

Abstract
Objective:
Having a strong sense of purpose in life is associated with positive health behaviors. However, the processes through which purpose leads to health are unclear. The current study compared neural responses in individuals with higher vs. lower purpose when making health-related decisions in response to messages encouraging health behavior change.
Methods:
220 adults with a sedentary lifestyle who were likely to feel conflicted in response to health messages underwent fMRI while viewing messages encouraging physical activity and indicated the self-relevance of the messages. We focused on activity within dorsal anterior cingulate cortex (dACC), anterior insula (AI), dorsolateral prefrontal cortex (DLPFC), and ventrolateral prefrontal cortex (VLPFC) as identified by meta-analytically defined maps of regions previously implicated in conflict-related processing, while participants considered the self-relevance of the messages.
Results:
Individuals with higher (vs. lower) purpose showed less activity in dACC, AI, DLPFC, and VLPFC while making health-decisions. Lower brain response in these regions mediated the effect of higher purpose on greater endorsement of the messages.
Conclusions:
Individuals with strong purpose may be less likely to experience conflict-related regulatory burden during health decision-making, which may in turn allow them to accept conflicting yet beneficial health messages. Reduced brain reactivity in dACC, AI, DLPFC, and VLPFC may reflect reduced conflict-related processing during health decision-making relevant to longer-term lifestyle goals. This adds to mounting evidence linking purpose and a range of positive health- related outcomes, as well as evidence suggesting that dACC, AI, DLPFC, and VLPFC track conflict-related processes relevant to longer-term goals and values.
Keywords: Purpose in life, conflict, health communication, physical activity, fMRI
Having a strong sense of purpose in life, or a set of goals derived from an individual’s core values, is associated with reduced risk of chronic conditions such as cognitive impairment (Lewis, Turiano, Payne, & Hill, 2017), stroke (Kim, Sun, Park, & Peterson, 2013; Yu et al., 2015), cardiovascular events (Cohen, Bavishi, & Rozanski, 2016), better physical and biologic functioning such as reduced allostatic load (Zilioli, Slatcher, Ong, & Gruenewald, 2015), enhanced glucoregulation (Hafez et al., 2018), and reduced risk of mortality (Boyle, Barnes, Buchman, & Bennett, 2009). Further, health benefits of having stronger purpose in life may be attributable to focused attention to and engagement in healthier behaviors. Supporting this view, stronger purpose in life is associated with greater likelihood of using preventative health services (Kim, Strecher, & Ryff, 2014), increased medication adherence (Musich, Wang, Kraemer, Hawkins, & Wicker, 2017), and more physical activity (Hooker & Masters, 2014). Together, previous studies support the health benefits of having strong purpose in life. Yet, the processes underlying the link between purpose and health relevant outcomes remain unclear. The current study tested whether people with a stronger sense of purpose in life might be more receptive to health messages, specifically focusing on physical activity behavior given its strong links to improved mental, physical, and behavioral health outcomes including reduced risk of several leadings causes of death (e.g., heart disease and cancer; Guilbert, 2003; Manley, 1996).
One key challenge to changing people’s health behaviors is the classic dilemma that those at highest risk for disease and most in need of change (e.g., increased physical activity), tend to be the most resistant to the idea of change when confronted with health messages (Resnicow & McMaster, 2012). People may resist self-relevant health messages due to conflicting motivations: On one hand, self-improvement motives can drive individuals to endorse the relevance of a helpful health message, and in turn choose to change a health risk behavior (Sedikides & Hepper, 2009). On the other, self-enhancement motives can make people feel defensive and deny the self-relevance of the health message because acknowledging one’s unhealthy behavior can threaten their sense of self-worth (Cohen & Sherman, 2014; Sherman & Cohen, 2006). Together, these competing motivations increase a person’s ambivalence and make decision-making processes more effortful. Unfortunately, those at highest risk are often most defensive (Sherman & Cohen, 2006). As such, we focused our investigation on sedentary individuals, a group likely to experience such threat in response to messages about physical activity.
This type of conflict often occurs quickly and people tend to resolve the conflict by adjusting their psychological views to be more consonant with a positive self-view (Steele, 1988). Further, defensiveness can push people to feign indifference even when they might be consciously aware of the conflicted feelings. For these reasons, health-message induced decisional conflicts are often difficult for people to consciously detect and report accurately. In addition, self-reports require people to retrospectively reflect on the message during exposure, but report after the exposure has occurred, when psychological processes such as defensiveness have already altered cognitions. For these reasons, we used functional magnetic resonance imaging (fMRI) to capture message-induced processes in real-time that might be otherwise difficult to assess with self-reports.
Past health decision-making studies have shown that reduced conflict in decision-making can lead to positive outcomes, such as a better emotional experience (Knops et al., 2013; O’Connor & Jacobsen, 2007; O’Connor, Jacobsen, & Stacey, 2002; Stacey et al., 2011), less regret about decisions (Brehaut et al., 2003; Hu et al., 2008), and less delay in making decisions (O’Connor & Jacobsen, 2007). Importantly, decreased conflict predicted greater likelihood of adherence to health regimens (Graham, Haworth, Chorney, Bance, & Hong, 2015), suggesting a greater openness to change.
Decisional conflict arises in part when people are unclear about their core values and goals (e.g., Decisional Conflict Scale; O’Connor, 1995). By contrast, one’s purpose in life is a function of goals associated with core values, providing clearer direction in an environment replete with choices and resulting conflict (Hill, Edmonds, Peterson, Luyckx, & Andrews, 2016; Kashdan & McKnight, 2013; McKnight & Kashdan, 2009). Goal clarification is considered a key initial step in decision-making (Brown, 2012; Mann, Harmoni, & Power, 1991). Thus, people with a higher sense of purpose may experience less decisional conflict from messages encouraging longer-term lifestyle changes in the domain of personally-relevant behaviors.
