

Abstract
Background
Overactive bladder (OAB) is common and morbid. Medication and diagnosis claims may be specific, but lack sensitivity to identify patients with overactive bladder. We used an “electronic health record (EHR) phenotype” to identify cases and describe treatment choices and anticholinergic burden for OAB.
Methods
We conducted a retrospective cohort study in a large, integrated health delivery system between July 2011 and June 2012 (2-year follow-up). We examined care from primary care and specialty clinics, medication and procedure use, and anticholinergic burden for each patient.
Results
There were 7362 patients with an EHR OAB phenotype; 50% of patients were > 65 years old, 74% were female, and 83% were white. The distribution of care included primary care physician (PCP)/specialty co-management (25% of patients); PCP care only (18%); urology only (13%); or some other combination of specialty care (33%). Only 40% of patients were prescribed at least 1 OAB medication during the study. The mean duration of prescribed medication was 1.5 months (95% confidence interval [CI], 1.4 to 1.6 months; range, < 1 month to 24 months). Independent predictors of receipt of an OAB medication included increasing age (odds ratio [OR], 1.4 for every 10 years; 95% CI, 1.4 to 1.5), women (OR, 1.6 compared with men; 95% CI, 1.4 to 1.8), diabetes (OR, 1.3; 95% CI, 1.1 to 1.5), and certain sources of care compared with PCP-only care: PCP/specialty co-management (OR, 1.8; 95% CI, 1.5 to 2.0), urology (OR, 2.2; 95% CI, 1.8 to 2.6), and multiple specialists (OR, 1.4; 95% CI, 1.2 to 1.8). Very few patients received other treatments: biofeedback (< 1%), onabotulinumtoxinA (2%), or sacral nerve stimulation (1%). Patients who received OAB medications had significantly higher anticholinergic burden than patients who did not (anticholinergic total standardized daily dose, 125 versus 46; P < .001).
Conclusions
Although OAB is common and morbid, in a longitudinal study using an EHR OAB phenotype 40% of patients were treated with OAB medication and only briefly.
Keywords: Antimuscarinics, Anticholinergic burden, Electronic health records, Integrated delivery system, Medication and procedure use, Overactive bladder, Overactive bladder syndrome, Primary and specialty care, Urgency, Urinary incontinence
Background
Overactive bladder (OAB) is defined by the International Continence Society (ICS) as a symptom syndrome defined by urinary urgency, frequency, and nocturia, with or without incontinence [1–3]. OAB is common and its prevalence can vary widely depending on the patient population and disease definition, affecting 7–27% of men and 9–43% of women [1, 2]. OAB is associated with impaired sleep quality, depression, falls, fractures, social isolation, and worse quality of life [1, 3].
OAB can be difficult-to-treat in part because of the anticholinergic side effects of the most commonly prescribed medications. Recently, anticholinergic medications, including OAB medications, have been implicated in the development of cognitive impairment and dementia [4, 5].
OAB is underreported by patients and poorly recognized in primary care [6]. OAB may also be under-recognized by specialists in integrated health systems. Prior studies have been limited by use of claims or prescribing data to identify OAB patients, which may focus only on highly-specified patient populations who have multiple visits for OAB, an explicit diagnosis of OAB, or OAB medication prescriptions [7–9]. Such methods may misclassify patients who present with the complex of symptoms that define OAB. In addition, prior studies have not described care of patients with OAB within an integrated delivery system utilizing electronic health records (EHRs), in which patients could receive care from some combination of primary and specialty care, including urology, gynecology, and urogynecology.
EHR-based disease phenotypes have the potential to more sensitively identify patient cohorts [10, 11]. Based on an initial chart review, modification, and refinement, EHR phenotypes use a mix of coded data and free-text criteria to identify patients with target conditions. EHR phenotypes are particularly useful for conditions like OAB that do not have reliable, well-defined diagnostic criteria (e.g., simply using International Statistical Classification of Diseases and Related Health Problems-9 [ICD-9] codes for OAB).
The aim of this study was to identify patients with an EHR OAB phenotype and conduct a health system-based, longitudinal cohort assessment to describe care by different specialties, medication use, and procedures, as well as to assess the anticholinergic burden of patients who did and did not receive OAB medications.
Methods
Setting, data source, and overview
Partners HealthCare is an integrated health delivery system that provides primary and specialty care in Eastern Massachusetts. The system has eight acute care hospitals including Brigham and Women’s Hospital and Massachusetts General Hospital. Partners HealthCare includes approximately 1000 primary care physicians (PCPs) and about 5500 specialists. All Partners HealthCare entities share a common data infrastructure.
Because of limitations of prior methods of identifying patients with OAB, we developed an OAB EHR phenotype through identification of coded fields, a pilot chart review, a definitive chart review, and EHR model training. We retrospectively identified Partners HealthCare patients using an OAB EHR phenotype – a combination of structured variables and natural language processing of free text – who met criteria for OAB between July 1, 2011 and June 30, 2012 [10, 11]. We followed patients from their index visit – the date on which they met criteria for OAB – for 2 years. We examined visit, medication, and utilization data (Fig. 1).
