

Dear Editor,
In December 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, formerly known as 2019 novel coronavirus) infection was discovered in Wuhan, Hubei Province of China, for the first time. The disease caused by SARS-CoV-2 (COVID-19) is transmitted by respiratory droplets and close contact (1, 2). By mid-March 2020, more than 180 000 cases with COVID-19 have been reported in the world and currently it is accepted as a pandemic by the World Health Organization. Until recently, COVID-19 infection and pneumonia have been rarely reported in pediatric patients; however, there have been a couple of pediatric COVID-19 pneumonia cases that occurred likely secondary to familial spread (3, 4). Herein, we aim to briefly communicate a pediatric COVID-19 case, which is a result of familial aggregation.
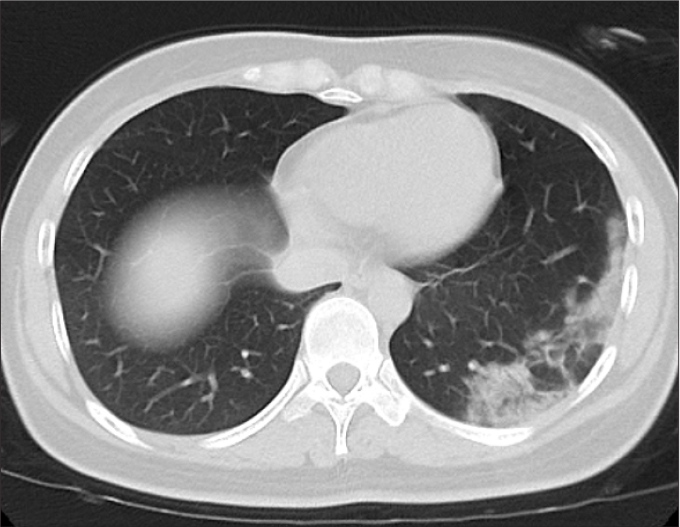
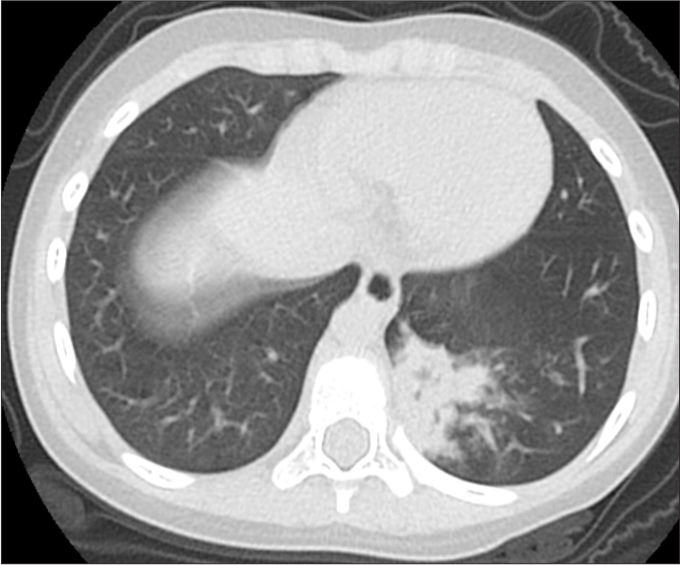
A 57-year old male police officer was referred to fever clinic of Xiangyang First People’s Hospital Affiliated to Hubei Medical College on February 1, 2020. Main complaints were mild cough for 3 days, low grade fever for 10 hours (maximum temperature 37.6°C), diarrhea, and anorexia. In his social history: on January 20, 2020, he escorted a male criminal to Wuhan and returned to Xiangyang 5 days later. Blood lab results were white blood cell count, 12.3×109/L (↑); neutrophil percentage, 89.0% (↑); eosinophil percentage, 0.1% (↓); lymphocyte absolute value, 0.71×109/L (↓); neutrophil count, 9.48×109/L (↑); lymphocyte percentage, 7.2% (↓); monocyte percentage, 2.2% (↓); C-reactive protein, 14.8 mg/L (↑); and oxygen saturation, 92%. Unenhanced chest CT revealed bilateral multi-focal ground glass opacities with consolidation (Fig. 1) (5); subsequent SARS-CoV-2 nucleic acid test was positive, confirming the diagnosis of COVID-19. He was immediately referred to isolation ward for intensive treatment with oxygen inhalation, intravenous cefuroxime sodium 1.5 g and oral abidol tablets (200 mg), lopinavir/ritonavir 200/50 mg. On February 6, 2020, he developed dyspnea and severe cough with 75% oxygen saturation. Further treatments included non-invasive ventilator to assist respiration, infusion of intravenous plasma donated by a recovered COVID-19 patient, and sputum aspiration by fibrobronchoscopy. Following his recovery on February 13, 2020, he was discharged and referred to a designated hotel for 14 days of isolation.
Figure 1. a, b.

A 57-year-old man presented with fever and positive polymerase chain reaction assay for SARS-CoV-2. Axial chest CT images (a, b) show multifocal ground glass opacities with consolidation.
Upon confirmation of COVID-19 pneumonia, we immediately informed the local Centers for Disease Control to investigate the patient’s close contacts in the past seven days. His 30-year-old daughter (Fig. 2) and 3-year-old granddaughter (Fig. 3) who lived with him were also tested positive for SARS-CoV-2, with chest CT findings of COVID-19 pneumonia. His granddaughter only complained of low fever (maximum temperature 37.7°C) for three days and the fever subsided without any medicine. Patient’s daughter was treated with oral abidol, lopinavir/ritonavir 200/50 mg and recovered after 8 days. Patient’s granddaughter was administered azithromycin 0.2 g/day per oral and recovered after 5 days. Our case emphasizes that COVID-19 can easily result in familial spread and it may lead to COVID-19 pneumonia in young adults and children, which can be asymptomatic in the initial phases of the infection. Careful testing for COVID-19 and further evaluation with imaging to rule out COVID-19 pneumonia in test positive individuals can be helpful for early diagnosis.
Figure 2.
Axial CT image of a 30-year-old female (daughter of the patient in Fig. 1) shows multi-focal round glass opacities with consolidation related with COVID-19 in the left lower lobe.
Figure 3.
Axial CT image of a 3-year-old female (granddaughter of the patient in Fig. 1) shows consolidation associated with COVID-19.
Footnotes
Conflict of interest disclosure
The authors declared no conflicts of interest.
References
- 1.Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727–733. doi: 10.1056/NEJMoa2001017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Munster VJ, Koopmans M, van Doremalen N, van Riel D, de Wit E. A novel coronavirus emerging in China - key questions for impact assessment. N Engl J Med. 2020 Jan 24; doi: 10.1056/NEJMp2000929. [DOI] [PubMed] [Google Scholar]
- 3.Xia W, Shao J, Guo Y, Peng X, Li Z, Hu D. Clinical and CT features in pediatric patients with COVID-19 infection: Different points from adults. Pediatr Pulmonol. 2020 Mar 5; doi: 10.1056/NEJMp2000929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.An P, Song P, Lian K, Wang Y. CT manifestations of novel coronavirus pneumonia: a case report. Balkan Med J. 2020 Mar 6; doi: 10.4274/balkanmedj.galenos.2020.2020.2.15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W, et al. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: A report of 1014 cases. Radiology. 2020 doi: 10.1002/ppul.24718. 200642. [DOI] [PMC free article] [PubMed] [Google Scholar]