

Abstract
Background
The aim of this study was to explore the relationship between outdoor activity (OA) and insufficient sleep duration (ISD) among Chinese children and to assess the potential age- and gender-specific effects.
Material/Methods
A national sample of 62 517 children aged 6–17 years were recruited from 7 provinces of China in the autumn of 2013. Children and their caregivers reported daily sleep duration (<7 h, 7–9 h and ≥9 h), daily OA time (<1 h, 1–2 h, and ≥2 h), and other behavior and demographic information by standardized questionnaire. ISD was defined as <9 h/day. Logistic regression analysis was used to evaluate the relationship between ISD and OA.
Results
In total, 46 639 children (50.9% boys) completed this survey. The prevalence of ISD was 74.9% (73.7% in boys and 76.1% in girls). Stratified by age, compared with <1 h OA, the odds ratios for ISD were 0.67 (95% confidence interval: 0.62–0.72, aged 6–13 years) and 0.69 (0.49–0.98, 14–17 years) in the ≥2 h OA group; 0.91 (0.85–0.97, 6–13 years) and 0.73 (0.54–0.97, 14–17 years) in the 1–2 h OA group. Further stratified by gender, we found similar trends for both boys and girls in each age group, although some results became non-significant.
Conclusions
Adequate OA time per day is associated with decreased risks for ISD among children aged 6–17 years, but age and gender can modify the association.
MeSH Keywords: Child, Motor Activity, Sleep
Background
Sleep is an important factor that influences cognitive, behavioral, and functional development of children [1]. According to the recommendation of the National Sleep Foundation (NSF), school-aged children need over 9 hours of sleep per night to maintain health and normal daily performance [2]. However, along with the rapid development of modern society, the sleep duration of children has been decreasing globally in recent decades [3]. For instance, nearly 16% of American urban children failed to meet the NSF criteria [4] in the early 2000s, and the prevalence of insufficient sleep increased to 45% [5] by 2006. Many researchers reported similar results in different countries and areas [6,7], showing that insufficient sleep of school-aged children has become a public health problem.
Evidence suggests that insufficient sleep duration (ISD) is associated with many behavior-related factors, especially activity level [8]. Outdoor activity (OA) is a specific form of physical activity (PA) that not only provides exercise but also allows children exposure to fresh air and sunshine, an environment that promotes health with low cost [9]. Limited research had been performed on the association between OA and sleep, with inconclusive results [10–13]. According to a study focused on adult women [11], those who spent more time on OA had better sleep than those who had less time outdoors. On the contrary, Sijtsma et al. [12] found no association between outdoor play and sleep duration among children age 2–5 years, and Lin et al. [10] also found this result in children 10–13 years old. In a study of children in 8 European countries [13], time spent playing outside was associated with sleep in univariate analyses, but this association did not persist in multivariate analyses. Sampling heterogeneity may compromise the power of studies [10–13]; therefore, multi-center studies with larger sample sizes are necessary.
Our study investigated: (i) distribution of OA among different age groups of Chinese school-aged children and adolescents, (ii) the prevalence of insufficient sleep in Chinese school-aged children, and (iii) the association between OA time and insufficient sleep among different age and gender groups. We hypothesized that insufficient OA time is associated with insufficient sleep in Chinese children age 6–17 years.
Material and Methods
Participant enrollment
Seven provinces (Beijing, Tianjin, Liaoning, Ningxia, Shanghai, Hunan, and Guangdong) which represent the northern, northeastern, northwestern, eastern, central, and southern areas of China, were chosen as research centers [14]. In each center, multi-level stratified cluster random sampling was conducted, then we recruited children and collected baseline information from September to November 2013. Finally, approximately 12–16 primary and secondary schools (except for special education schools for children with severe physical or mental disability) with at least a total of 10 000 students aged 6–17 years were enrolled in each center. With school permission, all parents of participants signed the informed consent. Overall, there were 62 517 children who participated in this study.
Questionnaire survey
A Structured questionnaire was used to collect data, including demographic factors (age, gender, education level of mother and father, urban/rural area), lifestyle (daily hours of vigorous and moderate physical activities, walking, and sedentary, daily OA time, and sleep duration) and dietary pattern (daily servings of fruit, vegetables, sugary beverages, and meat). The questionnaire was designed based on the multi-factors model, which was proved to be acceptable for participants in the early stages of the project [14].
Details of the questionnaire distribution and quality control can be found in a previous publication [15]. Questionnaire items are described briefly as follows:
OA
OA was obtained by the question, “How many hours each day do you spend on outdoor activity? including but not restricted ball sports, swimming, hide and seek and so on (except for just sitting or lying down outside).” Outdoor activity was categorized as <1 h, 1–2 h (excluding for 2 h) and ≥2 h.
Sleep duration
Sleep duration determined by asking, “How many hours each day do you spend on sleep? just calculate the duration between fall asleep time and awake time (the period between bedtime and falling asleep time should be omitted).” The response options included <7 h, 7–9 h (excluding for 9 h), and ≥9 h.
Definition of ISD
Based on NSF recommendations, ISD is defined as “less than 9 h per day” for school-aged children. Because this was a national study, it was difficult create subgroups; it is more appropriate to regard 9 h of sleep (median of 8–10 h) for children 14–17 years old as the cut-off point.
Daily PA, sedentary behavior, dietary pattern, and anthropometric measurement
The details of questionnaire information about PA, sedentary behavior, and dietary pattern and details of anthropometric measurement have been reported elsewhere [15].
