

Abstract
Juvenile localized scleroderma (morphea) is the predominant scleroderma in childhood which affects the skin and may extend to the underlying fascia, muscle, joints and bone. The assessment of activity and damage can be done with a validated instrument like LoSCAT. Disease classified as “low severity” which includes superficial plaque morphea can be treated with topical mid potent- potent steroids, tacrolimus, calcipotriol or imiquimod in combination with phototherapy. Methotrexate is recommended for linear, deep and generalized morphea. Steroids are effective in the early inflammatory stage and used in combination with methotrexate. Methotrexate is continued for at least 12 months after adequate response is achieved. Mycophenolate mofetil is given in cases where methotrexate is contraindicated or for those who do not respond to methotrexate. There are also reports of improvement of disease with ciclosporine and hydroxychloroquine. In severe cases, recalcitrant to standard therapy there may be a role for biologics, JAK inhibitors, and IVIG. Supportive measures like physiotherapy and psychiatric counseling are also important in the management of morphea. Orthopedic surgery and other measures like autologous fat transfer may be advocated once the disease is inactive.
Keywords: Children, management, morphea
Introduction
Localized scleroderma or morphea, an autoimmune disorder, is the most common form of scleroderma in children. It involves the skin and can extend to the fascia, muscle, and bone. About 20% of patients can develop extracutaneous features including arthritis, uveitis, and seizures. In about 50% of patients the disease undergoes spontaneous resolution, the shortest active disease duration being in plaque morphea (2.7 years) and longer in deep morphea (5.5 years).[1]
Classification
Morphea in children (juvenile localized scleroderma) has been classified by Zulian and Laxer.[2] The different types described are:
(1) Circumscribed morphea, subtypes - superficial and deep, (2) Linear scleroderma, subtypes - trunk/limbs and head and neck, (3) Generalized morphea, (4) Pansclerotic morphea, and (5) Mixed morphea.
Demographics
The disease is reportedly more prevalent in Caucasians with an annual incidence of 2.7 per 100,000.[1] It is more prevalent in females. The mean age of onset of disease is between 6-9 years.[3] Congenital forms have been described.[4]
Pathogenesis
A variety of factors are involved in the occurrence of morphea. These include autoimmunity, genetic predisposition (HLA class I and II alleles), and environmental triggers (infections, trauma, toxins, drugs and radiation). The fibrosis which occurs is secondary to a series of events that occurs in the skin, starting with an influx of mononuclear cells which infiltrate the dermis and surround the blood vessels. This is followed by vascular injury resulting in functional and structural changes in the vessels, especially the vessels underlying the epidermis. There is also upregulation of adhesion molecules like intercellular adhesion molecule1 and vascular cell adhesion molecule in response to cytokines such as IFN-γ, IL-1 and TNFs. Interleukin-4 (IL-4) produced by the CD4+ Th2 lymphocytes upregulates the production of transforming growth factor-beta (TGF-β). The fibrosis is induced by excessive TGF-β and IL-4 activity.[5,6]
Cutaneous Manifestations[2,3]
Linear morphea/linear scleroderma
Linear scleroderma presents as linear indurated plaques with dyspigmentation on the limbs, head (en coup de sabre), or rarely the trunk. The lesions may follow lines of Blaschko. When it crosses a joint there may be resultant immobility. The lesions may extend to the underlying muscle or bone causing atrophy and thinning of the affected limb [Figure 1].
Figure 1.

Linear morphea affecting the left lower limb
Linear scleroderma affecting the frontal or frontoparietal region with or without hemifacial atrophy is called en coup de sabre type of morphea [Figure 2].
Figure 2.

En coup de sabre or linear scleroderma of the frontoparietal region
Parry Romberg syndrome is associated with hemiatrophy of the face without dermal sclerosis [Figure 3].
Figure 3.

Parry Romberg syndrome causing hemiatrophy of the face
Plaque morphea
Plaque type of morphea presents as skin colored, brownish, hypopigmented, or ivory white lesions on the trunk [Figure 4]. Smaller lesions, few millimeters in size, are called guttate lesions [Figure 5].
Figure 4.

Plaque type morphea with brownish indurated plaques on the trunk
Figure 5.

Hypopigmented guttate lesions on the dorsa of hands
Deep morphea
Deep morphea as the name indicates affects the deeper tissues, causing deep seated induration, the overlying skin may appear normal, slightly pigmented or slightly erythematous.
Disabling pansclerotic morphea/pansclerotic morphea
Disabling pansclerotic morphea affects skin and subcutaneous tissue with fixity to the underlying structures. It usually affects females, is relentlessly progressive, with widespread involvement, causing joint contractures and limiting mobility [Figure 6]. It can be differentiated from diffuse systemic sclerosis in that the generalized sclerosis spares the fingertips and toes.
Figure 6.

Involvement of the lower limbs in pansclerotic morphea
Mixed morphea refers to occurrence of two or more subtypes in the patient. In children, linear morphea often occurs in association with the plaque type.
Hypopigmented lesions were described in 54% of patients in one series and may even resemble vitiligo.[7]
Other rare variants include atrophoderma of Pasini and Pierini and bullous morphea.[8,9]
There are only about 25 cases of congenital morphea reported in world literature and the data has been reviewed.[4] The most common subtype seen was linear morphea. Associated extracutaneous manifestations were musculoskeletal in those with limb involvement and neurologic in those with lesions on the head. The overall prognosis was good.
