

Abstract
Background
The World Health Organization has declared COVID-19 a global pandemic. This paper presents an epidemiological analysis of the first phase of the COVID-19 epidemic in Poland.
Material/Methods
This cross-sectional study was carried out between 3 and 27 March 2020 on a sample of 1389 laboratory-confirmed COVID-19 cases in Poland. Data were obtained from epidemiological reports collected by the Chief Sanitary Inspectorate. Analysis includes the number of COVID-19 cases, number of deaths, number of hospitalizations, number of people quarantined, and number of laboratory tests performed.
Results
The first case was confirmed on 4 March 2020. Over 24 days after the first case, the total number of confirmed infections rose to 1389 (34,000 laboratory tests were performed). The highest incidence rates (over 5 per 100,000) were observed in the 2 central administrative regions (Mazowieckie and Łódzkie) and in the south-western region of Dolnośląskie, which borders the Czech Republic and Germany. Based on available data about age and sex, a clearly higher incidence was observed in the 20–29 years (4.0 per 100,000), 40–49 years (4.1 per 100,000), and 50–59 years (4.3 per 100,000) age groups. In the period analyzed (24 days), there were 16 confirmed deaths (average age 65.5 years; 81.2% males).
Conclusions
The proportion of women and men with confirmed COVID-19 infection was similar to the sex ratio in the general population. Infections were relatively less common in those aged under 20 years. The largest numbers of confirmed cases were detected in 3 of the 4 largest cities, each of which has an international airport.
MeSH Keywords: Coronavirus, Coronavirus Infections, COVID-19, Epidemics, Incidence
Background
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a new strain of coronavirus that causes the coronavirus disease 2019 (COVID-19) in humans [1]. The origins and possible animal vectors of SARS-CoV-2 are yet to be determined [2]. According to current evidence, SARS-CoV-2 human transmission occurs through respiratory droplets and contact routes [3,4]. Since its emergence in China at the end of 2019, outbreaks of the disease have spread rapidly through Asia, the Americas, Europe, Australia, and Africa, resulting in a pandemic proclaimed by the World Health Organization (WHO) on 11 March 2020 [1,5].
The severity of symptoms in the clinical presentation of COVID-19 ranges from mild to critical, while some cases remain asymptomatic. At diagnosis, most cases are mild or moderate, 14% require hospitalization and oxygen support, and 5% require treatment in the intensive care unit [6]. The most common clinical manifestations in adults are fever, dry cough, and fatigue. Less frequent symptoms are productive cough, sore throat, pain, nausea, and diarrhea. Dyspnea, acute respiratory disease syndrome, sepsis, and multiorgan failure can occur as the condition becomes more severe [7–9].
The most common laboratory and radiologic findings are lymphopenia and bilateral ground-glass opacities on chest computed tomography (CT), respectively. Other laboratory findings include elevated levels of C-reactive protein, prolonged prothrombin time, elevated lactate dehydrogenase (LDH), and thrombocytopenia [9,10], as well as elevated alanine aminotransferase (ALT), aspartate aminotransferase (ASP), and γ-glutamyltransferase (γ-GT) levels [11].
According to the WHO interim guidance, suspected COVID-19 cases should be screened for the virus with nucleic acid amplification tests, such as real-time reverse-transcription polymerase chain reaction (rRT-PCR), performed in properly equipped laboratories by qualified personnel. Respiratory material should be collected either from the upper respiratory tract as a nasopharyngeal or oropharyngeal swab in ambulatory patients, or from the lower respiratory tract (from sputum, endotracheal aspirate, or bronchoalveolar lavage) in patients with severe disease [12].
As of 27 March 2020, China had reported 82,079 cases of COVID-19 and 3298 deaths [13]. Based on “The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19) – China, 2020”, a study that included 72,314 patient records out of which 44,672 were confirmed COVID-19 cases, the majority of cases were 30–69 years old (77.8%), male (51.4%), and classified as mild severity (80.9%). The case-fatality rate (CFR) was 2.8% for males and 1.7% for females. The highest CFR was noted in those aged ≥80 years (14.8%). The CFRs were higher among patients with underlying chronic conditions (cardiovascular disease, 10.5%; diabetes, 7.3%; and hypertension, 6%) [6].