If stronger purpose in life is associated with reduced decisional conflict, then it therefore follows that purpose should be associated with reduced conflict-related neural activity during health decision-making relevant to longer-term lifestyle changes. Conflict-related neural processing involves activity in multiple brain regions, and our focal ROIs are often active in decision-making contexts (Sanfey, Rilling, Aronson, Nystrom, & Cohen, 2003), likely indexing multiple psychological processes. Key regions include dorsal anterior cingulate cortex (dACC) previously associated with conflict-specific monitoring (Botvinick, Nystrom, Fissell, Carter, & Cohen, 1999), anterior insula (AI), previously associated with arousing emotional states while experiencing conflicts (Harlé, Chang, van ‘t Wout, & Sanfey, 2012), dorsolateral prefrontal cortex (DLPFC), associated with maintenance of cognitive demands during conflictive states (MacDonald, Cohen, Stenger, & Carter, 2000), and ventrolateral prefrontal cortex (VLPFC), associated with conflict-driven cognitive control (Egner, 2011).
Activity in dACC, AI, and DLPFC has been deeply studied in the context of immediate conflict in behavioral response during cognitive tasks (Nee, Wager, & Jonides, 2007). However, these regions are also implicated in longer-term conflict processing, such as when dealing with conflicting information in relation to the self (Bush, Luu, & Posner, 2000), reappraising self-relevant items (Giuliani, Mann, Tomiyama, & Berkman, 2014), and biased self-processing (Kircher et al., 2000). Therefore, activity in these regions may also represent conflict processing in relation to the self, and/or more generally, longer-term conflict processing relevant to lifestyle goals and changes. Together, increased activity in these regions is associated with cognitive effort (Botvinick, Braver, Barch, Carter, & Cohen, 2001), consistent with the idea that conflicts may interfere with the ease of message acceptance.
A second possibility is that purpose does not alter conflict, but rather directly alters anticipated neural signals associated with other forms of self-relevance judgments and positive valuation when making health related decisions. If purpose operates through these pathways, then one would expect to see greater activity within the medial prefrontal cortex (MPFC) and posterior cingulate cortex (PCC), previously associated with self-relevance (Murray, Schaer, & Debbané, 2012) (SI 2), and ventromedial prefrontal cortex (VMPFC) and ventral striatum (VS), previously associated with reward/positive valuation (Bartra, McGuire, & Kable, 2013), rather than within our focal ROIs in dACC, AI, DLPFC, and VLPFC.
In this study, participants were exposed to self-relevant health messages to test whether a stronger sense of purpose in life was associated with an increased likelihood of endorsing the health messages, and to examine the neural pathways supporting these effects. To this end, we examined the relationship between purpose in life and neural activity during exposure to health messages. Finding evidence for decreased brain activity within dACC, AI, DLPFC, and VLPFC, which have been robustly associated with conflict, an additional analysis tested if these brain responses mediated the association between higher purpose and increased endorsement of health messages.
Method
Participants
We recruited sedentary and obese/overweight adults for whom health advice about physical activity is most self-relevant and likely to trigger feelings of conflict (n=220; mean age=33.75 years, SD=11.62; 144 females; 96 Black, 86 White, 16 Asians, 9 Hispanic, 13 Other; mean years of education=15.88 years, SD=2.97).1 Participants responded to an online advertisement and flyers for a study on “daily activities” to avoid selection bias related to individual health status. Eligibility criteria included engagement in less than 200 minutes of walking, moderate, and vigorous physical activity throughout the seven days prior to the screening using a short form International Physical Activity Questionnaire (IPAQ), 2) a body mass index (BMI) over 25, derived from self-reported weight and height, standard fMRI scanning criteria (no metal in body, not claustrophobic, not pregnant/nursing, right-handed), no current use of illicit drugs or psychotropic medications, and no history of serious psychiatric/medical conditions. Participants with usable data were included in final message rating outcome analyses (n=204), neural outcome analyses (n=177), and analyses linking neural and message rating outcomes (n=176). The study was approved by the University of Pennsylvania Institutional Review Board.
Procedure
Participants visited the laboratory for the baseline appointment and an fMRI appointment approximately 10 days later (M=9.60 days, SD=5.00). At baseline, all participants provided informed consent and self-reported their level of purpose in life. During the following fMRI appointment, participants were presented with a series of health messages encouraging health behavior change.2 All measures were embedded among other tasks and surveys not reported here. Self-reports were collected using an online survey tool (Qualtrics), and scanner tasks were presented using PsychoPy2 (Peirce, 2007).
Measures and tasks
Purpose in life.
Individual differences in purpose in life were measured by a modified seven-item version of the Psychological Well-Being Scales (Ryff, 1989) that showed reliability and validity in nationally representative samples (Abbott et al., 2006; Ryff, 2014). Participants rated the degree to which they agreed with statements such as “I have a sense of direction and purpose in life,” rated on a 1 (strongly disagree) to 6 (strongly agree) scale. Scores were averaged across seven items, with higher scores reflecting a greater sense of having purpose in life (Cronbach α =.79).
Health messages fMRI task.