Extracutaneous Features
In a study of 750 patients with juvenile localized scleroderma (JLS), 22.4% had extracutaneous manifestations which included articular (47.2%), neurologic (17.1%), vascular (9.3%), ocular (8.3%), gastrointestinal (6.2%), respiratory (2.6%), cardiac, and renal.[6]
Musculoskeletal involvement is usually associated with linear scleroderma affecting the limbs and includes arthralgia, arthritis, joint contracture, atrophy of the limb, limb length discrepancies, and gait abnormalities.
In en coup de sabre type, the patient may have neurological abnormalities like migraine, trigeminal neuralgia, seizures, behavioral changes, and learning disability. The ocular abnormalities include absence of eyebrows and eyelashes on the affected areas, enophthalmos, anterior uveitis, and myopathy of the eye muscles.[3] The oral and dental abnormalities (odontostomatologic abnormalities) include malocclusion, skeletal asymmetry, overgrowth of the anterior lower third of the face, temporomandibular joint involvement, and hemiatrophy of the ipsilateral tongue.[10]
Disabling pansclerotic morphea has been associated with restrictive pulmonary disease, bronchopneumonia, cardiomyopathy, gastrointestinal reflux, gangrene, and squamous cell carcinoma.[11,12,13]
The most common vascular abnormality reported is Raynaud's phenomenon, other rare associations include deep vein thrombosis and vasculitis.[6]
Associated autoimmune diseases include psoriasis, vitiligo, alopecia areata, SLE, Sjogren's disease, and rheumatoid arthritis. The association is highest with generalized morphea.[14]
Differential diagnosis of morphea in children (Text box 1)
Text box 1.
Differential diagnosis
| Hyperpigmented patches |
| Fixed drug eruption |
| Macular lichen planus |
| Post inflammatory hyperpigmentation |
| Hypopigmented patches/guttate lesions |
| Vitiligo |
| Lichen sclerosus |
| Erythematous patches |
| Acquired port wine stain |
| Linear lesions |
| Linear atrophoderma of Moulin |
| Acrodermatitis chronica atrophicans (Lyme disease) |
| Linear melorheostosis |
| Plaque morphea |
| Chronic graft versus host disease |
| Hypertrophic scar/keloid |
| Connective tissue nevi |
| Post radiation |
| Deep morphea |
| Lipodystrophy |
| Other forms of panniculitis |
| Pansclerotic morphea |
| Systemic sclerosis |
The differential diagnosis depends on the stage of disease and the type of morphea. Difficulty and delay in the diagnosis of morphea in children occurs because early morphea can present as nonspecific hypopigmented or hyperpigmented lesions. Morphea presenting as hyperpigmented patches may mimic fixed drug eruption and macular lichen planus, both of which can be distinguished from morphea by their distinct histopathological features.
Early lesions of morphea have been mistaken for acquired port wine stains resulting in delayed diagnosis.[15]
Indurated plaques of morphea may resemble hypertrophic scars or keloids or connective tissue nevi from which it can be distinguished, if needed, by histopathology.
Guttate and plaque type of morphea may resemble extragenital lichen sclerosus et atrophicus. The absence of delling points towards a diagnosis of morphea. The two conditions may also occur together in the same patient.
Morphea profunda may mimic localized lipodystrophy which in some cases may be iatrogenic (following steroid injections).
The linear form of atrophoderma (linear atrophoderma of Moulin) lacks the inflammation and induration associated with linear morphea.[16] Other conditions that may mimic linear morphea are acrodermatitis chronica atrophicans (Lyme disease) and linear melorheostosis, the latter may co-exist with linear morphea.[17] X ray of the bone shows the characteristic “flowing candlewax pattern” caused by the irregular and wavy sclerotic changes.[18]
Pansclerotic and generalized morphea share features of widespread sclerosis as seen in systemic sclerosis but spares the fingers and toes as mentioned earlier.[19]
Assessment of Activity of Disease (Text box 2)
Text box 2.
Assessment of activity of skin lesions
| Clinical features: Appearance of new lesions, extension of existing plaques, warmth, lilac borders, skin induration and edema |
| LoSCAT, Physician's global assessment |
| Ultrasound (20 MHz) |
| Skin Biopsy |
| Clinical inactivity: |
| No erythema, no new or enlarging lesions in the last 3 months, no change in thickness, no worsening of joint contractures, PGA. Visual analog scale of 0, no active extracutaneous features |
| Assessment of extracutaneous involvement |
| Skeletal X rays- linear scleroderma involving limbs, special attention to the affected joints |
| Lesions affecting scalp and face |
| MRI brain |
| Ophthalmic evaluation |
| Orthodontist/maxillofacial surgeon |
| Focused systemic evaluation in patients with pansclerotic morphea |
Clinical assessment of activity and damage
The disease exhibits an early active phase and a late fibrotic phase. The clinical features that suggest activity of disease are appearance of new lesions, extension of existing plaques, erythema, tactile warmth, violaceous/lilac color bordering the sclerosis (not always discernable on types V-VI skin), and skin induration/edema.
Features of damage include dyspigmentation, atrophy, and skin thickening. There is lack of hair growth and veins may be visible.[14]
Signs of activity and damage may be present concurrently. Treatment should be directed at only the active lesions.
Localized scleroderma cutaneous assessment tool (LoSCAT)
The Localized scleroderma cutaneous assessment tool LoSCAT[20] consists of:
Localized scleroderma skin severity index (LoSSI) which includes 4 domains: Surface area, degree of erythema, skin induration, and appearance of new lesions or extension of old lesions, each one graded from 0 to 3 in 18 anatomic sites (The mLoSSI or modified LoSSI does not take the surface area into account)
Localized Scleroderma Skin Damage index (LoSDI) which is calculated by summing up 3 scores indicating damage, dermal atrophy, subcutaneous atrophy, and dyspigmentation.
