

Abstract
Purpose
To evaluate the chest CT findings in an environmentally homogeneous cohort from the cruise ship Diamond Princess with coronavirus disease 2019 (COVID-19).
Materials and Methods
This retrospective study comprised 104 cases (mean age, 62 years ± 16 [standard deviation], range, 25–93 years) with COVID-19 confirmed with reverse-transcription polymerase change reaction findings. CT images were reviewed, and the CT severity score was calculated for each lobe and the entire lung. CT findings were compared between asymptomatic and symptomatic cases.
Results
Of 104 cases, 76 (73%) were asymptomatic, 41 (54%) of which had lung opacities on CT. Twenty-eight (27%) cases were symptomatic, 22 (79%) of which had abnormal CT findings. Symptomatic cases showed lung opacities and airway abnormalities on CT more frequently than asymptomatic cases [lung opacity; 22 (79%) vs 41 (54%), airway abnormalities; 14 (50%) vs 15 (20%)]. Asymptomatic cases showed more ground-glass opacity (GGO) over consolidation (83%), while symptomatic cases more frequently showed consolidation over GGO (41%). The CT severity score was higher in symptomatic cases than asymptomatic cases, particularly in the lower lobes [symptomatic vs asymptomatic cases; right lower lobe: 2 ± 1 (0–4) vs 1 ± 1 (0–4); left lower lobe: 2 ± 1 (0–4) vs 1 ± 1 (0–3); total score: 7 ± 5 (1–17) vs 4 ± 2 (1–11)].
Conclusion
This study documented a high incidence of subclinical CT changes in cases with COVID-19. Compared with symptomatic cases, asymptomatic cases showed more GGO over consolidation and milder extension of disease on CT.
An earlier incorrect version appeared online. This article was corrected on April 8, 2020.
© RSNA, 2020
Summary
This study revealed a high incidence of subclinical CT changes in COVID-19 infected cases, which showed more ground-glass opacity predominance over consolidation and milder severity on CT than in symptomatic cases.
Key Points
■ Of 104 cases analyzed, 76 (73%) were asymptomatic, 41 (54%) of which had pneumonic changes on CT; 28 (27%) cases were symptomatic, 22 (79%) of which had abnormal CT findings.
■ Asymptomatic cases showed more ground-glass opacity (GGO) predominance over consolidation (83%), while symptomatic cases were more likely to show a consolidation predominance over GGO (41%).
■ Asymptomatic cases showed milder CT severity score than symptomatic cases.
Introduction
The respiratory infection caused by a new strain of coronavirus not previously identified in humans, severe acute respiratory syndrome coronavirus 2, has received the name of coronavirus 19 (COVID-19) (1). Originally reported in December 2019 as “pneumonia of unknown cause” in Wuhan City, Hubei Province, China, COVID-19 has spread rapidly and progressively to other regions of China as well as adjacent Asian countries (2). The International Health Regulations Emergency Committee of the World Health Organization (WHO) officially declared the outbreak a “public health emergency of international concern” on January 30, 2020, and the disease was declared pandemic on March 11, 2020.
Recently, the international cruise ship Diamond Princess, carrying about 3700 passengers, temporarily became the largest cluster of COVID-19 cases outside China (3). The cruise ship docked at Yokohama Bay, Japan, on February 3, 2020, and after quarantine, passengers started to disembark on February 14, 2020. The Ministry of Health, Labor, and Welfare from Japan reported that of the 1723 national passengers, a cumulative number of 454 cases were recognized as pathogen carriers on real-time reverse-transcription polymerase chain reaction (RT-PCR) testing, including 189 asymptomatic cases who initially tested negative on February 17, 2020. During and after the quarantine period, passengers and crew members were referred to the Japan Self-Defense Forces Central Hospital by the government.
The clinical course and spectrum of radiologic patterns seen in COVID-19 have gradually become apparent with recent publications; however, most publications have been focused on symptomatic cases occurring in China (9,13,15–19). This prompted us to undertake the present study to retrospectively evaluate the CT findings in laboratory-confirmed cases of COVID-19, conveniently sampled from the passengers and crew members of the Diamond Princess cruise ship in Japan. We specifically compared the radiologic findings of COVID-19 infection between asymptomatic and symptomatic cases.
