

Abstract
Increased levels of psychological stress during adolescence have been associated with a decline in academic performance, school dropout and increased risk of mental health problems. Intervening during this developmental period may prevent these problems. The school environment seems particularly suitable for interventions and over the past decade, various school-based stress reduction programs have been developed. The present study aims to evaluate the results of (quasi-)experimental studies on the effectiveness of school-based intervention programs targeting adolescent psychological stress and to investigate moderators of effectiveness. A three-level random effects meta-analytic model was conducted. The search resulted in the inclusion of k = 54 studies, reporting on analyses in 61 independent samples, yielding 123 effect sizes (N = 16,475 individuals). The results indicated a moderate overall effect on psychological stress. Yet, significant effects were only found in selected student samples. School-based intervention programs targeting selected adolescents have the potential to reduce psychological stress. Recommendations for practice, policy and future research are discussed.
Keywords: Psychological stress, Meta-analysis, Adolescent, School-based intervention programs
Introduction
Stress—the condition or feeling that results when individuals perceive that the demands of a situation exceed their personal, psychological or social resources (Lazarus 1966)—seems to be a significant worldwide problem for both adolescents (Klinger et al. 2015) and adults (Schaufeli et al. 2009). In adolescence, a developmental period characterized by increased stress-sensitivity (Romeo 2013), high levels of stress have been linked to various negative associates, including reductions in academic performance (Kaplan et al. 2005), school drop-out (Dupéré et al. 2015), increased mental health problems (Snyder et al. 2017), and reduced well-being (Chappel et al. 2014). In order to prevent adverse development, it is important to address heightened stress levels during adolescence. Over the past decade, various school-based intervention programs have been implemented to reduce adolescent stress and accompanying effectiveness studies have been conducted. As knowledge on the overall effectiveness of such programs and factors influencing their effectiveness is limited, it is important to conduct an extensive meta-analysis. The current multilevel meta-analytic study therefore examined the effectiveness of school-based intervention programs in reducing adolescent psychological stress and which study, sample and intervention characteristics influence program effectiveness.
The school environment seems particularly suitable for intervention programs to reduce stress. Adolescents spend a substantial part of their time—on average six hours per school day—in school (Hofferth 2009), which makes the school an important context for cognitive development, as well as the development of social skills and emotional control, relevant for adequately dealing with stress (Resurrección et al. 2014). Since enhanced social and emotional functioning is beneficial for academic performance and school success (Zins et al. 2007), schools may benefit from implementing interventions that aim to improve social and emotional functioning. Moreover, school-based mental health services have been associated with a lower stigma and a greater utilization rate, especially among ethnic minority adolescents (Stephan et al. 2007). As such, school-based intervention programs provide a promising environment for low-threshold care, with the potential to also reach adolescents who are reluctant to search for care outside the school environment.
Over the past decade, various school-based intervention programs targeting adolescent stress have been developed. Some of these programs directly target stress, while other programs address stress as an indirect treatment aim. Moreover, to reduce stress and improve well-being of adolescents, these programs offer different approaches and apply various hypothesized mechanisms of change. For example, mindfulness (i.e., bringing non-judgmental attention to the present moment through meditation techniques and awareness exercises), relaxation exercises (e.g., progressive relaxation, muscle relaxation, visualization-based relaxation) and life skills training, comprising different cognitive-behavioral techniques (e.g., emotion regulation, problem-solving, conflict resolution), are often used (Rew et al. 2014). In terms of effectiveness, some studies on school-based stress intervention programs have yielded positive results (e.g., Jellesma and Cornelis 2012; De Wolfe and Saunders 1995; White 2012), whereas other studies indicated that interventions were not effective in reducing stress (e.g., Lang et al. 2017; Lau and Hue 2011; Terjestam et al. 2016).
The conflicting results of earlier studies are an important reason to conduct a meta-analysis to assess the effectiveness of school-based intervention programs in reducing adolescent psychological stress. Reportedly, there are only three reviews of the literature in this area (Feiss et al. 2019; Kraag et al. 2006; Rew et al. 2014). In their meta-analytic review, Kraag et al. (2006) investigated the effectiveness of school-based universal intervention programs targeting stress in children and adolescents. They demonstrated that these programs were effective in decreasing stress symptoms. Such promising results were supported by a narrative review on the effectiveness of stress reduction interventions in adolescents from community and clinical populations (Rew et al. 2014). In contrast, Feiss et al. (2019) showed that school-based stress prevention programs did not reduce stress symptoms in adolescents. In addition to generating conflicting findings, previous reviews bear a number of limitations. First, particularly the reviews by Kraag et al. (2006) and Rew et al. (2014) suffer from low quality of the included studies, limiting the robustness of their results. Second, Kraag et al. (2006) and Feiss et al. (2019) performed a traditional meta-analysis, a technique that does not allow the inclusion of multiple relevant effect sizes within studies. Third, Feiss et al. (2019) focused on school-based programs in the United States and based their meta-analysis on only four studies that assessed the effectiveness of such programs in terms of stress reduction. As such, their results do not inform us about the overall effectiveness of school-based intervention programs targeting stress in adolescents.
Because of these limitations, as well as the widespread implementation of school-based stress reduction programs and accompanying effectiveness studies since publication of the comprehensive review by Kraag et al. (2006), it is important to update the findings and conduct a new extensive meta-analysis. Consistent with Feiss et al. (2019), the present study included intervention programs in general adolescent populations (i.e., community samples) as well as selected adolescent populations (i.e., samples based on self-selection or screening, for instance on high stress or anxiety levels), given the potential of targeted interventions to be more efficient and to address problems early on (Offord 2000). Indeed, Feiss et al. (2019) demonstrated that targeted interventions yielded greater reductions in stress than universal interventions. Furthermore, the current study advances previous literature by performing a multilevel meta-analysis to fully exploit the available research data (i.e. allowing the inclusion of all relevant effect sizes per study) and generate more statistical power (Assink and Wibbelink 2016). This increased power ensures that extensive moderator analyses can be conducted. Investigating moderators is of crucial importance to better understand study results and to detect which interventions or components work best and which subgroups benefit most (Kraemer et al. 2002). This knowledge is necessary for the development of effective interventions and the selection of the best intervention for a specific population.
Based on previous meta-analyses on the effectiveness of intervention programs in youth, various study, sample and intervention characteristics may moderate program effectiveness. In terms of study characteristics, type of stress measured, publication year, publication status, study quality, the (in)dependence of authors, type of control condition, study design and timing of measurements were deemed important to consider. With regard to type of stress, effectiveness may vary across specific types of stress, such as school stress (e.g., pressure from study and worrying about grades or workload) or social stress (i.e., stress that stems from interpersonal relationships or from the social environment in general, such as the adolescents’ home life). Whether the study was performed recently or not might moderate the effectiveness, since the likelihood of reporting null-results has increased over the last two decades (Kaplan and Irvin 2015). However, previous research demonstrated no difference in publication year (Zoogman et al. 2015). Larger effects have been found for published versus unpublished studies (Conley et al. 2016), lower versus higher quality studies (Kraag et al. 2006), studies with quasi-experimental designs versus randomized controlled trials (RCTs) (Suter and Bruns 2009) and studies by researchers who developed the intervention program they studied versus independent researchers (Petrosino and Soydan 2005). Moreover, comparison with active versus passive control groups may impact findings of effectiveness studies (Feiss et al. 2019), and should therefore be considered. Furthermore, it is important to not only focus on post-intervention assessments, but also on follow-up assessments to investigate the long-term effects of school-based intervention programs.
Additionally, sample characteristics may affect the magnitude of the effects of school-based programs on stress reduction, for example age, gender distribution, socioeconomic status (SES) and ethnicity. A higher likelihood of effectiveness of intervention programs has been found in older versus younger samples and in samples with a higher proportion of females (Stice et al. 2009). Participants with low socioeconomic or minority backgrounds might respond differently to school-based intervention programs, possibly related to the implementation of the program. More specifically, schools in disadvantaged areas often suffer from various problems, such as high levels of unemployment, high staff turnover, poor facilities and lack of resources (Harris and Chapman 2004). This might make it more difficult to adequately implement intervention programs, resulting in lower effectiveness (Durlak et al. 2011). Furthermore, interventions in selected high-risk samples versus community samples (Stice et al. 2009), and targeted compared to universal intervention programs (Feiss et al. 2019) have been found to be more effective, suggesting that intervention programs generate more positive changes if problems are more severe at the start of the intervention. Moreover, it is possible that the selection method for including participants moderates program effectiveness. Inclusion based on self-selection might be more effective than inclusion based on screening, because it is likely that self-selected participants are more motivated to attend and actively participate in an intervention program (Stice et al. 2009).
Finally, there are some intervention characteristics that may affect the effectiveness of school-based intervention programs targeting psychological stress, including intensity, type of instructors and components and focus of the program. Previous meta-analyses demonstrated larger effects for less intensive interventions (Stice et al. 2009), and interventions delivered by external professionals (e.g. mental health professionals) as opposed to professionals working at the involved schools (Werner-Seidler et al. 2017). Moreover, techniques taught in intervention programs may affect effectiveness, with problem solving and emotional coping skills showing larger effects compared to relaxation techniques (Kraag et al. 2006). Whether or not the intervention directly addresses stress reduction might influence program effectiveness, because intervention programs with a direct focus on stress reduction may generate larger effects than interventions that address stress indirectly.
Current Study
Given the increased number of school-based intervention programs targeting psychological stress in adolescents, and the limited knowledge on their overall effectiveness and factors influencing program effectiveness, it is important to conduct a new extensive meta-analysis. The current multilevel meta-analysis therefore aimed to determine the effectiveness of different school-based intervention programs in reducing psychological stress in adolescents. The second aim was to investigate which study (i.e., type of stress, publication year, publication status, study quality, study design, (in)dependence of authors, type of comparison condition, timing of measurements and time to follow-up), sample (i.e., age, gender, SES, ethnicity, target group and selection method), and intervention characteristics (i.e., intensity, type of instructor, components and focus of intervention) moderate the effectiveness of these programs.
School-based intervention programs were expected to reduce psychological stress in adolescents (Kraag et al. 2006). Larger effects were expected for published versus unpublished studies (Conley et al. 2016), for lower versus higher quality studies (Kraag et al. 2006), for studies by researchers who developed the intervention program they studied versus independent researchers (Petrosino and Soydan 2005), for studies with quasi-experimental designs versus RCTs (Suter and Bruns 2009) and for studies with active compared to passive control groups (Feiss et al. 2019). Larger effects were also expected for older, female samples (Stice et al. 2009), for samples with lower proportions of participants with low socioeconomic and minority backgrounds, and for selected samples, particularly based on self-selection (Stice et al. 2009). Furthermore, less intensive programs (Stice et al. 2009), intervention programs given by external professionals as opposed to professionals working at the involved schools (Werner-Seidler et al. 2017), having problem solving and emotional coping skills versus relaxation techniques as a component (Kraag et al. 2006), and that directly versus indirectly addressed stress reduction were expected to have larger effects. For type of stress, publication year and timing of measurements no hypotheses were formulated.
