

Abstract
Background
The adverse life-long consequences of being looked-after as a child are well recognised, but follow-up periods for mortality risk have mostly ended in young adulthood and mortality suggested to differ by age of placement, gender and cohort in small samples.
Methods
Data on 353,601 Office for National Statistics Longitudinal Study (LS) members during census years 1971–2001, and Cox proportional hazards regression models with time-varying covariates (age as the timescale), were used to examine whether childhood out-of-home care was associated with all-cause mortality until the end of 2013. After adjusting for baseline age and age2, gender, born outside the United Kingdom, number of census observations in childhood and baseline census year we tested whether mortality risk varied for those in care by age, gender and baseline census year, by separate assessment of interaction terms. Supplementary analyses assessed robustness of findings.
Results
Adults who had been in care at any census (maximum of two) had an adjusted all-cause mortality hazard ratio 1.62 (95% CI 1.43, 1.86) times higher than adults who had never been in care. The excess mortality was mainly attributable to deaths categorised as self-harm, accidents and mental & behavioural causes. Mortality risk was elevated if the LS member was initially assessed in 1981 or 2001, compared to 1971. There was no significant variation in mortality risk for those in care by age or gender. The main findings were consistent irrespective of choice of comparison group (whole population, disadvantaged population), care placement (residential, non-residential) and age at death (all ages, adulthood only).
Conclusions
In this large, nationally representative study of dependent children resident in England and Wales, those who had been in care during childhood had a higher risk of mortality long after they had left care on average, mainly from unnatural causes. No differences by age or gender were found. Children in care have not benefitted from the general decline in mortality risk over time.
Keywords: Mortality, England, Wales, Longitudinal, Looked after children, Child welfare, Foster care, Life course
Background
As of March 2018, the number of children looked-after by local authorities in England and Wales was 75,420 and 6407 respectively; equivalent to 62 and 102 per 10,000 population under aged 18 [1, 2]. Both the number of, and rate of children being looked-after, have increased steadily over the past decade, due to a combination of more children entering, and fewer children leaving, care [1].
The adverse life-long consequences of being looked-after as a child are well recognised. This includes worse physical [3–6] and mental health [3–5, 7–13], lower educational attainment, higher rates of unemployment [3, 5, 10, 11, 13], and less stability of housing after care [3, 5, 10, 11, 13]. A small number of studies have shown that children in care have higher mortality than the general population of children, but follow-up periods have mostly ended in young adulthood [14–16]. Only one study we aware of has examined mortality 30 years after care status assessment, but was restricted to children in residential care in 1971 only [3]. As a consequence of the United Kingdom’s (UK’s) 1989 Children Act recommending that placement priority be given to a child’s extended relatives and friends, the percentage of children in residential care has decreased and children in relative household care increased [17–19]. Therefore, it is important to understand whether the previously observed higher mortality risk for looked-after children in residential settings applies to all looked-after children, extends beyond the early adult years, and has continued in later cohorts, in order to identify and hopefully reduce preventable deaths in this vulnerable population.
In addition, studies showed a weak association between care status and mortality in girls placed in early childhood, but stronger evidence for girls placed in care at later ages and for boys placed at any age, mainly from unnatural deaths [15, 16]. One possible explanation concerns the age and gender differences in resilience, with young girls more likely to be resilient to stressful circumstances than young boys [20]. Another includes children entering care at different ages do so for different reasons, parental abuse and developmental issues more common for entry at younger ages and behavioural issues/delinquency more common at older ages [21]. As well, being in care during later childhood may reflect longer placements and multiple placements, which have been associated with more extensive adult emotional and behavioural issues [13, 22]. It is therefore possible that being in care during later childhood and adolescence may be a marker for later adult mortality risk, particularly from unnatural causes.
Thus, we used data from a large nationally representative longitudinal data set to examine 1) whether children who had been in care have higher mortality up to 42 years later than children had in the general population. We also test whether these associations vary, or are explained, by gender or age and year when first observed. The hypotheses for these tests are that given previous findings of gender and age differences, 2) boys in care will have higher mortality than girls in care; and 3) being first observed in care later in childhood will be associated with higher mortality than care earlier in childhood. Finally, 4) given the introduction and implementation of the UK’s 1989 Children Act, there will be a reduction in mortality for those observed more recently.
Methods
Data
The Office for National Statistics (ONS) Longitudinal Study (LS) is a 1% representative sample of the population of England and Wales, drawn initially from respondents to the 1971 census who had been born on one of four birthdays [23]. The LS is updated with new members if they have one of the same four birthdays and are either newly-born or immigrants. Members are followed-up in every subsequent 10-year census and are linked to life events data such as births, deaths, and cancer registrations. In order to only include dependent children who could potentially be placed in non-parental care, the sample for this analysis includes individuals aged less than 18 years, of single marital status, not living alone/independently, and not a visitor in the household/residential setting at each of the censuses 1971, 1981, 1991 or 2001. LS members were including in the analysis sample with data from one or two censuses during childhood. Data from only one census occurred if they were not observed at a census 10 years earlier or later or they no longer met the criteria for a dependent child at the next census. LS variables included in the current study did not have any missing values. The analysis sample consisted of 353,601 members with 61% having one and 39% two observations (Table 1 and Supplementary Table S1).
Table 1.
Distribution of care status by number of observations in childhood, ONS Longitudinal Study
| Number of observations | Care status | N | % |
|---|---|---|---|
| One | Y | 3439 | 1.59 |
| N | 212,224 | 98.41 | |
| Two | Y Y | 237 | 0.17 |
| Y N | 763 | 0.55 | |
| N Y | 2005 | 1.45 | |
| N N | 134,933 | 97.82 | |
| Total | 491,539 | 100.00 | |
| N | 353,601 |
Y: in care; N not in care.