The Physician's Global Assessment (PGA) of disease activity and damage is done using a 100 mm visual analog scale.
High frequency ultrasound
High frequency ultrasound is a noninvasive tool used in the diagnosis of morphea and has also proved useful in the assessment of response to treatment [Figures 7 and 8].[21] The sensitivity and specificity of ultrasound diagnosis was found to be 100% and 98.8%, respectively, in a study of 51 patients with morphea with echogenicity of the subcutaneous tissue and increased blood flow being the most accurate signs of activity.[22]
Figure 7.
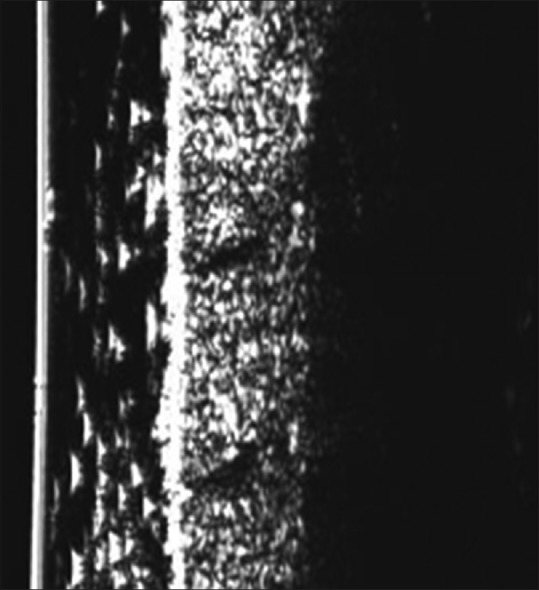
Dermascan (20 Megahertz) in active disease on the abdomen showing increased thickening and decreased echogenicity of the dermis and increased echogenicity of the subcutis
Figure 8.
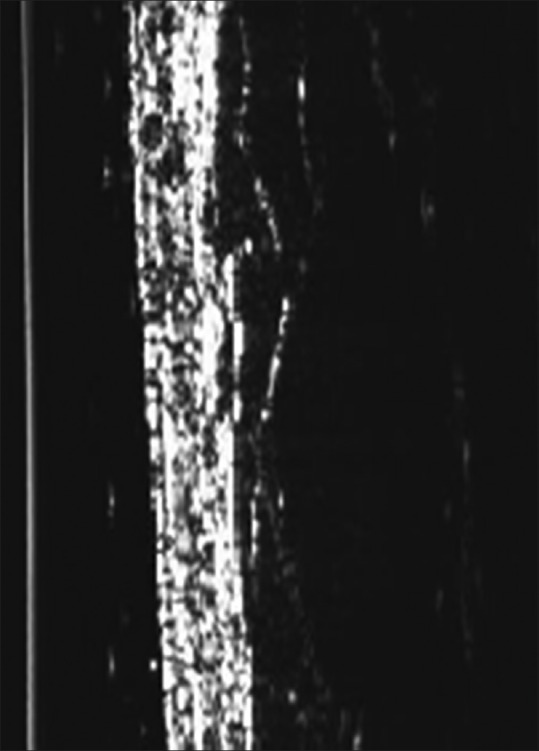
Dermascan (20 MHz) on normal skin showing hyperechoic dermis and hypoechogenicity of subcutaneous tissue with intervening hyperechoic fibrous septa
Infrared thermography
Infrared thermography which measures infrared heat generated from the body has been used to detect active lesions in children with morphea. It has a sensitivity and specificity of 92% and 68%, respectively, presence of atrophy may result in false positive results.[23]
Other tools used to measure activity of disease include computerized skin score which measures activity of a single lesion, durometer which measures skin hardness, and cutimeter which measures skin elasticity and relaxation. The clinical utility of these instruments is still not known as they have not been adequately studied.[24]
Prognosis
Most patients with JLS have a good prognosis and achieve remission.[25] However, the course may be prolonged in some patients. One study showed that about 12.5% of patients, all with linear variant, showed activity of disease even after 10 years of follow up. The delay in start of therapy was associated with longer disease activity. Functional damage is more prevalent in pansclerotic, linear, and mixed types of morphea. Disease reactivation is seen most often within 2 years of discontinuation of treatment warranting close follow up during that period.[25]
Causes for Relapse of Disease
The relapse rate in one study was reported to be 50%. The causes identified were ANA positivity and older age of onset (disease onset ≥10 years). Noncompliance with medication also contributed to relapse.[26]
Aims of Treatment
The aims of treatment are to arrest activity of disease, induce inactivity, prevent disfigurement, joint contractures and mobility restriction.
Inactivity has been defined by an expert panel including PRES (Pediatric Rheumatology European Society) Scleroderma Working Group by the following features- no erythema, no new or enlarging lesions in the last 3 months, no change in thickness, no worsening of joint contractures, physician's global assessment on visual analog scale of 0, and no active extracutaneous involvement.
Remission is defined as 12 months of disease inactivity. The treatment should not be stopped before 12 months of disease inactivity.[27]
Investigations
Routine laboratory investigations: CBC, LFT, creatinine, urine microscopic examination, ESR, and CRP.