Statistical analysis
Data analyses were performed with SPSS 24.0. We performed descriptive analyses for all the data, in which continuous variables were expressed as mean values and standard deviation, and categorical variables were expressed as percentage. We conducted t tests and one-way analysis of variance to evaluate the sex differences and OA differences of continuous variables, respectively; Student-Newman-Keuls test was conducted for post hoc analyses between different outdoor time groups. Chi-square tests were performed to evaluated the differences in categorical variables. Logistic regression models were run to evaluate the association between OA and ISD, with the <1 h OA group as reference, which was adjusted for age, gender, urban/rural area, father’s education, mother’s education, body mass index (BMI), dietary pattern, PA, and sedentary behavior. Robustness testing indicated that the results did not differ across areas and schools. Regression results are presented using odds ratios (ORs) and corresponding 95% confidence intervals (CIs). P values <0.05 were interpreted as statistically significant.
Results
Characteristics of participants
The study flow chart is shown in Figure 1. The sample comprised 62 517 children, with 46 639 children (missing data: 25.40%) aged 6–17 years (mean 10.82 years, 50.9% boys) included in final analysis. There were 15 878 children excluded from the analysis due to lack of sleep and OA information. Compared with those included in analysis, children with missing information had no differences in age, height, level of VPA and MPA, and servings of fruits vegetables consumed. The baseline characteristics of the participants are described in Table 1 and Supplementary Table 1. The overall prevalence of ISD was 74.9% (73.7% in boys, 76.1% in girls, p<0.001) and 37.5% of the participants reported daily OA time less than 1 h. More girls had <1 h OA time than boys (Table 1). Children tended to have increased OA time as they age from 6 to 10 years, but this trend reversed when they prepared to enter puberty (Figure 2). Similar patterns occur in both boys and girls.
Figure 1.
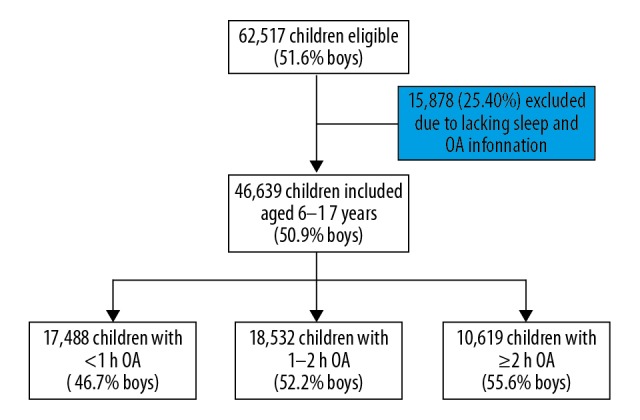
The flow chart of the study.
Table 1.
Sample characteristics by gender.
| ALL | Boy | Girl | P | |
|---|---|---|---|---|
| Sample size | 46639 | 23743 (50.9%) | 22896 (49.1%) | |
| Age | 10.82±3.31 | 10.69±3.27 | 10.95±3.35 | <0.001 |
| Outdoor activity (%) | ||||
| <1 h | 37.5 | 34.4 | 40.7 | <0.001 |
| 1–2 h | 39.7 | 40.8 | 38.7 | |
| ≥2 h | 22.8 | 24.9 | 20.6 | |
| Insufficient sleep duration (%) | 74.9 | 73.7 | 76.1 | <0.001 |
| 6–13 years | 68.2 | 67.6 | 68.8 | 0.022 |
| 14–17 years | 96.4 | 95.1 | 97.5 | <0.001 |
| Sedentary | 5.68±3.69 | 5.51±3.66 | 5.85±3.72 | <0.001 |
| 6–13 years | 5.25±3.49 | 5.18±3.49 | 5.32±3.49 | <0.001 |
| 14–17 years | 7.07±3.97 | 6.69±4.00 | 7.41±3.92 | <0.001 |
| Doing homework | 1.92±1.21 | 1.87±1.19 | 1.97±1.23 | <0.001 |
| 6–13 years | 1.73±1.11 | 1.72±1.11 | 1.74±1.11 | 0.127 |
| 14–17 years | 2.52±1.32 | 2.39±1.32 | 2.64±1.31 | <0.001 |
| Watching TV | 0.91±1.02 | 0.95±1.04 | 0.87±1.00 | 0.01 |
| 6–13 years | 0.95±0.96 | 0.99±1.00 | 0.90±0.91 | <0.001 |
| 14–17 years | 0.78±1.19 | 0.76±1.12 | 0.80±1.24 | 0.130 |
| Playing computer game | 0.68±1.09 | 0.79±1.22 | 0.58±0.93 | <0.001 |
| 6–13 years | 0.61±0.98 | 0.70±1.09 | 0.51±0.83 | <0.001 |
| 14–17 years | 0.93±1.37 | 1.10±1.56 | 0.78±1.16 | <0.001 |
| Urban/rural area (%) | ||||
| Urban | 62.1 | 61.8 | 62.4 | 0.181 |
| Rural | 37.9 | 38.2 | 37.6 | |
| BMI (kg/m2) | 18.60±3.79 | 18.90±3.98 | 18.28±3.57 | <0.001 |
| 6–13 years | 17.88±3.55 | 18.30±3.75 | 17.44±3.25 | <0.001 |
| 14–17 years | 20.87±3.66 | 21.03±4.01 | 20.73±3.31 | <0.001 |
| Physical activity (PA, hour/day) | ||||
| VPA | 0.46±0.72 | 0.53±0.76 | 0.39±0.67 | <0.001 |
| 6–13 years | 0.46±0.67 | 0.51±0.71 | 0.41±0.61 | <0.001 |
| 14–17 years | 0.45±0.86 | 0.59±0.90 | 0.33±0.80 | <0.001 |
| MPA | 0.46±0.71 | 0.50±0.75 | 0.42±0.66 | <0.001 |
| 6–13 years | 0.47±0.69 | 0.49±0.72 | 0.44±0.65 | <0.001 |
| 14–17 years | 0.43±0.77 | 0.52±0.84 | 0.36±0.70 | <0.001 |
| Walking | 0.76±1.08 | 0.79±1.14 | 0.72±1.01 | <0.001 |
| 6–13 years | 0.73±1.05 | 0.76±1.11 | 0.70±0.98 | <0.001 |
| 14–17 years | 0.84±1.15 | 0.92±1.23 | 0.77±1.07 | <0.001 |
BMI – body mass index; PA – physical activity; VPA – vigorous physical activity; MPA – moderate physical activity. P value presented as the difference between boys and girls.