Age at each census
Analysing repeated measures highlighted some inconsistencies in the recording of age. When cleaning the time variables, we prioritised the reliability of year of birth and year of death data over age at each census (i.e. correcting age at census to year of census – year of birth), unless there was an obvious keying error. This process maintained the intra-individual consistency of the data although it is also possible that some unreliability could have been introduced depending on whether a birthday fell before or after the census date.
Age and cause of death
Age of death was calculated by ONS from year and month of death data from annual matches of LS members with death certificate data [24]. At the time of analysis, all-cause mortality data were available up to 31st December 2013. Individuals who had emigrated or not died by the end of 2013 were treated as right censored. The ONS previously derived a 20-group cause of death categorisation from underlying cause of death data on death certificates, using the International Classification of Diseases coding in use at the time of death [25]. For comparison with previous literature, we further collapsed these 20 categories into a four category cause of death variable: (1) “Unnatural” (Mental or behavioural, accidents or self-harm), (2) “Circulatory” (Ischemic heart disease, Stroke, Pulmonary disease), (3) “Cancer” (Lung cancer, Other cancers, Benign neoplasms) or (4) “Other” (Infectious & parasitic, diabetes, gastro-intestinal tract disease, liver disease, abnormalities & lab results, muscular diseases, nervous system, genito-urinary, other endocrine, skin disease, other cause).
Care status
For each census from 1971 to 2001, dependent children were classified into those: i) living with a parent, ii) living with a relative (excluding children or relatives aged < 16) or with unrelated others (formal and informal foster care), or iii) living in residential care (a children’s home or place of detention).
Covariates
Baseline was the first census the sample member responded, out of the potential census years 1971, 1981, 1991 and 2001. Baseline age, gender, country of birth and census year were investigated as potential confounders. Non-linear baseline age effects were modelled using age and age2 terms. Responses on census questions about place of birth were collapsed into born in the UK (0 = England, Wales, Scotland and Northern Ireland) or not (1 = any other country listed). To control for any negative selection bias (members may have survived for longer to be observed twice in childhood), a dummy variable indicated if the LS member had been observed in two censuses while still a dependent child.
Statistical analysis
All care categories and baseline covariates were compared by mortality status at follow-up using Analysis of Variance (ANOVA) for continuous variables and the chi-square statistic for categorical variables. In addition, for LS members who had died, distribution of cause of death was compared across the two care categories separately. We collapsed the care categories into a binary in care or not variable for the main survival analyses using Cox proportional hazards regression models with time-varying covariates (with age as the timescale) that account for intra-individual correlation [26]. Time at risk was assessed from age at baseline census until age at death or right censoring (i.e. the age they reached the end of follow-up). Models were initially fitted unadjusted (model 1), and adjusted for age and age2 at baseline, gender, country of birth, baseline census year and the number of childhood observations (model 2). To check for potential increased risks of mortality for children in care by gender, baseline age or during specific periods, we added interaction terms for gender, baseline age and cohort with care status to the adjusted model in models 3, 4 and 5 respectively.
Supplementary analyses checked the robustness of findings. First, in model SM1 we reduced the reference group to those not in care and living in a socially disadvantaged household since children in care are more likely to be from a disadvantaged family and to be living with a more disadvantaged family while in care [27, 28]. Disadvantage was defined as the head of household being in a routine occupational class according to the National Statistics Socio-economic Classification [29]. Frailty models could not be estimated to assess potential confounding by unobserved individual characteristics because of the large sample size. To assess whether mortality applied to those in residential care and non-residential (models SM2 and SM3), we separately re-analysed the data for those in these care situations. A final analysis removed observations for those who had died before the age of 18 (model SM4), under the assumption that death during childhood was more likely to be a consequence of pre-existing poor health than their experience of care. It has also been suggested that mortality from age 18 reflects difficulties in adapting to independent living [15].
All analyses were carried out using Stata 14 [30].
Results
Sample characteristics by mortality status at follow-up are shown in Table 2. For those LS members who had died (Table 3, n = 8814), a higher proportion of deaths for the non-parental care categories occurred within the “Unnatural” (self-harm, accidents and mental/behavioural) causes of deaths, rather than the cardiovascular, cancer or other categories (p < 0.0005).
Table 2.
Sample characteristics by mortality status at end of follow-up on 31st December 2013, ONS Longitudinal Study
| TOTAL (n = 353,601) |
Dead (n = 8814) |
Alive (n = 344,787) |
p-value (difference by death status) | |
|---|---|---|---|---|
| 1st observation (baseline) | ||||
| Median age (SIQR) | 353,601 | 9.0 (10.0) | 7.0 (6.5) | 0.0001 |
| Gender (%) | < 0.0005 | |||
| Male | 180,905 | 5607 (3.10) | 175,298 (96.90) | |
| Female | 172,696 | 3207 (1.86) | 169,489 (98.14) | |
| Country of birth (%) | < 0.0005 | |||
| UK | 338,661 | 8514 (2.51) | 330,147 (97.49) | |
| Other | 14,940 | 300 (2.01) | 14,640 (97.99) | |
| Census year (%) | < 0.0005 | |||
| 1971 | 135,810 | 6631 (4.88) | 129,179 (95.12) | |
| 1981 | 73,667 | 1428 (1.94) | 72,239 (98.06) | |
| 1991 | 74,440 | 583 (0.78) | 73,857 (99.22) | |
| 2001 | 69,684 | 172 (0.25) | 69,512 (99.75) | |
| In Care (%) | < 0.0005 | |||
| Yes | 5681 | 227 (4.00) | 5454 (97.53) | |
| No | 347,920 | 8587 (2.47) | 339,333 (96.00) | |
| 2nd observation | ||||
| In Care (%) | < 0.0005 | |||
| Yes | 2242 | 69 (3.08) | 2173 (96.92) | |
| No | 135,696 | 2421 (1.78) | 133,275 (98.22) | |
| Follow-up | ||||
| Median age of death or censoring (SIQR) | 353,801 | 40.0 (37.5) | 38.0 (37.5) | 0.023 |
ONS Office of National Statistics; SIQR Semi inter-quartile range.