Eosinophilia, elevated ESR and CRP and hypergammaglobulinemia are markers of activity, usually seen in association with generalized, deep, and pansclerotic morphea. Elevated creatinine kinase and aldolase are seen in patients with new lesions.[28]
Autoantibody screen: ANA is positive in about 50% of patients with JLS.[2] Rheumatoid factor may be positive in children with active arthritis.[29] Anti-histone antibodies and anti-single stranded DNA are associated with increased severity of disease.[30] Other antibodies like anti-topoisomerase and anti-centromere are rarely positive in children.
Skin biopsy
The diagnosis of morphea is usually based on clinical features. Skin biopsies aid in establishing the diagnosis in doubtful cases. Deep biopsies including the subcutis are required. In the early inflammatory phase there is a dermal infiltrate of lymphocytes, plasma cells, eosinophils, and mast cells with increased deposition of collagen. In the late sclerotic stage, the collagen in the dermis appears thickened and hypocellular, the inflammation is sparse, eccrine glands are atrophic and appear higher as a result of replacement of subcutaneous tissue by collagen and blood vessels are reduced in number with thickened walls and narrow lumens. There is loss of CD34+ dendritic cells [Figures 9 and 10].[31] A recent study has shown that a bottom-heavy pattern of sclerosis and severe inflammation in biopsy specimens correlate with pain, tightness, and functional limitation in patients with morphea.[32]
Figure 9.
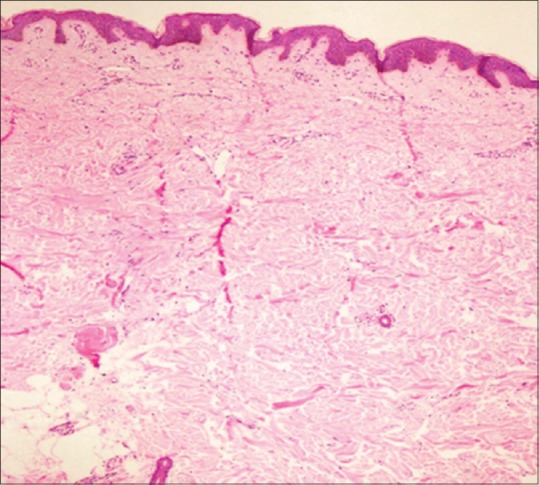
H and E: Late sclerotic phase with atrophy of adnexal structures. Eccrine glands are situated at a relatively high level in the dermis with sparse superficial perivascular inflammation (10×)
Figure 10.
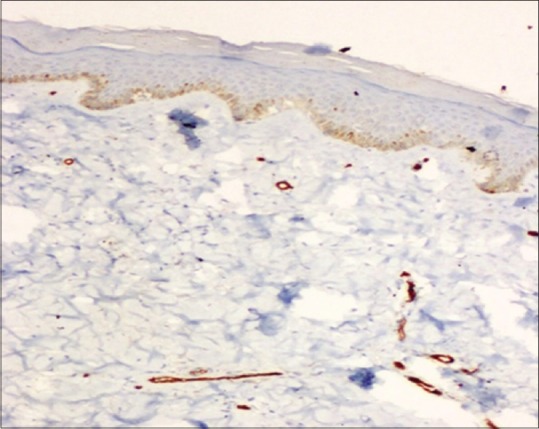
Marked reduction of CD 34 immunostain (10×)
MRI
MRI of the brain is recommended by Zulian F et al. for all patients with morphea affecting the face, head and neck.[29] The changes reported include cerebral atrophy, white matter lesions, intraparenchymal calcifications, and vascular involvement.[33]
MRI is also useful to gauge the depth of involvement and activity of deep morphea.[34]
Treatment
The choice of treatment is decided by (i) the type of morphea (superficial vs deep), (ii) sites of involvement (face/limbs/trunk), (iii) localized or generalized in distribution, (iv) presence of extracutaneous involvement, (v) feasibility (example-phototherapy), (vi) cost and, (vii) risk-benefit ratio.
Immunosuppressive treatment should be avoided during immunization with live vaccines.
Childhood Arthritis and Rheumatology Research Alliance (CARRA), a subgroup of the pediatric rheumatology research network, defines low severity disease as “circumscribed superficial morphea not associated with subcutaneous atrophy, extracutaneous involvement, or scalp hair loss. Moderate to high-disease severity includes all other subtypes, and patients who have deeper tissue or extracutaneous involvement”.[35]
“Low severity” disease can be managed by topical or intralesional steroids, tacrolimus, calcipotriol, or calcipotriol and steroid combination, imiquimod, and/or phototherapy.[3] However, patients do need to be monitored for progression or increase in depth of involvement.