As of 27 March 2020, the European Union/European Economic Area (EU/EEA) and the United Kingdom together had reported 265,421 cases of COVID-19 and 15,798 deaths [13]. People with underlying chronic diseases and the elderly were at greater risk of severe illness and death. The available data from Italy, Spain, and Germany indicated that absolute numbers of deaths had rapidly increased with age for those aged 60 years and above [14].
According to the Istituto Superiore di Sanità, which collects data on cases that have tested positive for SARS-CoV-2 in Italy, the majority of cases were above 50 years old (73.6%), male (57.2%), and classified as mild severity (39.7%). The case-fatality rate (CFR) was 9.2% for males and 6.5% for females. The highest CFR had been noted in the group aged 80–89 years (25.2%), closely followed by those aged ≥90 years (24.5%). It was reported that 73.8% of the fatalities had hypertension, 33.9% had diabetes, 30.1% had ischemic heart disease, 22% had atrial fibrillation, and 20.2% had chronic renal failure [15–17].
As reported by the Instituto de Salud Carlos III, which collects data on cases that tested positive for SARS-CoV-2 in Spain, the majority of cases were above 40 years old (81.6%), male (50.4%), and not hospitalized (54%). The case-fatality rate (CFR) was 3.7%. The highest CFR was in those aged over 80 years (14.6%). Men had a higher prevalence of symptoms (fever and cough), pneumonia, and underlying diseases (cardiovascular, respiratory, diabetes), and a higher percentage of hospitalizations, admissions to intensive care units, and case-fatality rate than women [18].
This article presents an epidemiological analysis of the first phase of the COVID-19 epidemic in Poland.
Material and Methods
This cross-sectional study was carried out between 3 and 27 March 2020 on a sample of 1389 laboratory-confirmed COVID-19 cases in Poland. Data were obtained from epidemiological reports collected by the Chief Sanitary Inspectorate, which is a public administration authority involved in public health services in Poland, and it was tasked with responding to the novel coronavirus (SARS-CoV-2) outbreak. The State Sanitary Inspectorate has territorial representatives within administrative regions (poviat and voivodship – Polish equivalents of the county and province, respectively), including 318 poviat sanitary inspectorates, 16 voivodship inspectorates, and 10 border sanitary inspectorates [19]. According to the administrative division, data on the number of COVID-19 cases was reported by poviat sanitary inspectorates to voivodship sanitary inspectorates, which sent daily reports to the Chief Sanitary Inspectorate.
A report of a laboratory-confirmed SARS-CoV-2 case included sex, age, administrative region, and date of laboratory test. Moreover, the State Sanitary Inspection collected data on: (1) the number of hospitalizations due to COVID-19 (confirmed/suspected cases); (2) the number of people quarantined (those who had had close contact with a suspected or confirmed COVID-19 case); and (3) the number of deaths from COVID-19. Data on laboratory tests (real-time RT-PCR assays for the detection of SARS-CoV-2) were obtained from official announcements of the Polish Ministry of Health.
Laboratory testing for COVID-19 was performed for suspected cases according to the ECDC/WHO guidelines (real-time RT-PCR assays for the detection of SARS-CoV-2) [20]. Testing was free of charge and available throughout Poland. By 27 March 2020, there had been 1389 laboratory-confirmed SARS-CoV-2 cases identified.
Due to missing data (sex and age) resulting from restrictions on the flow of information and the number of laboratories involved, this preliminary analysis included the characteristics of 1157 confirmed COVID-19 cases.
The population data were taken from the Local Data Bank (Central Statistical Office), showing the current state of the population as of 30 June 2019 [21].