During the fMRI appointment, participants completed the health messages task in which they viewed and listened to 30 messages that suggested various reasons and strategies to increase physical activity. The effects of purpose on responses to three different categories of messaging were tested, including: 1) messages highlighting risks associated with being sedentary (10 risk messages; e.g., “Sedentary people like you are at serious risk for heart disease.”), 2) reasons to become more active (10 why messages; e.g., “You can lower your risk of getting cancer if you start to exercise regularly.”), and 3) strategies to become more active (10 how messages; e.g., “Make a habit of walking up and down the stairs whenever you can.”). As within-subjects contrasts to facilitate fMRI analysis, three sub categories of 30 control messages paralleled the health message subcategories, including messages highlighting risks (n=10), reasons (n=10), and strategies (n=10) regarding other daily behaviors unrelated to physical activity. Two runs (15 health and 15 control messages in each run) were presented in a randomized order, containing trials consisting of a health/control message (8s) and a self-relevance rating (4s). Each trial was separated by a fixation rest period (3s); every fifth trial was separated by a a longer (10s) period of rest. Message texts were accompanied by a simple pictogram and audio of the text to control for reading speed. All message types were controlled for reading levels using the Simple Measure of Gobbledygook (SMOG) grade and argument strength. The stimuli and detailed instructions for the health messages fMRI task can be downloaded from https://github.com/cnlab/purpose/tree/master/health%20messages%20task. Data relevant to the central analyses can be found on https://github.com/cnlab/purpose/tree/master/data.
Health messages endorsement.
Outside the scanner, participants were presented with the same messages they saw during the health messages fMRI task, and rated the degree to which they agreed with each message (agree ratings) and felt confident that they could do what the message was recommending (confidence ratings) using a scale ranging from 1 (strongly disagree) to 5 (strongly agree). The agree and confidence ratings within each message type category were highly correlated (rmean=.60, ps<.0001) and were combined to create mean message endorsement scores (see supplemental information [SI] 1 for results of each endorsement type).
Demographics.
At the end of the baseline visit, participants self-reported their age, sex, ethnicity, and years of education. The ethnicity variable was converted into a binary variable indicating Black (the majority of the current sample) vs. non-Black status. Purpose in life was significantly associated with ethnicity, such that Blacks reported higher purpose than non-Blacks (r=.207, p=.002). Therefore, ethnicity was controlled for in all analyses. Purpose was not associated with age, sex, or education (ps>.10).
Analysis Plan
Separate regression analyses tested the links between purpose in life, neural activity within our focal ROIs including dACC, AI, DLPFC, and VLPFC (chosen for their roles in conflict and reward using neurosynth.org), and health message endorsement. Further, we also analyzed other potentially relevant ROIs associated with reward, self-relevance, salience, and executive processing (SI 2, 3). First, the association between purpose in life and health message endorsement was tested. Second, the associations between purpose in life and neural activity in key ROIs, while considering the self-relevance of the health messages, were tested. Finally, given evidence that purpose in life was associated with decreased activity within the maps of regions implicated in conflict-related processing including dACC, AI, DLPFC, and VLPFC, the indirect effect of purpose in life on increased message endorsement through reduced neural responses in these regions was tested.
The coefficient of determination (R2, R2adjusted), beta coefficients (β), and 95% confidence intervals (CI) are reported. All reported p values are two-tailed. All analyses were performed in R (v3.0.1, www.r-project.org) using the R-studio interface (v0.98.1103).
fMRI data acquisition, preprocessing, and modeling.
The imaging data were acquired on 3 Tesla Siemens Trio scanners equipped with a 32 or 64 channel head coil. The head coil type was not associated with any of the neural outcomes (ps>.10). Participants were self-guided through two runs of the health messages task (run1=376, run2=344 volumes, 720 volumes total), and one run of the self localizer task (308 volumes) (SI 2).
High-resolution T1-weighted structural images were collected using an MPRAGE sequence (TI=1,100ms, 160 slices, slice thickness=1mm, voxel size=0.9 × 0.9 × 1). T2*- weighted functional images were recorded (repetition time=1,500ms, echo time=25ms, flip angle=70°, −30° tilt relative to AC-PC line, 54 slices, field of view=200mm, slice thickness=3mm, multiband acceleration factor=2, voxel size=3.0 × 3.0 × 3.0 mm).
The anatomical and functional data were acquired and preprocessed using a standard processing stream using Statistical Parametric Mapping (SPM8; Wellcome Department of Cognitive Neurology, Institute of Neurology, London, UK) for all stages apart from the initial despiking, which was carried out using the 3dDespike program as implemented in the AFNI toolbox. Differences in time of acquisition were corrected using a sinc interpolation algorithm with the first slice as reference. Data were spatially realigned to the first slice of each volume, and co-registered to functional and structural images using two six-parameter affine stages. The mean image across all blood oxygen level-dependent (BOLD) functional images was registered to high-resolution T1 images (total of 12 parameter affine). Following co-registration, the high-resolution T1 images were segmented into gray matter, white matter and cerebrospinal fluid to create a brain mask used to determine voxels to be included in first and second-level models. Structural and functional images were then normalized to the skull-stripped MNI template (“MNI152_T1_1mm_brain.nii”) from the FMRIB Software Library (FSL). In the final preprocessing step, the functional images were smoothed using a Gaussian kernel (8-mm FWHM). To allow for the stabilization of the BOLD signal, the first five volumes (7.5s) of each run were discarded before analysis. Movement parameters (six rigid-body parameters, three for translation and three for rotation) derived from spatial realignment were included as nuisance regressors in all first-level models. Data were high pass filtered with a cutoff of 128s.
