

To the Editor
Since the Italian “Patient Zero” was identified, an enormous effort was made by the entire Radiotherapy (RT) centers, included the “Fondazione IRCCS-Istituto Nazionale dei Tumori di Milano” (INT) [1], to pursue the Care Mission during the Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-COVID 19 pandemic [2], [3].
The cases reported (www.ecdc.europa.eu) are non-stop increasing and Italian Health facilities are facing strong difficulties. After a first, confused phase, to date several shared advices have been published by many Authors. In fact, Italian RT centers have never stopped, but are consistently optimizing their activity [3], [4].
The acknowledged (SARS-CoV-2)-COVID 19 diagnosis tools are the Reverse transcriptase-polymerase chain reaction (RT-PCR) and the Gene sequencing of respiratory or blood samples: of note, the diagnostic accuracy of the throat swabs has been valued as 30–60% [5].
Ai et al. showed a sensitiveness equal to 97% of the CT scan of the chest, to find out COVID-19 in their cohort of 1014 patients (pts) with a positive SARS-CoV-2 RT-PCR [6].
RT centers must be safe sets for the struggle against Cancer. The clinical needs often overtake the laboratories promptness to process samples. Thus, the desideratum, whenever feasible and ethical, is to overcome this gap, as highlighted by Boldrini et al. [7].
The worldwide shared modern RT algorithm is based on a simulation-computed tomography (sim-CT) scan, used to determine volumes which must be irradiated [8]. Incidental findings on sim-CT in the set of breast cancer pts are described in up to 10–20% of pts [9]: indeed, it is a diagnostic tool in the clinical setting of RT.
Since the last 7th of April, the Radiation Oncologists of the INT are daily triaging by phone call the pts to be admitted the following day to our Department of Radiation Oncology. The same is being done by the RT Nurses for the pts to be medicated in the Department. Thus, we assume that pts entering in our RT Unit are asymptomatic.
Up to now have been reported cases of asymptomatic SARS-CoV-2 infections [10]. Dealing with frail pts impose the RT units to avoid any COVID-19 suspicion.
As oncological screening is now suspended in the United Kingdom [11], we are trying to think outside the box, drawing up a shared and welcomed-by-pts sim-CT protocol as it follows. A tension of 120 kV is applied to the X-ray tube of the tomograph with a current of 200 mAs/slice. The resulting dose index is 16.6 mGy; we acquire CT scans with 20–30 mAs/slice current [12].
Every sim-CT is being read by at least one Radiation Oncologist; once a suspicious COVID-19 lung pattern [6] has been found, the sim-CT is evaluated by a Radiologist of our Institution (Fig. 1 ).
Fig. 1.
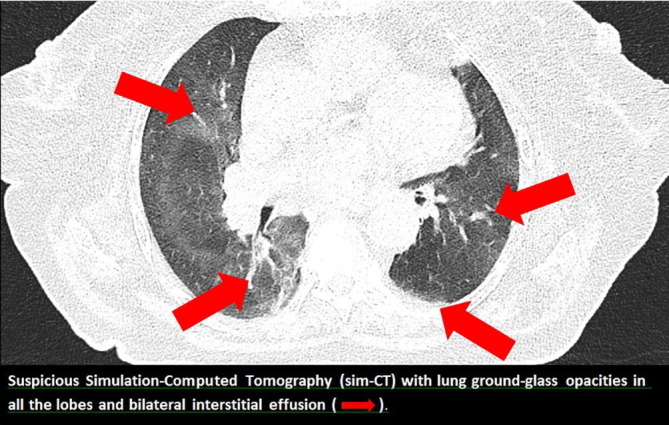
A lung suspicious case.
Since the 20th of April 2020 we have collected 163 sim-CTs; we have taken into account for our purposes just those pts who did not have a recent CT scan at the moment of our sim-CT. To date (12th of May 2020) we have collected 101 sim-CTs, 4 of whom have been considered highly suspicious of COVID-19.