Methods
The current study adhered to PRISMA guidelines (Moher et al. 2009).
Selection Criteria
Available studies were searched that investigated the effects of school-based intervention programs on psychological stress in adolescents, meeting the following inclusion criteria: (1) studies had to evaluate the effectiveness of a school-based intervention program promoting psychosocial functioning (e.g., stress reduction, mental health, well-being, or coping skills), (2) studies had at least one psychological stress outcome, measured with self-report questionnaires, (3) studies had to target adolescents, with a mean age of 10 to 18 years old at the start of the intervention, (4) studies had to compare an experimental group and a control group, (5) studies had to include pre- and post-intervention assessment measures and/or follow-up assessment measures, (6) studies had to be written in English and (7) studies had to have available statistics suitable for performing meta-analyses (i.e., statistics to extract an effect size).
Search Strategy
Through a systematic computer search, relevant publications were identified using the search engines Cumulative Index to Nursing and Allied Health Literature (CINAHL), PubMed, Education Resources Information Center (ERIC), PsycINFO and Cochrane. The search period was—since records began—up until June 2019, and four search terms were used. The search strings were “intervention* or program*” in combination with “stress or distress” in combination with “adolesc* or child or children or youth” in combination with “controlled clinical trial or controlled trial or random* or experiment* or comparison group* or controls or control condition* or control group* or control subject* or no treatment group* or waiting list or wait list or waitlist or treatment as usual or care as usual”. In addition, not statements were used to exclude studies that involved oxidative stress, distress syndrome, parenting stress, immunization, vaccination or venipuncture, studies that involved animals, infants, toddlers, preschool or kindergarten, studies about pregnancy, neonatal and prenatal, and study protocols, reviews and meta-analyses. Google Scholar was used to check the first 100 hits for missing relevant publications and to search for gray literature (i.e., unpublished work). Furthermore, a manual search through the reference lists of the identified publications, relevant review (Rew et al. 2014) and meta-analyses (Feiss et al. 2019; Kraag et al. 2006) was conducted.
Coding of Studies
A detailed coding system was used to register study characteristics, outcome variables and moderators. All studies were coded by the first author. A subsample of the studies was double coded by either of two other researchers and responses of the two coders were compared (Inter-rater reliability (IRR) was 89.8% for a subset of 42.6% of the studies). Inconsistent responses were discussed with a fourth researcher to reach consensus. Effect sizes were coded for psychological stress (e.g., perceived stress, symptoms of stress). Positive effect sizes reflect improvements in functioning in the intervention group when compared to the control group. The following study, sample, and intervention characteristics were coded as moderators.
Study characteristics were type of stress outcome (school stress versus social stress), publication year (as a continuous variable), publication status (published or not published), study design ((cluster) RCT or quasi-experimental study, with RCT defined as randomly allocating participants to the experimental or control group, cluster RCT defined as randomly allocating groups of participants, and quasi-experimental design defined as a controlled study without random assignment of groups), type of comparison condition (passive control versus active control, with passive control defined as no intervention, regular school activities and waitlist control, and active control defined as treatment-as-usual and other interventions), the independence of the authors (whether or not the authors owned or (co-)developed the intervention), timing of measurements (whether the measurement was post-intervention or at follow-up, with post-intervention defined as measurement immediately after completion of the intervention and follow-up defined as measurement after the post-intervention measurement), time to follow-up (in weeks) since completion of the intervention (as a continuous variable), and study quality (as a continuous variable). The Quality Assessment Tool for Quantitative Studies (Thomas et al. 2004) was used to assess study quality, based on the characteristics selection bias, study design, confounders, blinding, data collection methods (validity and reliability) and withdrawals and dropout. Each variable was scored with 0 (not accounted for/missing), 1 (somewhat accounted for) and 2 (completely accounted for). Using these six variables, a total quality score was calculated for each study (range 0–12).
Sample characteristics were target group (non-selected or selected student samples, with non-selected students defined as samples of students from the general population and selected students defined as samples of students who self-selected or were selected based on prior screening), selection method (self-selection versus selection based on prior screening, such as participants self-selecting for an optional program or participants screened on high stress or anxiety levels), percentage of boys (as a continuous variable), percentage of low SES (i.e., low income, analyzed as a continuous variable), percentage of minorities (i.e., non-Caucasian, analyzed as a continuous variable) and mean age of the adolescents (if mean age was not reported, the midpoint of the age range was used, analyzed as a continuous variable).
Intervention characteristics were whether or not the intervention included the most often used stress reduction techniques (Rew et al. 2014), i.e., mindfulness (yes or no), relaxation exercises (yes or no) and cognitive-behavioral techniques (yes or no), intensity of the intervention (session duration multiplied by frequency of sessions; if session duration was reported as “a lesson”, the average of 45 min was used, analyzed as a continuous variable), type of instructors (specialized instructors or other instructors, including school personnel or researchers) and program target (whether stress reduction was a direct target of the intervention program or an indirect program target, based on the presence or absence of components that directly target stress management). Interventions with stress reduction as a direct program target included components to train mindfulness, yoga, relaxation or coping skills to manage stress, whereas interventions with stress reduction as an indirect program target included activities such as gardening or swimming, or components to train general coping or social skills. Program integrity (i.e., whether the intervention was applied according to protocol) was initially coded, but eventually not included as a moderator because few studies reported information about program integrity.
Analysis of Effect Sizes
Using an online effect size calculator (Wilson n.d.), Cohen’s d’s were calculated for each effect size indicating the effectiveness of school-based intervention programs on psychological stress on the basis of differences between adolescents receiving an intervention program and adolescents in a control group. In most cases, Cohen’s d was calculated based on means and standard deviations (SD) or standard errors (SE). Group differences were computed for both pre- and post-intervention and pre-intervention d’s were subtracted from post-intervention d’s to account for baseline differences between groups (e.g., Van der Stouwe et al. 2014). When there were no means and SD/SE reported (13.8% of the total number of effect sizes), Cohen’s d was calculated based on mean difference scores, t-, F- or chi-square values. A small effect size was considered d = 0.20, a moderate effect size d = 0.50 and a large effect size d = 0.80 (Cohen 1988). Dummy variables were computed for the categorical moderators and continuous moderators were mean centered.
A three-level meta-analytic model was used in R to calculate an overall effect size and to conduct moderator analyses (Assink and Wibbelink 2016), thereby taking into account the dependency of multiple effect sizes from the same study (Van den Noortgate et al. 2013). Three levels of variance were included in the model: the sampling variance of each effect size (level 1), the within-study variance of effect sizes in the same study (level 2) and the between-study variance of effect sizes from different studies (level 3). The overall effect was estimated using an intercept-only model for psychological stress. The analysis was repeated after removal of outliers (i.e., extreme effect sizes, with an Interquartile Range (IQR) > 3) (Elbaum et al. 2000). Separate log-likelihood tests were performed to test if there was significant variance within (level 2) and between (level 3) studies (i.e., significant heterogeneity). If there was significant heterogeneity for at least one of the levels, moderator analyses were performed. In that case, possible moderators were included in the three-level intercept model (Assink and Wibbelink 2016). The Knapp and Hartung-method (Knapp and Hartung 2003) was applied, resulting in a decreased risk of Type 1-errors (Assink and Wibbelink 2016). Moderators were only included if there were at least three effect sizes for the specific moderator and at least one effect size per category of the moderator.
Publication Bias
It is important to consider publication bias when conducting a meta-analytic study, because it is more likely that studies with positive results are published compared to studies that have negative or non-significant results, which could result in an underrepresentation of studies with minimal or negative effects. First, Rosenthal’s fail-safe test was performed, indicating no publication bias when the fail-safe N exceeds the critical value (derived by the formula 5 × k + 10, where k is the number of studies) (Rosenthal 1979). The critical value represents the number of studies with null results needed to make the overall result nonsignificant. Second, the funnel plot was visually inspected to detect asymmetry, which is an indication for publication bias. Third, in accordance with the Egger’s asymmetry test (Egger et al. 1997), a multilevel analysis was conducted with the sampling variance as a moderator to detect small study biases. Fourth, a trim and fill analysis was performed to test the influence of missing effect sizes on the results by repeating the meta-analysis after imputing the missing effect sizes (Duval and Tweedie 2000a, b).
Results
Study Selection
As displayed in the flowchart (Fig. 1), the electronic search identified 4398 unique hits for all databases after the removal of duplicates. After first selection by screening the title and abstract of the publications, 300 studies were potentially eligible. Following full text screening, 55 studies met the inclusion criteria. Of these 55 studies, six studies were excluded because they were earlier versions of included studies. The alternative search yielded 5 additional studies, which resulted in a final number of k = 54 included studies, reporting on analyses in 61 independent samples, yielding N = 123 effect sizes based on N = 9196 participants in an intervention group and N = 7279 participants in a control group.
Fig. 1.

Flow chart
All studies included in this meta-analytic review were issued between 1989 and 2019. Almost all studies were published, only 3 studies were not (i.e., dissertations). School or social stress, as an alternative to general stress, were examined in only 8 studies (based on 8 independent samples; 5 for school stress and 3 for social stress). Studies were (clustered) RCTs (37 studies, 41 independent samples) or quasi-experimental (17 studies, 20 samples). Most studies (32 studies, 36 samples) used a passive control group. About half of the studies was written by independent authors (26 studies, 27 samples). Only few studies (17 studies, 17 samples) included follow-up measurements, ranging from 4 to 48 weeks after the post-intervention assessment, with a mean of 17 weeks. Study quality ranged from 1 to 11, with a mean score of 6. Almost half (26 studies, 29 samples) included selected students, while the other half (28 studies, 32 samples) included non-selected, community sample students. Of the selected student samples, 16 were generated by screening and 13 by self-selection. Across samples, average age ranged between 10.3 and 17.7 years with an overall mean of 14.6 years. The mean percentage of boys was 41.4% (based on 58 samples), the mean percentage of minorities was 52.8% (based on 22 samples) and the mean percentage of low SES was 42.2% (based on 20 samples). With regard to the intervention programs, 47 studies (53 samples) directly focused on stress reduction, while the other studies did not. In terms of intervention components, mindfulness was included in 19 studies (21 samples), relaxation techniques in 21 studies (25 samples) and cognitive behavioral techniques in 25 studies (28 samples). The intensity of the intervention programs ranged from 100 to 9900 min, with a mean of 1015 min (based on 53 samples). Interventions were delivered by specialized instructors in 20 studies (22 samples) and by other instructors (e.g., school personnel, researchers) in 30 studies (35 samples). Details of the selected studies are provided in Table 1.