The health messages task was modeled including regressors for each message type (risk messages about health, why to be less sedentary and more active, how to be less sedentary and more active, risk messages about other daily activities, why to perform other daily activities, how to perform other daily activities) and the corresponding response periods. Parameter estimates of activity during the response periods (i.e., self-relevance ratings) of 30 health messages were compared with the response periods of 30 everyday activity control messages for each person within subjects using MarsBaR (Brett, Anton, Valabregue, & Poline, 2002), and converted to percent signal change. Second-level random-effects models were constructed by averaging across participants and were submitted to a further ROI analysis described below.
ROI analysis.
A functionally defined map of conflict-related activity was extracted from the online database Neurosynth (www.neurosynth.org) (Yarkoni, Poldrack, Nichols, Van Essen, & Wager, 2011). Neurosynth automatically synthesizes published fMRI data (413,429 activations reported in 11,406 studies as of February 2018). Using meta-analytic procedures, Neurosynth allows the users to search common activation patterns during psychological states with representational search terms. Our primary ROIs were derived from the search term ‘conflict’ (273 studies; using Neurosynth’s default threshold p<.01, corrected). This map included activity in the dACC, bilateral AI, right DLPFC, right VLPFC, ACC, and PCC associated with conflict processing for reverse inferences (Figure 1A). A ‘reverse inference map’ was also derived from the search term ‘reward’ (671 studies; using Neurosynth’s default threshold p<.01, corrected), which included VS, VMPFC, and ventral tegmental area (Figure 1B).
Figure1.
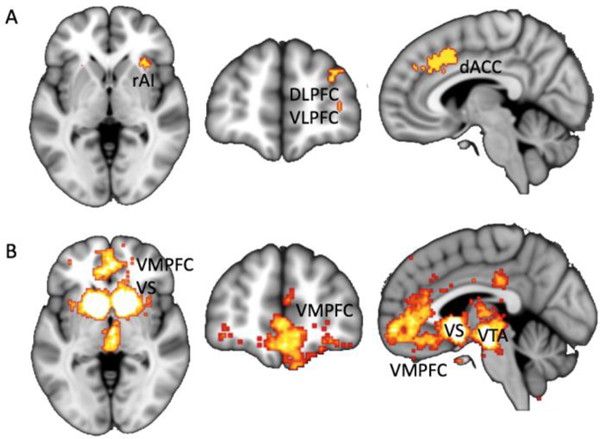
Neurosynth reverse inference maps of the terms A. ‘conflict’ and B. ‘reward’, extracted from neurosynth.org (p<.01, corrected). Note: dACC = dorsal anterior cingulate cortex; DLPFC = dorsolateral prefrontal cortex; rAI = right anterior insula; VLPFC = ventrolateral prefrontal cortex; VMPFC = ventromedial prefrontal cortex; VS = ventral striatum; VTA = ventral tegmental area.
In addition to the primary a priori ROI analyses, exploratory whole-brain analyses were done for regions associated with purpose in life. Whole-brain analyses of neural activity during health messages task across message types (SI 5, 6) and regions associated with purpose (SI 7, 8) are reported in supplementary information.
Results
Effects of Purpose in Life on Health Message Endorsement
The first analysis tested whether individual differences in purpose in life were associated with the likelihood of endorsing the health messages following message exposure. As noted above, given that Black and non-Black participants showed different levels of purpose in life, race was controlled for in all analyses. Regression analyses revealed that participants with a higher (vs. lower) sense of purpose were more likely to endorse the self-relevance of the how messages that suggested specific ways for the participant to become more active (R2=.058, R2adjusted=.049, β=.201, t(201)=2.869, p=.005, 95% CI [.032, .174]), as well as why messages that explained why one should become more active and less sedentary (R2=.034, R2adjusted=.024, β=.140, t(201)=1.972, p=.050, 95% CI [0, .151]). However, purpose was not associated with risk message ratings that highlighted the risk of staying sedentary (R2=.005, R2adjusted=−.005, β=.065, t(202)=.902, p=368).
Effects of Purpose in Life on Neural Activity during Health Message Exposure
Next, the link between purpose and brain responses within dACC, AI, DLPFC, and VLPFC, identified using the meta-analytically defined (i.e., Neurosynth) conflict mask, while considering the self-relevance of health messages was tested. Brain activity during the three health message types (how, why, risk), compared to corresponding control message types, were used as an outcome variable in three separate regression models.
Higher (vs. lower) purpose in life was associated with attenuated activity within the mask while viewing the how health messages compared to how control messages (R2=.026, R2adjusted=.015, β=−.164, t(174)=−2.138, p=.034, 95% CI [−.032 −.001]), with particularly robust effects in dACC, right AI, right DLPFC, and right VLPFC (SI 3, 4). However, purpose was not associated with activity within these regions while viewing the why (p=.474) or risk messages (p=.552).
Additional analyses tested whether purpose was related to neural responses within VS and VMPFC (defined based on a Neurosynth search associated with the term “reward”), or other regions chosen for their roles in self-related processes, salience, and executive processing, when considering the self-relevance of health messages. Purpose in life was not associated with brain activity in any of these additional brain ROIs (ps>.50; SI 3, 4).
Neural Activity Mediating the Purpose Effects on Message Endorsement
Finally, an indirect effect model was tested whereby the effect of purpose on increased health message endorsement is mediated by lower activity in dACC, AI, DLPFC, and VLPFC while considering the self-relevance of messages, using bootstrapping (Preacher & Hayes, 2008). Based on significant links between purpose in life and how message ratings of self-relevance, and neural activity during exposure to how messages, analyses focused on ratings and neural activity associated with how health messages. Results from the bootstrapped estimates of the indirect effect showed a significant indirect effect of purpose on increased endorsement of health messages through decreased neural activity in brain regions identified using the neurosynth ‘conflict’ map during health message exposure (bias-corrected confidence intervals: .0006 to .0360 which does not contain 0).