Figure 2.

Distribution of daily outdoor activity time among children aged 6–17 years in China. (A) Data from all of the subjects; (B) data from boys; (C) data from girls.
Participants characteristic among OA time groups
In total, the prevalence of ISD was highest in children with <1 h OA time (78.3%, Table 2), and lowest in children with ≥2 h OA time (70.0%, Table 2), and the trend remained when stratified by age and gender (all p<0.001, Table 2).
Table 2.
Sample characteristics by outdoor activity.
| <1 h | 1–2 h | ≥2 h | P | |
|---|---|---|---|---|
| N | 17488 (37.5%) | 18532 (39.7%) | 10619 (22.8%) | |
| Age | 10.82±3.31 | 10.69±3.27 | 10.95±3.35 | <0.001 |
| Insufficient sleep duration (%) | 78.3 | 74.5 | 70.0 | <0.001 |
| 6–13 years | 70.6 | 68.8 | 63.6 | <0.001 |
| Boys | 69.5 | 68.5 | 63.6 | <0.001** |
| Girls | 71.5 | 69.0 | 63.6 | <0.001 |
| 14–17 years | 97.6 | 95.8 | 94.6 | <0.001# |
| Boys | 96.7 | 95.1 | 92.7 | <0.001 |
| Girls | 98.2 | 96.5 | 97.0 | <0.001*,# |
| Sedentary | 5.98±3.87 | 5.61±3.57 | 5.31±3.56 | <0.001 |
| Doing homework | 2.01±1.25 | 1.85±1.16 | 1.87±1.23 | <0.001# |
| Watching TV | 0.81±0.99 | 0.90±0.96 | 1.09±1.14 | <0.001 |
| Playing computer game | 0.59±1.07 | 0.66±1.01 | 0.87±1.25 | <0.001 |
| Urban/rural area (%) | ||||
| Urban | 64.6 | 61.8 | 58.6 | <0.001 |
| Rural | 35.4 | 38.2 | 41.4 | |
| Father’s education (%) | ||||
| Low | 68.2 | 69.4 | 75.0 | <0.001** |
| High | 31.8 | 30.6 | 25.0 | |
| Mather’s education (%) | ||||
| Low | 71.0 | 71.6 | 77.6 | <0.001** |
| High | 29.0 | 28.4 | 22.4 | |
| BMI | 18.62±3.79 | 18.52±3.77 | 18.69±3.83 | 0.001* |
| Physical activity (PA, hour/day) | ||||
| VPA | 0.27±0.47 | 0.46±0.58 | 0.77±1.09 | <0.001 |
| MVA | 0.30±0.50 | 0.47±0.61 | 0.71±1.02 | <0.001 |
| Walking | 0.58±0.86 | 0.76±1.00 | 1.06±1.41 | <0.001 |
| Dietary pattern (servings/day) | ||||
| Fruit | 1.15±0.99 | 1.30±1.04 | 1.48±1.23 | <0.001 |
| Vegetable | 1.67±1.35 | 1.82±1.38 | 1.99±1.53 | <0.001 |
| Sugar beverage | 0.37±0.69 | 0.38±0.71 | 0.45±0.80 | <0.001** |
| Meat | 1.10±1.11 | 1.14±1.11 | 1.23±1.29 | <0.001 |
BMI – body mass index; PA – physical activity; VPA – vigorous physical activity; MPA – moderate physical activity.
No significant difference between group <1 h and group >2 h;
no significant difference between group <1 h and group 1–2 h;
no significant difference between group 1–2 h and group >2 h.
Compared with children who had <1 h OA time, participants who had ≥2 h OA time were younger and had less daily sedentary time (p<0.001, Table 2), but had higher daily VPA, MPA, and walking time (all p<0.001, Table 2). In sedentary behavior, children with ≥2 h OA time had a longer daily time watching TV and playing computer games (both p<0.001, Table 2), and shorter daily time doing homework (p<0.001, Table 2) compared with children with <1 h OA time. In dietary pattern, compared to children with <1 h OA time, those with ≥2 h OA time had more intake of food (fruit, vegetable, sugary beverage, and meat) (all p<0.001, Table 2). Participants who had OA time ≥2 h also were more likely to have both parents with low educational level and were more likely came from a rural area, when compared with the <1 h OA group (all p<0.001, Table 2). A similar trend was found when we compared the 1–2 h OA group with the <1 h OA group, although the intake of sugary beverages and the distribution difference of caregiver’s educational level became non-significant.