Table 1.
Detailed description of the selected studies
| Authors | N | Age range, mean age (SD), grade, gender, ethnicitya | Study design | Target group (selection) | Intervention | Program target (stress reduction) | Stress outcomeb |
|---|---|---|---|---|---|---|---|
| Bennett and Dorjee (2016) | 24 |
16–18 years, 17.70 (0.73) 11–12th grade, 58% boys |
Quasi-experimental | Self-selected (voluntary) | Mindfulness-based stress reduction | Direct | Psychological stress (DASS, 7 items), perceived stress (body barometer, 1 item) |
| Bluth et al. (2016) | 27 |
17.0 9–12th grade, 59% boys, 82% minorities |
RCT | Self-selected (voluntary) | Learning to BREATHE | Direct | Perceived stress (PSS, 10 items) |
| Burckhardt et al. (2016) | 63 |
15–18 years 10–11th grade, 61% boys |
Cluster RCT | Screened (high depression, anxiety, stress levels) | Strong Minds | Direct | Stress levels (DASS, 7 items) |
| Butzer et al. (2017) | 209 |
12.64 (0.33) 7th grade, 37% boys, 47% minorities |
Cluster RCT | Community | Kripalu Yoga in the schools | Direct | Perceived stress (PSS, 10 items) |
| Campbell et al. (2019) | 1007 |
13–19 years, 15.96 (1.17) 9–12th grade, 50% boys, 30% minorities |
Quasi-experimental | Community | .b (the Mindfulness in Schools Project) | Direct | Perceived stress (PSS, 9 items) |
| Carreres-Ponsoda et al. (2017) | 30 |
16–18 years, 16.80 50% boys |
RCT | Self-selected (voluntary) | Mindfulness-based stress reduction | Direct | Perceived stress (PSS, 14 items) |
| Carter (2010) | 64 |
13–16 years, 14.70 (0.74) 9–10th grade, 45% boys, 22% minorities |
Cluster RCT | Self-selected (self-identified and identified by others) | The Best of Coping program | Direct | Stress appraisal of challenge, threat and resources (SAMA, 4, 7 and 3 items) |
| Cross et al. (2018) | 2945 |
13.0 8–9th grade, 50% boys |
Cluster RCT | Community | Friendly Schools Program | Indirect | Stress scores (DASS, 7 items) |
| Da Silva et al. (2019) | 20 |
11–14 years, 12.10 (1.50) 70% boys |
RCT | Screened (ADHD) | Swimming-learning program | Indirect | Perceived stress (PSS, 14 items) |
| De Anda (1998) | 54 |
12–14 years, 13.00 30% boys, 53% minorities |
Quasi-experimental | Self-selected (voluntary) | Cognitive-behavioral stress management program | Direct | Degree of experienced stress (ASCM, 4 items) |
| Dowling et al. (2019) | 675 |
15–18 years, 15.87 (0.69) 5th grade, 50% boys |
Cluster RCT | Community | MindOut program | Direct | Levels of symptoms related to stress (DASS, 7 items) |
| Ebrahmimi et al. (2015) | 40 |
14–18 years, 16.48 (1.10) 100% boys |
Quasi-experimental | Self-selected (voluntary) | Spiritual intelligence training | Direct | Stress scores (DASS, 7 items) |
| Eggert et al. (1995) | 105 |
15.86 (1.01) 9–12th grade, 42% boys, 72% minorities |
Quasi-experimental | Screened (suicide risk) | Personal growth class | Direct | Perceived stress and pressure from others (4 items) |
| Eslami et al. (2016) | 126 |
16.33 (7.02) 0% boys |
RCT | Community | Assertiveness training program | Direct | Stress levels (DASS, 7 items) |
| Fridrici and Lohaus (2009) | 904 |
12–18 years 8–9th grade, 50% boys |
Cluster RCT | Community | Stress prevention intervention | Direct | General stress (3 items) |
| Fung et al. (2019) | 145 |
13–15 years, 13.99 (0.36) 9th grade, 32% boys, 97% minorities |
RCT | Screened (depressive symptoms) | Learning to breathe | Direct | Perceived stress (PSS, 9 items) |
| Garcia et al. (2013) | 41 |
13–16 years, 14.80 (0.72) 9–10th grade, 0% boys, 100% minorities |
RCT | Self-selected (voluntary) | Project Wing’s Girl’s group | Direct | Perceived stress (PSS, 14 items), level of stress symptoms (DASS, 14 items) |
| Goodman and Newman (2014) | 60 |
9th or 12th grade 0% boys |
RCT | Self-selected (voluntary) | Digital storytelling | Direct | Experienced daily stress (ASQ, 31 items) |
| Hampel et al. (2008) | 320 |
10–14 years, 11.70 (1.18) 5–8th grade, 50% boys |
Quasi-experimental | Community | Anti-stress training | Direct | Interpersonal, academic stress (7 items) |
| Hiebert et al. (1989) Study 1 | 79 |
13–14 years 8th grade, 48% boys |
Cluster RCT | Community | Progressive relaxation | Direct | Stress symptoms (SOSI, 59 items) |
| Hiebert et al. (1989) Study 2 | 22 |
17–18 years 11–12th grade, 63% boys |
Quasi-experimental | Self-selected (elective module) | Progressive relaxation | Direct | Stress symptoms (SOSI, 59 items) |
| Jamali et al. 2016 | 100 |
13–14 years, 13.50 (1.01) 50% boys |
RCT | Community | Life skills training | Indirect | Perceived stress (10 items) |
| Jellesma and Cornelis (2012) | 54 |
8–13 years, 10.58 (1.58) 3th/6th grade, 65% boys |
Cluster RCT | Community | Mind Magic Program | Direct | Psychological, mental stress (10-point scale) |
| Jose and Sajeena (2017) | 60 | 8–10th grade | Cluster RCT | Self-selected | Yoga therapy | Direct | Perceived stress (PSS, 10 items) |
| Khalsa et al. (2012) | 100 |
15–19 years, 16.80 (0.60) 11–12th grade, 58% boys, 10% minorities |
Cluster RCT | Community | Yoga Ed program | Direct | Perception of stress (PSS, 10 items), social stress (BASC, 13 items) |
| Kiselica et al. (1994) | 48 | 9th grade, 54% boys, 0% minorities | Cluster RCT | Screened (anxiety symptoms) | Stress inoculation training | Direct | Stress symptoms (SOSI, 118 items) |
| Kraag et al. (2009) | 1437 |
10.30 (0.64) 5–6th grade, 50 % boys |
Cluster RCT | Community | Learn Young, Learn Fair | Direct | Physiological, psychological stress symptoms (MUSIC) |
| Kuyken et al. (2013) | 522 |
12–16 years, 14.80 (1.50) 70% boys, 28% minorities |
Quasi-experimental | Community | Mindfulness in Schools Program | Direct | Perceived stress (PSS, 10 items) |
| Lai et al. (2016) | 2304 |
14–16 years, 15.40 (1.00) 8–10th grade, 51% boys |
Quasi-experimental | Community | The Little Prince is Depressed | Direct | Stress levels (DASS, 7 items) |
| Lang et al. (2017) | 122 |
16.22 (1.12) 65% boys |
Cluster RCT | Community | EPHECT coping training | Direct | Perceived stress (ASQ, 30 items) |
| Lau and Hue (2011) | 48 |
14–16 years, 15.83 38% boys 0% minorities |
Quasi-experimental | Self-selected (voluntary) | Mindfulness program | Direct | Perceived stress (PSS, 10) |
| Lee et al. (2018) | 20 | 10–11 years, 10.50 | RCT | Screened (emotional and behavioral problems) | Horticulture-related activities | Indirect | Stress levels: social, school stress (PSS, 10 items) |
| Livheim et al. (2015) | 32 |
14–15 years 28% boys |
RCT | Screened (depressive symptoms) | Acceptance and Commitment Therapy | Direct | Perceived stress (PSS, 10 items), stress levels (DASS, 7 items) |
| Manjushambika et al. (2017) | 65 |
11–17 years, 14.50 42% boys |
Quasi-experimental | Screened | Jacobson’s Progressive Muscle Relaxation | Direct | Educational stress (ESSA, 16 items) |
| Marsland et al. (2019) | 70 |