Table 3.
Causes of death by care status, ONS Longitudinal Study
| Care in childhood | TOTAL | Unnatural (%) | Circulatory (%) | Cancer (%) | Other (%) |
|---|---|---|---|---|---|
| Parental care | 8587 | 26.52 | 18.91 | 28.07 | 26.51 |
| Residential care | 88 | 35.23 | 18.18 | 18.18 | 28.41 |
| Non-residential care | 139 | 38.13 | 20.86 | 21.58 | 19.42 |
| TOTAL N | 8814 | 2361 | 1669 | 2456 | 2328 |
ONS Office of National Statistics.
Those who had been in care in childhood were, at any given time point during the follow-up period, 70% more likely to die (Hazard ratio 1.70; 95% CI 1.49, 1.93) than those who had not been in care (Table 4, model 1). This was attenuated slightly with the addition of controls (model 2). There was no indication of an interaction between care status and gender (model 3, p = 0.49) and only weak support for a care status by baseline age interaction (model 4, p = 0.09). In the final model (Table 4, model 5), the association between care and all-cause mortality varied by baseline census year (p = 0.0009); for those first observed in the 1971 census, the hazard ratio for the care group was 1.44 (95% CI 1.23, 1.69) times that for those who had not been in care. When average hazard ratios were predicted for each care by baseline census year group (Fig. 1), mortality risk declined over time for those not in care but remained higher for care groups in all census years, especially for the 1981 and 2001 census years, resulting in 4.61:1 difference in mortality risk for those who had been in care versus not.
Table 4.
Hazard ratios (95% confidence intervals) from Cox regression models of death by care status, ONS Longitudinal Study
| Model 1: Care status |
Model 2: + Controls |
Model 3: + Gender interaction |
Model 4: + Age interaction |
Model 5: + Baseline census interaction |
|
|---|---|---|---|---|---|
| Main effects | |||||
| In care | 1.70 (1.49, 1.93) | 1.63 (1.43, 1.86) | 1.69 (1.43, 1.99) | 2.01 (1.53, 2.65) | 1.44 (1.23, 1.69) |
| Baseline age | 0.97 (0.95, 0.99) | 0.97 (0.95, 0.99) | 0.97 (0.95, 0.99) | 0.97 (0.95, 0.99) | |
| Baseline age2 | 1.003 (1.002, 1.004) | 1.003 (1.002, 1.004) | 1.003 (1.002, 1.004) | 1.003 (1.002, 1.004) | |
| Male | 1.64 (1.57, 1.71) | 1.64 (1.57, 1.71) | 1.64 (1.57, 1.71) | 1.64 (1.57, 1.71) | |
| Born outside UK | 1.31 (1.17, 1.46) | 1.31 (1.17, 1.47) | 1.30 (1.16, 1.46) | 1.31 (1.17, 1.47) | |
| Baseline census | |||||
| 1971 (ref) | 1.00 | 1.00 | 1.00 | 1.00 | |
| 1981 | 1.07 (1.00, 1.14) | 1.07 (1.00, 1.14) | 1.07 (1.00, 1.14) | 1.06 (0.99, 1.13) | |
| 1991 | 0.84 (0.77, 0.93) | 0.84 (0.77, 0.93) | 0.85 (0.77, 0.93) | 0.84 (0.76, 0.93) | |
| 2001 | 0.47 (0.40, 0.56) | 0.47 (0.40, 0.56) | 0.47 (0.40, 0.57) | 0.45 (0.38, 0.54) | |
| Number of observations | |||||
| One (ref) | 1.00 | 1.00 | 1.00 | 1.00 | |
| Two | 0.67 (0.62, 0.72) | 0.67 (0.62, 0.72) | 0.67 (0.62, 0.72) | 0.67 (0.62, 0.72) | |
| Interaction terms | |||||
| Care by male gender | 1.10 (0.84, 1.44) | ||||
| Care by age | 0.98 (0.96, 1.00) | ||||
| Care by baseline census | |||||
| In care in 1971 (ref) | 1.00 | ||||
| In care in 1981 | 1.36 (0.99, 1.88) | ||||
| In care in 1991 | 1.34 (0.81, 2.23) | ||||
| In care in 2001 | 3.19 (1.74, 5.86) | ||||
N = 353,601, observations = 491,539.
Fig. 1.