Data from epidemiological reports were anonymized. It was not possible to identify individual subjects at any stage of the analysis. All procedures involving human participants were in accordance with the ethical standards of the National Research Committee and with the 1964 Helsinki Declaration and its later amendments.
All analyses were performed with IBM SPSS ver. 25. The level of statistical significance was not determined because the observations pertained to the entire population. The maps were made using QGIS 3.12.1 software.
Results
By 27 March 27, there had been 1389 cases of COVID-19 infections officially identified in Poland (confirmed by laboratory tests). A total of 34,000 laboratory tests to detect infection had been conducted. The first case was confirmed on 4 March 2020 in a 66-year-old man who had arrived from Germany. The details are shown in Figure 1.
Figure 1.
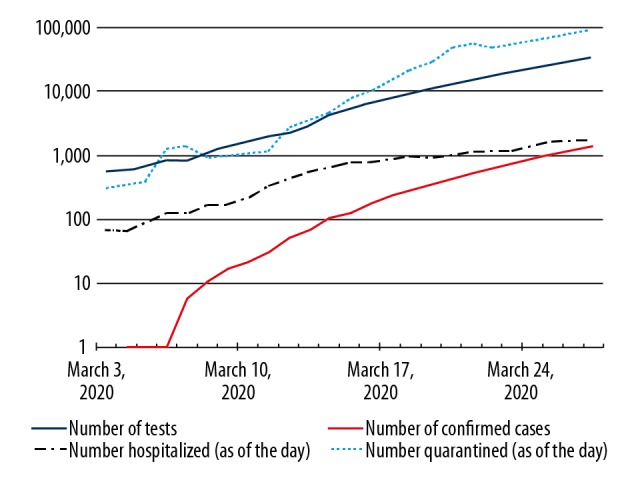
Development of the COVID-19 epidemic in Poland. Number of: confirmed cases (total), hospitalized patients with suspected or confirmed infection, quarantined people, and laboratory tests performed (total). Data are presented on a logarithmic scale.
The highest incidence rates (over 5 per 100,000 inhabitants) were in the 2 central voivodships (Mazowieckie and Łódzkie) and a south-western voivodship (Dolnośląskie) that borders the Czech Republic and Germany. The capital of Poland (Warsaw) is located in Mazowieckie voivodship. The detailed data are presented in Figure 2.
Figure 2.
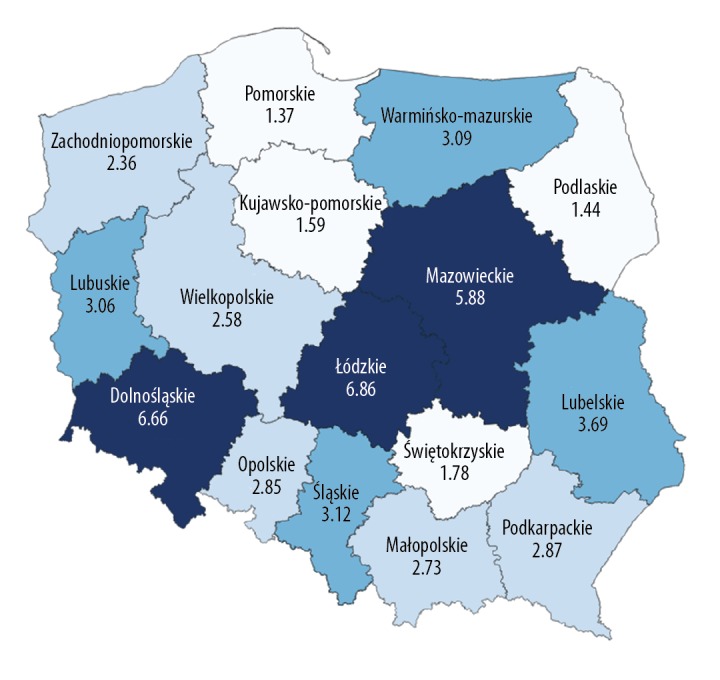
The incidence rate per 100,000 inhabitants by voivodship in Poland (n=1389).