8–14 years, 10.65 (1.49) 3–8th grade, 54% boys, 70% minorities |
RCT | Screened (asthma) | I Can Cope | Direct | Perceived stress (PSS, 10 items) |
| Metz et al. (2013) | 216 |
16.45 (0.95) 10–12th grade, 34% boys, 11% minorities |
Quasi-experimental | Community | Learning to Breathe | Direct | Perceived stress level (1 item) |
| Noggle et al. (2012) | 51 |
17.20 (0.70) 11–12th grade, 46% boys, 8% minorities |
Cluster RCT | Community | Kripula yoga | Direct | Perceived stress (PSS, 10 items) |
| Norlander et al. (2005) | 95 |
11.31 (1.09) 44% boys |
Quasi-experimental | Community | Relaxation | Direct | Experienced stress levels (10 items) |
| Puolakanaho et al. (2019) | 205 |
15.27 (0.39) 9th grade, 51% boys |
RCT | Community | Youth COMPASS | Direct | Overall stress (1 item), school stress (4 items) |
| Quach et al. (2016) | 149 |
12–15 years, 13.18 (0.72) 7–9th grade, 38% boys, 99% minorities |
RCT | Community | Mindfulness meditation and hatha yoga | Direct | Perceived stress (PSS, 10 items) |
| Reiss (2013) | 40 |
16–18 years, 17.25 (0.54) 12th grade, 65% boys |
Quasi-experimental | Self-selected (voluntary) | Mindfulness meditation treatment | Direct | Perceived stress (PSS, 10 items) |
| Rentala et al. (2019) | 60 | 16–19 years, 17.13, 0% boys | RCT | Screened (high stress levels) | Holistic group health promotion program | Direct | Stress levels (DASS, 7 items), educational stress (ESSA, 16 items) |
| Ruiz-Aranda et al. (2012) | 147 |
13–16 years, 14.18 (0.64) 40% boys |
RCT | Community | Emotional intelligence education program | Indirect | Social stress (BASC, 13 items) |
| Sibinga et al. (2013) | 41 |
11–14 years, 12.50 7–8th grade, 100% boys, 95% minorities |
RCT | Community | Mindfulness-based stress reduction | Direct | Perceived stress (PSS, 10 items) |
| Sibinga et al. (2016) | 300 |
12.00 5–8th grade, 49% boys, 100% minorities |
Cluster RCT | Community | Mindfulness-based stress reduction | Direct | Perceived stress (PSS, 6 items) |
| Silbert and Berry (1991) | 145, 178 |
14–18 years, 15.00 10th grade, 50% boys, 70% minorities |
Quasi-experimental | Screened, community | Suicide prevention unit | Indirect | Subjective experience of stress (SSS, 14 items) |
| Singhal et al. (2014) | 19 |
13–18 years 9th grade, 0% boys |
Quasi-experimental | Screened (sub-clinical depression) | Coping skills program | Direct | Academic stress (SAAS) |
| Singhal et al. (2018) | 120 |
13–18 years 8th, 9th and 11th grade |
Cluster RCT | Screened (sub-clinical depression) | Coping skills program | Direct | Academic stress (SAAS) |
| Solar (2013) | 10 |
14–18 years, 16.00 (1.25) 9–12th grade, 70% boys, 30% minorities |
RCT | Screened (emotional / learning disability or other health impairment) | Mindfulness meditation | Direct | Perceived stress (PSS, 10 items) |
| Terjestam (2011) | 393 |
12–15 years, 13.90 7–9th grade, 48% boys |
Cluster RCT | Community | Meditation based technique for stillness | Direct | General stress (3 items) |
| Terjestam et al. (2010) | 119 |
13–14 years, 13.18 7th grade, 49% boys |
Quasi-experimental | Community | Qigong | Direct | General stress (3 items) |
| Terjestam et al. (2016) | 307 |
5–8th grade 52% boys |
Cluster RCT | Community | Compas program | Direct | Stress levels (General Stress Scale, 3 items) |
| Van der Gucht et al. (2018) | 390 |
13–20 years, 15.40 (1.20) 9–11th grade, 37% boys |
Cluster RCT | Community | Mindfulness group training | Direct | Stress symptoms (DASS, 7 items) |
| Van Ryzin and Roseth (2018) | 1449 |
7th grade 52% boys, 24% minorities |
Cluster RCT | Community | Cooperation in the classroom | Indirect | Perceived stress (PSS, 4 items) |
| Zafar and Khalily (2015) | 100 |
12–18 years 50% boys |
RCT | Screened (high depression, anxiety, stress levels) | Didactic therapy | Direct | Stress levels (DASS, 14 items) |
DASS depression anxiety stress scale, RCT randomized controlled trial, PSS perceived stress scale, SAMA stress appraisal measure for adolescents, ASCM the adolescent stress and coping measure, ASQ adolescent stress questionnaire, SOSI symptoms of stress inventory, MUSIC Maastricht University Stress Instrument for Children, BASC behavior assessment system for children and adolescents, ESSA education stress scale for adolescents, SAA scale for academic stress
aPercentage of minorities (i.e., non-Caucasian)
bDescriptions of authors
Overall Effect
Test statistics for the overall effect can be found in Table 2. The overall effect size of school-based intervention programs on psychological stress was moderate (d = 0.543, p < 0.001), indicating that intervention programs are effective in reducing psychological stress. The heterogeneity test revealed that there was significant within-study and between-study variance (p < 0.0001).
Table 2.
Result for the overall mean effect size
| Outcome | N studies (samples) | N ES | N participants | Mean d (SE) | 95% CI | t-value | LRT | % var | Fail-safe N (cv) |
|---|---|---|---|---|---|---|---|---|---|
| Psychological stress | 54 (61) | 123 | 16,475 | 0.543 (0.133) | 0.279-0.806 | 4.082*** | Level 2: 16.32*** | Level 1: 1.5% | 16,223 (280) |
| Level 3: 100.41*** | Level 2: 1.2% | ||||||||
| Level 3: 97.3% |
N studies (samples) number of studies and independent samples, N ES number of effect sizes, mean d mean effect size Cohen’s d, SE standard error, CI confidence interval, t-value difference in mean d with zero, LRT likelihood-ratio test for level 2 and level 3, % var percentage of variance explained, Fail-safeN (cv) fail-safe number and Rosenthal’s critical value in parentheses
***p < 0.001
Sensitivity Analysis
To account for the possible influence of outliers, the meta-analysis was repeated after removal of ten outliers (i.e., ten extreme positive effect sizes). This yielded a smaller but still significant effect on psychological stress (d = 0.276, SE = 0.064, p< 0.001).
Publication Bias
The Rosenthal fail-safe test revealed that there was no indication of publication bias because the fail-safe N exceeded the critical value (see Table 2). However, the funnel plot (see Fig. 2) demonstrated asymmetry and the regression analysis of the sampling variance was significant (p < 0.001), indicating publication bias. The trim and fill analysis revealed that 26 effect sizes were missing on the left side of the distribution and results after imputation demonstrated a significant but very small overall effect on psychological stress (d = 0.068, SE = 0.011, p < 0.0001), thereby supporting the suggestion that studies with positive results are overrepresented, resulting in an inflation of the overall effect.
Fig. 2.
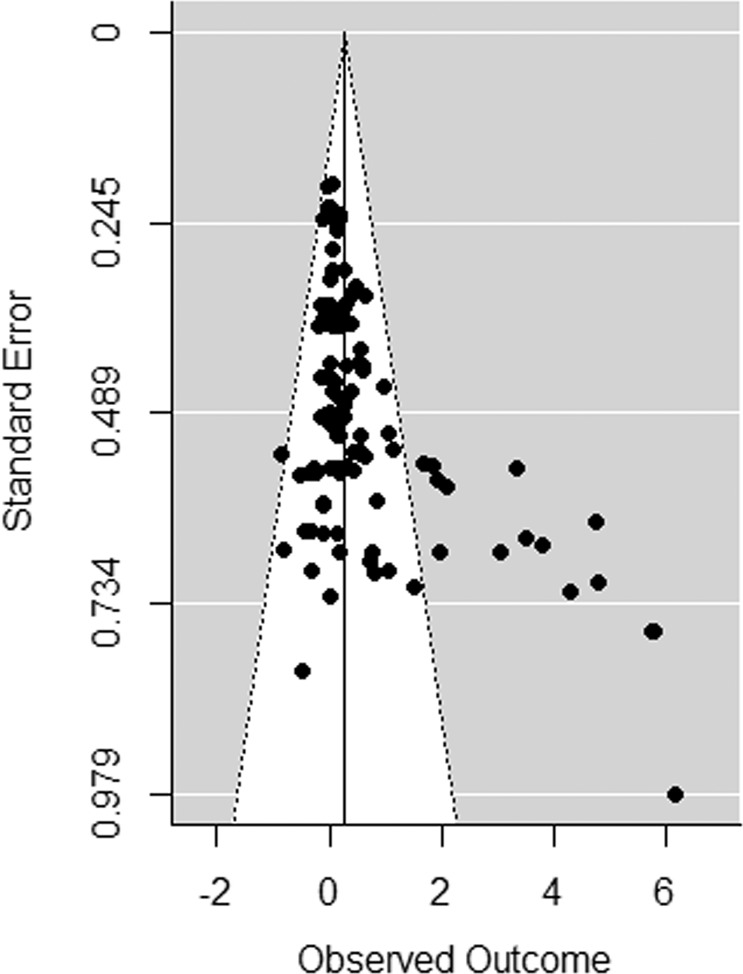
Funnel plot for psychological stress
Moderator Analyses
The results of the moderator analyses on psychological stress are reported in Table 3. Significant results are described here.
Table 3.