Topical Treatment
Topical Tacrolimus
Topical tacrolimus 0.1% has proved to be effective in the treatment of plaque morphea in a randomized placebo-controlled study done on 10 patients. The ointment was applied twice daily for 12 weeks resulting in significant reduction in clinical activity. Studies have also confirmed that it is more effective when used in early inflamed lesions than late sclerotic lesions.[36,37]
Topical steroids
Active, solitary, superficial small-moderately sized plaques may be treated with fluticasone ointment or mometasone ointment. Improvement is seen in 6–12 weeks. To avoid steroid-induced atrophy, continuous use should be avoided.[38]
Intralesional triamcinolone acetonide 10 mg/ml may be given to the edges of active lesions of en coup de sabre (avoid injecting close to the eye) to decrease inflammation.[39]
Calcipotriol and calcipotriol- steroid combination
Topical vitamin D analogues like calcipotriene/calcipotriol either alone or in combination with steroids have been shown to be effective in the treatment of morphea in prospective open label studies.[40,41] One of the suggested mechanisms of action is through inhibition of Th2 cytokine and TGFβ-induced periostin expression.[42]
Imiquimod
5% imiquimod has been found to be effective in the treatment of pediatric morphea in a prospective open label study recruiting 9 patients, wherein at the end of 36 weeks there was a reduction in thickness of the plaque. One patient developed ulceration of the plaque. It is thought that imiquimod acts by inducing the release of various cytokines including γ interferon, which in turn inhibits the fibroblast production of collagen and glycosaminoglycan.[43]
Systemic treatment
Methotrexate-steroid combination
An early open labeled study on the use of oral corticosteroids in doses of 0.5–1 mg/kg alone showed that it was effective in the early inflammatory phase of the disease.[44]
Methotrexate has been widely used in the treatment of morphea with good results. One retrospective study evaluating methotrexate used both as monotherapy and in combination with steroids in 17 patients found it to be effective, the average time to remission and methotrexate being discontinued was 19.6 months. However, 8/17 patients required more than one course of methotrexate.[45] In a randomized, double blind, placebo-controlled trial, which included 46 patients in the methotrexate group and 24 in the placebo group (both groups having received oral steroids 1 mg/kg in the initial part of treatment for 3 months followed by a taper), patients on methotrexate (15 mg/m2/week) significantly improved as compared to the placebo group.[46]
Experts have veered towards the use of methotrexate in combination with systemic steroids.[24,29] Systemic steroids can be administered orally or intravenously, two schedules that have been used (1) prednisolone 1-2 mg/kg for 2-3 months with subsequent gradual tapering or (2) pulsed intravenous methylprednisolone given once a month.[47] Methotrexate given in a dose of 15 mg/m2/week either orally or subcutaneously is usually continued for 12 months after satisfactory improvement is achieved, after which it may be tapered and stopped, although in some cases longer duration of treatment may be warranted.[29] The relapse rate was lower in those on longer periods of treatment with methotrexate.[46] Cytokines of Th1, Th2, and Th17 lineage are implicated in the pathogenesis of scleroderma, both systemic and localized.[48] The mechanism of action of methotrexate is through reduction in levels of IL-1, IL-2, IL-4, and IL-6 which results in improvement in sclerosis.[46]
In summary, in patients with progressive, disabling morphea or lesions that are cosmetically disfiguring, the current recommendation is to give methotrexate 15 mg/m2/week either orally or subcutaneously (maximum 25 mg/m2/week). Systemic steroids are given in the initial phase of treatment for a minimum period of 3 months. It is effective in the early inflammatory stage of the disease.[27,29]
Mycophenolate mofetil
Mycophenolate mofetil has been found to be effective in the treatment resistant JLS.[49] In a retrospective chart review of 10 patients who had severe treatment resistant disease, the addition of MMF 600–1200 mg/m2/day twice daily to patients receiving concomitant methotrexate or treated in the past with it, resulted in a favorable response with good clinical improvement seen within a mean period of 3.5 months. The mechanism of action is secondary to the antifibrotic and immunosuppressive actions of the drug. It is recommended in children with treatment resistant disease.[29]
Hydroxychloroquine (HCQ)
This drug has been shown to be effective in the treatment of morphea in a retrospective study of 84 patients between the ages of 4–77 years. 93% of patients showed either complete or partial response. The only side effect experienced was nausea.[50] Maximal response was seen in a median time of 12 months. The most recent recommendations for the treatment of juvenile localized scleroderma does not mention HCQ.[29] Further prospective studies are required to establish its role in the treatment of morphea in children.
Ciclosporine
Retrospective analysis of the use of ciclosporine in patients with severe morphea has shown the drug to be effective. Of the 12 patients, both children and adults were included, 5 showed complete remission. The dose ranged from 1.2 to 3 mg/kg and the mean duration of treatment was 18.6 months. Three patients received concomitant steroids.[51] When given early in the course of disease it prevents contractures.
Biologics and small molecules
The evidence for the use of biologics and small molecules is based on case reports. In most instances the agents have been used in severe therapy resistant cases of morphea.
Toculizumab is an anti- IL-6 receptor monoclonal antibody that has been reported to be effective in the treatment of pansclerotic morphea.[52] IL-6 levels have been found to be elevated in localized scleroderma. It is a proinflammatory cytokine which stimulates fibroblast activity and increases collagen synthesis. It was added to methotrexate for the treatment of pansclerotic morphea by Zhang et al. The common side effects were infections, cytopenias, transaminitis, and hypercholesterolemia.[52] Bosentan has been found to be effective in the treatment of intractable cutaneous ulcers of pansclerotic morphea.[53]
Ruxolitinib has been tried in pansclerotic morphea with minimal response.[11] The mechanism of action is thought to be by inhibition of IL-4 signaling there by decreasing collagen synthesis and extracellular matrix deposition by the fibroblasts. Studies in animal models suggest that TGF-β induced fibrosis is JAK2 dependent.[54,55]
Everolimus (mTOR inhibitor) used as salvage therapy to treat generalized morphea in an adult has shown promising results.[56]
Infliximab was found to be to be effective in recalcitrant morphea in a 14-year-old girl. Leflunomide was added to prevent the development of neutralizing antibodies.[57]
Subcutaneous immunoglobulin has been shown to be effective when injected subcutaneously into lesional skin in a case of deep morphea at a dose of 1.6 gm twice weekly, resulting in clinical and histopathological improvement.[58] Intravenous immunoglobulin has been tried in pansclerotic morphea with variable response.[59]
Phototherapy/Photochemotherapy
Oral psoralen and UVA (PUVA can also be instituted as a bath or topical application), UVA1 and UVB (narrow band and broad band), targeted phototherapy and extracorporeal photochemotherapy have been used in the treatment of JLS. It is generally not useful if deeper structures like subcutis or fascia or muscle are involved.[38] Most of the available data are from studies done in adults.
