Mitchell R, et al. Orthotopic transplantation of Achilles tendon allograft in rats: with or without incorporation of autologous mesenchymal stem cells. Cell Transplant. 2018;27(2):245-255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Cuttle L, Nataatmadja M, Fraser JF, Kempf M, Kimble RM, Hayes MT. Collagen in the scarless fetal skin wound: detection with picrosirius-polarization. Wound Repair Regen. 2005;13(2):198-204. [DOI] [PubMed] [Google Scholar]
- 26. Da Ré, Guerra F, de Souza Pires IL, de Aro AA, Camargo LC, Pimentel ER, Palomari ET. Protocol on induction of TMJ articular disc degeneration in rats by utilization of botulinum toxin. Arch Oral Biol. 2010;55(7):530-534. [DOI] [PubMed] [Google Scholar]
- 27. Woods AK, Broomfield J, Monk P, Vollrath F, Glyn-Jones S. Dynamic shear analysis: a novel method to determine mechanical integrity of normal and torn human acetabular labra: Implications for prediction of outcome of repair. Bone Joint Res. 2018;7(7):440-446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Leunig M, Beck M, Woo A, Dora C, Kerboull M, Ganz R. Acetabular rim degeneration: a constant finding in the aged hip. Clin Orthop Relat Res. 2003;(413):201-207. [DOI] [PubMed] [Google Scholar]
- 29. Elias-Jones CJ, Farrow L, Reilly JH, et al. Inflammation and neovascularization in hip Impingement: not just wear and tear. Am J Sports Med. 2015;43(8):1875-1881. [DOI] [PubMed] [Google Scholar]
- 30. Chinzei N, Hashimoto S, Fujishiro T, et al. Inflammation and degeneration in cartilage samples from patients with femoroacetabular impingement. J Bone Joint Surg Am. 2016;98-A(2):135-141. [DOI] [PubMed] [Google Scholar]
- 31. Arakaki PA, Marques MR, Santos MC. MMP-1 polymorphism and its relationship to pathological processes. J Biosci. 2009;34(2):313-320. [DOI] [PubMed] [Google Scholar]
- 32. Deng B, Ren JZ, Meng XQ, et al. Expression profiles of MMP-1 and TIMP-1 in lumbar intervertebral disc degeneration. Genet Mol Res. 2015;14(4):19080-19086. [DOI] [PubMed] [Google Scholar]
- 33. Lei P, Sun R, Li K, Hu Y, Liao Z. Morphological changes and expression of MMPs and TIMPs in rabbit degenerated lateral meniscus after PCL-transection. Int J Clin Exp Med. 2015;8(10):17950-17958. [PMC free article] [PubMed] [Google Scholar]
- 34. Kaspiris A, Khaldi L, Grivas TB, et al. Subchondral cyst development and MMP-1 expression during progression of osteoarthritis: an immunohistochemical study. Orthop Traumatol Surg Res. 2013;99(5):523-529. [DOI] [PubMed] [Google Scholar]
- 35. Kapoor M, Martel-Pelletier J, Lajeunesse D, Pelletier JP, Fahmi H. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat Rev Rheumatol. 2011;7(1):33-42. [DOI] [PubMed] [Google Scholar]
- 36. Van Doren SR. Matrix metalloproteinase interactions with collagen and elastin. Matrix Biol. 2015;44-46:224-231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Yu TY, Pang JH, Wu KP, Chen MJ, Chen CH, Tsai WC. Aging is associated with increased activities of matrix metalloproteinase-2 and -9 in tenocytes. BMC Musculoskelet Disord. 2013;14:2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Duerr S, Stremme S, Soeder S, Bau B, Aigner T. MMP-2/gelatinase A is a gene product of human adult articular chondrocytes and is increased in osteoarthritic cartilage. Clin Exp Rheumatol. 2004;22(5):603-608. [PubMed] [Google Scholar]
- 39. Wang H, Lafdil F, Wang L, Yin S, Feng D, Gao B. Tissue inhibitor of metalloproteinase 1 (TIMP-1) deficiency exacerbates carbon tetrachloride-induced liver injury and fibrosis in mice: involvement of hepatocyte STAT3 in TIMP-1 production. Cell Biosci. 2011;1(1):14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Makki MS, Haqqi TM. Histone deacetylase inhibitor vorinostat (SAHA) suppresses IL-1β-induced matrix metallopeptidase-13 expression by inhibiting IL-6 in osteoarthritis chondrocyte. Am J Pathol. 2016;186(10):2701-2708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Bsat S, Frei H, Beaulé PE. The acetabular labrum: a review of its function. Bone Joint J. 2016;98-B(6):730-735. [DOI] [PubMed] [Google Scholar]
- 42. Smith MV, Panchal HB, Ruberte Thiele RA, Sekiya JK. Effect of acetabular labrum tears on hip stability and labral strain in a joint compression model. Am J Sports Med. 2011;39(suppl):103S-110S. [DOI] [PubMed] [Google Scholar]
- 43. de Morais EF, Pinheiro JC, Leite RB, Santos PPA, Barboza CAG, Freitas RA. Matrix metalloproteinase-8 levels in periodontal disease patients: A systematic review. J Periodontal Res. 2018;53(2):156-163. [DOI] [PubMed] [Google Scholar]
- 44. Audenaert EA, Dhollander AA, Forsyth RG, Corten K, Verbruggen G, Pattyn C. Histologic assessment of acetabular labrum healing. Arthroscopy. 2012;28(12):1784-1789. [DOI] [PubMed] [Google Scholar]
- 45. Philippon MJ, Arnoczky SP, Torrie A. Arthroscopic repair of the acetabular labrum: a histologic assessment of healing in an ovine model. Arthroscopy. 2007;23(4):376-380. [DOI] [PubMed] [Google Scholar]