Materials and Methods
Cases
This study was approved by the institutional ethics review board, and written informed consent was obtained from all cases. In this retrospective study, the medical records were reviewed for clinical and imaging findings of cases diagnosed with COVID-19 from February 7 to 28, 2020. Passengers and crew members of the Diamond Princess cruise ship underwent RT-PCR testing during the quarantine period, and those who showed positive results were transferred to hospitals in Japan. Among all RT-PCR positive cases from the cruise ship, asymptomatic, mildly symptomatic, or familial clusters with infection among relatives were admitted to the Japan Self-Defense Forces Central Hospital (Tokyo, Japan) for further investigation. Consecutive cases from this single-center cohort who had confirmed COVID-19 infection and underwent chest CT were included. Those who showed negative results on RT-PCR underwent repeat RT-PCR examination. On admission, all cases underwent chest CT irrespective of the RT-PCR results, based on the following grounds: (a) a previous report describing positive CT findings in cases with RT-PCR positive status without symptoms (4,5), (b) previous reports of person-to-person transmission from asymptomatic cases (6–8), and (c) the need to judge the precaution level necessary on admission to prevent nosocomial infection in the hospital. Based on our previous experience, CT parameters were optimized to minimize patient exposure to radiation as detailed below.
Clinical Data
The following data were extracted from the medical records: demographic data, medical history, presence or absence of underlying comorbidities, symptoms, and signs. Cases were classified as symptomatic if they had any signs or symptoms of pneumonia, including fever (> 37.5°C), cough, dyspnea, and fatigue on admission. Otherwise, cases were classified as asymptomatic.
Chest CT Acquisition
Nonenhanced chest CT was performed using a six-row multidetector CT unit (SOMATOM Emotion 6; Siemens, Tokyo, Japan) on admission with the following parameters: tube voltage, 130 kVp; effective current, 95 mA; collimation, 6 × 2 mm, helical pitch, 1.4. Acquisition parameters were modified to minimize patient radiation exposure while maintaining sufficient resolution for chest CT evaluation. Based on measurements of the dosimetry phantom (diameter 32 cm, length 35 cm) under automatic exposure control (CARE Dose4D; Siemens, Tokyo, Japan), the radiation exposure of each patient was estimated to be less than 2.8 mSv. CT images were acquired during a single inspiratory breath-hold to minimize motion artifacts. A 2.0-mm gapless section was reconstructed before being reviewed on the picture archiving and communication system monitor.
Image Analysis
Image analysis was performed independently by three chest radiologists (A.F., M.J., and S.I., with 31, 19, and 6 years of experience, respectively), who were blinded to the clinical data, followed by joint consensus. The chest CT findings were recorded based on the Fleischner Society glossary of terms (9–12). Parameters evaluated included: the presence or absence of ground-glass opacity (GGO), consolidation, intra- or interlobular septal thickening, linear opacities (including subpleural curvilinear opacities), and “reversed halo” sign. According to the proportion of each pattern in comparison with the totality of the lung opacification, cases were classified as GGO dominant or consolidation dominant, if the proportion of each one of the patterns was respectively greater than 50% of the total (13). Zonal distribution patterns of the lesion were visually classified as peripheral predominant (involving mainly the peripheral one-third of the lung), central or peribronchovascular predominant, or mixed (without predilection for subpleural or central region) (14).
The number of lobes involved and laterality of lung abnormalities were determined. A semiquantitative scoring system was used to quantitatively estimate the pulmonary involvement of all these abnormalities on the basis of the percentage of the total lung involved per lobe (9,15). The extension of the lung opacification was visually scored from 0 to 5 as follows: score 1, 1%–5% involvement; score 2, 6%–25% involvement; score 3; 26%–50% involvement; score 4, 51%–75% involvement; score 5, 76%–100% involvement. Total lung scores were calculated as the sum of individual lobe scores.
The presence or absence of pleural effusion, thoracic lymphadenopathy (as defined by lymph node size of ≥ 10 mm in short-axis dimension), airway abnormalities (ie, airway wall thickening, bronchiectasis, and endoluminal secretions), and any underlying lung disease, including emphysema or fibrosis was also recorded.
Statistics
Statistical analysis was done using the SPSS 11.0 statistical software program (Dr. SPSS II for Windows, standard version 11.0; SPSS, Chicago, Ill). Quantitative variables were expressed as mean ± standard deviation (range), and the categorical variables were presented as the percentage of the total. The comparisons of categorical data were evaluated using Pearson χ2 test and nonpaired quantitative data using the Mann-Whitney U test, according to the normal distribution assessed by the Shapiro-Wilk test. Statistical significance level was set at P < .05.