Fig. 1.
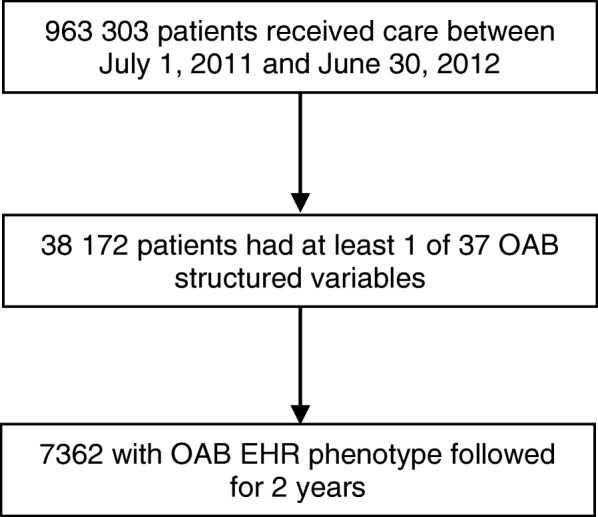
Patient Flow. OAB, overactive bladder; EHR, electronic health record
EHR OAB phenotype
Identification of OAB-related coded fields
The development of the OAB EHR phenotype began with two clinician investigators (JAL, KRL), with input from the rest of the study team, identifying 37 ICD-9 diagnosis codes, medications, or problem list entries that could be potentially associated with OAB (Supplementary Table 1). ICD-9 codes included “hypertonicity of bladder,” “retention of urine,” “urgency of urination,” and others. Problem list entries included “bladder dysfunction,” “hyperactive bladder,” “urgent desire to urinate,” and others. We designated each of the 37 variables as either “highly likely” to be associated with a patient who had a diagnosis of OAB or “likely” to be associated with a diagnosis of OAB.
Pilot chart review
To determine the most efficient sample size for a larger chart review, JAL and KRL conducted a pilot chart review of 20 charts with a highly likely code, 20 charts with only a likely code, and 20 charts with no OAB-related code. On chart review, highly likely codes had a positive predictive value of 70%, likely codes had a positive predictive value of 35%, and, for charts with no OAB-related code a PPV of 0%. Based on these estimates for the PPV of highly-likely and likely codes and the distribution of highly-likely and likely codes, we determined that, a sample size of 729 reviewed charts would yield a 95% CI (i.e., the 95% CI for the PPV would be at most 10% wide). We subsequently identified patients 18 years or older who had any of these 37 diagnosis codes, medications, or problem list entries.
Definitive chart review
Three physician reviewers examined a random sample of 729 charts to identify those which met pre-specified, database collected and calculated criteria, consistent with ICS and International Consultation on Incontinence definitions, for a clinical diagnosis of OAB [12]. For the chart review, we created four phenotype classifications (definite, probable, possible, and not OAB) based on a combination of features including the results of urodynamic testing or, in the absence of urodynamic testing, documentation in patient notes. Patients were considered to have definite OAB if they had urodynamic testing results of detrusor hyperreflexia, detrusor instability, uninhibited contraction, or equivalent language. For the vast majority of patients who did not have urodynamic testing, we required chart documentation of 3 symptoms: 1) urinary urgency in the absence of urinary tract infection, history of genitourinary procedure within the past 90 days, or other obvious pathology, 2) urinary frequency (voiding eight or more times or an unknown quantity per day), and 3) nocturia (awakening two or more times or an unknown number to void). We defined urgency as a sudden, compelling need to void which is difficult to defer. A patient was classified as having definite OAB if they had urgency, frequency, and nocturia; probable OAB if they had urgency and frequency; possible OAB if they had only urgency; and not OAB if they had none of the symptoms or had an alternative cause of symptoms. If a urinalysis showed five or more white blood cells per high power field, we required a negative culture to rule out alternate cause of urgency.
Reviewers also responded to the prompt, “Do you agree or disagree with the assigned category of the OAB diagnosis?” using a 4-point Likert scale (completely agree, partially agree, partially disagree, completely disagree). We considered OAB cases as those which were classified as definite OAB with which the reviewer completely agreed; definitely OAB with which the reviewer partially agreed; or classified as probable OAB with which the reviewer completely agreed.
OAB EHR phenotype based on coded fields and free-text
To develop our OAB EHR phenotype, we randomly selected 70% of patients classified by chart review for training and held the remaining 30% for the testing set. We trained an L1-regularized (Least Absolute Shrinkage and Selector Operator, LASSO) [13, 14] logistic regression using the gold standard labels assigned from chart review (1 for OAB; 0 otherwise) as the dependent variable and the coded and free-text elements in the EHR as model features. We incorporated free-text from outpatient clinical notes into our phenotyping algorithm via natural language processing. We aggregated all outpatient clinical notes into a single document for each patient and employed a “bag-of-words” (BOW) representation.