Association between OA time and ISD
The ORs for ISD are presented in Table 3. Compared with the <1 h OA time group, both the 1–2 h OA group and ≥2 h OA group were significantly associated with ISD (ORs: 0.85 and 0.60, 95% CI: 0.80–0.89 and 0.56–0.63, respectively, Table 3) after adjustment for age and gender, similar association (ORs: 0.87 and 0.64, 95% CI: 0.82–0.93 and 0.59–0.69, respectively, Table 3) were found in multivariate analysis.
Table 3.
Odds ratio (OR) and 95% confidence interval (CI) for insufficient sleep duration according to outdoor activity time among children aged 6–17 years.
| <1 h | 1–2 h | ≥2 h | |
|---|---|---|---|
| Age- and gender-adjusted | 1 | 0.85 (0.80, 0.89)# | 0.60 (0.56, 0.63)# |
| Multivariate-adjusted* | 1 | 0.87 (0.82, 0.93)# | 0.64 (0.59, 0.69)# |
| Age | |||
| 6–13 years* | 1 | 0.91 (0.85, 0.97)# | 0.67 (0.62, 0.72)# |
| 14–17 years* | 1 | 0.73 (0.54, 0.97)# | 0.69 (0.49, 0.98)# |
| Age/gender groups | |||
| 6–13 years | |||
| Boys** | 1 | 0.94 (0.86, 1.03) | 0.70 (0.62, 0.77)# |
| Girls** | 1 | 0.87 (0.80, 0.96)# | 0.64 (0.57, 0.71)# |
| 14–17years | |||
| Boys** | 1 | 0.79 (0.52, 1.20) | 0.62 (0.39, 0.99)# |
| Girls** | 1 | 0.61 (0.40, 0.93)# | 0.87 (0.49, 1.54) |
Adjusted for age, gender, urban/rural area, father’s education, mother’s education, BMI, dietary pattern, physical activity and inactivity;
adjusted for age, urban/rural area, father’s education, mother’s education, BMI, dietary pattern, physical activity and inactivity;
p<0.05.
Stratified by age and relative to the OA <1 h group, OA ≥2 h was inversely associated with ISD in both age groups (multivariate-adjusted, ORs: 0.67 and 0.69; 95% CI: 0.62–0.72 and 0.49–0.98, 6–13 years old and 14–17 years old, respectively, Table 3), as well as the 1–2 h OA group (multivariate-adjusted, ORs: 0.91 and 0.73, 95% CI: 0.85–0.97 and 0.54–0.97, respectively, Table 3).
Further stratified by gender, for boys with ≥2 h OA, a lower ISD risk relative to <1 h OA was found in the 6–13 years group and 14–17 years group (ORs: 0.70 and 0.62; 95% CI: 0.62–0.77 and 0.39–0.99, respectively, Table 3), and their female counterparts showed a similar trend (ORs: 0.64 and 0.87; 95% CI: 0.57–0.71 and 0.49–1.54, aged 6–13 and aged 14–17 groups, respectively, Table 3), although in the 14–17 years group, the relationship became non-significant. Relative to <1 h OA, although the p value was >0.05, boys 6–13 years and 14–17 years that had 1–2 h OA showed an inverse trend with ISD risk (ORs: 0.94 and 0.79; 95% CI: 0.86–1.03 and 0.52–1.20, respectively, Table 3). For girls, OA with 1–2 h was inversely associated with ISD in each age group (ORs: 0.87 and 0.61; 95% CI: 0.80–0.96 and 0.40–0.93, respectively, Table 3).
Discussion
Sleep is essential for physical and mental health of children [16], but ISD has become a serious epidemic. Although age [7], BMI [17], and lifestyle [18] are known to play important roles, the mechanism underlying these effects is unclear due to the complexity of sleep behavior. By performing a multi-center national survey of Chinese children, we determined that 37.5% of Chinese children had less than 1 h of OA time per day. Moreover, OA time increased as school-aged children aged to 10 years, then decreased during the period 11–17 years (Figure 2). Most importantly, more than 2 h of OA is associated with decreased risk of ISD in boys aged 6–17 years and girls aged 6–13 years, but 1–2 h OA is associated with decreased risk of ISD only in girls aged 6–17 years.
In our study, the rate of ISD was 74.9% (Table 1), which is consistent with previous research [19] in China. Considering the academic burden Chinese children generally face, it is easier to understand the relatively high level of ISD [20]. A previous study showed the rate of ISD is higher in girls than in boys [21], which was confirmed by our research (Table 1), and this may be explained by research showing that girls need less sleep than boys [21]. The discrepancy between school-aged and adolescent age groups (Table 1), puberty onset [22], and academic burden increased by age [23] may account for this.
We found that the average daily PA time for Chinese children generally met the WHO requirement (moderate to vigorous PA, Table 1) [24]. To the best of our knowledge, there is no recommendation for OA. Our literature review showed that a 1-h increase in daily OA would benefit children (e.g., reduced risk of myopia [25] and increased PA [26]). However, in our study, 37.5% of children had less than 1 h of OA (Table 1). It is not surprising that children in urban area of China have decreased opportunity to play outdoors [27] due to the crowed environment in cities and lack of open spaces for play [28]. Considering that the 7 centers we chose were mainly urban areas (Table 2), it is easy to understand the relatively high proportion of children who have <1 h OA time. Interestingly, having less than 1 h OA becomes more common when children age from 11 to 17 years old (Figure 2), whereas the opposite trend is found in children age 6–10 years. Children spend more time outdoors before puberty onset [29,30], and the decreased activity after age 11 years may be related to the increasing academic burden that limits time for OA [29]. We found that boys had more OA than girls (Table 1), which is also in accordance with previous research [30]. The activity preference is gender-dependent, as girls tend to prefer quiet and less active play, while boys tend prefer outdoor vigorous activity [30], thus explaining the gender differences in our results.