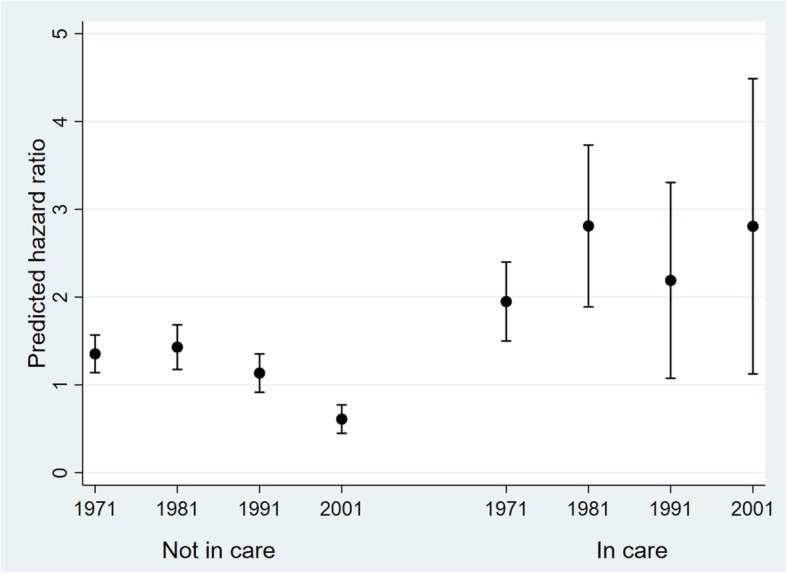
Predicted mortality hazard ratios for care status by baseline census year interaction, ONS Longitudinal Study. Adjusted for age and age2 at baseline, gender, country of birth and number of observations per individual
Supplementary analyses
Marginal predictions from the final model are first shown in Table 5 (model 5). When the reference group who had not been in care was confined to those in disadvantaged households only, there was minimal attenuation of the predicted hazard ratios (model SM1). This suggests the findings were robust to the choice of the comparison group.
Table 5.
Marginal predictions of the mortality hazard ratios for all combinations of care status with baseline census year from sensitivity models, ONS Longitudinal Study
| In care | Baseline census | Model 5 | Model SM1 Disadvantaged non-care group | Model SM2 Residential care only | Model SM3 Non-residential care only |
Model SM4 Deaths > 17 years old only |
|---|---|---|---|---|---|---|
| No | 1971 | 1.35 (1.14, 1.57) | 1.35 (0.92, 1.78) | 1.30 (1.09, 1.51) | 1.31 (1.11, 1.52) | 2.95 (2.46, 3.44) |
| No | 1981 | 1.43 (1.18, 1.68) | 1.59 (1.02, 2.16) | 1.38 (1.13, 1.63) | 1.39 (1.14, 1.64) | 3.27 (2.66, 3.88) |
| No | 1991 | 1.13 (0.92, 1.35) | 1.43 (0.87, 2.00) | 1.09 (0.88, 1.31) | 1.10 (0.89, 1.32) | 2.47 (1.95, 2.99) |
| No | 2001 | 0.61 (0.45, 0.77) | 0.55 (0.22, 0.89) | 0.59 (0.43, 0.74) | 0.59 (0.44, 0.75) | 1.72 (1.16, 2.28) |
| Yes | 1971 | 1.95 (1.50, 2.40) | 1.77 (1.12, 2.42) | 3.36 (2.33, 4.39) | 1.43 (1.06, 1.80) | 4.15 (3.16, 5.13) |
| Yes | 1981 | 2.81 (1.89, 3.73) | 2.59 (1.41, 3.77) | 7.24 (3.91, 10.57) | 1.93 (1.16, 2.69) | 6.25 (4.09, 8.40) |
| Yes | 1991 | 2.19 (1.08, 3.31) | 2.08 (0.83, 3.33) | 4.15 (−0.68, 8.98) | 1.92 (0.86, 2.99) | 4.98 (2.21, 7.75) |
| Yes | 2001 | 2.81 (1.13, 4.49) | 2.70 (0.83, 4.57) | 31.50 (−4.98, 67.97) | 2.09 (0.66, 3.51) | 9.05 (2.10, 16.00) |
| Wald test | 16.42 | 13.11 | 30.14 | 12.71 | 13.59 | |
| p | 0.0009 | 0.004 | < 0.00005 | 0.005 | 0.004 | |
| N | 353,601 | 81,967 | 350,477 | 353,090 | 353,601 | |
| Observations | 491,539 | 93,567 | 485,770 | 490,627 | 491,539 |
When the reference group remained unchanged and instead the care group was confined to those who had been in residential care (model SM2), the predicted hazard ratios were amplified, consistent with the assumption that those in residential care had poorer health in childhood than those in non-residential care. This was most marked for the more recent baseline census years due to small cell sizes for the residential care by census year interaction estimates (Supplementary Table S2). When the reference group remained unchanged and the care group was confined to those who had been in non-residential care (model SM3), the predicted hazard ratios were attenuated but more similar to those observed for the final model. Nevertheless, despite no difference in the hazard ratios for the non-residential care group (1.43; 95% CI 1.06, 1.80) versus non-care group (1.31; 95% CI 1.11, 1.52) for those first observed in 1971, a significant difference over time emerged so that for those first observed in 2001 the predicted average hazard ratios were 2.09 (95% CI 0.66, 3.51) and 0.59 (95% CI 0.44, 0.75), respectively.
The full analysis sample was then reduced by removing any LS members who had died while still a child (i.e. < 18 years, model SM4). The predicted average hazard ratios were amplified but the general pattern of results remained the same despite few deaths among cohorts with shorter follow-up resulting in wider confidence intervals for these predictions.
Discussion
Statement of principal findings
In this large, nationally representative follow-up study of dependent children resident in England and Wales, consistent with hypothesis 1, all-cause mortality was higher among adults who had been in care up to 42 years earlier. There was no support for hypothesis 2; boys in care did not have a higher mortality risk than girls in care, nor for hypothesis 3 concerning an increased vulnerability if first observed in care at older ages. Finally, the reduction in mortality for those who were not in care across the census years 1971–2001 is not replicated for children who were in care; the difference in the mortality ratio for children in care was greater in 1981 and 2001 than in the 1971 census, contrary to hypothesis 4. The excess mortality for those who had been in care was mainly attributable to deaths categorised as self-harm, accidents and mental & behavioural causes.