UVA and UVA1 have a longer wavelength leading to deeper penetration. The actions of UVA are multiple ranging from decrease in TGF-β, increase in interferon γ, apoptosis of Langerhans cells and T cells, induction of metalloproteinases that degrade collagen and inhibition of collagen synthesis.[60] The limitations of UVA1 are the lack of availability in most centers, diminished effectiveness after repeated treatment due to increase in pigment, and need for longer exposure times.[61] The recurrence rate is about 46%.[39] There are also reports of limited efficacy of UVA1 in Fitzpatrick IV-VI skin types.
A recent meta-analysis of studies comparing effectiveness of methotrexate with that of UVA therapy with or without psoralen has shown that methotrexate with glucocorticoids was superior to UVA. UVA1 is indicated in patients with disease that does not cross joints or lead to cosmetic damage.[62]
In a prospective study, 13 patients including those in the pediatric age group were treated with systemic PUVA, topical PUVA, and narrow band UVB. The patient was subjected to only one type of treatment. The treatment was effective in all patients regardless of the modality chosen and improvement was evident by both clinical assessment and ultrasound examination.[63]
In summary, the current recommendation by experts is to use phototherapy, UVA1 or narrow band UVB, preferably for children >12 years with superficial, non-progressive morphea that does not cross joints or occurring in “non-cosmetically sensitive areas”.[27]
Orthopedic complications
Patients with linear scleroderma are particularly prone to orthopedic complications. In one study, 51% of children had orthopedic complications, of whom 88% had joint contractures, this occurred despite immunosuppressive therapy, making it important to involve orthopedic surgeons early in the management of disease.[64] German guidelines recommend that functional surgical correction should be done only in the inactive stage of the disease, several years after the end of disease activity. Concurrent physiotherapy (except in the acute inflammatory stage) to improve mobility, muscle strengthening and build up exercises, massage, and manual lymphatic drainage have also been recommended by the same group.[38]
Other surgical and cosmetic procedures
Reconstructive surgery including autologous fat transfers, and injection of fillers for correction of cosmetic problems in en coup de sabre form of localized scleroderma can be done once the disease is inactive.[38] One expert group recommends a minimum of 6 months of disease inactivity.[27]
Psychosocial burden of disease
Morphea is a disease with a negative impact on the quality of life. One study found that female gender and the number of extracutaneous features impacted the quality of life in children.[65] The study also found that medical management together with supportive measures improving the physical and mental well-being decreased the negative impact on the QOL. Professional counseling and intervention should be offered to those at risk of depression and other complications.
The consensus-based recommendations for the treatment of JLS has been recently published.[29]
The current recommendation for the management of moderate to severe morphea is methotrexate in combination with systemic steroids as an initial “bridge therapy”. In cases of resistance or failure of therapy, the options are mycophenolate mofetil, ciclosporine, and hydroxychloroquine. Phototherapy has a role in superficial morphea along with topical therapy but interference with the school schedule is a major deterrent to the routine use in children. Topical therapy with steroids, combination of calcipotriol-steroid (fixed-combination), or tacrolimus is used in limited disease. An algorithmic approach to the treatment of morphea has been shown in Figure 11.
Figure 11.

Treatment of morphea: algorithmic approach
Burnt out and inactive morphea does not require medical treatment but reconstructive surgery or autologous fat transfer, if feasible should be considered and patients referred to a plastic surgeon. Professional counseling by a psychologist will help those with cosmetically disfiguring disease. Biologics have been used in the treatment of pansclerotic and deep morphea not responding to conventional therapy.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Peterson LS, Nelson AM, Su WP, Mason T, O’Fallon WM, Gabriel SE. The epidemiology of morphea (localized scleroderma) in Olmsted County 1960-1993. J Rheumatol. 1997;24:73–80. [PubMed] [Google Scholar]
- 2.Laxer RM, Zulian F. Localized scleroderma. Curr Opin Rheumatol. 2006;18:606–13. doi: 10.1097/01.bor.0000245727.40630.c3. [DOI] [PubMed] [Google Scholar]
- 3.Li SC. Scleroderma in children and adolescents: Localized scleroderma and systemic sclerosis. Pediatr Clin North Am. 2018;65:757–81. doi: 10.1016/j.pcl.2018.04.002. [DOI] [PubMed] [Google Scholar]