As determined a priori, we set the predictive probability of the LASSO model to maximize the sum of sensitivity and specificity (NLP-only model: sensitivity, 48%; specificity, 84%; c-statistic, 0.64; NPV, 89%; PPV, 37%). For the final predictive model, because we intended to examine medications as an outcome, we omitted medications as a coded field, sacrificing some PPV. The final model (Supplementary Table 2) had a sensitivity of 54%, specificity of 80%, c-statistic of 0.72, negative predictive value of 83%, and, consistent with our pilot and final chart review, a PPV of 54% (see Discussion).
Data extraction and analysis
For cases that met the EHR phenotype definition of OAB, we extracted sociodemographic information including age, sex, race/ethnicity, primary language, insurance type, and marital status. Sociodemographic information was collected during patient registration at Partners HealthCare sites. In addition, we used the EHR problem list and diagnosis entries to determine if the patient had moderate-to-severe chronic kidney disease; chronic obstructive pulmonary disease; congestive heart failure; or diabetes mellitus (Supplementary Table 3). We also examined two relative contraindications to anticholinergic treatment: glaucoma and dementia.
We classified patients according to what specialties cared for the patient (source of care) over the following 2 years. We classified patients’ source of care as PCP only; a single “OAB-related specialist,” including urology, gynecology, or urogynecology; a combination of OAB-related specialists; co-management by a PCP and any OAB-related specialists; or other (ie, patients who did not receive care from a PCP, urologist, gynecologist, or urogynecologist).
We identified the first OAB-related medication that patients received during follow-up, including darifenacin, fesoterodine, flavoxate, hyoscyamine, imipramine, mirabegron, oxybutynin, solifenacin, tolterodine, and trospium. Among patients who received an OAB medication, we measured the number of different medications prescribed to individual patients over 2 years of follow-up. In addition, we measured the total number of months of medication each patient was prescribed and calculated the average duration of medication prescription coverage among patients who received any medication. We used Current Procedural Terminology (CPT) codes to identify procedures including biofeedback, onabotulinumtoxinA injections, and sacral nerve stimulation (Supplementary Table 4).
We measured anticholinergic burden of OAB and non-OAB medications using the method of Gray and colleagues [5, 15]. Briefly, we multiplied the medication strength by the number of units of medication dispensed to calculate a total medication dose for each anticholinergic medication, the anticholinergic total standardized daily dose (TSDD). We then converted the total dose for each medication into a standardized daily dose by dividing by the minimum reported effective dose of each medication. We then added the standardized daily dose across medications to calculate a TSDD for anticholinergic medications and examined the difference in anticholinergic TSDD between those who did and did not receive OAB medications.
Statistical analysis
We described basic associations using proportions. We compared proportions – including sociodemographic, clinical, and treatment difference between men and women – using the chi-squared test. To examine independent predictors of receipt of OAB medications, we used multivariable logistic regression. We modeled age in decades and omitted insurance status, which was strongly colinear with age. Language was also omitted, as it was strongly colinear with race/ethnicity. We used the linear trend test to assess the relationship between number of OAB medications prescribed during the study period and increasing TSDD. For all analyses we used SAS (version 9.4, Cary, NC) and considered P values < .05 significant.
Results
Cohort derivation and characteristics
Of the 963,303 patients with EHR records during the study period, 38,172 had at least one coded variable that was potentially related to OAB. Of these, 7362 patients had an OAB EHR phenotype without medications as predictors. Of these patients, 50% were over 65 years old, 74% were female, and 83% were white (Table 1). In total, 45% of patients had private insurance, 47% had Medicare, and 5% had Medicaid. Comorbid conditions included chronic obstructive pulmonary disease (20%), diabetes (17%), congestive heart failure (9%), chronic kidney disease (4%), glaucoma (3%), and dementia (3%).
Table 1.