Results in relation to other studies
Our overall finding that being in care in childhood was associated with higher adult all-cause mortality is consistent with the few previous studies on this topic [3, 14–16]. We expand on most of these studies [14–16] by showing that the elevated risk of mortality is apparent long past early adulthood for some LS members. One UK study, using the same data set as us, had compared mortality rates 30 years after care assessment but was restricted to the 1971 baseline census year only, with care in residential facilities only [3]. This is an important restriction, as their data show a relative risk of 2.43 (our calculation) for those in residential care is substantively attenuated in our data (relative risk 1.62) based on all care experiences and the addition of more recent censuses.
Only two other studies we are aware of have investigated gender, timing of care experience and mortality [15, 16]. Although both studies stratified results by gender, neither reported statistical tests of gender differences in deaths among care leavers. However, it is clear that our results on gender concur with theirs in finding no gender differences overall.
Extrapolating from their results also suggests that the age in care with mortality relationship from these studies found a lower risk if in care aged 1–10 compared with being in care aged 11–17 years in the Finnish study [15], but a non-significantly lower mortality risk aged 0–6 year compared with aged 7–12 years first in care in the Swedish study [16]. Our estimated hazard ratio of 0.98 for the interaction between age and being in care disagrees with both prior studies but warrants replication before drawing any inferences. Nevertheless, differences in findings between the two studies and ours could be due to the different sampling procedures, or the longer follow-up period in our study, or to the greater degree of accuracy in their study about when placements began and ended, or to the other studies employing a categorical rather than linear age term.
As far as we are aware, we are the first study to show that the relationship between care status and mortality varied by census year, exemplifying the inverse care law [31].
Implications and future research
The mechanism(s) by which being in care could be affecting mortality until later in adulthood is unclear. Numerous studies have shown that the mental and physical health, well known predictors of later mortality [32, 33], of children who enter care are worse than for the general population of children [5, 34–37]. This could be due to children with chronic conditions being more likely to be placed into care [32, 36, 37] or could reflect adverse effects of early life neglect and abuse [35, 38]. While we could not run the survival analysis for specific causes of death due to small numbers, descriptive data in our study showed the higher risk of mortality confined to ‘unnatural’ causes of death, rather than other categories, implicating mental ill-health as a key concern warranting further research. Furthermore, the finding of an increased risk of mortality when restricting the analysis to deaths in adulthood is consistent with the idea that children who have been in care find the transition to adulthood more difficult to negotiate [15]. A joint focus on physical and mental health, work, family and living arrangements at this life stage for care experienced individuals would be instructive.
Adults who have been in care are already known to have poorer social outcomes [3, 5, 8, 12, 39], with educational attainment, unemployment, unskilled occupation, homelessness and prison residence specifically known to be related to mortality [3, 40, 41]. One study examining mortality differences of Swedish 18-year olds who had been in foster care found that their mortality risk was similar to a comparison group that had been in contact with Welfare services, a group that should have had an equivalent distribution of social and health issues [16]. We found higher mortality risk for those who had been in care when a socially disadvantaged comparison group was used. Social determinants of health are also known to elevate cardiovascular and cancer mortality [42, 43], but this was not seen in our data. Taken together these findings suggest that it may not be the traditional social determinants that are driving the excess mortality risk, rather it could be a consequence of something specific to the need for care which is not being ameliorated by being cared for away from parents. If this is confirmed, then more upstream interventions are indicated.
Possible explanations for the differences in risk for care-experienced children across censuses are unclear. There was a suggestion that for the 1981 census, mortality was also higher for children who were not in care in childhood. Whatever mechanism was generally elevating mortality at that time, maybe entering the workforce during the 1990 and post-2008 recessions [44, 45], they could have been particularly challenging for children transitioning out of care during that time. Particularly for the 2001 census, there are concerns that reduced council funding due to austerity measures has resulted in reduced quality of care for looked-after children [46, 47], which could affect the mental health of these young people [48]. Alternatively, the elevated 2001 census mortality risk could be comparable to other censuses as they age, as a higher percentage of deaths occurred in the 20–40 year old age range for those who had been in care versus post-40 in the no care group; however when we restricted the follow-up to 13 years in all in census years, the excess 1991 and 2001 census mortality risk for children in care remained (HR 3.10 vs. 3.19 in Table 4).
By separately analysing residential and non-residential care experiences, we have a more nuanced understanding of the potential impact of being placed in care. With the reduction in relative risk of death and notwithstanding the higher hazard associated with non-residential care in 2001 (when the proportion of residential out-of-home care plummeted, Supplementary Table S2), this gives some support to the 1989 Children Act recommendation to give priority to relative care where possible.
Strengths and limitations of the study
The main strength of this paper is its ability to follow-up a nationally representative group of English and Welsh children prospectively for up to 42 years after initial care assessment. This allowed us to investigate whether care status in childhood was associated with mortality decades after the children had left care. Combined with the additional strength of the LS regularly being linked to national death records, this meant that there was no loss to follow-up. The repeated data collections across five censuses also allowed us to assess whether associations have changed over time; a distinct possibility as policies related to looked-after children, and their transitions to adulthood, have changed over the four decades of this study.