In the multivariate analyses, we found that increased OA time was associated with decreased risk of ISD, after univariate and multivariate adjustment (Table 3). Compared with PA, OA increases exposure to sunlight and fresh air [31], which is believed to benefit night sleep [32,33]. Although the mechanism is unknown, it is accepted that OA is associated with sleep [11,34]. For humans, a normal circadian rhythm strongly depends on cues from sunlight and the subsequent restricted melatonin release [35,36], which can prevent children from falling to sleep in the daytime. Lack of sunlight at night causes melatonin levels to surge (the dim light onset effect) [36], which promotes sleep onset, which could be one reason that OA time is associated with longer sleep duration. In addition, exposure to fresh air could be another beneficial effect of outdoor play. Compared with indoor activity, playing outside provides children a well-ventilated environment. It is reported that sufficient oxygen may protect against sleep problems [37]; thus, we speculate that OA helps children maintain long sleep duration by providing fresh air and normal circadian rhythm.
Many studies [30] have reported that boys are more active than girls (Table 1). Furthermore, it widely accepted that boys need more sleep than girls [21]. This may indicate that males need to spend more time on OA to reach the same effect as females to achieve decreased risk of ISD, which might account for the slightly different results in boys and girls. Compared to <1 h OA time, children who spend more than 2 h on OA showed significantly decreased risk of ISD, except for teenage girls, in which the relationship became non-significant, although the trend was still present (Table 3). In a previous review [38], decreased outdoor time was found to be related to increased use of electronic media. In further analysis, we also found that, compared to those with 1–2 h OA, teenage girls who had ≥2 h OA spent more time watching TV (0.85±1.24 vs. 0.96±1.21, 1–2 h and ≥2 h, respectively, p<0.05) and playing computer games (0.82±1.09 vs. 0.96±1.26, 1–2 h and ≥2 h, respectively, p<0.05). Use of electronic media is believed to be negatively associated with sleep duration among children and adolescents [39]. Based on the above evidence, we speculate that the association between OA and ISD among girls in the 14–17 years group may be affected by the consumption of TV and computer games to became non-significant.
We used <9 h as the criteria of insufficient sleep due to the NSF’s recommendation and our study’s relatively wide age span. Although one study defined inadequate sleep duration as <10 h (for ages 6–11) and <9 h (for 12–17 years old), but based on our previous research [15], our criteria is more appropriate for Chinese children. Thus, it could be that the different criteria we used could be why our results disagree with several previous studies [10,12,13]. On the other hand, the age composition and ethnic cultural background of study samples, which have been thought to be relevant to sleep [6,13], could also be another cause of conflicting results.
To the best of our knowledge, this is the first study exploring the association of self-reported OA and sleep time among Chinese children aged 6–17 years, using a representative national multi-center dataset. In addition, both PA and OA were assessed, as PA adjusted, the results can elucidate the single effect of OA for sleep duration. We found that age and gender are specific factors when considering the relationship between OA and ISD, and the inner mechanism still needs further research to confirm.
This study has several limitations. Firstly, causal inferences about the relationship between outdoor time and sleep duration cannot be elucidated due to the cross-sectional design. Secondly, the use of self-reported sleep duration and outdoor playing time may have recall bias, and the questionnaire we used has not been tested for reliability and validity. The items of sleep and OA we collected were presented as categorical values, which may involve some loss of information. The use of longitudinal designs, objective tools, and continuous variables to assess sleep duration and outdoor time in further researches would improve our understanding of the relationship between sleep and OA. As previously reported, attending school and studying are the main psychological stressors among Chinese children [40], which could be a contributor to inadequate sleep duration. However, in a national survey with a large sample size, it is difficult to collect all information related to the outcomes of interest, and in future we will try to explore more psychological stressors. Furthermore, our study only focused on the duration of sleep and outdoor time during the whole week, which fails to differentiate between weekday and weekend, and sleep quality and OA type could be relevant to consider in future studies.
Conclusions
In summary, this study provides initial evidence that sufficient time spent outdoors is associated with decreased risk of insufficient sleep in children 6–17 years old in China. The association is age- and gender-dependent, which suggest the definition of sufficient OA time should consider the factors of age and gender. Based on our findings, further research is warranted to determine the age and gender effects on the association between OA and ISD, and to investigate whether the intervention of promoting time spent outdoors is a useful way to prevent insufficient sleep in children.
Supplementary Data
Supplementary Table 1.
Sample characteristics by gender.