Cases of COVID-19 were confirmed in 199 out of the 380 poviats in Poland. The actual numbers may have been higher because data from Mazowieckie voivodship were registered with a delay. The highest numbers of cases were identified in the largest cities in Poland: Wrocław (Dolnośląskie voivodship), Warsaw (Mazowieckie voivodship), and Łódź (Łódzkie voivodship). The details are shown in Figure 3.
Figure 3.
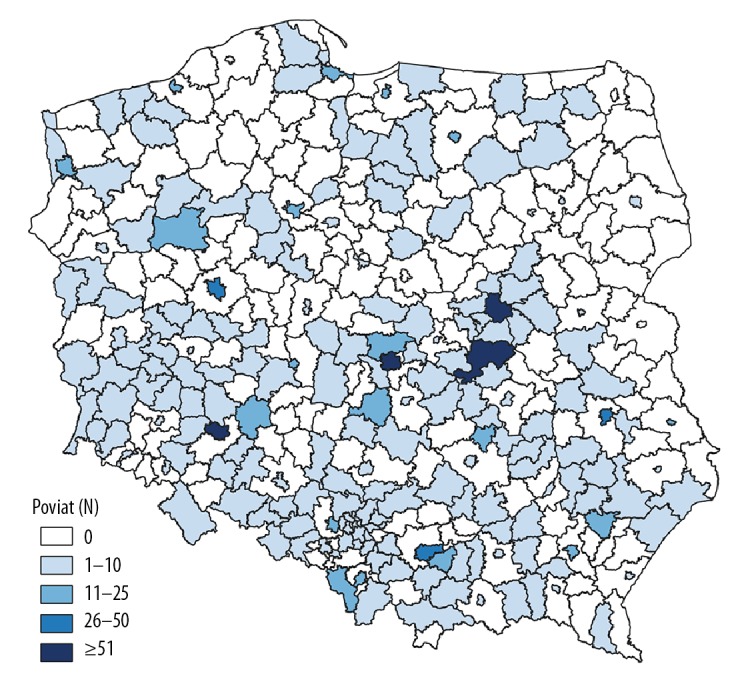
Number of confirmed COVID-19 cases in poviats in Poland (n=1300). * Detailed data for the Mazowieckie voivodship was recorded with a delay.
Of the 1157 confirmed cases for which data on the age and sex of those infected were available at the time this manuscript was prepared, women represented 50.5% of the cases. The age and sex distributions for confirmed COVID-19 cases were generally similar to the distribution of these variables in the general population. The biggest difference concerned the share of the youngest age groups – those under 10 years and 10–19 years – which together constituted 20.0% of the population, while the percentage of confirmed cases within this group was 7.4%.
The share of the group aged 20–39 years (30.2%) among the confirmed cases was similar to the share of this age group in the population (28.2%). Those aged 60 years and older accounted for 24.8% of confirmed cases, compared to 25.0% in the general population. The detailed data are presented in Table 1.
Table 1.
Confirmed COVID-19 cases: age and sex distribution compared to the general Polish population.