Cohort Characteristics by Sex
| Characteristic | Overall (n = 7362) | Female (n = 5417) | Male (n = 1945) | P value |
|---|---|---|---|---|
| No. (column %) | ||||
| Less than 65 years old | 3646 (50) | 2797 (52) | 849 (44) | < .001 |
| 65 years old or older | 3716 (50) | 2620 (48) | 1096 (56) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Race/ethnicity | ||||
| White/Caucasian | 6103 (83) | 4516 (83) | 1587 (82) | .012 |
| Black/African American | 338 (5) | 233 (4) | 105 (5) | |
| Hispanic/Latino | 270 (4) | 211 (4) | 59 (3) | |
| Asian/Pacific Islander | 125 (2) | 82 (2) | 43 (2) | |
| Other/unknown | 526 (7) | 375 (7) | 151 (8) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Language | ||||
| English | 6704 (91) | 4933 (91) | 1771 (91) | .011 |
| Spanish | 310 (4) | 245 (5) | 65 (3) | |
| Other/unknown | 348 (5) | 239 (4) | 109 (6) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Insurance | ||||
| Private | 3344 (45) | 2489 (46) | 855 (44) | < .001 |
| Medicare | 3428 (47) | 2467 (46) | 961 (49) | |
| Medicaid | 362 (5) | 272 (5) | 90 (5) | |
| None | 228 (3) | 189 (3) | 39 (2) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Marital status | ||||
| Married/partnered | 3522 (48) | 2417 (45) | 1105 (57) | < .001 |
| Single | 1591 (22) | 1166 (22) | 425 (22) | |
| Widowed | 979 (13) | 865 (16) | 114 (6) | |
| Divorced/separated | 757 (10) | 618 (11) | 139 (7) | |
| Other/unknown | 513 (7) | 351 (6) | 162 (8) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Comorbidities | ||||
| Chronic kidney disease (moderate/severe) | 293 (4) | 175 (3) | 118 (6) | < .001 |
| No chronic kidney disease (moderate/severe) | 7069 (96) | 5242 (97) | 1827 (94) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Chronic obstructive pulmonary disease | 1504 (20) | 1169 (22) | 335 (17) | < .001 |
| No chronic obstructive pulmonary disease | 5858 (80) | 4248 (78) | 1610 (83) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Congestive heart failure | 694 (9) | 439 (8) | 255 (13) | < .001 |
| No congestive heart failure | 6668 (91) | 4978 (92) | 1690 (87) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Dementia | 236 (3) | 154 (3) | 82 (4) | .0032 |
| No dementia | 7126 (97) | 5263 (97) | 1863 (96) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Diabetes mellitus | 1223 (17) | 815 (15) | 408 (21) | < .001 |
| No diabetes mellitus | 6139 (83) | 4602 (85) | 1537 (79) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Glaucoma | 249 (3) | 197 (4) | 52 (3) | .044 |
| No glaucoma | 7113 (97) | 5220 (96) | 1893 (97) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
Sources of care
The distribution of care included primary care/specialty co-management (for 25% of patients); primary care only (17%); urology only (13%); or another combination of specialty care (33%; Table 2). Men were more likely to get care from urologists and essentially did not receive care from gynecologists or urogynecologists.
Table 2.
Patterns of Care by Sex
| Characteristic | Overall (n = 7362) | Female (n = 5417) | Male (n = 1945) | P value |
|---|---|---|---|---|
| No. (column %) | ||||
| Source of care | ||||
| Co-managed* | 1828 (25) | 1366 (25) | 462 (24) | < .001 |
| PCP only† | 1288 (17) | 1021 (19) | 267 (14) | |
| Urologist only‡ | 938 (13) | 374 (7) | 564 (29) | |
| Gynecologist only§ | 195 (3) | 195 (4) | 0 (0) | |
| Urogynecologist only║ | 76 (1) | 76 (1) | 0 (0) | |
| Urologist, gynecologist, and/or urogynecologist only¶ | 637 (9) | 633 (12) | 4 (0) | |
| Other# | 2400 (33) | 1752 (32) | 648 (33) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Initial medication | ||||
| Darifenacin | 100 (1) | 75 (1) | 25 (1) | .006 |
| Fesoterodine | 55 (1) | 41 (1) | 14 (1) | |
| Flavoxate | 9 (0) | 9 (0) | 0 (0) | |
| Hyoscyamine | 83 (1) | 65 (1) | 18 (1) | |
| Imipramine | 133 (2) | 103 (2) | 30 (2) | |
| Mirabegron | 27 (0) | 20 (0) | 7 (0) | |
| Oxybutynin | 1545 (21) | 1184 (22) | 361 (19) | |
| Solifenacin | 428 (6) | 324 (6) | 104 (5) | |
| Tolterodine | 485 (7) | 359 (7) | 126 (6) | |
| Trospium | 91 (1) | 75 (1) | 16 (1) | |
| None | 4406 (60) | 3162 (58) | 1244 (64) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Treatment | ||||
| Biofeedback | 10 (0) | 9 (0) | 1 (0) | .24 |
| No biofeedback | 7352 (100) | 5408 (100) | 1944 (100) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| OnabotulinumtoxinA | 171 (2) | 131 (2) | 40 (2) | .36 |
| No onabotulinumtoxinA | 7191 (98) | 5286 (98) | 1905 (98) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Sacral nerve stimulation | 74 (1) | 56 (1) | 18 (1) | .68 |
| No sacral nerve stimulation | 7288 (99) | 5361 (99) | 1927 (99) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
| Bladder augmentation | 0 (0) | 0 (0) | 0 (0) | NA |
| No bladder augmentation | 7362 (100) | 5417 (100) | 1945 (100) | |
| Total | 7362 (100) | 5417 (100) | 1945 (100) | |
NA, not applicable; PCP, primary care physician.