Results
Clinical Findings
Demographics and clinical characteristics of the study population are summarized in Table 1. The study population comprised 104 cases (54 men, mean age, 60 years ± 17, range: 31–87 years; 50 women, 63 years ± 15, range: 25–93 years). Of these cases, 76 (73%) were asymptomatic, and 28 (27%) cases were symptomatic. The most frequent symptoms on admission were cough (20 [19%] cases), fever (11 [11%] cases), and fatigue (10 [10%] cases).
Table 1:
Characteristics of the Patient Cohort

Chest CT Findings
The frequencies of the major chest CT findings of all cases are summarized in Table 2. Abnormal lung opacities (GGO and/or consolidation) and airway abnormalities (bronchiectasis and/or bronchial wall thickening) were present in 63 (61%) and 29 (28%) of the whole cohort, respectively. Lung opacities on CT were found in 41 (54%) of 76 asymptomatic. Twenty-two (79%) of 28 symptomatic cases had abnormal CT findings consistent with viral pneumonia. Comparing the two groups, symptomatic cases showed lung parenchymal and airway abnormalities on CT more frequently than did asymptomatic cases [symptomatic vs asymptomatic, lung opacity: 22 (79%) vs 41 (54%), P = .023; airway lesion: 14 (50%) vs 15 (20%), P < .002]. No significant differences in age, sex distribution, or comorbidities were identified between symptomatic and asymptomatic cases. Representative CT patterns of asymptomatic cases are shown in Figures 1–3.
Table 2:
Frequency of Lung Abnormalities on CT

Figure 1:
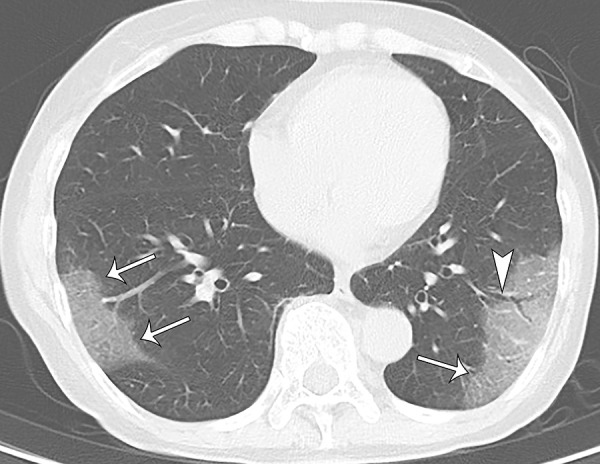
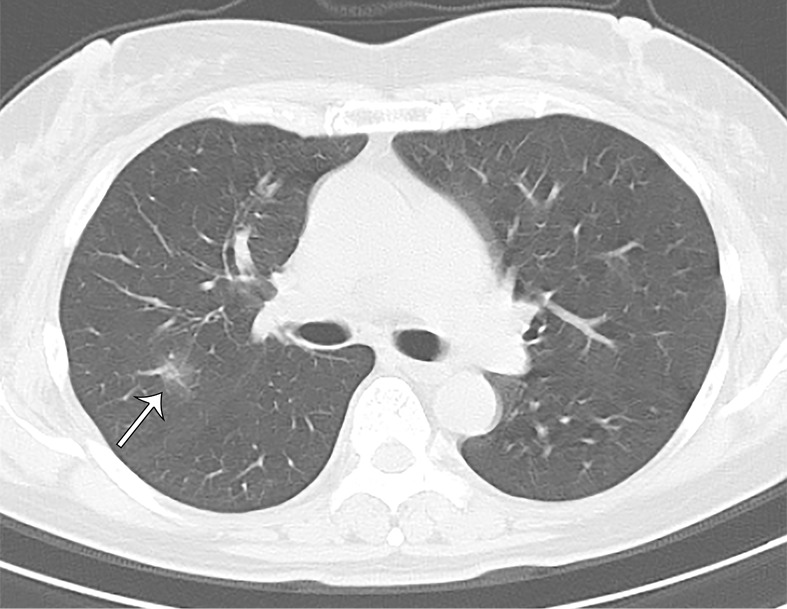
A 70-year-old asymptomatic woman. On axial CT image, focal subpleural ground-glass opacities with smooth intralobular and interlobular septal thickening were demonstrated in the right and left lower lobes (arrows). The left lower lobe lesion was accompanied by air bronchogram with mild bronchial dilatation (arrowhead).