Discussion
Purpose in life is associated with positive health outcomes, however, the processes through which purpose promotes health have been unclear. Kashdan and McKnight (2014) suggest that, “A person with a clearly defined purpose ought to... have less difficulty deciding between competing options when reflecting on her purpose.” The current study supports this cognitive account for the link between purpose and health: Making healthy decisions might be less conflicting, and hence less effortful, for people with a stronger sense of purpose in life, compared to those with vague or no sense of values or direction.
The current study found that people with greater (vs. lower) purpose showed less activity in a set of brain regions including dACC, AI, DLPFC, and VLPFC, chosen for their role in conflict processing during health decision-making, which in turn predicted greater endorsement of self-relevant health advice.
Adhering to a healthy lifestyle requires the ability to consistently make choices in the midst of conflicting and competing options. Individuals with strong life purpose may experience less conflict when deciding to, for example, get their cholesterol level checked (Kim et al., 2014) or start exercising (Hooker & Masters, 2014). Further, dealing with conflicting information in relation to the self is a specific from of self processing that implicates some of the key ROIs we focused on (e.g., dACC; Bush et al., 2000). Although the current neural data cannot directly identify the source of the conflict, self-relevance might reduce conflict by biasing attention during decision-making that involves conflicting choices.
Health messages are often generally categorized into why to engage in a health action, and how to engage in a health action (suggesting various strategies one could use). In the current study, the effect of purpose in life was strongest when participants were exposed to how messages. One possibility is that how messages may be more concretely tied to decision-making processes and hence the experience of decisional conflict most relevant to purpose. It may also be the case that how messages are most concretely relevant to enacting a broader purpose (e.g., to stay healthy in order to help friends and family). By contrast, people with a high vs. low sense of purpose may be less affected by suggestions about why a person needs to be more active, because they already have a “why” for their actions, and new reasons why may be orthogonal to each individual’s specific life purpose. Consistent with Friedrich Nietzsche’s assertion that “He who has a why to live can bear almost any how.” (Frankl, 1963), it is possible that participants who have stronger purpose in life are more open to suggestions for how to live a longer and healthier life. In other words, the broader “why” provided by life purpose, may provide intrinsic motivation and openness to accept skill- and information-based “how” messages, even if the specific messages themselves are not seen as subjectively rewarding (no differences were detected within brain regions such as VS and VMPFC, and MPFC and PCC, chosen for their roles in reward and self-relevance respectively, according to purpose in life). Therapeutic approaches such as Motivational Interviewing and Acceptance and Commitment Therapy are consistent with this perspective (Resnicow et al., 2002). In other words, our results are most consistent with the idea that greater purpose may reduce self-related conflicts or negative responses to messaging; dACC has been associated with dealing with conflicting information in relation to the self (Bush et al., 2000), DLPFC with reappraising self-relevant items (Giuliani et al., 2014), and AI with biased self-processing (Kircher et al., 2000). Purpose may help alleviate these types of reactions, and in turn facilitate positive outcomes. Related to this point, these findings are broadly consistent with past research showing a reduction in ACC activity among people with more (vs. less) religious conviction when administered a Stroop task (Inzlicht, McGregor, Hirsh, & Nash, 2009). Religiosity also has been associated with greater purpose in life across religions, gender, nationality, and race (Rizvi & Hossain, 2017). The current findings extend this work, by suggesting that activity in dACC, AI, DLPFC, and VLPFC tracks conflict processing relevant to longer-term life goals and values beyond more immediate behavioral conflict. Experiencing conflict often accompanies negative feelings such as emotional discomfort and pain (Jehn & Mannix, 2001). Therefore, reduced conflict-related pain could result in extra cognitive resources needed to focus and persevere through emotional and physical challenges. Consistent with this idea, the primary neural conflict regions evaluated in this study included the dACC and AI, that are also implicated under different circumstances in processing emotional (Eisenberger, Lieberman, & Williams, 2003) and physical pain (Wager et al., 2013). Having strong purpose in life can help manage physical pain experienced during post-knee surgery recovery (Smith & Zautra, 2004) and heat or cold habituation (Smith et al., 2009). Thus, future studies may explicitly test the link between purpose in life and pain in various health-related contexts (e.g., craving in addiction, end-of-life care, etc.).
This study should be interpreted in the context of limitations inherent in the study design. Primarily, psychological processes inferred from neuroimaging data should be interpreted with caution. As with all correlational neuroimaging studies, the neural ROIs in the current study are also associated with other psychological processes in addition to conflict. For example, activity in the regions defined by the neurosynth ‘conflict map’ are relevant to multiple processes that may or may not overlap with conflict-related processing. In particular, dACC activity is associated with several processes closely related, yet distinct, to conflict, such as error detection and aversiveness/pain (Wager et al., 2016). Future studies could also compare the types of measures we collected in this study to assess psychological conflict more directly. Further, given the correlational nature of this study, the direction of causality cannot be inferred as to whether purpose in life reduced conflict-related neural responses, or whether people who are more likely to show such responses have an easier time developing purpose in life. To test the causal link between purpose and reduced conflict processing in health decision-making, future research could experimentally manipulate purpose in life prior to health message exposure using interventions previously shown to increase state-level purpose (Burrow & Hill, 2013; Robatmili et al., 2015; Shin & Steger, 2014; van der Spek et al., 2014). Finally, various types of health messages used in this study (i.e., how, why, risk) parallel what would be seen in real life health communication contexts (e.g., from the media, a doctor, friends, etc.). However, the current study was not designed to examine the effects of purpose across different message types that may require different levels of explanation. Future studies may specifically test the effects of purpose on between-subjects exposure to different message types.