- 4.Mansour M, Liy Wong C, Zulian F, Li S, Morishita K, Yeh EA, et al. Natural history and extracutaneous involvement of congenital morphea: Multicenter retrospective cohort study and literature review. Pediatr Dermatol. 2018;35:761–8. doi: 10.1111/pde.13605. [DOI] [PubMed] [Google Scholar]
- 5.Badea I, Taylor M, Rosenberg A, Foldvari M. Pathogenesis and therapeutic approaches for improved topical treatment in localized scleroderma and systemic sclerosis. Rheumatology. 2009;48:213–21. doi: 10.1093/rheumatology/ken405. [DOI] [PubMed] [Google Scholar]
- 6.Zulian F, Vallongo C, Woo P, Russo R, Ruperto N, Harper J, et al. Localized scleroderma in childhood is not just a skin disease. Arthritis Rheum. 2005;52:2873–81. doi: 10.1002/art.21264. [DOI] [PubMed] [Google Scholar]
- 7.Sung JJ, Chen TS, Gilliam AC, McCalmont TH, Gilliam AE. Clinicohistopathological correlations in juvenile localized scleroderma: Studies on a subset of children with hypopigmented juvenile localized scleroderma due to loss of epidermal melanocytes. J Am Acad Dermatol. 2011;65:364–73. doi: 10.1016/j.jaad.2010.02.065. [DOI] [PubMed] [Google Scholar]
- 8.Kencka D, Blaszczyk M, Jabłońska S. Atrophoderma Pasini-Pierini is a primary atrophic abortive morphea. Dermatology. 1995;190:203–6. doi: 10.1159/000246685. [DOI] [PubMed] [Google Scholar]
- 9.Daoud MS, Su WP, Leiferman KM, Perniciaro C. Bullous morphea: Clinical, pathologic, and immunopathologic evaluation of thirteen cases. J Am Acad Dermatol. 1994;30:937–43. doi: 10.1016/s0190-9622(94)70113-x. [DOI] [PubMed] [Google Scholar]
- 10.Trainito S, Lorenzo F, Martini G, Klit Pedersen T, Favero V, Herlin T, et al. Odontostomatologic involvement in juvenile localised scleroderma of the face. J Paediatr Child Health. 2012;48:572–6. doi: 10.1111/j.1440-1754.2012.02435.x. [DOI] [PubMed] [Google Scholar]
- 11.Jie Soh H, Samuel C, Heaton V, Douglas Renton W, Cox A, Munro J. Challenges in the diagnosis and treatment of disabling pansclerotic morphea of childhood: Case-based review. Rheumatol Int. 2019;39:933–41. doi: 10.1007/s00296-019-04269-w. [DOI] [PubMed] [Google Scholar]
- 12.Wollina U, Buslau M, Heinig B, Petrov I, Unger E, Kyriopoulou E, et al. Disabling pansclerotic morphea of childhood poses a high risk of chronic ulceration of the skin and squamous cell carcinoma. Int J Low Extrem Wounds. 2007;6:291–8. doi: 10.1177/1534734607308731. [DOI] [PubMed] [Google Scholar]
- 13.Kura MM, Jindal SR. Disabling pansclerotic morphea of childhood with extracutaneous manifestations. Indian J Dermatol. 2013;58:159. doi: 10.4103/0019-5154.108079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Torok KS. Pediatric scleroderma: Systemic or localized forms. Pediatr Clin North Am. 2012;59:381–405. doi: 10.1016/j.pcl.2012.03.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nijhawan RI, Bard S, Blyumin M, Smidt AC, Chamlin SL, Connelly EA. Early localized morphea mimicking an acquired port-wine stain. J Am Acad Dermatol. 2011;64:779–82. doi: 10.1016/j.jaad.2009.10.017. [DOI] [PubMed] [Google Scholar]
- 16.Kharkar VD, Abak BA, Mahajan SA. Linear atrophoderma of moulin: A rare entity. Indian J Dermatol Venereol Leprol. 2018;84:591–4. doi: 10.4103/ijdvl.IJDVL_136_17. [DOI] [PubMed] [Google Scholar]
- 17.Birtane M, Eryavuz M, Unalan H, Tüzün F. Melorheostosis: Report of a new case with linear scleroderma. Clin Rheumatol. 1998;17:543–5. doi: 10.1007/BF01451298. [DOI] [PubMed] [Google Scholar]
- 18.Sureka B, Mittal MK, Udhaya KK, Sinha M, Mittal A, Thukral BB. Melorheostosis: Two atypical cases. Indian J Radiol Imaging. 2014;24:192–95. doi: 10.4103/0971-3026.134415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kim A, Marinkovich N, Vasquez R, Jacobe HT. Clinical features of morphea patients with the pansclerotic subtype: A cross-sectional study from the Morphea in Adults and Children (MAC cohort) J Rheumatol. 2014;41:106–12. doi: 10.3899/jrheum.130029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Arkachaisri T, Vilaiyuk S, Li S, O'Neil KM, Pope E, Higgins GC, et al. The localized scleroderma skin severity index and physician global assessment of disease activity: A work in progress toward development of localized scleroderma outcome measures. J Rheumatol. 2009;36:2819–29. doi: 10.3899/jrheum.081284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Szymańska E, Nowicki A, Mlosek K, Litniewski J, Lewandowski M, Secomski W, et al. Skin imaging with high frequency ultrasound - preliminary results. Eur J Ultrasound. 2000;12:9–16. doi: 10.1016/s0929-8266(00)00097-5. [DOI] [PubMed] [Google Scholar]
- 22.Wortsman X, Wortsman J, Sazunic I, Carreño L. Activity assessment in morphea using color Doppler ultrasound. J Am Acad Dermatol. 2011;65:942–8. doi: 10.1016/j.jaad.2010.08.027. [DOI] [PubMed] [Google Scholar]
- 23.Martini G, Murray KJ, Howell KJ, Harper J, Atherton D, Woo P, et al. Juvenile-onset localized scleroderma activity detection by infrared thermography. Rheumatology. 2002;41:1178–82. doi: 10.1093/rheumatology/41.10.1178. [DOI] [PubMed] [Google Scholar]