| Age groups | COVID-19 confirmed cases (n=1157) | Population | Difference: confirmed cases vs. population [percentage points] | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Female | Male | Total | Female | Male | Total | Female | Male | Total | |
| ≤9 | 2.1% | 1.0% | 1.6% | 9.5% | 10.8% | 10.1% | −7.5 | −9.7 | −8.6 |
| 10–19 | 5.5% | 6.3% | 5.9% | 9.3% | 10.5% | 9.9% | −3.9 | −4.2 | −4.0 |
| 20–29 | 17.3% | 15.0% | 16.2% | 11.4% | 12.7% | 12.1% | 5.8 | 2.3 | 4.1 |
| 30–39 | 12.2% | 15.9% | 14.0% | 15.4% | 16.9% | 16.1% | −3.3 | −1.0 | −2.1 |
| 40–49 | 17.3% | 22.5% | 19.9% | 13.9% | 15.1% | 14.5% | 3.4 | 7.5 | 5.4 |
| 50–59 | 21.1% | 14.3% | 17.7% | 12.1% | 12.5% | 12.3% | 8.9 | 1.8 | 5.4 |
| 60–69 | 13.9% | 14.7% | 14.3% | 14.2% | 12.9% | 13.6% | −0.3 | 1.8 | 0.7 |
| 70–79 | 6.7% | 6.6% | 6.7% | 8.2% | 6.0% | 7.1% | −1.5 | 0.7 | −0.4 |
| 80+ | 4.1% | 3.7% | 3.9% | 5.8% | 2.8% | 4.4% | −1.7 | 0.9 | −0.5 |
At 24 days after the official confirmation of the first COVID-19 case in Poland, the incidence rate (based on 1157 cases) was 3.01 per 100,000 residents and this was slightly higher among men (3.09) than among women (2.95). Based on available data about age and sex, a clearly higher incidence was noted in the 20–29 years (4.0 per 100,000), 40–49 years (4.1 per 100,000), and 50–59 years (4.3 per 100,000) age groups. The largest difference according to sex was noted in the age group of 80 years and older (2.1 among women vs. 4.0 among men). The details are presented in Figure 4.
Figure 4.

Incidence of COVID-19 in Poland (confirmed cases) per 100,000 population (n=1157).
In the period analyzed (24 days), there were 16 confirmed deaths due to COVID-19 (Table 2). Most of the fatalities (81.2%) were men. Comorbidities were present in all fatalities but one. The average age at death was 65.5 years (median 67.5). The youngest person was 37 years old and the oldest was 84. The average age was 59.3 years among women (median 57) and 66.5 years among men (median 68).
Table 2.
Characteristics of deaths from COVID-19 (confirmed cases).
| No. | Age | Sex | Date of death | Voivodship | Comorbidities |
|---|---|---|---|---|---|
| 1 | 57 | Female | 12 Mar 2020 | Wielkopolskie | Yes |
| 2 | 73 | Male | 13 Mar 2020 | Dolnośląskie | Yes |
| 3 | 66 | Male | 15 Mar 2020 | Lubelskie | Yes |
| 4 | 67 | Male | 16 Mar 2020 | Podkarpackie | Yes |
| 5 | 57 | Male | 17 Mar 2020 | Dolnośląskie | Yes |
| 6 | 37 | Female | 22 Mar 2020 | Wielkopolskie | Yes |
| 7 | 43 | Male | 22 Mar 2020 | Mazowieckie | No |
| 8 | 83 | Male | 23 Mar 2020 | Śląskie | Yes |
| 9 | 68 | Male | 24 Mar 2020 | Lubelskie | Yes |
| 10 | 71 | Male | 24 Mar 2020 | Śląskie | Yes |
| 11 | 41 | Male | 25 Mar 2020 | Dolnośląskie | Yes |
| 12 | 71 | Male | 25 Mar 2020 | Dolnośląskie | Yes |
| 13 | 80 | Male | 25 Mar 2020 | Świętokrzyskie | Yes |
| 14 | 67 | Male | 26 Mar 2020 | Zachodniopomorskie | Yes |
| 15 | 78 | Male | 26 Mar 2020 | Mazowieckie | Yes |
| 16 | 84 | Female | 26 Mar 2020 | Mazowieckie | Yes |
Discussion
Key results
Within 24 days of confirmation of the first COVID-19 case in Poland, the number of cases increased to 1389. The sex distribution among the confirmed cases was similar to the sex ratio in the general population (for women: 50.5% of those infected, which is 51.6% of the population). Age distribution by sex was also similar to the sex ratio in the general population. The largest difference from the general population was noted among people under 20 years of age, as the age cohort of 0–19 years accounted for 7.4% of those infected and 20.0% of the general population. Incidence rates in Poland were highest in the 20–29, 40–49, and 50–59 years age groups. A significant difference in incidence rates according to sex was noted among individuals aged 80 years and over (2.1 among women vs. 4.0 among men). Most cases occurred in the largest cities (Warsaw, Łódź, and Wrocław). All these cities have international airports. Among the 16 confirmed deaths due to COVID-19, 13 of the fatalities (81.2%) were men.