Results for the moderator analyses on psychological stress
| Moderator | N samples | N ES | B0 (95% CI) | t0 | B1 (95% CI) | t1 | F(df1, df2) | p |
|---|---|---|---|---|---|---|---|---|
| Study characteristics | ||||||||
| Type of stress | F (1, 13) = 4.754 | 0.048 | ||||||
| School stress (RC) | 5 | 10 | 2.739 (1.465–4.012) | 4.646*** | ||||
| Social stress | 3 | 5 | 0.531 (−1.247 to 2.309) | 0.646 | −2.207 (−4.394 to −0.020) | −2.180* | ||
| Publication year (continuous) | 61 | 123 | 0.539 (0.276–0.801) | 4.061*** | 0.020 (−0.013 to 0.054) | 1.198 | F (1, 121) = 1.436 | 0.233 |
| Publication status | F (1, 121) = 1.557 | 0.215 | ||||||
| Published (RC) | 58 | 114 | 0.579 (0.310–0.848) | 4.266*** | ||||
| Not published | 3 | 9 | −0.210 (−1.433 to 1.012) | −0.340 | −0.789 (−2.041 to 0.463) | −1.248 | ||
| Design | F (1, 121) = 0.566 | 0.453 | ||||||
| (Cluster) RCT (RC) | 41 | 74 | 0.613 (0.291–0.936) | 3.765*** | ||||
| Quasi-experimental | 20 | 49 | 0.400 (−0.060 to 0.859) | 1.723 | −0.213 (−0.775 to 0.348) | −0.752 | ||
| Type of comparison condition | F (1, 121) = 1.336 | 0.250 | ||||||
| Passive control (RC) | 36 | 80 | 0.671 (0.328–1.014) | 3.872*** | ||||
| Active control | 25 | 43 | 0.359 (−0.051 to 0.769) | 1.732 | −0.312 (−0.847 to 0.223) | −1.156 | ||
| Authors | F (1, 108) = 1.115 | 0.293 | ||||||
| Independent (RC) | 27 | 54 | 0.665 (0.292–1.038) | 3.534*** | ||||
| Dependent | 25 | 56 | 0.380 (−0.003 to 0.763) | 1.967 | −0.285 (−0.820 to 0.250) | −1.056 | ||
| Time of measurements | F (1, 121) = 6.693 | 0.011 | ||||||
| Post-intervention (RC) | 44 | 93 | 0.522 (0.257–0.786) | 3.906*** | ||||
| Follow-up | 17 | 30 | 0.672 (0.390–0.953) | 4.724*** | 0.150 (0.035–0.265) | 2.587* | ||
| Time to follow-up (continuous) | 17 | 30 | 0.964 (0.037–1.891) | 2.131* | 0.006 (−0.017 to 0.028) | 0.504 | F (1, 28) = 0.254 | 0.618 |
| Study quality (continuous) | 61 | 123 | 0.546 (0.280–0.812) | 4.063*** | 0.019 (−0.096 to 0.134) | 0.327 | F (1, 121) = 0.107 | 0.744 |
| Sample characteristics | ||||||||
| Target group | F (1, 121) = 7.065 | 0.009 | ||||||
| Selected (RC) | 29 | 58 | 0.908 (0.537–1.280) | 4.844*** | ||||
| Not-selected | 32 | 65 | 0.234 (−0.104 to 0.572) | 1.370 | −0.674 (−1.177 to 0.172 | −2.658** | ||
| Selection method | F (1, 56) = 3.119 | 0.083 | ||||||
| Screened (RC) | 16 | 31 | 1.406 (0.676–2.135) | 3.860*** | ||||
| Self-selected | 13 | 27 | 0.443 (−0.370 to 1.256) | 1.091 | −0.963 (−2.055 to 0.129) | −1.766 | ||
| % boys (continuous) | 58 | 119 | 0.491 (0.245–0.737) | 3.949*** | 0.000 (−0.009 to 0.010) | 0.096 | F (1, 117) = 0.009 | 0.924 |
| % low SES (continuous) | 20 | 41 | 0.233 (0.015–0.451) | 2.163* | −0.000 (−0.004 to 0.004) | −0.034 | F (1, 39) = 0.001 | 0.973 |
| % minorities (continuous) | 22 | 41 | 0.110 (0.007–0.213) | 2.164* | 0.001 (−0.001 to 0.003) | 0.986 | F (1, 39) = 0.972 | 0.330 |
| Mean age (continuous) | 61 | 123 | 0.548 (0.284–0.813) | 4.101*** | 0.039 (−0.090 to 0.169) | 0.601 | F (1, 121) = 0.361 | 0.549 |
| Intervention characteristics | ||||||||
| Component mindfulness | F (1, 121) = 1.644 | 0.202 | ||||||
| Yes (RC) | 21 | 31 | 0.360 (−0.020 to 0.740) | 1.874 | ||||
| No | 40 | 92 | 0.633 (0.341–0.926) | 4.281*** | 0.274 (−0.149 to 0.696) | 1.282 | ||
| Component relaxation | F (1, 121) = 3.288 | 0.072 | ||||||
| Yes (RC) | 25 | 42 | 0.828 (0.422–1.233) | 4.040*** | ||||
| No | 36 | 81 | 0.345 (0.008–0.682) | 2.025* | −0.483 (−1.010 to 0.044) | −1.813 | ||
| Component cognitive-behavioral | F (1, 121) = 2.613 | 0.109 | ||||||
| Yes (RC) | 28 | 78 | 0.772 (0.388–1.156) | 3.983*** | ||||
| No | 33 | 45 | 0.345 (−0.010 to 0.700) | 1.923 | −0.427 (−0.950 to 0.096) | −1.617 | ||
| Intensity (continuous) | 53 | 100 | 0.489 (0.222–0.756) | 3.632*** | −0.000 (−0.000 to 0.000) | −0.256 | F (1, 98) = 0.065 | 0.799 |
| Type of instructors | F (1, 110) = 2.445 | 0.121 | ||||||
| Specialized (RC) | 22 | 47 | 0.603 (0.271–0.934) | 3.601*** | ||||
| Other | 35 | 65 | 0.270 (0.010–0.53) | 2.056* | −0.333 (−0.754 to 0.089) | −1.564 | ||
| Program target | F (1, 121) = 0.089 | 0.765 | ||||||
| Direct (RC) | 53 | 111 | 0.559 (0.274–0.844) | 3.879*** | ||||
| Indirect | 8 | 12 | 0.440 (−0.289 to 1.170) | 1.196 | −0.118 (−0.902 to 0.665) | −0.299 | ||
N samples number of independent samples, N ES number of effect sizes, B0 mean effect size Cohen’s d,CI confidence interval, B1 estimated regression coefficient, t-values difference in mean d with zero, F-value omnibus test of regression coefficients, pp-value of omnibus test, RC reference category
*p < 0.05; **p < 0.01; ***p < 0.001
Study characteristics
The type of stress and timing of measurements moderated the effect, yielding significant effects for school stress, but not for social stress. Larger effects were found at follow-up compared to post-intervention.
Sample characteristics
The target group moderated the effect, demonstrating significant effects in selected student samples, but not in non-selected samples.
Intervention characteristics
No intervention characteristics moderated the effects.
Discussion
In order to prevent adverse adolescent development resulting from high levels of stress, it is important that heightened stress levels are addressed early on. Although various school-based intervention programs have been implemented to reduce adolescent stress, little is known on their overall effectiveness and factors influencing their effectiveness as previous reviews investigating stress reduction in adolescents through school-based intervention programs have generated conflicting and selective findings (Feiss et al. 2019; Kraag et al. 2006; Rew et al. 2014). In this comprehensive multilevel meta-analytic review, the extent to which school-based intervention programs are effective in reducing adolescent psychological stress was examined. In addition, study (e.g., publication status, study design), sample (e.g., age, target group) and intervention characteristics (e.g., intensity, components) were investigated as moderators of effectiveness. The current meta-analysis showed that school-based intervention programs had a moderate overall effect on reducing psychological stress. Significant program effects were only observed in selected student samples and not in community samples. Based on a subsample of studies with specific measures of school and social stress (instead of or in addition to general measures of stress), interventions were particularly effective in reducing school stress, not social stress. In addition, larger effects were found at follow-up compared to post-intervention.
The overall finding that school-based intervention programs are effective in reducing adolescent stress is consistent with the conclusion of Kraag et al. (2006). However, Kraag et al. (2006) only focused on universal interventions delivered to students from the general population, showing that this group benefits from school-based interventions. In contrast, based on the moderator analyses, the present study suggests that school-based interventions targeting psychological stress are not effective in community samples, and that only selected students benefit from such interventions. These contrasting findings may be explained by the difference between the two studies in age groups. In Kraag et al. (2006) participants were between 9 and 14 years, while in the current study participants were between 10 and 18 years old (with a mean age of 15 years). A difference in effectiveness of universal programs between age groups might be explained by the changing importance of the class environment with age. Specifically, while primary school students spend every day with the same teacher and classmates with whom they generally develop close relationships and feel comfortable (Coffey 2013), students in secondary school typically develop fewer close relationships, especially with their teachers (Tobbell and O’Donnell 2013). Consequently, the class environment in secondary school may be less safe to learn new skills than in primary school (i.e., for older compared to younger adolescents). This may result in smaller effectiveness of universal programs in secondary schools or older adolescents. Indeed, for a universal school-based intervention program targeting anxiety, it has been demonstrated that effectiveness was lower for secondary compared to primary school students (Barrett et al. 2005). Additionally, the contrasting findings may be explained by methodological differences between Kraag et al. (2006) and the current study. First, Kraag et al. (2006) included both psychological and physiological stress symptoms. Possibly, large positive effects in terms of physiological outcomes, which are not included in the present study, may explain the difference in findings. Second, Kraag and colleagues computed the effect sizes as the difference in mean change from pretest to posttest between the treatment and control group. This is in contrast with the current study that used group differences (i.e., between the intervention and control group) for both pre- and post-intervention assessments, thus correcting for pre-intervention differences between groups. The results of Kraag and colleagues could be influenced by baseline differences between the intervention and control groups. Third, Kraag et al. (2006) showed publication bias for the effect on stress symptoms, which suggests that their effect on stress reduction was overestimated.
Finding only significant effects for selected student samples compared to non-selected samples is in line with earlier research on school-based stress reduction programs (Feiss et al. 2019). Moreover, previous studies demonstrated that targeted programs were more effective than universal school-based depression programs (Werner-Seidler et al. 2017). This is probably associated with the difference in baseline symptoms between students of the general population and selected students, with selected students demonstrating higher levels of problem severity. Recent research demonstrated that program improvement is more evident in students with a high level of baseline problems (Stjerneklar et al. 2019). Moreover, selected students may be more motivated to actively participate in the intervention than students from the general population because they experience distress about their problems, resulting in larger program effects (Stice et al. 2009).
Based on a subsample of included studies, the results indicated that school-based intervention programs particularly affected school stress (e.g., study pressure, workload, worry on grades) and not social stress. A possible explanation is that adolescents can relate more to study-related stress and may apply their school-learned skills particularly in the context of study situations rather than social situations. Additionally, in the present study, three of five studies (i.e., 7 of 10 effect sizes) that measured school stress examined an intervention program containing a specific component on dealing with academic stress, while none of the three studies that measured social stress examined an intervention program with a specific component on dealing with social stress. The matching of a specific program component with a similar outcome variable might explain the observed larger effects for school stress. Yet, as perceived school-related stress affects many adolescents worldwide (Klinger et al. 2015), it is promising that school-based interventions have the potential to alleviate school-related stress. At the same time, given the limited number of studies and accompanying effect sizes with specific measures of school stress and social stress (i.e., 15 effect sizes), this finding should be interpreted with caution. To better understand the impact of intervention programs on stress reduction, future studies are recommended to include measures of stress that match the type of stress targeted in the intervention program studied.
Follow-up assessments yielded larger effects in terms of reductions in psychological stress than assessments at post-intervention. On the one hand, this might indicate a sleeper effect, i.e., improved longer term outcomes, which has been suggested for reductions in depressive symptoms that are only expected at a later stage when adolescents have experienced challenging situations (Spence and Shortt 2007). This sleeper effect may also apply to reductions in psychological stress following universal and selective interventions, as larger effects at follow-up were likely in both selected and non-selected student samples. Yet, recent meta-analyses demonstrated marginal evidence for a sleeper effect of psychotherapy interventions (Flückiger and Del Re 2017). On the other hand, finding larger effects at follow-up may be due to differences in sample composition between studies with and without follow-up assessments. In the current study, studies with follow-up assessments included more females and more selected student samples than studies with only post-intervention measurements (68% vs. 56% females and 63% vs. 42% selected samples), characteristics that have been associated with larger program effects (Stice et al. 2009).
Limitations
Several limitations need to be considered in this meta-analysis. First, although efforts were made to minimize publication bias by including gray literature and contacting authors of included studies for unpublished work, publication bias was indicated and might have inflated the overall estimates. Even though the validity of the available methods to detect publication bias is questioned for multilevel meta-analyses (Assink and Wibbelink 2016), making these specific results difficult to interpret, it is important to keep in mind that the program effects might be overestimated.