Figure 3a:
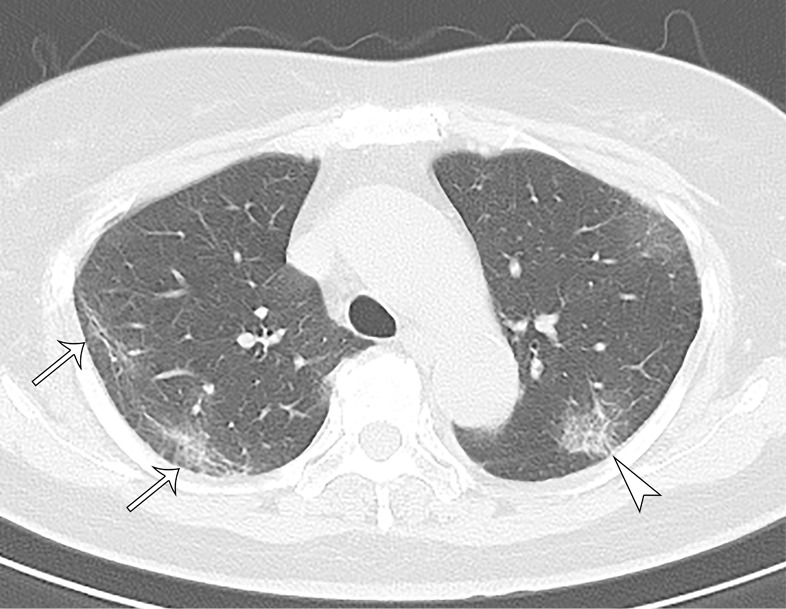
A 73-year-old asymptomatic woman. (a) On axial CT images, focal peripheral ground-glass opacities with intralobular and interlobular smooth septal thickening were shown in the left (arrowhead) and right upper lobe (arrows). The right upper lobe lesions were accompanied by subpleural curvilinear lines (arrow). (b, c) Diffuse ground-glass (reticular) opacities with consolidation with bronchiectasis and bronchial wall thickening were demonstrated in the left and right lower lobes.
Figure 2b:
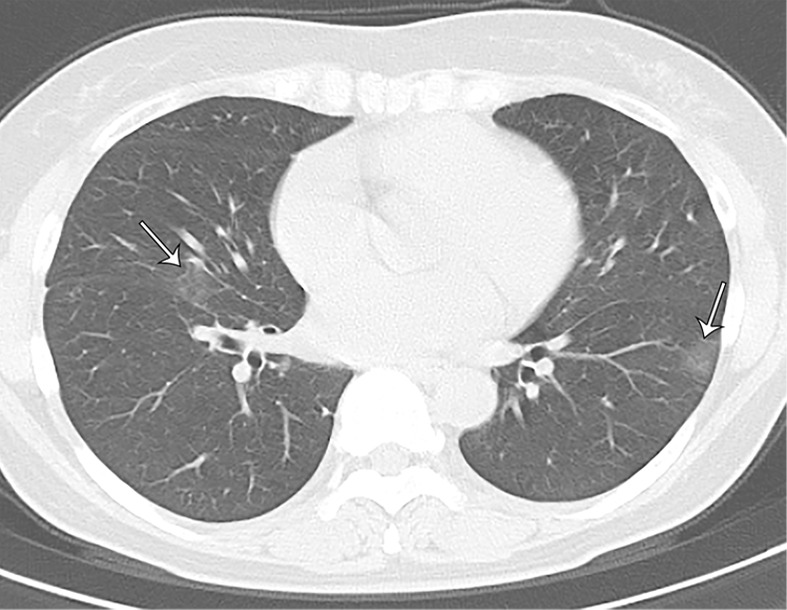
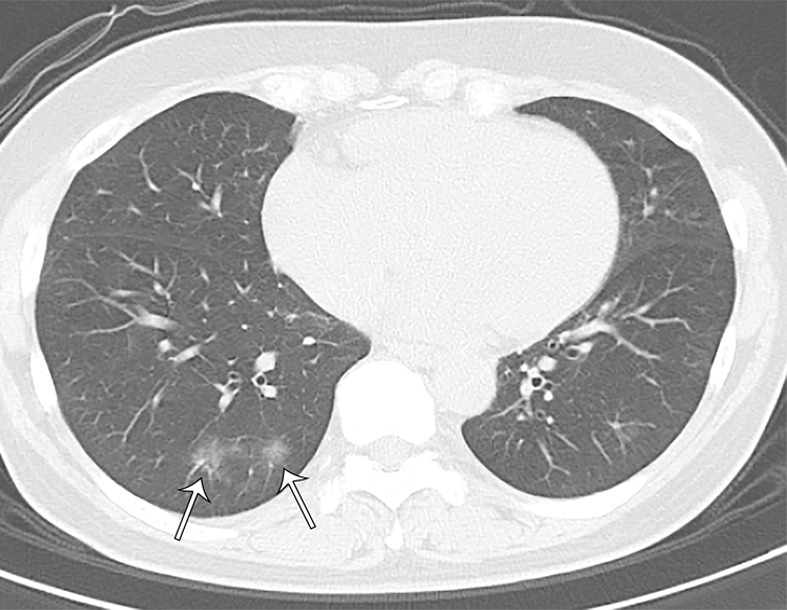
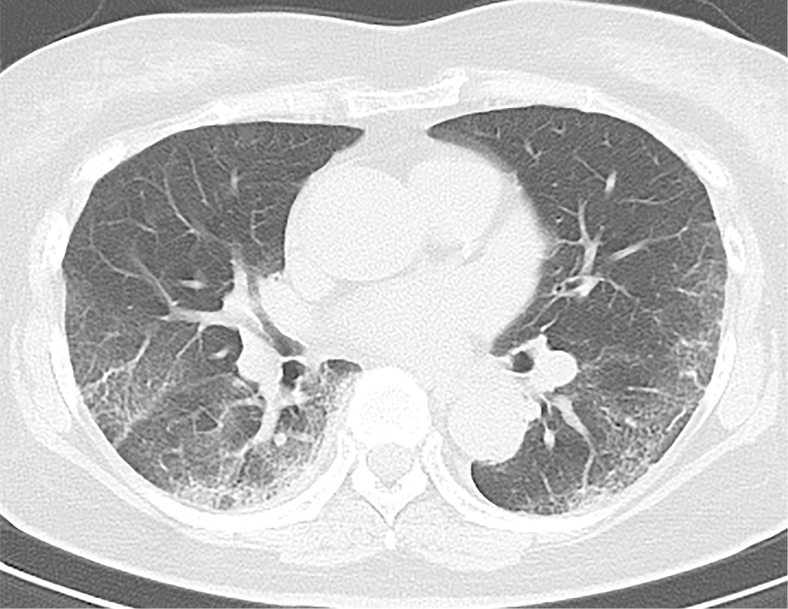
A 66-year-old asymptomatic woman. On axial CT images, focal rounded ground-glass opacities (arrows) with partial consolidation in a peribronchial and subpleural distribution were noted in the right upper (a), middle (b), and lower (c) lobes and left lower (b) lobe.
Figure 2c:
A 66-year-old asymptomatic woman. On axial CT images, focal rounded ground-glass opacities (arrows) with partial consolidation in a peribronchial and subpleural distribution were noted in the right upper (a), middle (b), and lower (c) lobes and left lower (b) lobe.
Figure 3b:
A 73-year-old asymptomatic woman. (a) On axial CT images, focal peripheral ground-glass opacities with intralobular and interlobular smooth septal thickening were shown in the left (arrowhead) and right upper lobe (arrows). The right upper lobe lesions were accompanied by subpleural curvilinear lines (arrow). (b, c) Diffuse ground-glass (reticular) opacities with consolidation with bronchiectasis and bronchial wall thickening were demonstrated in the left and right lower lobes.