The major disadvantage of using the LS dataset is that census data are only collected every 10 years and a limited range of relevant covariates was available to us. Moreover, as the data are from the census, we are unable to identify children with and without local authority care orders. As well, 61% of the sample only contributed information at one census during childhood, resulting in some imprecision concerning measurement and timing of the exact periods in which children were in care. Given the relatively young age of the sample at follow-up, and corresponding low percentage of deaths in the population, it is unlikely that missing census data was due to mortality. However, in our data children in care were more likely to be non-respondents to a preceding or proceeding census. A further limitation is the shorter follow-up period for children observed more recently, with a less than 13-year follow-up for those observed in the 2001 census year. This could have biased the care by census year interaction tests, most likely making differences conservatively estimated. Finally, lack of data on reason(s) for care placement and family characteristics prior to care, which are likely to correlate highly with mortality, point toward some residual confounding in our data.
Conclusions
Adults who have been in care in childhood experience higher mortality risk after they have left care, especially to causes which can be ascribed as ‘unnatural deaths’. Further research should focus on the mechanisms underpinning these findings, particularly the role of mental health and why being in care during the early 1980s and 2000s is associated with excess mortality. If the findings reflect a true causal relationship between care and unnatural death in adulthood, current guidelines for transitions from child to adult health services [49] should be expanded to well beyond the initial young adult period.
Supplementary information
Additional file 1: Table S1. Distribution of observations in childhood by census year, ONS Longitudinal Study. Table S2. Distribution of observations in out-of-home care by census year, ONS Longitudinal Study.
Acknowledgements
The permission of the Office for National Statistics to use the Longitudinal Study is gratefully acknowledged, as is the help provided by staff of the Centre for Longitudinal Study Information & User Support (CeLSIUS), particularly Rachel Stuchbury. CeLSIUS is supported by the ESRC Census of Population Programme (Award Ref: ES/R00823X/1).The authors alone are responsible for the interpretation of the data.
This work contains statistical data from ONS which is Crown Copyright. The use of the ONS statistical data in this work does not imply the endorsement of the ONS in relation to the interpretation or analysis of the statistical data. This work uses research datasets which may not exactly reproduce National Statistics aggregates.
The derivation of 1971 and 1981 NSSEC & Goldthorpe classes is provided in Bukodi and Neuburger (2009) “Data Note. Job and occupational histories for the NSHD 1946 Birth Cohort” as part of the ESRC Gender Network Grant, Project 1 ‘Changing occupational careers of men and women’, Reference: RES-225-25-2001. The code was kindly provided by Erzsebet Bukodi and adapted for use in the LS by Buscha and Sturgis as part of the ESRC grant ‘Inter-cohort Trends in Intergenerational Mobility in England and Wales: income, status, and class (InTIME)’, Reference: ES/K003259/1.
Abbreviations
- ANOVA
Analysis of variance
- CeLSIUS
Centre for longitudinal study information & user support
- CI
Confidence interval
- LS
Longitudinal Study
- ONS
Office for national Statistics
- SIQR
Semi inter-quartile range
- UK
United Kingdom
Authors’ contributions
ETM conceived and designed the study, acquired the data, cleaned and analysed the data, interpreted the data, and drafted and revised the paper. AS contributed to the creation and design of the study, acquired the data, interpreted the data, and critically revised the paper. RL and BM contributed to the creation and design of the study, interpreted the data, and critically revised the paper. All Authors read and approved the manuscript.
Funding
This work was funded by the Nuffield Foundation (JUS/43052). The funders had no role in the study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Availability of data and materials
The datasets generated and/or analysed during the current study are available to anyone in the UK who can fulfil the requirements of ONS’s Approved Researcher Scheme. The data can be accessed through the Secure Research Service (SRS) safe setting rooms at ONS offices. The application process is fully detailed on the CeLSIUS website at [www.ucl.ac.uk/celsius] where all the necessary forms can be found under the ‘Using the ONS Longitudinal Study’ section.
Ethics approval and consent to participate
This project was reviewed by the Office for National Statistics Microdata Release Panel (ONS-MRP). The ethical acceptability of research projects is one of the aspects considered by the ONS-MRP. If there are concerns about the ethical acceptability of a piece of research, the ONS-MRP has the option of referring the project to the National Statistician’s Data Ethics Advisory Committee. Referral wasn’t considered necessary.
Consent for publication
The manuscript does not contain any individual person’s data. All results are aggregated. The ONS checks all outputs for any unintended disclosure of personal information and has approved the final version of the manuscript for publication.
Competing interests
Rebecca Lacey is an Associate Editor for BMC Public Health.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary information accompanies this paper at 10.1186/s12889-020-08867-3.
References
- 1.Department of Education. Children looked-after in England (including adoption), year ending 31 March 2018. 28 September 2018: SFR 50/2017. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/664995/SFR50_2017-Children_looked_after_in_England.pdf. Accessed 7 Aug 2019.
- 2.Statistics for Wales. Experimental statistics: Children looked-after by local authorities. 2018. https://gweddill.gov.wales/statistics-and-research/children-looked-after-local-authorities/?lang=en. Accessed 7 Aug 2019.