Nonetheless, the current findings provide novel evidence for a potential path linking purpose to health-relevant outcomes. Our findings suggest that individuals with higher purpose are less likely to show increased brain activity in regions chosen for their role in conflict processing during health decision-making, which may allow them to accept and internalize health advice. More generally, our findings are consistent with the idea that in addition to immediate cognitive conflicts, dACC, AI, DLPFC, and VLPFC also track conflict-related processes relevant to long-term life goals and values. Provided that public health and healthcare professional often have difficulties persuading adults to enhance their health behaviors, future health intervention studies may consider testing strategies to boost one’s sense of purpose in order to identify causal links between purpose and increased receptivity to health advice that can otherwise trigger decisional conflicts. If successful, purpose-based health messaging interventions may provide new avenues for health behavior change.
Supplementary Material
Acknowledgments
We thank Alison Elliott, Elizabeth Beard, and Katherine Wu for research assistance. Dr. Strecher, one of the co-authors, is Founder and CEO of JOOL Health, a digital well-being company. This research was supported by NIH/National Cancer Institute Grant 1R01CA180015–01 (PI: E.B.F.), NIH New Innovator Award 1DP2DA03515601 (PI: E.B.F.), the U.S. Army Research Laboratory including work under Cooperative Agreement Number W911NF-10–2-0022 (PI: E.B.F.), and HopeLab (PI: Y.K, E.B.F.). E.K. gratefully acknowledges support from (PI: E.K.; NIH/ K99AG055696). The content is solely the responsibility of the authors and does not represent the views of the funding agencies.
Footnotes
The rest of authors declare no conflict of interest.
This study was a part of a larger investigation that focused on the orthogonal question of self-transcendence effects on health behavior change (Kang et al., 2018). Kang et al. focused on experimentally manipulating self-transcendent orientations, and the current results remained parallel controlling for the self-transcendence manipulations. No prior report examined individual differences in purpose in life using this dataset.
Participants also completed an end-point visit approximately one month after the fMRI appointment that is not the focus of the current report (Kang et al., 2018).
References
- Abbott RA, Ploubidis GB, Huppert FA, Kuh D, Wadsworth MEJ, & Croudace TJ (2006). Psychometric evaluation and predictive validity of Ryff’s psychological well-being items in a UK birth cohort sample of women. Health and Quality of Life Outcomes, 4, 76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bartra O, McGuire JT, & Kable JW (2013). The valuation system: a coordinate-based meta-analysis of BOLD fMRI experiments examining neural correlates of subjective value. NeuroImage, 76, 412–427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Botvinick MM, Braver TS, Barch DM, Carter CS, & Cohen JD (2001). Conflict monitoring and cognitive control. Psychological Review, 108(3), 624–652. [DOI] [PubMed] [Google Scholar]
- Botvinick M, Nystrom LE, Fissell K, Carter CS, & Cohen JD (1999). Conflict monitoring versus selection-for-action in anterior cingulate cortex. Nature, 402(6758), 179–181. [DOI] [PubMed] [Google Scholar]
- Boyle PA, Barnes LL, Buchman AS, & Bennett DA (2009). Purpose in life is associated with mortality among community-dwelling older persons. Psychosomatic Medicine, 71(5), 574–579. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brehaut JC, O’Connor AM, Wood TJ, Hack TF, Siminoff L, Gordon E, & FeldmanStewart D (2003). Validation of a decision regret scale. Medical Decision Making: An International Journal of the Society for Medical Decision Making, 23(4), 281–292. [DOI] [PubMed] [Google Scholar]
- Brett M, Anton J-L, Valabregue R, & Poline J-B (2002). Region of interest analysis using the MarsBar toolbox for SPM 99. NeuroImage, 16(2), S497. [Google Scholar]
- Brown P (2012). Career coach: decision-making. Pulse, Retrieved July, 12. [Google Scholar]
- Burrow AL, & Hill PL (2013). Derailed by diversity? Purpose buffers the relationship between ethnic composition on trains and passenger negative mood. Personality & Social Psychology Bulletin, 39(12), 1610–1619. [DOI] [PubMed] [Google Scholar]
- Bush G, Luu P, & Posner MI (2000). Cognitive and emotional influences in anterior cingulate cortex. Trends in Cognitive Sciences, 4(6), 215–222. [DOI] [PubMed] [Google Scholar]
- Cohen GL, & Sherman DK (2014). The psychology of change: self-affirmation and social psychological intervention. Annual Review of Psychology, 65, 333–371. [DOI] [PubMed] [Google Scholar]
- Cohen R, Bavishi C, & Rozanski A (2016). Purpose in Life and Its Relationship to All-Cause Mortality and Cardiovascular Events: A Meta-Analysis. Psychosomatic Medicine, 78(2), 122–133. [DOI] [PubMed] [Google Scholar]
- Egner T (2011). Right ventrolateral prefrontal cortex mediates individual differences in conflict-driven cognitive control. Journal of Cognitive Neuroscience, 23(12), 3903–3913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberger NI, Lieberman MD, & Williams KD (2003). Does rejection hurt? An FMRI study of social exclusion. Science, 302(5643), 290–292. [DOI] [PubMed] [Google Scholar]
- Frankl VE (1963). Man’ s search for meaning. I. Lasch. Trans. New York: Pocketbooks (original Work Published 1946; ). [Google Scholar]