Figure 3c:
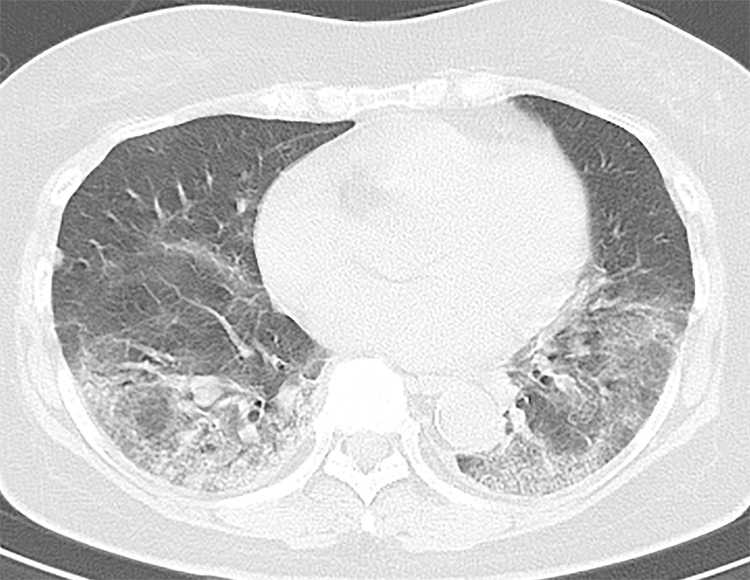
A 73-year-old asymptomatic woman. (a) On axial CT images, focal peripheral ground-glass opacities with intralobular and interlobular smooth septal thickening were shown in the left (arrowhead) and right upper lobe (arrows). The right upper lobe lesions were accompanied by subpleural curvilinear lines (arrow). (b, c) Diffuse ground-glass (reticular) opacities with consolidation with bronchiectasis and bronchial wall thickening were demonstrated in the left and right lower lobes.
CT patterns were compared between asymptomatic and symptomatic cases who had positive lung parenchymal CT findings. The results are summarized in Table 3. Of 41 asymptomatic cases with lung opacities on CT, 17 (41%) cases had pure GGO, seven (17%) GGO with intra- and interlobular septal thickening without consolidation, and 17 (41%) GGO with consolidation. Of 22 symptomatic cases who had lung opacities on CT, five (23%) cases had pure GGO, four (18%) GGO with intra- and interlobular septal thickening and without consolidation, and 13 (59%) GGO with consolidation. In terms of the predominance of the lung parenchymal findings, asymptomatic cases showed GGO predominance over consolidation, while symptomatic cases were more likely to show consolidation predominance over GGO [asymptomatic vs symptomatic cases; GGO predominance: 34 (83%) vs 13 (59%); consolidation predominance: seven (17%) vs nine (41%), P = .038]. In terms of the number of lesions, asymptomatic cases had a single lesion in nine (22%) and more than two in 32 (78%) cases, compared to symptomatic cases, who had a single lesion in four (18%) and more than two in 18 (82%) cases. In terms of the axial distribution, more than half of the cases in each group showed a peripheral dominant distribution [24 (59%) asymptomatic vs 11 (50%) symptomatic cases]. On the other hand, only asymptomatic cases [four (10%) cases] showed a central dominant distribution with single or multiple rounded GGO in one or multiple lobes. Symptomatic cases were more likely to show a mixed distribution (coexisting peripheral and central distribution) than asymptomatic cases [11 (50%) symptomatic vs 13 (32%) asymptomatic cases]. In both groups, the lower lobes were the most frequently affected; left and right lower lobe involvement were present in 17 (77%) and 17 (77%) of symptomatic cases and in 29 (71%) and 29 (71%) of asymptomatic cases. In addition, more than two lung lobes were affected in more than 75% of cases and bilateral lungs in more than 80% in both clinical groups. The CT severity score was significantly higher in symptomatic cases than asymptomatic cases in the right and left lower lobes and overall lung [symptomatic vs asymptomatic cases; right lower lobe: 2 ± 1 (0–4) vs 1 ± 1 (0–4), P = .048; left lower lobe: 2 ± 1 (0–4) vs 1 ± 1 (0–3), P = .019; total lung score: 7 ± 5 (1–17) vs 4 ± 2 (1–11), P = .025.
Table 3:
Summary of CT Findings in Cases with Lung Opacities

Airway abnormalities included dilated bronchi in association with GGO or consolidation (ie, as “air bronchograms”), without airway secretions. Cavitation, thoracic lymphadenopathy and pleural effusion were not observed.
Discussion
In this study, we investigated the chest CT findings in laboratory-confirmed COVID-19 cases in an environmentally homogeneous cohort of cruise ship passengers and crew members, comparing the CT characteristics of asymptomatic and symptomatic cases. Although lung parenchymal and airway abnormalities were more frequent in symptomatically than asymptomatic cases, noticeably, we found lung parenchymal changes on CT in up to 54% of the asymptomatic cases. In those who showed CT abnormalities, asymptomatic cases showed significant predominance of GGO, while consolidation was predominant in symptomatic cases. Similarly, the CT severity score was significantly higher in symptomatic cases than asymptomatic cases in both lower lobes and on total lung assessment.