- 3.Melzer H, Guinea-Martin D, Millard B, Blackwell L. A thirty-year prospective study of children in residential care in the 1970s. Scott J Residential Child Care. 2008;7(1):1–6. [Google Scholar]
- 4.Bueler C, Orme J, Post J, Patterson D. The Long-term correlates of family foster care. Child Youth Serv Rev. 2000;22(8):595–625. [Google Scholar]
- 5.Viner R, Taylor B. Adult health and social outcomes of children who have been in public care: Population-based study. Pediatrics. 2005;115(4):894–899. doi: 10.1542/peds.2004-1311. [DOI] [PubMed] [Google Scholar]
- 6.Zlotnick C, Tam T, Soman L. Life course outcomes on mental and physical health: the impact of foster care in adulthood. Amer J of Public Health. 2012;102(3):534–540. doi: 10.2105/AJPH.2011.300285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Akister J, Owens M, Goodyer I. Leaving care and mental health: outcomes for children in out-of-home care during the transition to adulthood. Health Res Policy Syst. 2010;8(10):1–9. doi: 10.1186/1478-4505-8-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Barn R, Andrew L, Mantovani N. Life after care: the experiences of young people from different ethnic groups. 2005. https://www.jrf.org.uk/sites/default/files/jrf/migrated/files/1859351921.pdf. Accessed 7 Aug 2019.
- 9.Botchway S, Quiqley M, Gray R. Pregnancy-associated outcomes in women who spent some of their childhood looked-after by local authorities: findings from the UK Millenium Cohort Study. BMJ Open. 2014;4(12):1–9. doi: 10.1136/bmjopen-2014-005468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cashmore J, Paxman M. Wards leaving care: follow up five years on. Child Aust. 2006;31(3):18–25. [Google Scholar]
- 11.Cheung S, Buchanan A. Malaise scores in adulthood of children and young people who have been in care. J Child Psychol Psychiatry. 1997;38(5):575–580. doi: 10.1111/j.1469-7610.1997.tb01544.x. [DOI] [PubMed] [Google Scholar]
- 12.Courtney M, Okpych N, Charles P, Mikell D, Stevenson B, Park K, et al. Findings from the California Youth Transitions to Adulthood Study (CalYOUTH): conditions of youth at age 19. 2016. https://www.chapinhall.org/wp-content/uploads/CY_YT_RE0517_1.pdf. Accessed 7 Aug 2019.
- 13.Dregan A, Gulliford M. Foster care, residential care and public care placement patters are associated with adult life trajectories: population-based cohort study. Soc Psychiatry Psychiatr Epidemiol. 2012;47(9):1517–1526. doi: 10.1007/s00127-011-0458-5. [DOI] [PubMed] [Google Scholar]
- 14.Barth R, Blackwell D. Death rates among california's foster care and former foster care populations. Child Youth Serv Rev. 1998;20(7):577–604. [Google Scholar]
- 15.Kalland M, Pensola T, Merilainen J, Sinkkonen J. Mortality in children registered in the Finnish child welfare registry: population based study. BMJ. 2001;323:207–208. doi: 10.1136/bmj.323.7306.207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Vinnerljung B, Ribe M. Mortality after care among young adult foster children in Sweden. Int J Soc Welf. 2001;10(3):164–173. [Google Scholar]
- 17.Department of Health. Statutory guidance on promoting the health and well-being of looked-after children. 2009. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/276500/promoting_health_of_looked_after_children.pdf. Accessed 7 Aug 2019.
- 18.National Institute for Health and Care Excellence. Looked-after children and young people. Quality Standard. 3 April 2013. https://www.nice.org.uk/guidance/qs31. Accessed 7 Aug 2019.
- 19.Murray ET, Lacey R, Sacker A. P21. The health of adults who had been in care up to 40 years earlier: are there differences by type of care? J Epidemiol Community Health. 2018;72(Suppl_1):A70–1.
- 20.Sun J, Stewart D. Age and gender effects on resilience in children and adolescents. Int J Ment Health Promot. 2007;9(4):16–25. [Google Scholar]
- 21.McGrath-Lone L, Dearden L, Nasim B, Harron K, Gilbert R. Changes in first entry to out-of-home care from 1992 to 2012 among children in England. Child Abuse Negl. 2016;51:163–171. doi: 10.1016/j.chiabu.2015.10.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ford T, Vostanis P, Meltzer H, Goodman R. Psychiatric disorder among British children looked after by local authorities: comparison with children living in private households. Br J Psychiatry. 2007;190:319–325. doi: 10.1192/bjp.bp.106.025023. [DOI] [PubMed] [Google Scholar]
- 23.Shelton N, Marhsall C, Stuchbury R, Grundy E, Dennett A, Tomlinson J, et al. Cohort profile: the Office for National Statistics Longitudinal Study (The LS) Int J Epidemiol. 2018;48(2):383–384. doi: 10.1093/ije/dyy243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hattersley L, Creeser R. Longitudinal Study 1971-1991: History, organisation and quality of data. HM Stationery Office;1995 https://www.ucl.ac.uk/celsius/documents-pdfs/LS7.pdf. Accessed 7 Aug 2019.
- 25.Centre for Longitudinal Study Information and User Support (CeLSIUS). Derived variables: UDCOD [Underlying cause of death (20 categories)]. http://www.celsius.lshtm.ac.uk/derive/icd20.html Accessed 1 May 2019..
- 26.Bellera CA, MacGrogan G, Debled M, de Lara CT, Brouste V, Mathoulin-Pélissier S. Variables with time-varying effects and the Cox model:some statistical concepts illustrated with a prognostic factor study in breast cancer. BMC Med Res Methodol. 2010;10(1):20. [DOI] [PMC free article] [PubMed]
- 27.Berridge D. Theory and explanation in child welfare: education and looked-after children. Child Fam Soc Work. 2007;12(1):1–10. [Google Scholar]
- 28.McDermid S, Holmes L, Kirton D, Signoretta P. The demographic characteristics of foster carers in the UK: Motivations, barriers and messages forrecruitment and retention. London: Childhood Wellbeing Research Centre; 2013.