- Giuliani NR, Mann T, Tomiyama AJ, & Berkman ET (2014). Neural systems underlying the reappraisal of personally craved foods. Journal of Cognitive Neuroscience, 26(7), 1390–1402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham ME, Haworth R, Chorney J, Bance M, & Hong P (2015). Decisional Conflict in Parents Considering Bone-Anchored Hearing Devices in Children With Unilateral Aural Atresia. The Annals of Otology, Rhinology, and Laryngology, 124(12), 925–930. [DOI] [PubMed] [Google Scholar]
- Guilbert JJ (2003). The world health report 2002 - reducing risks, promoting healthy life. Education for Health, 16(2), 230. [DOI] [PubMed] [Google Scholar]
- Hafez D, Heisler M, Choi H, Ankuda CK, Winkelman T, & Kullgren JT (2018). Association Between Purpose in Life and Glucose Control Among Older Adults. Annals of Behavioral Medicine: A Publication of the Society of Behavioral Medicine, 52(4), 309–318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harlé KM, Chang LJ, van ‘t Wout M, & Sanfey AG (2012). The neural mechanisms of affect infusion in social economic decision-making: a mediating role of the anterior insula. NeuroImage, 61(1), 32–40. [DOI] [PubMed] [Google Scholar]
- Hill PL, Edmonds GW, Peterson M, Luyckx K, & Andrews JA (2016). Purpose in Life in Emerging Adulthood: Development and Validation of a New Brief Measure. The Journal of Positive Psychology, 11(3), 237–245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hooker SA, & Masters KS (2014). Purpose in life is associated with physical activity measured by accelerometer. Journal of Health Psychology, 21(6), 962–971. [DOI] [PubMed] [Google Scholar]
- Hu JC, Kwan L, Krupski TL, Anger JT, Maliski SL, Connor S, & Litwin MS (2008). Determinants of treatment regret in low-income, uninsured men with prostate cancer. Urology, 72(6), 1274–1279. [DOI] [PubMed] [Google Scholar]
- Inzlicht M, McGregor I, Hirsh JB, & Nash K (2009). Neural markers of religious conviction. Psychological Science, 20(3), 385–392. [DOI] [PubMed] [Google Scholar]
- Jehn KA, & Mannix EA (2001). The Dynamic Nature of Conflict: A Longitudinal Study of Intragroup Conflict and Group Performance. Academy of Management Journal. Academy of Management, 44(2), 238–251. [Google Scholar]
- Kang Y, Cooper N, Pandey P, Scholz C, O’Donnell MB, Lieberman MD, ... Falk EB (2018). Effects of self-transcendence on neural responses to persuasive messages and health behavior change. Proceedings of the National Academy of Sciences of the United States of America, 115(40), 9974–9979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kashdan TB, & McKnight PE (2013). Commitment to a purpose in life: an antidote to the suffering by individuals with social anxiety disorder. Emotion, 13(6), 1150–1159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim ES, Strecher VJ, & Ryff CD (2014). Purpose in life and use of preventive health care services. Proceedings of the National Academy of Sciences of the United States of America, 111(46), 16331–16336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim ES, Sun JK, Park N, & Peterson C (2013). Purpose in life and reduced incidence of stroke in older adults: “The Health and Retirement Study.” Journal of Psychosomatic Research, 74(5), 427–432. [DOI] [PubMed] [Google Scholar]
- Kircher TT, Senior C, Phillips ML, Benson PJ, Bullmore ET, Brammer M, ... David AS (2000). Towards a functional neuroanatomy of self processing: effects of faces and words. Brain Research. Cognitive Brain Research, 10(1–2), 133–144. [DOI] [PubMed] [Google Scholar]
- Knops AM, Goossens A, Ubbink DT, Legemate DA, Stalpers LJ, & Bossuyt PM (2013). Interpreting patient decisional conflict scores: behavior and emotions in decisions about treatment. Medical Decision Making: An International Journal of the Society for Medical Decision Making, 33(1), 78–84. [DOI] [PubMed] [Google Scholar]
- Lewis NA, Turiano NA, Payne BR, & Hill PL (2017). Purpose in life and cognitive functioning in adulthood. Neuropsychology, Development, and Cognition. Section B, Aging, Neuropsychology and Cognition, 24(6), 662–671. [DOI] [PubMed] [Google Scholar]
- MacDonald AW 3rd, Cohen JD, Stenger VA, & Carter CS (2000). Dissociating the role of the dorsolateral prefrontal and anterior cingulate cortex in cognitive control. Science, 288(5472), 1835–1838. [DOI] [PubMed] [Google Scholar]
- Manley AF (1996). Physical Activity And Health: A Report Of The Surgeon General. DIANE Publishing. [Google Scholar]
- Mann L, Harmoni R, & Power C (1991). The GOFER course in decision making. Teaching Decision Making to Adolescents, 61–78. [Google Scholar]
- McKnight PE, & Kashdan TB (2009). Purpose in life as a system that creates and sustains health and well-being: an integrative, testable theory. Review of General Psychology: Journal of Division 1, of the American Psychological Association, 13(3), 242. [Google Scholar]
- Murray RJ, Schaer M, & Debbane M (2012). Degrees of separation: a quantitative neuroimaging meta-analysis investigating self-specificity and shared neural activation between self- and other-reflection. Neuroscience and Biobehavioral Reviews, 36(3), 1043–1059. [DOI] [PubMed] [Google Scholar]
- Musich S, Wang SS, Kraemer S, Hawkins K, & Wicker E (2017). Purpose in Life and Positive Health Outcomes Among Older Adults. Population Health Management 10.1089/pop.2017.0063 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nee DE, Wager TD, & Jonides J (2007). Interference resolution: Insights from a meta-analysis of neuroimaging tasks. Cognitive, Affective & Behavioral Neuroscience, 7(1), 1–17. [DOI] [PubMed] [Google Scholar]