Although various CT findings were observed in cases with COVID-19, we found several common characteristic CT patterns, such as (a) single or multiple half-round or rectangular-shaped GGO in subpleural area with or without intra- or interlobular septal thickening (Fig 1), (b) single or multiple rounded GGO in both peribronchial and subpleural areas (Fig 2), (c) bilateral diffuse or multiple patchy GGO with or without intra- or interlobular septal thickening or consolidation in both peribronchial and subpleural areas, with a lower lobe predilection (Fig 3). Dilated bronchi were frequently associated with all of these CT patterns. These observations are mostly consistent with those of previous studies from China (9,13,15–19). All of the above-described characteristic CT patterns were found in both groups. However, differences were observed in the extension of the lung involvement as calculated by the mean CT severity score. The maximum total lung CT score was 11 in asymptomatic cases and 17 in symptomatic cases. In addition, the predominance of opacities also differed between the two groups; GGO was predominant in asymptomatic cases, whereas consolidation was predominant in symptomatic cases.
Figure 2a:
A 66-year-old asymptomatic woman. On axial CT images, focal rounded ground-glass opacities (arrows) with partial consolidation in a peribronchial and subpleural distribution were noted in the right upper (a), middle (b), and lower (c) lobes and left lower (b) lobe.
Some studies have reported clinical-radiologic dissociation in COVID-19 infection (20). For instance, several previous reports described asymptomatic cases who had evidence of lung opacities on chest CT (4,5,13). These observations have been confirmed by the results of the present study, highlighting the relative high prevalence of CT abnormalities even in asymptomatic cases. The presence of the subclinical CT findings in COVID-19 is an enigma. To the best of our knowledge, such cases with subclinical CT abnormalities have not been reported in either Middle East respiratory syndrome coronavirus (MERS-CoV) or severe acute respiratory syndrome (SARS-Cov) infection. Several hypotheses could explain this discrepancy. One possibility is that these cases have developed immunity against severe acute respirator syndrome coronavirus 2 (SARS-CoV-2) due to reinfection, leading to subclinical presentation. Such a case of relapse was reported from China and a suspected case of reinfection from Japan (21,22). Other possibilities are that such cases are still in the healing phase of COVID-19, and the symptoms may have already subsided by the time of admission and CT scan. However, the lack of typical characteristic of the healing stage of COVID-19 pneumonia have not been frequently observed (eg, perilobular pattern), weakening this hypothesis (9,19). Other possibilities include a discrepancy between the timing of CT positivity and clinical symptoms like in other types of pneumonia. The clinical-radiologic dissociation noted in many of COVID-19 cases in this cohort is a conundrum that still needs further investigation.
RT-PCR is currently considered the reference standard diagnostic method for COVID-19. However, the sensitivity of this method in throat swabs in COVID-19 is around 59% (23). To date, in several studies the sensitivity of chest CT has exceeded that of RT-PCR, and the authors emphasized the potential of chest CT as the primary screening tool for COVID-19 (23,24). The sensitivity of chest CT is unquestionable and encouraged for cases where there is need to determine the extension of disease and alternative diagnoses. The results of this study, however, do not directly allow the conclusion that all persons with positive RT-PCR findings should undergo chest CT for screening purposes. Before arriving at any such conclusion, the bioactivity and clinical impact of asymptomatic CT findings in COVID-19 infection will have to be investigated. One important issue is the need to distinguish the natural history of symptomatic and asymptomatic COVID-19 cases presenting with CT abnormalities, including the potential for infectivity and progression to acute severe respiratory distress. More appropriate use of CT screening will be possible when this information becomes available.
This study has various limitations. First, it included only adult cases. Second, because it included only passengers and crew members of a cruise ship, we acknowledge a selection bias. However, this environmentally homogeneous cohort enabled an investigation that eliminates other potential geographic confounders.
In conclusion, this study documented a high incidence of subclinical CT changes in COVID-19. Asymptomatic cases showed more GGO over consolidation and milder extension of lung parenchymal opacities. Further studies still are warranted to uncover the underlying mechanism responsible for the clinical-radiologic dissociation seen in some of asymptomatic COVID-19 cases, as well as to determine the impact of these findings on clinical decision-making.