- 29.Office for National Statistics. The national statistics socio-economic classification user manual. Basingstoke: Palgrave Macmillan; 2005.
- 30.StataCorp. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP; 2015.
- 31.Hart JT. The inverse care law. Lancet. 1971;297(7696):405–412. doi: 10.1016/s0140-6736(71)92410-x. [DOI] [PubMed] [Google Scholar]
- 32.Walker E, McGee RDB. Mortality in mental disorders and global disease burden implications: a systematic review and meta-analysis. JAMA Psychiatry. 2015;72(4):334–341. doi: 10.1001/jamapsychiatry.2014.2502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Nunes B, Flores T, Mielke G, Thume E, Facchini L. Multimorbidity and mortality in older adults_a systematic review and meta-analysis. Arch Gerontol Geriatr. 2016;67:130–138. doi: 10.1016/j.archger.2016.07.008. [DOI] [PubMed] [Google Scholar]
- 34.Dimigen G, Del Priore C, Butler S, Evans S, Ferguson L, Swan M. Psychiatric disorder among children at time of entering local authority care: questionnaire survey. BMJ. 1999;319(7211):675–675. doi: 10.1136/bmj.319.7211.675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Berger L, Bruch S, Johnson E, James S, Rubin D. Estimating the "Impact" of out-of-home placement on child well-being: approaching the problem of selection bias. Child Dev. 2009;80(6):1856–1876. doi: 10.1111/j.1467-8624.2009.01372.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Martin A, Ford T, Goodman R, Meltzer H, Logan S. Physical illness in looked-after children: a cross-sectional study. Arch Dis Child Educ Pract Ed. 2014;99(2):103–107. doi: 10.1136/archdischild-2013-303993. [DOI] [PubMed] [Google Scholar]
- 37.Tarren-Sweeney M. The mental health of children in out-of-home care. Curr Opin Psychiatry. 2008;21(4):345–349. doi: 10.1097/YCO.0b013e32830321fa. [DOI] [PubMed] [Google Scholar]
- 38.Berens A, Nelson C. The science of early adversity: is there a role for large institutions in the care of vulnerable children? Lancet. 2015;386:388–398. doi: 10.1016/S0140-6736(14)61131-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Department of Education. Outcomes for children looked after by local authorities in England, 31 March 2016. 2017. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/695360/SFR20_2018_Text__1_.pdf. Accessed 7 Aug 2019.
- 40.Byhoff E, Hamati M, Power R, Burgard S, Chopra V. Increasing educational attainment and mortality reduction: a systematic review and taxonomy. BMC Public Health. 2017;17(1):719. doi: 10.1186/s12889-017-4754-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Lynch J, Smith G, Kaplan G, House J. Income inequality and mortality: importance to health of individual income, psychosocial environment, or material conditions. BMJ. 2000;320(7243):1200–1204. doi: 10.1136/bmj.320.7243.1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Stringhini S, Zaninotto P, Kumari M, Kivimaki M, Lassale C, Batty G. Socio-economic trajectories and cardiovascular disease mortality in older people: the English Longitudinal Study of Ageing. Int J Epidemiol. 2018;47(1):36–46. doi: 10.1093/ije/dyx106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Singh G, Jemal A. Socioeconomic and racial/ethnic disparities in cancer mortality, incidence, and survival in the United States, 1950-2014: over six decades of changing patterns and widening inequalities. J Environ Public Health. 2017;2819372:1–19. doi: 10.1155/2017/2819372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Falagas M, Vouloumanou E, Mavros M. Karageotgopoulos. Economic crises and mortality: a review of the literature. Int J Clin Pract Suppl. 2009;63(8):1128–1135. doi: 10.1111/j.1742-1241.2009.02124.x. [DOI] [PubMed] [Google Scholar]
- 45.Parmar D, Stravropoulou C, Ioannidis J. Health outcomes during the 2008 financial crises in Europe: systematic literature review. BMJ. 2016;354(i4588):1–11. doi: 10.1136/bmj.i4588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Children's Commissioner . Stability Index 2018: Overview and findings. London: Children's Commissioner for England; 2018. [Google Scholar]
- 47.Greenfield P, Marsh S. Vulnerable Children treated 'like cattle' in care home system.,” The Guardian, 10 Nov 2018. https://www.theguardian.com/society/2018/nov/10/vulnerable-children-treated-like-cattle-in-care-home-system. Accessed 7 Aug 2019.
- 48.House of Commons Education Committee. Mental health and well-being of looked-after children. Fourth Report of Session 2015-16. 2016. https://publications.parliament.uk/pa/cm201516/cmselect/cmeduc/481/481.pdf. Accessed 7 Aug 2019.
- 49.NICE, “Looked-after children and young people (QS31). 2013. https://www.nice.org.uk/sharedlearning/nice-qs-the-health-and-wellbeing-of-looked-after-children-and-young-people. Accessed 7 Aug 2019.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Additional file 1: Table S1. Distribution of observations in childhood by census year, ONS Longitudinal Study. Table S2. Distribution of observations in out-of-home care by census year, ONS Longitudinal Study.
Data Availability Statement
The datasets generated and/or analysed during the current study are available to anyone in the UK who can fulfil the requirements of ONS’s Approved Researcher Scheme. The data can be accessed through the Secure Research Service (SRS) safe setting rooms at ONS offices. The application process is fully detailed on the CeLSIUS website at [www.ucl.ac.uk/celsius] where all the necessary forms can be found under the ‘Using the ONS Longitudinal Study’ section.