Second, extreme positive effect sizes (i.e., outliers) were observed. A sensitivity analysis was therefore conducted to account for their possible influence, by repeating the meta-analysis after the removal of outliers. Although the effect on psychological stress was smaller after correction, it remained significant. This indicates that the outliers moderately overestimated the overall effect. To further understand the impact of outliers, the included studies with extreme scores were examined. These studies were all based on selected rather than community student samples, had higher proportions of female participants and more often included follow-up assessments; factors that were found to be associated with larger effects in the present study and in previous research (Stice et al. 2009). As such, extreme scores seem to result from combinations of characteristics associated with larger effects.
Lastly, limited information was available for some of the study, sample, and intervention characteristics, including percentage of SES, percentage of minorities and program integrity. This limited the possibilities to conduct moderator analyses. It is important that future intervention studies report sufficient information about the study, sample, and intervention characteristics in order to be able to determine what works for whom in school-based intervention programs targeting stress.
Recommendations for Future Research
The present multilevel meta-analytic study evaluated the effectiveness of school-based intervention programs targeting adolescent psychological stress. In addition to new insights into the effectiveness of school-based intervention programs targeting psychological stress in adolescents, the current study generates recommendations for future research. It is recommended that future studies report information about program integrity (i.e., whether the intervention program was implemented as originally planned). As non-significant or negative results may be caused by incorrect program implementation, and not by an ineffective program, information about the program implementation is necessary to draw correct conclusions about the effectiveness of intervention programs. Furthermore, although no significant effects were found for universal interventions, contradicting earlier findings (Kraag et al. 2006), it is still important to examine them. Universal interventions reach larger groups of adolescents, including adolescents with (emerging) problems who do not search for care outside the school environment. It is of great importance to identify if adolescents with (emerging) problems benefit from universal interventions, or to examine how universal intervention programs can be adjusted to achieve the desired results for adolescents in need (e.g., improvement in functioning, effective referral). Overall, further research is necessary to identify the working mechanisms of effective school-based intervention programs targeting adolescent stress, for specific types of stress (e.g., school stress, social stress).
Conclusion
Previous reviews have investigated the reduction of adolescent stress through school-based intervention programs, however, these studies have yielded conflicting and selective findings. To overcome these limitations, the present multilevel meta-analytic study examined the effectiveness of school-based intervention programs in reducing psychological stress in adolescents and examined study, sample and intervention characteristics as moderators of effectiveness. The current study showed that school-based intervention programs were effective at reducing adolescent psychological stress, particularly for selected student samples. Furthermore, findings based on a small subsample of studies suggest that interventions were particularly effective in reducing school stress rather than social stress. Lastly, larger effects were found at follow-up compared to post-intervention, although this finding likely results from the sample composition of studies including follow-up assessments. Since heightened stress is an increasing mental health issue among adolescents (Walburg 2014), it is important that governments and schools are aware of the availability and potential of school-based intervention programs to reduce psychological stress in adolescents, and implement such programs in practice. This pertains particularly to interventions directed at students who self-select or enroll following a screening, as they benefit most from such interventions. School-based intervention programs aimed at reducing adolescent stress are scarce compared to programs aimed at reducing anxiety or depressive symptoms (Feiss et al. 2019). Yet, teaching adolescents skills to adequately deal with stress is of interest to both adolescents and schools, since addressing psychological stress through school-based intervention programs may prevent emerging mental health issues that likely also affect school performance.
Biographies
Amanda W. G. van Loon
is a doctoral student of Social and Behavioural Sciences at Utrecht University. Her major research interests include adolescence, intervention effectiveness and mental health.
Hanneke E. Creemers
is an Assistant Professor of Forensic Child and Youth Care Sciences at the University of Amsterdam. Her research focuses on the development of severe child and parenting problems and the effectiveness of interventions to reduce such problems.
Wieke Y. Beumer
is a research/student assistant of Social and Behavioural Sciences at Utrecht University. Her major research interests include child development, adolescence and sexuality.
Ana Okorn
is a research assistant of Social and Behavioural Sciences at Utrecht University. Her major research interests include early child development, parenting and family functioning.
Simone Vogelaar
is a doctoral student of Developmental and Educational Psychology at Leiden University. Her major research interests include adolescence, secondary education, and stress.
Nadira Saab
is an Associate Professor at ICLON Leiden University Graduate School of Teaching. Her major research interest includes educational science.
Anne C. Miers
is an Associate Professor of Developmental and Educational Psychology at Leiden University. Her major research interests include adolescence, social performance, and social anxiety.
P. Michiel Westenberg
is a Professor of Developmental and Educational Psychology at Leiden University. His major research interests include adolescence, secondary education, and stress.
Jessica J. Asscher
works at Utrecht University as full Professor Forensic Child and Youth Care Sciences and at the University of Amsterdam. Her research focuses on effectiveness of (judicial) youth and child care interventions and on the development of severe child rearing and child behavior problems.
Authors’ Contributions
A.W.G.L conceived of the study, participated in the design, data collection, and analysis for the study, and drafted the manuscript; H.E.C. conceived of the study, participated in its design and coordination and drafted the manuscript; W.Y.B. participated in data collection and interpretation and helped to draft the manuscript; A.O. participated in the data collection and interpretation and helped to draft the manuscript; S.V. participated in interpretation of the data and contributed to drafts of the manuscript; N.S. participated in interpretation of the data and contributed to drafts of the manuscript; A.C.M. participated in interpretation of the data and contributed to drafts of the manuscript; P.M.W. participated in interpretation of the data and contributed to drafts of the manuscript; J.J.A. conceived of the study, participated in its design and coordination and drafted the manuscript. All authors read and approved the final manuscript.
Funding
This work was supported by a grant from the Netherlands Organisation of Scientific Research (NWO), grant number 400.17.601, work package 3.
Data sharing and declaration
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.
Compliance with Ethical Standards
Conflict of Interest
The authors declare that they have no conflict of interest.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- *References marked with an asterisk indicate studies included in the meta-analysis.
- Assink M, Wibbelink CJM. Fitting three-level meta-analytic models in R: a step-by-step tutorial. The Quantitative Methods for Psychology. 2016;12(3):154–174. [Google Scholar]
- Barrett PM, Lock S, Farrell LJ. Developmental differences in universal preventive intervention for child anxiety. Clinical Child Psychology and Psychiatry. 2005;10(4):539–555. [Google Scholar]
- *Bennett K, Dorjee D. The impact of a Mindfulness-Based Stress Reduction course (MBSR) on well-being and academic attainment of sixth-form students. Mindfulness. 2016;7(1):105–114. [Google Scholar]
- *Bluth K, Campo RA, Pruteanu-Malinici S, Reams A, Mullarkey M, Broderick PC. A school-based mindfulness pilot study for ethnically diverse at-risk adolescents. Mindfulness. 2016;7(1):90–104. doi: 10.1007/s12671-014-0376-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Burckhardt R, Manicavasagar V, Batterham PJ, Hadzi-Pavlovic D. A randomized controlled trial of strong minds: a school-based mental health program combining acceptance and commitment therapy and positive psychology. Journal of School Psychology. 2016;57:41–52. doi: 10.1016/j.jsp.2016.05.008. [DOI] [PubMed] [Google Scholar]
- *Butzer B, LoRusso A, Shin SH, Khalsa SBS. Evaluation of yoga for preventing adolescent substance use risk factors in a middle school setting: a preliminary group-randomized controlled trial. Journal of Youth and Adolescence. 2017;46(3):603–632. doi: 10.1007/s10964-016-0513-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Campbell AJ, Lanthier RP, Weiss BA, Shaine MD. The impact of a schoolwide mindfulness program on adolescent well-being, stress, and emotion regulation: a nonrandomized controlled study in a naturalistic setting. Journal of Child and Adolescent Counseling. 2019;5(1):18–34. [Google Scholar]
- *Carreres-Ponsoda F, Escartí A, Llopis-Goig R, Cortell-Tormo JM. The effect of an out-of-school mindfulness program on adolescents’ stress reduction and emotional wellbeing. Cuadernos de Psicología del Deporte. 2017;17(3):35–44. [Google Scholar]
- *Carter, A. E. (2010). Evaluating the best of coping program: enhancing coping skills in adolescents. ProQuest Dissertations and Theses. University of Windsor, Windsor, Canada.
- Chappel AM, Suldo SM, Ogg JA. Associations between adolescents’ family stressors and life satisfaction. Journal of Child and Family Studies. 2014;23(1):76–84. [Google Scholar]
- Coffey A. Relationships: the key to successful transition from primary to secondary school? Improving Schools. 2013;16(3):261–271. [Google Scholar]
- Cohen, J. (1988). Statistical power analysis for the social sciences. Hillsdale, NJ: Erlbaum.