Disclosures of Conflicts of Interest: S.I. disclosed no relevant relationships. A.F. disclosed no relevant relationships. M.J. disclosed no relevant relationships. N.K. disclosed no relevant relationships. S.W. disclosed no relevant relationships. Y.S. disclosed no relevant relationships. S.U. disclosed no relevant relationships. Y.U. disclosed no relevant relationships.
Abbreviations:
- COVID- 19
- coronavirus disease 19
- GGO
- ground-glass opacity
- RT-PCR
- reverse-transcription polymerase chain reaction
- WHO
- World Health Organization
References
- 1.World Health Organization . Naming the coronavirus disease (COVID-19) and the virus that causes it. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it. Accessed March 5, 2020.
- 2.Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020;395(10223):497–506 [Published correction appears in Lancet 2020;395(10223):496.]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.The Ministry of Health, Labour and Welfare . The infection control measures taken at the Cruise ship “Diamond Princess” (provisional translation). https://www.mhlw.go.jp/stf/seisakunitsuite/newpage_00001.html. Accessed March 5, 2020.
- 4.Shi H, Han X, Jiang N, et al. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study. Lancet Infect Dis 2020 Feb 24 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chung M, Bernheim A, Mei X, et al. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology 2020;295(1):202–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yu P, Zhu J, Zhang Z, Han Y, Huang L. A familial cluster of infection associated with the 2019 novel coronavirus indicating potential person-to-person transmission during the incubation period. J Infect Dis 2020 Feb 18 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rothe C, Schunk M, Sothmann P, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med 2020;382(10):970–971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bai Y, Yao L, Wei T, et al. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020 Feb 21 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pan F, Ye T, Sun P, et al. Time course of lung changes on chest CT during recovery from 2019 novel coronavirus (COVID-19) pneumonia. Radiology 2020 Feb 13:200370 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Koo HJ, Lim S, Choe J, Choi SH, Sung H, Do KH. Radiographic and CT features of viral pneumonia. RadioGraphics 2018;38(3):719–739. [DOI] [PubMed] [Google Scholar]
- 11.Hansell DM, Bankier AA, MacMahon H, McLoud TC, Müller NL, Remy J. Fleischner Society: glossary of terms for thoracic imaging. Radiology 2008;246(3):697–722. [DOI] [PubMed] [Google Scholar]
- 12.Chang YC, Yu CJ, Chang SC, et al. Pulmonary sequelae in convalescent patients after severe acute respiratory syndrome: evaluation with thin-section CT. Radiology 2005;236(3):1067–1075. [DOI] [PubMed] [Google Scholar]
- 13.Ng MY, Lee EY, Yang J, et al. Imaging profile of the COVID-19 infection: radiologic findings and literature review. Radiol Cardiothorac Imaging 2020;2(1):e200034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kanne JP. Chest CT findings in 2019 novel coronavirus (2019-nCoV) infections from Wuhan, China: key points for the radiologist. Radiology 2020;295(1):16–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bernheim A, Mei X, Huang M, et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020 Feb 20:200463 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zu ZY, Jiang MD, Xu PP, et al. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020 Feb 21:200490 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Song F, Shi N, Shan F, et al. Emerging 2019 Novel Coronavirus (2019-nCoV) Pneumonia. Radiology 2020;295(1):210–217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pan Y, Guan H, Zhou S, et al. Initial CT findings and temporal changes in patients with the novel coronavirus pneumonia (2019-nCoV): a study of 63 patients in Wuhan, China. Eur Radiol 2020 Feb 13 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kong W, Agarwal PP. Chest imaging appearance of COVID-19 infection. Radiol Cardiothorac Imaging 2020;2(1):e200028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet 2020;395(10223):514–523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chen D, Xu W, Lei Z, et al. Recurrence of positive SARS-CoV-2 RNA in COVID-19: A case report. Int J Infect Dis 2020 Mar 5 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Osaka Prefectural Government, Japan . About patient in conjunction with new coronavirus. http://www.pref.osaka.lg.jp.e.agb.hp.transer.com/hodo/index.php?site=fumin&pageId=37523. Accessed March 11, 2020. [Google Scholar]
- 23.Ai T, Yang Z, Hou H, et al. Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020 Feb 26:200642 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Fang Y, Zhang H, Xie J, et al. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020 Feb 19:200432 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]