- O’Connor AM (1995). Validation of a decisional conflict scale. Medical Decision Making: An International Journal of the Society for Medical Decision Making, 15(1), 25–30. [DOI] [PubMed] [Google Scholar]
- O’Connor AM, & Jacobsen MJ (2007). Decisional conflict: Supporting people experiencing uncertainty about options affecting their health. Ottawa: Ottawa Health Decision Centre. [Google Scholar]
- O’Connor AM, Jacobsen MJ, & Stacey D (2002). An evidence-based approach to managing women’s decisional conflict. Journal of Obstetric, Gynecologic & Neonatal Nursing, 31(5), 570–581. [DOI] [PubMed] [Google Scholar]
- Peirce JW (2007). PsychoPy—Psychophysics software in Python. Journal of Neuroscience Methods, 162(1), 8–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preacher KJ, & Hayes AF (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891. [DOI] [PubMed] [Google Scholar]
- Resnicow K, Dilorio C, Soet JE, Ernst D, Borrelli B, & Hecht J (2002). Motivational interviewing in health promotion: it sounds like something is changing. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 21(5), 444–451. [PubMed] [Google Scholar]
- Resnicow K, & McMaster F (2012). Motivational Interviewing: moving from why to how with autonomy support. The International Journal of Behavioral Nutrition and Physical Activity, 9, 19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rizvi MAK, & Hossain MZ (2017). Relationship Between Religious Belief and Happiness: A Systematic Literature Review. Journal of Religion and Health, 56(5), 1561–1582. [DOI] [PubMed] [Google Scholar]
- Robatmili S, Sohrabi F, Shahrak MA, Talepasand S, Nokani M, & Hasani M (2015). The Effect of Group Logotherapy on Meaning in Life and Depression Levels of Iranian Students. International Journal for the Advancement of Counseling, 37(1), 54–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryff CD (1989). Happiness is everything, or is it? Explorations on the meaning of psychological well-being. Journal of Personality and Social Psychology, 57(6), 1069. [Google Scholar]
- Ryff CD (2014). Psychological well-being revisited: advances in the science and practice of eudaimonia. Psychotherapy and Psychosomatics, 53(1), 10–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanfey AG, Rilling JK, Aronson JA, Nystrom LE, & Cohen JD (2003). The neural basis of economic decision-making in the Ultimatum Game. Science, 300(5626), 1755–1758. [DOI] [PubMed] [Google Scholar]
- Sedikides C, & Hepper E (2009). Self-improvement. Social and Personality Psychology Compass, 3 (6), 899–917. [Google Scholar]
- Sherman DK, & Cohen GL (2006). The Psychology of Self- defense: Self- Affirmation Theory. Advances in Experimental Social Psychology, 38, 183–242. [Google Scholar]
- Shin JY, & Steger MF (2014). Promoting Meaning and Purpose in Life In Parks AC & Schueller SM (Eds.), The Wiley Blackwell Handbook of Positive Psychological Interventions (Vol. 17, pp. 90–110). Chichester, UK: John Wiley & Sons, Ltd. [Google Scholar]
- Smith BW, Tooley EM, Montague EQ, Robinson AE, Cosper CJ, & Mullins PG The role of resilience and purpose in life in habituation to heat and cold pain. The Journal of Pain: Official Journal of the American Pain Society, 10(5), 493–500. [DOI] [PubMed] [Google Scholar]
- Smith BW, & Zautra AJ (2004). The role of purpose in life in recovery from knee surgery. International Journal of Behavioral Medicine, 11(4), 197–202. [DOI] [PubMed] [Google Scholar]
- Stacey D, Bennett CL, Barry MJ, Col NF, Eden KB, Holmes-Rovner M, ... Thomson R (2011). Decision aids for people facing health treatment or screening decisions. Cochrane Database of Systematic Reviews , (10), CD001431. [DOI] [PubMed] [Google Scholar]
- Steele CM (1988). The Psychology of Self-Affirmation: Sustaining the Integrity of the Self In Berkowitz L (Ed.), Advances in Experimental Social Psychology (Vol. 21, pp. 261–302). Academic Press. [Google Scholar]
- van der Spek N, Vos J, van Uden-Kraan CF, Breitbart W, Cuijpers P, Knipscheer-Kuipers K, ... Verdonck-de Leeuw IM (2014). Effectiveness and cost-effectiveness of meaning-centered group psychotherapy in cancer survivors: protocol of a randomized controlled trial. BMC Psychiatry, 14, 22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wager TD, Atlas LY, Botvinick MM, Chang LJ, Coghill RC, Davis KD, ...Yarkoni T (2016). Pain in the ACC? Proceedings of the National Academy of Sciences of the United States of America, 113(18), E2474–E2475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wager TD, Atlas LY, Lindquist MA, Roy M, Woo C-W, & Kross E (2013). An fMRI-based neurologic signature of physical pain. The New England Journal of Medicine, 368(15), 1388–1397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yarkoni T, Poldrack RA, Nichols TE, Van Essen DC, & Wager TD (2011). Large-scale automated synthesis of human functional neuroimaging data. Nature Methods, 8(8), 665–670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yu L, Boyle PA, Wilson RS, Levine SR, Schneider JA, & Bennett DA (2015). Purpose in life and cerebral infarcts in community-dwelling older people. Stroke; a Journal of Cerebral Circulation, 46(4), 1071–1076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zilioli S, Slatcher RB, Ong AD, & Gruenewald TL (2015). Purpose in life predicts allostatic load ten years later. Journal of Psychosomatic Research, 79(5), 451–457. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.