| ALL | Boy | Girl | P | |
|---|---|---|---|---|
| Sample size | 46639 | 23743 (50.9%) | 22896 (49.1%) | |
| Height (cm) | 145.86±17.09 | 146.88±18.48 | 144.79±15.45 | <0.001 |
| 6–13 years | 139.90±14.66 | 140.20±14.92 | 139.62±14.37 | <0.001 |
| 14–17 years | 164.81±8.20 | 170.52±6.78 | 159.73±5.60 | <0.001 |
| Weight (kg) | 41.07±15.64 | 42.48±17.06 | 39.62±13.87 | <0.001 |
| 6–13 years | 36.11±13.07 | 37.13±13.87 | 34.99±12.05 | <0.001 |
| 14–17 years | 56.94±12.24 | 61.38±13.46 | 52.98±9.42 | <0.001 |
| Waist circumference (cm) | 64.89±10.83 | 66.00±11.61 | 63.74±9.84 | <0.001 |
| 6–13 years | 62.56±10.23 | 63.75±10.93 | 61.26±9.24 | <0.001 |
| 14–17 years | 72.32±9.24 | 73.94±10.37 | 70.89±7.82 | <0.001 |
| Hip circumference (cm) | 77.15±12.09 | 77.03±12.20 | 77.27±11.97 | 0.032 |
| 6–13 years | 73.33±10.68 | 73.45±10.68 | 73.20±10.67 | 0.03 |
| 14–17 years | 89.35±7.31 | 89.69±8.13 | 89.04±6.49 | <0.001 |
| Father’s education (%) | ||||
| Low | 70.2 | 70.8 | 69.7 | 0.015 |
| High | 29.8 | 29.2 | 30.3 | |
| Mother’s education (%) | ||||
| Low | 72.7 | 73.1 | 72.3 | 0.088 |
| High | 27.3 | 26.9 | 27.7 | |
| Dietary pattern (servings/day) | ||||
| Fruit | 1.28±1.07 | 1.27±1.11 | 1.30±1.03 | 0.002 |
| 6–13 years | 1.34±1.09 | 1.33±1.13 | 1.35±1.05 | 0.065 |
| 14–17 years | 1.11±0.99 | 1.06±1.01 | 1.16±0.97 | <0.001 |
| Vegetable | 1.80±1.41 | 1.81±1.44 | 1.79±1.38 | 0.078 |
| 6–13 years | 1.81±1.41 | 1.81±1.44 | 1.82±1.37 | 0.791 |
| 14–17 years | 1.76±1.42 | 1.81±1.45 | 1.71±1.39 | <0.001 |
| Sugar beverage | 0.39±0.72 | 0.47±0.83 | 0.31±0.58 | <0.001 |
| 6–13 years | 0.33±0.63 | 0.38±0.72 | 0.27±0.52 | <0.001 |
| 14–17 years | 0.60±0.92 | 0.80±1.07 | 0.43±0.72 | <0.001 |
| Meat | 1.14±1.16 | 1.27±1.27 | 1.02±1.02 | <0.001 |
| 6–13 years | 1.13±1.14 | 1.23±1.24 | 1.01±1.00 | <0.001 |
| 14–17 years | 1.20±1.22 | 1.39±1.35 | 1.02±1.06 | <0.001 |
P value presented as the difference between boys and girls.
Acknowledgements
We thank all the children and their families for their participation. We also thank all the teachers and school doctors who distributed questionnaire and conducted anthropometric measurements and the postgraduate student who helped with the survey.
Abbreviations
- BMI
body mass index
- CI
confidence interval
- NSF
National Sleep Foundation
- OA
outdoor activity
- OR
odds ratio
- ISD
insufficient sleep duration
- PA
physical activity
- VPA
vigorous physical activity
- MPA
moderate physical activity
Footnotes
Conflict of interest
None.
Source of support: This work was funded by Ministry of Health (public welfare special fund, 2012, No. 201202010), National Natural Science foundation, P.R. China (No. 81872639) and Guangdong Medical Science Foundation, P.R. China (No. A2018136)
References
- 1.Beebe DW. Cognitive, behavioral, and functional consequences of inadequate sleep in children and adolescents. Pediatr Clin North Am. 2011;58:649–65. doi: 10.1016/j.pcl.2011.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health. 2015;1:40–43. doi: 10.1016/j.sleh.2014.12.010. [DOI] [PubMed] [Google Scholar]
- 3.Matricciani L, Olds T, Petkov J. In search of lost sleep: Secular trends in the sleep time of school-aged children and adolescents. Sleep Med Rev. 2012;16:203–11. doi: 10.1016/j.smrv.2011.03.005. [DOI] [PubMed] [Google Scholar]
- 4.Spilsbury JC, Storfer-Isser A, Drotar D, et al. Sleep behavior in an urban US sample of school-aged children. Arch Pediatr Adolesc Med. 2004;158:988–94. doi: 10.1001/archpedi.158.10.988. [DOI] [PubMed] [Google Scholar]
- 5.National Sleep Foundation. 2006 Teens and sleep. Sleep in America poll: Summary of findings. 2006. http://www.sleepfoundation.org/sleep-polls-data/sleep-in-america-poll/2006-teens-and-sleep.