- Conley CS, Durlak JA, Shapiro JB, Kirsch AC, Zahniser E. A meta-analysis of the impact of universal and indicated preventive technology-delivered interventions for higher education students. Prevention Science. 2016;17(6):659–678. doi: 10.1007/s11121-016-0662-3. [DOI] [PubMed] [Google Scholar]
- *Cross D, Shaw T, Epstein M, Pearce N, Barnes A, Burns S, et al. Impact of the friendly schools whole-school intervention on transition to secondary school and adolescent bullying behaviour. European Journal of Education. 2018;53(4):495–513. [Google Scholar]
- *Da Silva, L.A., Doyenart, R., Henrique Salvan, P., Rodrigues, W., Felipe Lopes, J., Gomes, K. et al. (2019). Swimming training improves mental health parameters, cognition and motor coordination in children with attention deficit hyperactivity disorder. International Journal of Environmental Health Research, 1–9. 10.1080/09603123.2019.1612041. [DOI] [PubMed]
- *De Anda D. The evaluation of a stress management program for middle school adolescents. Child and Adolescent Social Work Journal. 1998;15(1):73–85. [Google Scholar]
- De Wolfe AS, Saunders AM. Stress reduction in sixth-grade students. Journal of Experimental Education. 1995;63(4):315–329. [Google Scholar]
- Dowling Katherine, Simpkin Andrew J., Barry Margaret M. A Cluster Randomized-Controlled Trial of the MindOut Social and Emotional Learning Program for Disadvantaged Post-Primary School Students. Journal of Youth and Adolescence. 2019;48(7):1245–1263. doi: 10.1007/s10964-019-00987-3. [DOI] [PubMed] [Google Scholar]
- Dupéré V, Leventhal T, Dion E, Crosnoe R, Archambault I, Janosz M. Stressors and turning points in high school and dropout. Review of Educational Research. 2015;85(4):591–629. [Google Scholar]
- Durlak JA, Weissberg RP, Dymnicki AB, Taylor RD, Schellinger KB. The impact of enhancing students’ social and emotional learning: a meta-analysis of school-based universal interventions. Child Development. 2011;82(1):405–432. doi: 10.1111/j.1467-8624.2010.01564.x. [DOI] [PubMed] [Google Scholar]
- Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000;56(2):455–463. doi: 10.1111/j.0006-341x.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- Duval S, Tweedie R. A nonparametric “Trim and Fill” method of accounting for publication bias in meta-analysis. Journal of the American Statistical Association. 2000;95(449):89–98. [Google Scholar]
- *Ebrahmimi M, Jaliabadi Z, Gholami Ghareh Chenagh KH, Amini F, Arkian F. Effectiveness of training of spiritual intelligence components on consequences of psychological and self-esteem of adolescents. Journal of Medicine and Life. 2015;8(4):87–92. [PMC free article] [PubMed] [Google Scholar]
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315:629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Eggert LL, Thompson EA, Herting JR, Nicholas LJ. Reducing suicide potential among high-risk youth: tests of a school-based prevention program. Suicide and Life-Threatening Behavior. 1995;25(2):276–296. [PubMed] [Google Scholar]
- Elbaum B, Vaughn S, Hughes MT, Moody SW. How effective are one-to-one tutoring programs in reading for elementary students at risk for reading failure? A meta-analysis of the intervention research. Journal of Educational Psychology. 2000;92(4):605–619. [Google Scholar]
- *Eslami AA, Rabiei L, Afzali SM, Hamidizadeh S, Masoudi R. The effectiveness of assertiveness training on the levels of stress anxiety, and depression of high school students. Iranian Red Crescent Medical Journal. 2016;18(1):1–10. doi: 10.5812/ircmj.21096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feiss R, Dolinger SB, Merritt M, Reiche E, Martin K, Yanes JA, et al. A systematic review and meta-analysis of school-based stress, anxiety, and depression prevention programs for adolescents. Journal of Youth and Adolescence. 2019;48(9):1668–1685. doi: 10.1007/s10964-019-01085-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flückiger C, Del Re AC. The sleeper effect between psychotherapy orientations: a strategic argument of sustainability of treatment effects at follow-up. Epidemiology and Psychiatric Sciences. 2017;26(4):442–444. doi: 10.1017/S2045796016000780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Fridrici M, Lohaus A. Stress-prevention in secondary schools: online- versus face-to-face-training. Health Education. 2009;109(4):299–313. [Google Scholar]
- *Fung J, Kim JJ, Jin J, Chen G, Bear L, Lau AS. A randomized trial evaluating school-based mindfulness intervention for ethnic minority youth: exploring mediators and moderators of intervention effects. Journal of Abnormal Child Psychology. 2019;47(1):1–19. doi: 10.1007/s10802-018-0425-7. [DOI] [PubMed] [Google Scholar]
- *Garcia C, Pintor J, Vazquez G, Alvarez-Zumarraga E. Project wings, a coping intervention for latina adolescents: a pilot study. Western Journal of Nursing Research. 2013;35(4):434–458. doi: 10.1177/0193945911407524. [DOI] [PubMed] [Google Scholar]
- Rhonda Goodman, David Newman Testing a Digital Storytelling Intervention to Reduce Stress in Adolescent Females. Storytelling, Self, Society. 2014;10(2):177. [Google Scholar]
- *Hampel P, Meier M, Kümmel U. School-based stress management training for adolescents: longitudinal results from an experimental study. Journal of Youth and Adolescence. 2008;37(8):1009–1024. [Google Scholar]
- Harris Alma, Chapman Christopher. IMPROVING SCHOOLS IN DIFFICULT CONTEXTS: TOWARDS A DIFFERENTIATED APPROACH. British Journal of Educational Studies. 2004;52(4):417–431. [Google Scholar]
- *Hiebert B, Kirby B, Jaknavorian A. School-based relaxation: attempting primary prevention. Canadian Journal of Counselling. 1989;23(3):273–287. [Google Scholar]
- Hofferth SL. Changes in American children’s time – 1997 to 2003. International Journal of Time Use Research. 2009;6(1):26–47. doi: 10.13085/eijtur.6.1.26-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Jamali S, Sabokdast S, Nia HS, Goudarzian AH, Beik S, Allen KA. The effect of life skills training on mental health of Iranian middle school students: a preliminary study. Iranian Journal of Psychiatry. 2016;11(4):269–273. [PMC free article] [PubMed] [Google Scholar]
- *Jellesma FC, Cornelis J. Mind magic: a pilot study of preventive mind-body-based stress reduction in behaviorally inhibited and activated children. Journal of Holistic Nursing. 2012;30(1):55–62. doi: 10.1177/0898010111418117. [DOI] [PubMed] [Google Scholar]
- *Jose B, Sajeena Effectiveness of yoga therapy on stress and concentration among students of selected schools in Kerala. Asian Journal of Nursing Education and Research. 2017;7(3):299–304. [Google Scholar]
- Kaplan DS, Liu RX, Kaplan HB. School related stress in early adolescence and academic performance three years later: the conditional influence of self expectations. Social Psychology of Education. 2005;8:3–17. [Google Scholar]
- Kaplan Robert M., Irvin Veronica L. Likelihood of Null Effects of Large NHLBI Clinical Trials Has Increased over Time. PLOS ONE. 2015;10(8):e0132382. doi: 10.1371/journal.pone.0132382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Khalsa SBS, Hickey-Schultz L, Cohen D, Steiner N, Cope S. Evaluation of the mental health benefits of yoga in a secondary school: a preliminary randomized controlled trial. Journal of Behavioral Health Services and Research. 2012;39(1):80–90. doi: 10.1007/s11414-011-9249-8. [DOI] [PubMed] [Google Scholar]
- *Kiselica MS, Baker SB, Thomas RN, Reedy S. Effects of stress inoculation training on anxiety, stress, and academic performance among adolescents. Journal of Counseling Psychology. 1994;41(3):335–342. [Google Scholar]
- Klinger DA, Freeman JG, Bilz L, Liiv K, Ramelow D, Sebok SS, et al. Cross-national trends in perceived school pressure by gender and age from 1994 to 2010. European Journal of Public Health. 2015;25(2):51–56. doi: 10.1093/eurpub/ckv027. [DOI] [PubMed] [Google Scholar]
- Knapp G, Hartung J. Improved tests for a random effects meta-regression with a single covariate. Statistics in Medicine. 2003;22(17):2693–2710. doi: 10.1002/sim.1482. [DOI] [PubMed] [Google Scholar]
- *Kraag G, Van Breukelen GJP, Kok G, Hosman C. “Learn young, learn fair”, a stress management program for fifth and sixth graders: longitudinal results from an experimental study. Journal of Child Psychology and Psychiatry and Allied Disciplines. 2009;50(9):1185–1195. doi: 10.1111/j.1469-7610.2009.02088.x. [DOI] [PubMed] [Google Scholar]
- Kraag G, Zeegers MP, Kok G, Hosman C, Abu-Saad HH. School programs targeting stress management in children and adolescents: a meta-analysis. Journal of School Psychology. 2006;44(6):449–472. [Google Scholar]
- Kraemer HC, Wilson GT, Fairburn CG, Agras WS. Mediators and moderators of treatment effects in randomized clinical trials. Archives of General Psychiatry. 2002;59(10):877–883. doi: 10.1001/archpsyc.59.10.877. [DOI] [PubMed] [Google Scholar]
- *Kuyken W, Weare K, Ukoumunne OC, Vicary R, Motton N, Burnett R, et al. Effectiveness of the mindfulness in schools programme: non-randomised controlled feasibility study. British Journal of Psychiatry. 2013;203(2):126–131. doi: 10.1192/bjp.bp.113.126649. [DOI] [PubMed] [Google Scholar]
- *Lai ESY, Kwok CL, Wong PWC, Fu KW, Law YW, Yip PSF. The effectiveness and sustainability of a universal school-based programme for preventing depression in Chinese adolescents: a follow-up study using quasi-experimental design. PLoS ONE. 2016;11(2):1–20. doi: 10.1371/journal.pone.0149854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Lang C, Feldmeth AK, Brand S, Holsboer-Trachsler E, Pühse U, Gerber M. Effects of a physical education-based coping training on adolescents’ coping skills, stress perceptions and quality of sleep. Physical Education and Sport Pedagogy. 2017;22(3):213–230. [Google Scholar]
- *Lau NS, Hue MT. Preliminary outcomes of a mindfulness-based programme for Hong Kong adolescents in schools: well-being, stress and depressive symptoms. International Journal of Children’s Spirituality. 2011;16(4):315–330. [Google Scholar]
- Lazarus RS. Psychological stress and the coping process. New York: McGraw-Hill; 1966. [Google Scholar]
- *Lee MJ, Oh W, Jang JS, Lee JY. A pilot study: horticulture-related activities significantly reduce stress levels and salivary cortisol concentration of maladjusted elementary school children. Complementary Therapies in Medicine. 2018;37:172–177. doi: 10.1016/j.ctim.2018.01.004. [DOI] [PubMed] [Google Scholar]
- *Livheim F, Hayes L, Ghaderi A, Magnusdottir T, Högfeldt A, Rowse J, et al. The effectiveness of acceptance and commitment therapy for adolescent mental health: Swedish and Australian pilot outcomes. Journal of Child and Family Studies. 2015;24(4):1016–1030. [Google Scholar]
- *Manjushambika R, Prasanna B, Vijayaraghavan R, Sushama B. Effectiveness of Jacobson’s progressive muscle relaxation (JPMR) on educational stress among school going adolescents. International Journal of Nursing Education. 2017;9(4):110. [Google Scholar]
- *Marsland AL, Gentile D, Hinze-Crout A, von Stauffenberg C, Rosen RK, Tavares A, et al. A randomized pilot trial of a school-based psychoeducational intervention for children with asthma. Clinical and Experimental Allergy. 2019;49(5):591–602. doi: 10.1111/cea.13337. [DOI] [PubMed] [Google Scholar]
- *Metz SM, Frank JL, Reibel D, Cantrell T, Sanders R, Broderick PC. The effectiveness of the learning to BREATHE program on adolescent emotion regulation. Research in Human Development. 2013;10(3):252–272. [Google Scholar]
- Moher David, Liberati Alessandro, Tetzlaff Jennifer, Altman Douglas G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Medicine. 2009;6(7):e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Noggle JJ, Steiner NJ, Minami T, Khalsa SBS. Benefits of yoga for psychosocial well-being in a US high school curriculum. Journal of Developmental & Behavioral Pediatrics. 2012;33(3):193–201. doi: 10.1097/DBP.0b013e31824afdc4. [DOI] [PubMed] [Google Scholar]
- *Norlander T, Moås L, Archer T. Noise and stress in primary and secondary school children: noise reduction and increased concentration ability through a short but regular exercise and relaxation program. School Effectiveness and School Improvement. 2005;16(1):91–99. [Google Scholar]
- Offord DR. Selection of levels of prevention. Addictive Behaviors. 2000;25(6):833–842. doi: 10.1016/s0306-4603(00)00132-5. [DOI] [PubMed] [Google Scholar]
- Petrosino A, Soydan H. The impact of program developers as evaluators on criminal recidivism: results from meta-analyses of experimental and quasi-experimental research. Journal of Experimental Criminology. 2005;1(4):435–450. [Google Scholar]
- *Puolakanaho A, Lappalainen R, Lappalainen P, Muotka JS, Hirvonen R, Eklund KM, et al. Reducing stress and enhancing academic buoyancy among adolescents using a brief web-based program based on acceptance and commitment therapy: a randomized controlled trial. Journal of Youth and Adolescence. 2019;48(2):287–305. doi: 10.1007/s10964-018-0973-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Quach D, Jastrowski Mano KE, Alexander K. A randomized controlled trial examining the effect of mindfulness meditation on working memory capacity in adolescents. Journal of Adolescent Health. 2016;58(5):489–496. doi: 10.1016/j.jadohealth.2015.09.024. [DOI] [PubMed] [Google Scholar]
- *Reiss, V. (2013). Effectiveness of mindfulness training on ratings of perceived stress, mindfulness and well-being of adolescents enrolled in an international baccalaureate diploma program. ProQuest Dissertations and Theses. The University of Arizona, Tucson, USA.