*Patients with a PCP who also received care from a urologist, gynecologist, and/or urogynecologist
†Patients with a PCP who did not receive care from a urologist, gynecologist, or urogynecologist
‡Patients with a urologist who did not receive care from a PCP, gynecologist, or urogynecologist
§Patients with a gynecologist who did not receive care from a PCP, urologist, or urogynecologist
║Patients with a urogynecologist who did not receive care from a PCP, gynecologist, or urologist
¶Patients with a urologist, gynecologist, and/or urogynecologist (at least two of three) who did not receive care from a PCP
#Patients who did not receive care from a PCP, urologist, gynecologist, or urogynecologist but received care from other specialists
Medication use, classes, and persistence
Only 40% of patients received an OAB-related medication in the 2 years of follow-up. The most commonly prescribed medications were oxybutynin, tolterodine, and solifenacin. Patients who were co-managed by PCPs and a specialist had the highest medication receipt rate (48%), followed by patients seen by urogynecologists (47%), urologists (45%), a combination of specialists (41%), PCPs only (38%), other specialties (34%), and gynecologists only (30%) (p < .001); Supplementary Table 5 and Supplementary Table 6). Among patients with contraindications for anticholinergic treatment, 54% (127/236) of those with dementia and 46% (115/249) of those with glaucoma received OAB medication.
Among patients who received medications, the median number of OAB-related medications received in the subsequent 2 years was two (interquartile range, two to three; range one to seven). Among patients who received medication, the average duration of prescribed medication was 1.5 months (95% confidence interval [CI] 1.4–1.6 months; range, < 1–24 months).
In multivariable modeling, independent predictors of receipt of an OAB medication were increasing age (odds ratio [OR] 1.4 for every 10 years; 95% CI, 1.4–1.5), female sex (OR, 1.6 compared with male; 95% CI, 1.4–1.8), other marital status (OR, 0.5 compared with married; 95% CI, 0.4–0.6), widowed (OR, 0.7 compared with married; 95% CI, 0.6–0.9), diabetes (OR, 1.3; 95% CI, 1.1–1.5), and certain sources of care compared with PCP-only care: PCP/specialist co-management (OR, 1.8; 95% CI, 1.5–2.0), multiple specialists (OR, 1.4; 95% CI, 1.2–1.8), urogynecology (OR, 1.9; 95% CI, 1.2–3.1), and urology (OR, 2.2; 95% CI, 1.8–2.6). Marginally significant predictors of OAB medication prescribing were Hispanic race/ethnicity (OR, 1.3 compared with whites; 95% CI, 1.0–1.7) and chronic obstructive pulmonary disease (OR, 1.1; 95% CI, 1.0–1.3).
Other treatments
Few patients received other treatments of any type. Less than 1% of patients received biofeedback, 2% of patients received onabotulinumtoxinA, and 1% of patients received sacral nerve stimulation.
Anticholinergic burden
Over the 2-year follow-up, patients who received OAB medications had significantly higher anticholinergic burden than patients who did not (anticholinergic TSDD, 125 versus 46; P < .001). An increasing number of OAB medications were associated with a linear increase in anticholinergic burden: for each OAB medication prescribed there was an increase in anticholinergic TSDD of 31 (95% CI, 26–36; P < .001 for the increasing trend in anticholinergic burden).
Discussion
In this 2-year longitudinal study of patients identified using an EHR phenotype for OAB, only 40% of patients were prescribed an OAB medication. Of patients who received an OAB medication, the mean number of medications prescribed was two and the average duration of prescribing was only 1.5 months. Use of non-medication treatments, like onabotulinumtoxinA, was infrequent, perhaps as it only received US Food and Drug Administration approval for treatment of OAB in adults not responsive to anticholinergics in 2013.
Compared with our EHR phenotyping approach, studies that identified patients based on medication or diagnosis claims had slightly longer, but still short, treatment durations with high discontinuation rates. Studies using only medication claims – which, by design, could not measure the rate of medication prescribing – generally found longer durations of treatment, generally ranging from 2 to 6 months [8, 16–18]. One study relying on a single diagnosis code to define OAB patients had medication fill rates over the course of 1 year of 24% [7]. Another study using diagnosis codes had a same-visit, EHR medication prescribing rate of 17% [19]. A third study relying on both diagnosis codes and a medication prescription found that 92% of patients discontinued or switched their first anticholinergic medication over 24 months, with a mean time to discontinuation or switch of 5 months [9]. A systematic review of OAB medication use found that 43–83% of patients discontinue anticholinergics in the first 30 days; up to half of patients may have experienced “primary nonadherence,” in which patients never fill their first prescription [20, 21].
Failure to recognize, address, and treat OAB may leave patients at risk for complications, adverse effects, and with worse quality of life. Guidelines support lifestyle modifications as primary therapy but pharmacologic therapy may be underutilized. Unfortunately, OAB patients with incontinence who initiated treatment have been shown to have poorer outcomes and higher costs than patients without OAB [22]. OAB is under-recognized, undertreated, and undermanaged in primary care. Patients do not bring up OAB with their physicians, primary care clinicians do not screen for OAB, and patients are generally dissatisfied with treatments for OAB [2, 6, 23, 24]. In our cohort, fewer than 20% of OAB patients were managed in the PCP setting only and fewer than 30% were co-managed between a PCP and a specialist. Despite the existence of guidance for primary care treatment of patients with OAB [25], a minority of patients with OAB seek care, many delay seeking care, few patients are diagnosed, and PCPs may prematurely refer patients for specialty care [24, 26–28]. Guidelines for referral should include failure to respond to pharmacologic therapy, uncertain diagnosis, microscopic or gross hematuria, or suspicion of bladder carcinoma [6].