Interpretation
The first cases of COVID-19 in Europe were reported on 24 January 2020 in France, 4 days later in Germany and, on 31 January 31 in Italy, Spain, the United Kingdom, and Sweden. The first case of SARS-CoV-2 infection in Poland was reported on 4 March. On 12 March, the WHO Regional Director for Europe described this region as the center of the pandemic. Five days later, every European country had at least 1 confirmed case of COVID-19 [22,23].
The age and sex distribution of confirmed COVID-19 cases in Poland differed in some respects from other European countries. The first difference was that among all confirmed cases of COVID-19 in Poland, there were slightly more women, while in Spain and Italy the situation was the opposite. The pattern of deaths was similar, with men constituting the vast majority of fatalities, as in other countries.
The demographic structures of Spain and Poland are comparable, although in Spain the group of people aged above 65 years of age represents a slightly larger proportion of the general population. The overall proportion of confirmed COVID-19 cases in adults in the 50–59 age group and among women aged 30–49 and 70–79 years were similar [18].
The proportion of women among confirmed COVID-19 cases aged 50–69 was similar in Poland and Italy. A greater proportion of women and men in the younger age groups was noted in Poland in comparison with Italy. This may have been due to a larger proportion of young people in the Polish population, while in Italy those over age 65 years constitute a major part of the population [16]. The relatively high incidence of COVID-19 among those aged 20–29 years in Poland may have been due to the winter university break in Poland, when Northern Italy becomes a popular tourist destination. When they came back, they could have introduced COVID-19 to their home towns and transmitted the disease to their relatives (parents); hence, the high incidence in the age group of 50–59 years in Poland. The second hypothesis is that people aged 40–59 years were healthcare workers. At present it is impossible to test this hypothesis, but it merits further research.
The number of COVID-19 cases in the age group under 20 years was relatively small. However, people aged 20–29 years were one of the most affected age groups, which indicates that preventive measures against the new coronavirus should also target young adults. While deaths were most common in the elderly, asymptomatic young people or those with very mild symptoms may have spread the infection to their relatives, especially parents and grandparents.
Limitations
This study has several limitations. First, this study offers a preliminary characterization of confirmed COVID-19 cases in Poland. At the time this manuscript was submitted, the epidemic is ongoing and new COVID-19 cases are being reported every day. In cases of outbreaks occurring in specific facilities (e.g., nursing homes), the age structure of patients may change. Second, the laboratory testing method (real-time RT-PCR assays for the detection of SARS-CoV-2) is time-consuming and can generate reporting delays in the event of multiple outbreaks. Nevertheless, it is the only diagnostic method recommended by the WHO that guarantees reliable results [24]. Currently, rapid serological tests for the diagnosis of coronavirus are not used as a diagnostic method in COVID-19 in Poland. Third, the number of confirmed cases is strongly correlated with the number of tests performed, and this factor should be taken into account when assessing the results presented in this paper.
Conclusions
Analysis of the first phase of the COVID-19 epidemic development in Poland indicates the following conclusions:
The proportions of women and men among confirmed cases were similar to their respective shares in the general population.
Infections were relatively less common in Poles below 20 years of age.
Almost one-third of confirmed cases were people aged 20–39 years.
The largest number of confirmed cases were identified in 3 of the 4 largest cities, each of which has an international airport.
Among the confirmed deaths from COVID-19, the vast majority were men over 65 years of age.
Footnotes
Source of support: Self financing
References
- 1.European Center for Disease Prevention and Control. COVID-19. https://www.ecdc.europa.eu/en/novel-coronavirus-china.