After the Radiologists’ confirmation, each patient was screened with throat swabs. So far, none of the suspicious sim-CTs resulted in a diagnosis of COVID-19.
At the moment we are writing this Letter, this is the first data set available on sim-CT. Chest CT can be considered the primary tool in detecting COVID-19 compared to RT-PCR [5]. Thus, assuming a feasible not-negligible presence of asymptomatic pts in our Institution, especially in the early stages of the disease, sim-CT is pivotal in order to identify any possible infection. That could also produce a ripple effect, further reducing the infectious disease risk of healthcare staff and poor-health pts. Finally, it is also important to consider that only a few seconds are needed to perform a chest CT scan. Therefore, the costs in terms of “time required” and economic resources in developing this approach are far outweighed by the huge benefits.
Footnotes
The Editors of the Journal, the Publisher and the European Society for Radiotherapy and Oncology (ESTRO) cannot take responsibility for the statements or opinions expressed by the authors of these articles. Practitioners and researchers must always rely on their own experience and knowledge in evaluating and using any information, methods, compounds or experiments described herein. Because of rapid advances in the medical sciences, in particular, independent verification of diagnoses and drug dosages should be made. For more information see the editorial “Radiotherapy & Oncology during the COVID-19 pandemic”, Vol. 146, 2020.
References
- 1.Valenza F., Papagni G., Marchianò A. Response of a comprehensive cancer center to the COVID-19 pandemic: the experience of the Fondazione IRCCS–Istituto Nazionale dei Tumori di Milano. Tumori J. 2020 doi: 10.1177/0300891620923790. [DOI] [PubMed] [Google Scholar]
- 2.Fabrizio Carinci Covid-19: preparedness, decentralisation, and the hunt for patient zero bmj.m799 10.1136/bmj.m799 http://www.bmj.com/lookup/doi/10.1136/bmj.m799. [DOI] [PubMed]
- 3.Jereczek-Fossa B.A. COVID-19 outbreak and cancer radiotherapy disruption in Lombardy, Northern Italy. Clin Oncol. 2020 doi: 10.1016/j.clon.2020.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Meattini I., Franco P., Belgioia L. Radiation therapy during the coronavirus disease 2019 (covid-19) pandemic in Italy: a view of the nation's young oncologists. ESMO Open. 2020;5 doi: 10.1136/esmoopen-2020-000779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Yang Y., Yang M., Shen C. Evaluating the accuracy of different respiratory specimens in the laboratory diagnosis and monitoring the viral shedding of 2019-nCoV infections. medRxiv. 2020 doi: 10.1101/2020.02.11.20021493. [DOI] [Google Scholar]
- 6.Ai T., Yang Z., Hou H. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology. 2020;26 doi: 10.1148/radiol.2020200642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Boldrini L., Dinapoli N., Valentini V. Radiotherapy imaging: an unexpected ally in fighting COVID 19 pandemic. Radiother Oncol. 2020;148:223–224. doi: 10.1016/j.radonc.2020.04.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aird E.G., Conway J. CT simulation for radiotherapy treatment planning. Br J Radiol. 2002;75:937–949. doi: 10.1259/bjr.75.900.750937. [DOI] [PubMed] [Google Scholar]
- 9.Park J.S., Choi D.H., Huh S.J. Incidental findings on simulation CT images for adjuvant radiotherapy in breast cancer patients. Technol Cancer Res Treat. 2014;17:525–529. doi: 10.7785/tcrt.2012.500415. [DOI] [PubMed] [Google Scholar]
- 10.Gandhi M., Yokoe D.S., Havlir D.V. Asymptomatic transmission, the Achilles’ heel of current strategies to control Covid-19. New Engl J Med. 2020 doi: 10.1056/NEJMe2009758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jones D., Neal R.D., Duffy S.R.G., Scott S.E. Impact of the COVID-19 pandemic on the symptomatic diagnosis of cancer: the view from primary care. Lancet Oncol. 2020;21:603. doi: 10.1016/S1470-2045(20)30242-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.European Guidelines on Quality Criteria for Computed Tomography EUR 16262 EN.