Despite likely inadequate treatment, an increasing concern about OAB medications is anticholinergic burden in patients with high cumulative anticholinergic exposure. Studies have found associations between anticholinergic medication and brain atrophy, brain hypometabolism, progression to cognitive impairment, and increased healthcare utilization [29, 30]. Gray and colleagues found that dementia risk increased as the anticholinergic TSDD over 10 years increased when categories of 1–90, 91–365, 366–1095, and over 1095 were used [5]. Bladder antimuscarinics accounted for 10.5% of TSDD burden. We found a TSDD difference of 79 over 2 years between patients who did and did not receive OAB medications. Clinicians may not be aware of the cognitive risks associated with anticholinergic medications for OAB [31].
Our analysis has limitations that should be considered. First, our novel method of identifying OAB patients remains documentation-dependent. In order to be entered into the cohort, patients had to have at least one coded variable for OAB and clinicians or coders had to enter additional codes or documentation that indicated symptoms of OAB. Patients with unrecognized symptoms would not have such codes or documentation. Second, our OAB EHR phenotype of course does not have perfect sensitivity or PPV. We would have compared the sensitivity and PPV of our OAB EHR phenotype to other large-scale methods of OAB identification. However, as of November 2019, a PubMed search revealed no articles that reported the sensitivity or PPV for identifying OAB using claims or electronic health records. A conference presentation found that 25 different OAB-related ICD-9 codes had associations with OAB medications ranging from 0 to 21% (mean, 4%) [32].
Third, our measures of medication use represent medication prescribing, not fills or actual drug taking. Fourth, our detection period was restricted to 2 years, and may have identified patients with OAB characteristics prior to the identification period or prior receipt of OAB medications. Fifth, we could not include OAB health-related quality of life or other patient-reported outcome measures. Sixth, we only had access to documentation within our health system; care provided and documented elsewhere was not included. Seventh, patients were dichotomously defined as either having or not having OAB. We do not have a good method for determining disease duration, severity, or subtype. OAB disease duration and severity could be important in identifying differences between patients cared for by PCPs alone versus patients who saw specialists. OAB severity and subtype (e.g., incontinence-associated) could be associated with different patterns of OAB medication use. Eighth, we did not collect information about related symptoms, like constipation, which might also be associated with differential OAB medication use. Finally, as our results are based upon our health system, the results presented here may not be generalizable to other systems.
Despite these limitations, strengths of this study include our novel method of identifying an EHR phenotype for OAB and the relatively large sample of OAB patients. EHR phenotypes have the potential to expand understanding about the prevalence and treatment of OAB.
Conclusions
OAB is a common, morbid condition that is under-recognized. For patients identified using an OAB EHR phenotype in an integrated healthcare system, physicians prescribed medication to only 40% of patients over 2 years. Specialists were roughly twice as likely to prescribe medication to patients compared with PCPs. Even for patients who received medication, the average duration of medication use was only 1.5 months. Patients appear to have their symptoms inadequately addressed, as evidenced by the small number of patients who receive active treatment and the very short average duration of treatment. Treated patients who received OAB medications, predominantly antimuscarinics, had an increased anticholinergic burden.
Supplementary information
Additional file 1: Table S1. 37 OAB Structured Variables. Table S2. Final EHR Phenotype Model Variables and Coefficients. Table S3. Problem List Entries and Diagnosis Codes for Comorbid Conditions. Table S4. CPT Codes for Procedures. Table S5. Medication Prescribing by Patient Characteristics. Table S6. Cohort Characteristics by Source of Care.
Acknowledgements
The authors would like to recognize Sorbarikor Piawah, MD, Peter Olds, MD, and David Rubins, MD for their contributions to chart review.
Abbreviations
- BOW
Bag of words
- EHR
Electronic health record
- ICD-9
International Statistical Classification of Diseases and Related Health Problems
- ICS
International Continence Society
- LASSO
Least absolute shrinkage and selector operator
- OAB
Overactive bladder
- PCP
Primary care physician
- PPV
Positive predictive value
- TSDD
Total standardized daily dose
Authors’ contributions
JAL and HRN were responsible for acquisition of the data. JAL, JSW, HRN, SL, RSH, JD, RMK, and KRL made substantial contributions to conception and design; analysis and interpretation of data; drafting and revision of the manuscript for important intellectual content; read and approved the final manuscript; and agree both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Funding
This analysis was supported by a grant from Astellas Pharma, Inc. Two of the co-authors (JD and RMK) are employees of Astellas. Staff from Astellas were involved in the design and conduct of the study; interpretation of the data; preparation, review, and approval of the manuscript; and the decision to submit the manuscript for publication. Astellas was not involved in the collection, management, or analysis of the data.
Availability of data and materials
The dataset supporting the conclusions of this article is not publically available as the data contain identifiable information from patients who were receiving routine clinical care. An extract may be available from the corresponding author on reasonable request.