- 6.Olds T, Maher C, Blunden S, Matricciani L. Normative data on the sleep habits of Australian children and adolescents. Sleep. 2010;33:1381–88. doi: 10.1093/sleep/33.10.1381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sluggett L, Wagner SL, Hardy C, Harris RL. Associations between sleep duration and indicators of cardiometabolic disease in Canadian children and adolescents: Analyses of the 2007–2009 Canadian Health Measures Survey. Childhood Obesity. 2016;12:325–3. doi: 10.1089/chi.2015.0214. [DOI] [PubMed] [Google Scholar]
- 8.Lin Y, Tremblay MS, Katzmarzyk PT, et al. Temporal and bi-directional associations between sleep duration and physical activity/sedentary time in children: An international comparison. Prev Med. 2018;111:436–41. doi: 10.1016/j.ypmed.2017.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Liu J, Sekine M, Tatsuse T, et al. Outdoor physical activity and its relation with self-reported health in Japanese children: Results from the Toyama birth cohort study. Child Care Health Dev. 2015;41:920–27. doi: 10.1111/cch.12262. [DOI] [PubMed] [Google Scholar]
- 10.Lin Y, Borghese MM, Janssen I. Bi-directional association between sleep and outdoor active play among 10–13 year olds. BMC Public Health. 2018;18:224. doi: 10.1186/s12889-018-5122-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Murray K, Godbole S, Natarajan L, et al. The relations between sleep, time of physical activity, and time outdoors among adult women. PLoS One. 2017;12:e182013. doi: 10.1371/journal.pone.0182013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sijtsma A, Koller M, Sauer PJJ, Corpeleijn E. Television, sleep, outdoor play and BMI in young children: the GECKO Drenthe cohort. Eur J Pediatr. 2015;174:631–39. doi: 10.1007/s00431-014-2443-y. [DOI] [PubMed] [Google Scholar]
- 13.Hense S, Barba G, Pohlabeln H, et al. Factors that influence weekday sleep duration in European children. Sleep. 2011;34:633–39. doi: 10.1093/sleep/34.5.633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chen Y, Ma L, Ma Y, et al. A national school-based health lifestyles interventions among Chinese children and adolescents against obesity: Rationale, design and methodology of a randomized controlled trial in China. BMC Public Health. 2015;15:210. doi: 10.1186/s12889-015-1516-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cao M, Zhu Y, He B, et al. Association between sleep duration and obesity is age- and gender-dependent in Chinese urban children aged 6–18 years: A cross-sectional study. BMC Public Health. 2015 doi: 10.1186/s12889-015-2359-0. 15L 1029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Matricciani L, Bin YS, Lallukka T, et al. Past, present, and future: Trends in sleep duration and implications for public health. Sleep Health. 2017;3:317–23. doi: 10.1016/j.sleh.2017.07.006. [DOI] [PubMed] [Google Scholar]
- 17.Sivertsen B, Pallesen S, Sand L, Hysing M. Sleep and body mass index in adolescence: Results from a large population-based study of Norwegian adolescents aged 16 to 19 years. BMC Pediatr. 2014;14:204. doi: 10.1186/1471-2431-14-204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tambalis KD, Panagiotakos DB, Psarra G, Sidossis LS. Insufficient sleep duration is associated with dietary habits, screen time, and obesity in children. J Clin Sleep Med. 2018;14:1689–96. doi: 10.5664/jcsm.7374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Song C, Gong W, Ding C, et al. Sleep duration among Chinese children and adolescents aged 6–17 years old. Chin J Sch Health. 2017;38:1288–90. [Google Scholar]
- 20.Jiang X, Hardy LL, Baur LA, et al. Sleep duration, schedule and quality among urban Chinese children and adolescents: Associations with routine after-school activities. PLoS One. 2015;10:e115326. doi: 10.1371/journal.pone.0115326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Keyes KM, Maslowsky J, Hamilton A, Schulenberg J. The great sleep recession: Changes in sleep duration among US adolescents,1991–2012. Pediatrics. 2015;135:460–68. doi: 10.1542/peds.2014-2707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Carskadon MA, Vieira C, Acebo C. Association between puberty and delayed phase preference. Sleep. 1993;16:258–62. doi: 10.1093/sleep/16.3.258. [DOI] [PubMed] [Google Scholar]
- 23.Van Schalkwijk FJ, Blessinga AN, Willemen AM, et al. Social support moderates the effects of stress on sleep in adolescents. J Sleep Res. 2015;24:407–13. doi: 10.1111/jsr.12298. [DOI] [PubMed] [Google Scholar]
- 24.Tremblay MS, Carson V, Chaput J, et al. Canadian 24-hour movement guidelines for children and youth: An integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2016;41(6 Suppl 3):S311–27. doi: 10.1139/apnm-2016-0151. [DOI] [PubMed] [Google Scholar]
- 25.Sherwin JC, Reacher MH, Keogh RH, et al. The association between time spent outdoors and myopia in children and adolescents. Ophthalmology. 2012;119:2141–51. doi: 10.1016/j.ophtha.2012.04.020. [DOI] [PubMed] [Google Scholar]
- 26.Silva P, Santos MP. Playing outdoor and practising sport: A study of physical activity levels in Portuguese children. Eur J Sport Sci. 2017;17:208–14. doi: 10.1080/17461391.2016.1226389. [DOI] [PubMed] [Google Scholar]