- *Rentala, S., Lau, B. H., Aladakatti, R., & Thimmajja, S. G. (2019). Effectiveness of holistic group health promotion program on educational stress, anxiety, and depression among adolescent girls–A pilot study. Journal of Family Medicine and Primary Care, 8, 1082–1089. [DOI] [PMC free article] [PubMed]
- Resurrección DM, Salguero JM, Ruiz-Aranda D. Emotional intelligence and psychological maladjustment in adolescence: a systematic review. Journal of Adolescence. 2014;37(4):461–472. doi: 10.1016/j.adolescence.2014.03.012. [DOI] [PubMed] [Google Scholar]
- Rew L, Johnson K, Young C. A systematic review of interventions to reduce stress in adolescence. Issues in Mental Health Nursing. 2014;35(11):851–863. doi: 10.3109/01612840.2014.924044. [DOI] [PubMed] [Google Scholar]
- Romeo RD. The teenage brain: the stress response and the adolescent brain. Current Directions in Psychological Science. 2013;22(2):140–145. doi: 10.1177/0963721413475445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosenthal R. The file drawer problem and tolerance for null results. Psychological Bulletin. 1979;86(3):638–641. [Google Scholar]
- *Ruiz-Aranda D, Salguero JM, Cabello R, Palomera R, Berrocal PF. Can an emotional intelligence program improve adolescents’ psychosocial adjustment? Results from the intemo project. Social Behavior and Personality: An International Journal. 2012;40(8):1373–1379. [Google Scholar]
- Schaufeli WB, Leiter MP, Maslach C. Burnout: 35 years of research and practice. Career Development International. 2009;14(3):204–220. [Google Scholar]
- *Sibinga, E. M. S., Perry-Parrish, C., Chung, S. E., Johnson, S. B., Smith, M., & Ellen, J. M. (2013). School-based mindfulness instruction for urban male youth: A small randomized controlled trial. Preventive medicine, 57(6), 799–801. [DOI] [PubMed]
- *Sibinga EMS, Webb L, Ghazarian SR, Ellen JM. School-based mindfulness instruction: an RCT. Pediatrics. 2016;137(1):1–8. doi: 10.1542/peds.2015-2532. [DOI] [PubMed] [Google Scholar]
- *Silbert, K. L., & Berry, G. L. (1991). Psychological effects of a suicide prevention unit on adolescents’ level of stress, anxiety and hopelessness: implications for counselling psychologists. Counselling Psychology Quarterly, 4(1), 45–58.
- *Singhal M, Manjula M, Vijay Sagar KJ. Development of a school-based program for adolescents at-risk for depression in India: results from a pilot study. Asian Journal of Psychiatry. 2014;10:56–61. doi: 10.1016/j.ajp.2014.03.011. [DOI] [PubMed] [Google Scholar]
- *Singhal M, Munivenkatappa M, Kommu JVS, Philip M. Efficacy of an indicated intervention program for Indian adolescents with subclinical depression. Asian Journal of Psychiatry. 2018;33:99–104. doi: 10.1016/j.ajp.2018.03.007. [DOI] [PubMed] [Google Scholar]
- Snyder Hannah R., Young Jami F., Hankin Benjamin L. Chronic Stress Exposure and Generation Are Related to the P-Factor and Externalizing Specific Psychopathology in Youth. Journal of Clinical Child & Adolescent Psychology. 2017;48(2):306–315. doi: 10.1080/15374416.2017.1321002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Solar II, E. L. (2013). The effects of mindfulness meditation on adolescents with high-incidence disabilities. ProQuest Dissertations and Theses. George Mason University, Fairfax, USA.
- Spence SH, Shortt AL. Research review: Can we justify the widespread dissemination of universal, school-based interventions for the prevention of depression among children and adolescents? Journal of Child Psychology and Psychiatry and Allied Disciplines. 2007;48(6):526–542. doi: 10.1111/j.1469-7610.2007.01738.x. [DOI] [PubMed] [Google Scholar]
- Stephan SH, Weist M, Kataoka S, Adelsheim S, Mills C. Transformation of children’s mental health services: The role of school mental health. Psychiatric Services. 2007;58(10):1330–1338. doi: 10.1176/ps.2007.58.10.1330. [DOI] [PubMed] [Google Scholar]
- Stice E, Shaw H, Bohon C, Marti CN, Rohde P. A meta-analytic review of depression prevention programs for children and adolescents: factors that predict magnitude of intervention effects. Journal of Consulting and Clinical Psychology. 2009;77(3):486–503. doi: 10.1037/a0015168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stjerneklar S, Hougaard E, Thastum M. Guided internet-based cognitive behavioral therapy for adolescent anxiety: predictors of treatment response. Internet Interventions. 2019;15:116–125. doi: 10.1016/j.invent.2019.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suter JC, Bruns EJ. Effectiveness of the wraparound process for children with emotional and behavioral disorders: a meta-analysis. Clinical Child and Family Psychology Review. 2009;12(4):336–351. doi: 10.1007/s10567-009-0059-y. [DOI] [PubMed] [Google Scholar]
- *Terjestam Y. Stilness at school: well-being after eight weeks of meditation-based practice in secondary school. Psyke & Logos. 2011;32:105–116. [Google Scholar]
- *Terjestam Y, Bengtsson H, Jansson A. Cultivating awareness at school. Effects on effortful control, peer relations and well-being at school in grades 5, 7, and 8. School Psychology International. 2016;37(5):456–469. [Google Scholar]
- *Terjestam Y, Jouper J, Johansson C. Effects of scheduled qigong exercise on pupils’ well-being, self-image, distress, and stress. The Journal of Alternative and Complementary Medicine. 2010;16(9):939–944. doi: 10.1089/acm.2009.0405. [DOI] [PubMed] [Google Scholar]
- Thomas BH, Ciliska D, Dobbins M, Micucci S. A process for systematically reviewing the literature: providing the research evidence for public health nursing interventions. Worldviews on Evidence-Based Nursing. 2004;1(3):176–184. doi: 10.1111/j.1524-475X.2004.04006.x. [DOI] [PubMed] [Google Scholar]
- Tobbell J, O’Donnell VL. The formation of interpersonal and learning relationships in the transition from primary to secondary school: students, teachers and school context. International Journal of Educational Research. 2013;59:11–23. [Google Scholar]
- Van den Noortgate W, López-López JA, Marín-Martínez F, Sánchez-Meca J. Three-level meta-analysis of dependent effect sizes. Behavior Research Methods. 2013;45(2):576–594. doi: 10.3758/s13428-012-0261-6. [DOI] [PubMed] [Google Scholar]
- *Van der Gucht K, Takano K, Raes F, Kuppens P. Processes of change in a school-based mindfulness programme: cognitive reactivity and self-coldness as mediators. Cognition and Emotion. 2018;32(3):658–665. doi: 10.1080/02699931.2017.1310716. [DOI] [PubMed] [Google Scholar]
- van der Stouwe Trudy, Asscher Jessica J., Stams Geert Jan J.M., Deković Maja, van der Laan Peter H. The effectiveness of Multisystemic Therapy (MST): A meta-analysis. Clinical Psychology Review. 2014;34(6):468–481. doi: 10.1016/j.cpr.2014.06.006. [DOI] [PubMed] [Google Scholar]
- *Van Ryzin MJ, Roseth CJ. Cooperative learning in middle school: a means to improve peer relations and reduce victimization, bullying, and related outcomes. Journal of Educational Psychology. 2018;110(8):1192–1201. doi: 10.1037/edu0000265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walburg V. Burnout among high school students: a literature review. Children and Youth Services Review. 2014;42:28–33. [Google Scholar]
- Werner-Seidler A, Perry Y, Calear AL, Newby JM, Christensen H. School-based depression and anxiety prevention programs for young people: a systematic review and meta-analysis. Clinical Psychology Review. 2017;51:30–47. doi: 10.1016/j.cpr.2016.10.005. [DOI] [PubMed] [Google Scholar]
- White LS. Reducing stress in school-age girls through mindful yoga. Journal of Pediatric Health Care. 2012;26(1):45–56. doi: 10.1016/j.pedhc.2011.01.002. [DOI] [PubMed] [Google Scholar]
- Wilson, D. B. (n.d.). Practical meta-analysis effect size calculator [Online calculator]. Retrieved from https://www.campbellcollaboration.org/research-resources/effect-size-calculator.html.
- *Zafar H, Khalily MT. Didactic therapy for management of stress and co-morbid symptoms of depression and anxiety in Pakistani adolescents. Pakistan Journal of Psychological Research. 2015;30(1):131–149. [Google Scholar]
- Zins JE, Bloodworth MR, Weissberg RP, Walberg HJ. The scientific base linking social and emotional learning to school success. Journal of Educational and Psychological Consultation. 2007;17(2–3):191–210. [Google Scholar]
- Zoogman S, Goldberg SB, Hoyt WT, Miller L. Mindfulness interventions with youth: a meta-analysis. Mindfulness. 2015;6(2):290–302. [Google Scholar]