Ethics approval and consent to participate
The Partners HealthCare Human Research Committee approved the protocol (#2014P000290/BWH). No additional administrative approvals were required. The data were maintained within the Partners HealthCare firewall and were not anonymized. Data are only reported in aggregate in this manuscript.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Jeffrey A. Linder, Email: jlinder@northwestern.edu
Joel S. Weissman, Email: jweissman@partners.org
Harry Reyes Nieva, Email: harryreyesnieva@gmail.com.
Stuart Lipsitz, Email: slipsitz@partners.org.
R. Sterling Haring, Email: sharing1@jhu.edu.
Julie DeAngelis, Email: julie.deangelis@astellas.com.
Rita M. Kristy, Email: Rita.Kristy@astellas.com
Kevin R. Loughlin, Email: kloughlin@partners.org
Supplementary information
Supplementary information accompanies this paper at 10.1186/s12913-020-05315-1.
References
- 1.Stewart WF, Van Rooyen JB, Cundiff GW, et al. Prevalence and burden of overactive bladder in the United States. World J Urol. 2003;20(6):327–336. doi: 10.1007/s00345-002-0301-4. [DOI] [PubMed] [Google Scholar]
- 2.Milsom I, Abrams P, Cardozo L, Roberts RG, Thuroff J, Wein AJ. How widespread are the symptoms of an overactive bladder and how are they managed? A population-based prevalence study. BJU Int. 2001;87(9):760–766. doi: 10.1046/j.1464-410x.2001.02228.x. [DOI] [PubMed] [Google Scholar]
- 3.Gormley EA, Lightner DJ, Burgio KL, et al. Diagnosis and treatment of overactive bladder (non-neurogenic) in adults: AUA/SUFU guideline. J Urol. 2012;188(6 Suppl):2455–2463. doi: 10.1016/j.juro.2012.09.079. [DOI] [PubMed] [Google Scholar]
- 4.Campbell NL, Boustani MA, Lane KA, et al. Use of anticholinergics and the risk of cognitive impairment in an African American population. Neurology. 2010;75(2):152–159. doi: 10.1212/WNL.0b013e3181e7f2ab. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gray SL, Anderson ML, Dublin S, et al. Cumulative use of strong anticholinergics and incident dementia: a prospective cohort study. JAMA Intern Med. 2015;175(3):401–407. doi: 10.1001/jamainternmed.2014.7663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Macdiarmid SA. Maximizing the treatment of overactive bladder in the elderly. Rev Urol. 2008;10(1):6–13. [PMC free article] [PubMed] [Google Scholar]
- 7.Helfand BT, Evans RM, McVary KT. A comparison of the frequencies of medical therapies for overactive bladder in men and women: analysis of more than 7.2 million aging patients. Eur Urol. 2010;57(4):586–591. doi: 10.1016/j.eururo.2009.12.025. [DOI] [PubMed] [Google Scholar]
- 8.Wagg A, Compion G, Fahey A, Siddiqui E. Persistence with prescribed antimuscarinic therapy for overactive bladder: a UK experience. BJU Int. 2012;110(11):1767–1774. doi: 10.1111/j.1464-410X.2012.11023.x. [DOI] [PubMed] [Google Scholar]
- 9.Chancellor MB, Migliaccio-Walle K, Bramley TJ, Chaudhari SL, Corbell C, Globe D. Long-term patterns of use and treatment failure with anticholinergic agents for overactive bladder. Clin Ther. 2013;35(11):1744–1751. doi: 10.1016/j.clinthera.2013.08.017. [DOI] [PubMed] [Google Scholar]
- 10.Pathak J, Kho AN, Denny JC. Electronic health records-driven phenotyping: challenges, recent advances, and perspectives. J Am Med Inform Assoc. 2013;20(e2):e206–e211. doi: 10.1136/amiajnl-2013-002428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Liao KP, Cai T, Savova GK, et al. Development of phenotype algorithms using electronic medical records and incorporating natural language processing. BMJ. 2015;350:h1885. doi: 10.1136/bmj.h1885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Abrams P, Cardozo L, Wagg A, Wein A, editors. Incontinence, 6th ed. Bristol, UK: ICI-ICS. International Continence Society; 2017. [Google Scholar]
- 13.Tibshirani R. The lasso method for variable selection in the cox model. Stat Med. 1997;16(4):385–395. doi: 10.1002/(sici)1097-0258(19970228)16:4<385::aid-sim380>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 14.Tibshirani R. Regression shrinkage and selection via the lasso. J R Statist Soc B. 1996;58(1):267–288. [Google Scholar]
- 15.Hanlon JT, Boudreau RM, Roumani YF, et al. Number and dosage of central nervous system medications on recurrent falls in community elders: the health, aging and body composition study. J Gerontol A Biol Sci Med Sci. 2009;64A(4):492–498. doi: 10.1093/gerona/gln043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Nitti VW, Rovner ES, Franks B, et al. Persistence with mirabegron versus tolterodine in patients with overactive bladder. Am J Pharm Benefits. 2016;8(2):e25–e33. [Google Scholar]