- 27.Guo Y, Liu LJ, Xu L, et al. Outdoor activity and myopia among primary students in rural and urban regions of Beijing. Ophthalmology. 2013;120:277–83. doi: 10.1016/j.ophtha.2012.07.086. [DOI] [PubMed] [Google Scholar]
- 28.Jim CY, Chen WY. Recreation – amenity use and contingent valuation of urban greenspaces in Guangzhou, China. Landscape and Urban Planning. 2006;75:81–96. [Google Scholar]
- 29.Bringolf-Isler B, Grize L, Mäder U, et al. Built environment, parents’ perception, and children’s vigorous outdoor play. Prev Med. 2010;50:251–56. doi: 10.1016/j.ypmed.2010.03.008. [DOI] [PubMed] [Google Scholar]
- 30.Klinker CD, Schipperijn J, Kerr J, et al. Context-specific outdoor time and physical activity among school-children across gender and age: Using accelerometers and GPS to advance methods. Front Public Health. 2014;2:20. doi: 10.3389/fpubh.2014.00020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ngo C, Saw S, Dharani R, Flitcroft I. Does sunlight (bright lights) explain the protective effects of outdoor activity against myopia? Ophthalmic Physiol Opt. 2013;33:368–72. doi: 10.1111/opo.12051. [DOI] [PubMed] [Google Scholar]
- 32.Lee H, Kim S, Kim D. Effects of exercise with or without light exposure on sleep quality and hormone reponses. J Exerc Nutr Biochem. 2014;18:293–99. doi: 10.5717/jenb.2014.18.3.293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Buman MP, King AC. Exercise as a treatment to enhance sleep. American Journal of Lifestyle Medicine. 2010;4:500–14. [Google Scholar]
- 34.Xu H, Wen LM, Hardy LL, Rissel C. Associations of outdoor play and screen-time with nocturnal sleep duration and pattern among young children. Acta Paediatr. 2016;105(3):297–303. doi: 10.1111/apa.13285. [DOI] [PubMed] [Google Scholar]
- 35.Bauer M, Glenn T, Alda M, et al. Relationship between sunlight and the age of onset of bipolar disorder: An international multisite study. J Affect Disord. 2014;167:104–11. doi: 10.1016/j.jad.2014.05.032. [DOI] [PubMed] [Google Scholar]
- 36.Smolensky MH, Sackett-Lundeen LL, Portaluppi F. Nocturnal light pollution and underexposure to daytime sunlight: Complementary mechanisms of circadian disruption and related diseases. Chronobiol Int. 2015;32:1029–48. doi: 10.3109/07420528.2015.1072002. [DOI] [PubMed] [Google Scholar]
- 37.Bub KL, Buckhalt JA, El-Sheikh M. Children’s sleep and cognitive performance: A cross-domain analysis of change over time. Dev Psychol. 2011;47:1504–14. doi: 10.1037/a0025535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.McCurdy LE, Winterbottom KE, Mehta SS, Roberts JR. Using nature and outdoor activity to improve children’s health. Curr Probl Pediatr Adolesc Health Care. 2010;40:102–17. doi: 10.1016/j.cppeds.2010.02.003. [DOI] [PubMed] [Google Scholar]
- 39.LeBourgeois MK, Hale L, Chang A, et al. Digital media and sleep in childhood and adolescence. Pediatrics. 2017;140:S92–96. doi: 10.1542/peds.2016-1758J. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Huang X, Zhu G. Stressors and coping strategies among 1485 middle school students, Beijing. Chinese Preventive Medicine. 2011;12:860–64. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Table 1.
Sample characteristics by gender.
| ALL | Boy | Girl | P | |
|---|---|---|---|---|
| Sample size | 46639 | 23743 (50.9%) | 22896 (49.1%) | |
| Height (cm) | 145.86±17.09 | 146.88±18.48 | 144.79±15.45 | <0.001 |
| 6–13 years | 139.90±14.66 | 140.20±14.92 | 139.62±14.37 | <0.001 |
| 14–17 years | 164.81±8.20 | 170.52±6.78 | 159.73±5.60 | <0.001 |
| Weight (kg) | 41.07±15.64 | 42.48±17.06 | 39.62±13.87 | <0.001 |
| 6–13 years | 36.11±13.07 | 37.13±13.87 | 34.99±12.05 | <0.001 |
| 14–17 years | 56.94±12.24 | 61.38±13.46 | 52.98±9.42 | <0.001 |
| Waist circumference (cm) | 64.89±10.83 | 66.00±11.61 | 63.74±9.84 | <0.001 |
| 6–13 years | 62.56±10.23 | 63.75±10.93 | 61.26±9.24 | <0.001 |
| 14–17 years | 72.32±9.24 | 73.94±10.37 | 70.89±7.82 | <0.001 |
| Hip circumference (cm) | 77.15±12.09 | 77.03±12.20 | 77.27±11.97 | 0.032 |
| 6–13 years | 73.33±10.68 | 73.45±10.68 | 73.20±10.67 | 0.03 |
| 14–17 years | 89.35±7.31 | 89.69±8.13 | 89.04±6.49 | <0.001 |
| Father’s education (%) | ||||
| Low | 70.2 | 70.8 | 69.7 | 0.015 |
| High | 29.8 | 29.2 | 30.3 | |
| Mother’s education (%) | ||||
| Low | 72.7 | 73.1 | 72.3 | 0.088 |
| High | 27.3 | 26.9 | 27.7 | |
| Dietary pattern (servings/day) | ||||
| Fruit | 1.28±1.07 | 1.27±1.11 | 1.30±1.03 | 0.002 |
| 6–13 years | 1.34±1.09 | 1.33±1.13 | 1.35±1.05 | 0.065 |
| 14–17 years | 1.11±0.99 | 1.06±1.01 | 1.16±0.97 | <0.001 |
| Vegetable | 1.80±1.41 | 1.81±1.44 | 1.79±1.38 | 0.078 |
| 6–13 years | 1.81±1.41 | 1.81±1.44 | 1.82±1.37 | 0.791 |
| 14–17 years | 1.76±1.42 | 1.81±1.45 | 1.71±1.39 | <0.001 |
| Sugar beverage | 0.39±0.72 | 0.47±0.83 | 0.31±0.58 | <0.001 |
| 6–13 years | 0.33±0.63 | 0.38±0.72 | 0.27±0.52 | <0.001 |
| 14–17 years | 0.60±0.92 | 0.80±1.07 | 0.43±0.72 | <0.001 |
| Meat | 1.14±1.16 | 1.27±1.27 | 1.02±1.02 | <0.001 |
| 6–13 years | 1.13±1.14 | 1.23±1.24 | 1.01±1.00 | <0.001 |
| 14–17 years | 1.20±1.22 | 1.39±1.35 | 1.02±1.06 | <0.001 |
P value presented as the difference between boys and girls.