- 2.Ye G, Pan Z, Pan Y, et al. Clinical characteristics of severe acute respiratory syndrome coronavirus 2 reactivation J Infect 2020[Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liu J, Liao X, Qian S, et al. Community transmission of severe acute respiratory syndrome coronavirus 2, Shenzhen, China, 2020 Emerg Infect Dis 2020[Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cai J, Sun W, Huang J, et al. Indirect virus transmission in cluster of COVID-19 cases, Wenzhou, China, 2020 Emerg Infect Dis 2020[Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19–11 March 2020. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020.
- 6.The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. Vital surveillances: The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) – China, 2020. China CDC Weekly. 2020;2(8):113–22. [PMC free article] [PubMed] [Google Scholar]
- 7.Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet. 2020;395(10223):507–13. doi: 10.1016/S0140-6736(20)30211-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study Lancet Respir Med 2020[Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China JAMA 2020[Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China N Engl J Med 2020[Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zhao D, Yao F, Wang L, et al. A comparative study on the clinical features of COVID-19 pneumonia to other pneumonias Clin Infect Dis 2020[Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.World Health Organization. Laboratory testing for coronavirus disease 2019 (COVID-19) in suspected human cases: interim guidance. https://apps.who.int/iris/handle/10665/331329.
- 13.European Center for Disease Prevention and Control. Situation update worldwide, as of 28 March 2020. URL: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases.
- 14.European Center for Disease Prevention and Control. Rapid risk assessment: Coronavirus disease 2019 (COVID-19) pandemic: Increased transmission in the EU/EEA and the UK – seventh update. https://www.ecdc.europa.eu/sites/default/files/documents/RRA-seventh-update-Outbreak-of-coronavirus-disease-COVID-19.pdf.
- 15.Istituto Superiore di Sanità. Integrated surveillance COVID-19 in Italy. https://www.epicentro.iss.it/coronavirus/bollettino/Infografica_27marzo%20ITA.pdf [in Italian]
- 16.Istituto Superiore di Sanità. Epidemia COVID-19. Aggiornamento nazionale. https://www.epicentro.iss.it/coronavirus/bollettino/Bollettino-sorveglianza-integrata-COVID-19_26-marzo%202020.pdf [in Italian]
- 17.Istituto Superiore di Sanità. Characteristics of COVID-19 patients dying in Italy. Report based on available data on March 20th, 2020. https://www.epicentro.iss.it/coronavirus/bollettino/Report-COVID-2019_20_marzo_eng.pdf [in Italian]
- 18.Instituto de Salud Carlos III. Informesobre la situación de COVID-19 enEspaña. Informe COVID-19 nº 17. De Marzo De. 2020. https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/INFORMES/Informes%20COVID-19/Informe%20n%C2%BA%2017.%20Situaci%C3%B3n%20de%20COVID-19%20en%20Espa%C3%B1a%20a%2027%20marzo%20de%202020_revisado.pdf [in Italian]
- 19.Chief Sanitary Inspectorate. About the Inspection. [cited 2020 Mar 28]. https://gis.gov.pl/en/homepage/
- 20.European Centre for Disease Prevention and Control. Case definition and European surveillance for COVID-19, as of 2 March 2020. https://www.ecdc.europa.eu/en/case-definition-and-european-surveillance-human-infection-novel-coronavirus-2019-ncov.
- 21.Central Statistical Office. Local Data Bank, as of 30 June 2019. https://bdl.stat.gov.pl/BDL/metadane/cechy/3472?back=True.
- 22.European Centre for Disease Prevention and Control. Situation update worldwide, as of: January 24, January 28, January 31, March 4, March17. https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases.
- 23.World Health Organization. WHO announces COVID-19 outbreak a pandemic. http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic.
- 24.World Health Organization. Laboratory testing for coronavirus disease (COVID-19) in suspected human cases. https://www.who.int/publications-detail/laboratory-testing-for-2019-novel-coronavirus-in-suspected-human-cases-20200117.