- 17.Brostrøm S, Hallas J. Persistence of antimuscarinic drug use. Eur J Clin Pharmacol. 2009;65(3):309–314. doi: 10.1007/s00228-008-0600-9. [DOI] [PubMed] [Google Scholar]
- 18.Linner L, Schioler H, Samuelsson E, Milsom I, Nilsson F. Low persistence of anticholinergic drug use in Sweden. Eur J Clin Pharmacol. 2011;67(5):535–536. doi: 10.1007/s00228-010-0917-z. [DOI] [PubMed] [Google Scholar]
- 19.Moskowitz D, Adelstein SA, Lucioni A, Lee UJ, Kobashi KC. Use of third line therapy for overactive bladder in a practice with multiple subspecialty providers-are we doing enough? J Urol. 2018;199(3):779–784. doi: 10.1016/j.juro.2017.09.102. [DOI] [PubMed] [Google Scholar]
- 20.Sexton CC, Notte SM, Maroulis C, et al. Persistence and adherence in the treatment of overactive bladder syndrome with anticholinergic therapy: a systematic review of the literature. Int J Clin Pract. 2011;65(5):567–585. doi: 10.1111/j.1742-1241.2010.02626.x. [DOI] [PubMed] [Google Scholar]
- 21.Fischer MA, Stedman MR, Lii J, et al. Primary medication non-adherence: analysis of 195,930 electronic prescriptions. J Gen Intern Med. 2010;25(4):284–290. doi: 10.1007/s11606-010-1253-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yehoshua A, Chancellor M, Vasavada S, et al. Health resource utilization and cost for patients with incontinent overactive bladder treated with anticholinergics. J Manag Care Spec Pharm. 2016;22(4):406–413. doi: 10.18553/jmcp.2016.22.4.406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Shaw C, Tansey R, Jackson C, Hyde C, Allan R. Barriers to help seeking in people with urinary symptoms. Fam Pract. 2001;18(1):48–52. doi: 10.1093/fampra/18.1.48. [DOI] [PubMed] [Google Scholar]
- 24.Dmochowski RR, Newman DK. Impact of overactive bladder on women in the United States: results of a national survey. Curr Med Res Opin. 2007;23(1):65–76. doi: 10.1185/030079907X159533. [DOI] [PubMed] [Google Scholar]
- 25.Rosenberg MT, Witt ES, Barkin J, Miner M. A practical primary care approach to overactive bladder. Can J Urol. 2014;21(Suppl 2):2–11. [PubMed] [Google Scholar]
- 26.Coyne KS, Sexton CC, Kopp ZS, Ebel-Bitoun C, Milsom I, Chapple C. The impact of overactive bladder on mental health, work productivity and health-related quality of life in the UK and Sweden: results from EpiLUTS. BJU Int. 2011;108(9):1459–1471. doi: 10.1111/j.1464-410X.2010.10013.x. [DOI] [PubMed] [Google Scholar]
- 27.Cheung WW, Blank W, Borawski D, Tran W, Bluth MH. Prevalence of overactive bladder, its under-diagnosis, and risk factors in a male urologic veterans population. Int J Med Sci. 2010;7(6):391–394. doi: 10.7150/ijms.7.391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Smith AL, Nissim HA, Le TX, et al. Misconceptions and miscommunication among aging women with overactive bladder symptoms. Urology. 2011;77(1):55–59. doi: 10.1016/j.urology.2010.07.460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Campbell NL, Perkins AJ, Bradt P, et al. Association of anticholinergic burden with cognitive impairment and health care utilization among a diverse ambulatory older adult population. Pharmacotherapy. 2016;36(11):1123–1131. doi: 10.1002/phar.1843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Risacher SL, McDonald BC, Tallman EF, et al. Association between anticholinergic medication use and cognition, brain metabolism, and brain atrophy in cognitively normal older adults. JAMA Neurol. 2016;73(6):721–732. doi: 10.1001/jamaneurol.2016.0580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Araklitis G, Thiagamoorthy G, Hunter J, Rantell A, Robinson D, Cardozo L. Anticholinergic prescription: are healthcare professionals the real burden? Int Urogynecol J. 2017;28(8):1249–1256. doi: 10.1007/s00192-016-3258-3. [DOI] [PubMed] [Google Scholar]
- 32.Espinosa R, Davis M, Johnson SJ, Walker D, Ng DB, Gooch K. Impact of individual diangosis codes on database estimates of overactive bladder. ISPOR 2017; May 20–24, 2017; Boston, MA USA.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Table S1. 37 OAB Structured Variables. Table S2. Final EHR Phenotype Model Variables and Coefficients. Table S3. Problem List Entries and Diagnosis Codes for Comorbid Conditions. Table S4. CPT Codes for Procedures. Table S5. Medication Prescribing by Patient Characteristics. Table S6. Cohort Characteristics by Source of Care.
Data Availability Statement
The dataset supporting the conclusions of this article is not publically available as the data contain identifiable information from patients who were receiving routine clinical care. An extract may be available from the corresponding author on reasonable request.