- 24.Fett N, Werth VP. Update on morphea: Part II. Outcome measures and treatment. J Am Acad Dermatol. 2011;64:231–42. doi: 10.1016/j.jaad.2010.05.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Martini G, Fadanelli G, Agazzi A, Vittadello F, Meneghel A, Zulian F. Disease course and long-term outcome of juvenile localized scleroderma: Experience from a single pediatric rheumatology Centre and literature review. Autoimmun Rev. 2018;17:727–34. doi: 10.1016/j.autrev.2018.02.004. [DOI] [PubMed] [Google Scholar]
- 26.Kurzinski KL, Zigler CK, Torok KS. Prediction of disease relapse in a cohort of paediatric patients with localized scleroderma. Br J Dermatol. 2019;180:1183–9. doi: 10.1111/bjd.17312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Constantin T, Foeldvari I, Pain CE, Pálinkás A, Höger P, Moll M, et al. Development of minimum standards of care for juvenile localized scleroderma. Eur J Pediatr. 2018;177:961–77. doi: 10.1007/s00431-018-3144-8. [DOI] [PubMed] [Google Scholar]
- 28.Wu EY, Li SC, Torok KS, Virkud Y, Fuhlbrigge R, Rabinovich CE. A28: Description of the juvenile localized scleroderma subgroup of the CARRA registry. Arthritis Rheum. 2014;66:S43–4. [Google Scholar]
- 29.Zulian F, Culpo R, Sperotto F, Anton J, Avcin T, Baildam EM, et al. Consensus-based recommendations for the management of juvenile localised scleroderma. Ann Rheum Dis. 2019;78:1019–24. doi: 10.1136/annrheumdis-2018-214697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Arkachaisri T, Fertig N, Pino S, Medsger TA. Serum autoantibodies and their clinical associations in patients with childhood- and adult-onset linear scleroderma. A single-center study. J Rheumatol. 2008;35:2439–44. doi: 10.3899/jrheum.080098. [DOI] [PubMed] [Google Scholar]
- 31.Walters R, Pulitzer M, Kamino H. Elastic fiber pattern in scleroderma/morphea. J Cutan Pathol. 2009;36:952–7. doi: 10.1111/j.1600-0560.2009.01201.x. [DOI] [PubMed] [Google Scholar]
- 32.Walker D, Susa JS, Currimbhoy S, Jacobe H. Histopathological changes in morphea and their clinical correlates: Results from the Morphea in Adults and Children Cohort. J Am Acad Dermatol. 2017;76:1124–30. doi: 10.1016/j.jaad.2016.12.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Amaral TN, Marques Neto JF, Lapa AT, Peres FA, Guirau CR, Appenzeller S. Neurologic involvement in scleroderma en coup de sabre. Autoimmune Dis. 2012;2012:719685. doi: 10.1155/2012/719685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Horger M, Fierlbeck G, Kuemmerle-Deschner J, Tzaribachev N, Wehrmann M, Claussen CD, et al. MRI findings in deep and generalized morphea (Localized Scleroderma) AJR Am J Roentgenol. 2008;190:32–9. doi: 10.2214/AJR.07.2163. [DOI] [PubMed] [Google Scholar]
- 35.Li SC, Torok KS, Pope E, Dedeoglu F, Hong S, Jacobe HT, et al. Development of consensus treatment plans for juvenile localized scleroderma. Arthritis Care Res (Hoboken) 2012;64:1175–85. doi: 10.1002/acr.21687. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kroft EB, Groeneveld TJ, Seyger MM, de Jong EM. Efficacy of topical tacrolimus 0.1% in active plaque morphea. Am J Clin Dermatol. 2009;10:181–7. doi: 10.2165/00128071-200910030-00004. [DOI] [PubMed] [Google Scholar]
- 37.Stefanaki C, Stefanaki K, Kontochristopoulos G, Antoniou C, Stratigos A, Nicolaidou E, et al. Topical tacrolimus 01% ointment in the treatment of localized scleroderma An open label clinical and histological study. J Dermatol. 2008;35:712–8. doi: 10.1111/j.1346-8138.2008.00552.x. [DOI] [PubMed] [Google Scholar]
- 38.Kreuter A, Krieg T, Worm M, Wenzel J, Moinzadeh P, Kuhn A, et al. German guidelines for the diagnosis and therapy of localized scleroderma. J Dtsch Dermatol Ges. 2016;14:199–216. doi: 10.1111/ddg.12724. [DOI] [PubMed] [Google Scholar]
- 39.Narbutt J, Hołdrowicz A, Lesiak A. Morphea – Selected local treatment methods and their effectiveness. Reumatologia. 2017;55:305–13. doi: 10.5114/reum.2017.72628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cunningham BB, Landells ID, Langman C, Sailer DE, Paller AS. Topical calcipotriene for morphea/linear scleroderma. J Am Acad Dermatol. 1998;39:211–5. doi: 10.1016/s0190-9622(98)70077-5. [DOI] [PubMed] [Google Scholar]
- 41.Dytoc MT, Kossintseva I, Ting PT. First case series on the use of calcipotriol-betamethasone dipropionate for morphoea. Br J Dermatol. 2007;157:615–8. doi: 10.1111/j.1365-2133.2007.07971.x. [DOI] [PubMed] [Google Scholar]
- 42.Terao M, Yang L, Matsumura S, Yutani M, Murota H, Katayama I. A vitamin D analog inhibits Th2 cytokine- and TGFβ -induced periostin production in fibroblasts: A potential role for vitamin D in skin sclerosis. Dermatoendocrinol. 2015;7:e1010983. doi: 10.1080/19381980.2015.1010983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Pope E, Doria AS, Theriault M, Mohanta A, Laxer RM. Topical imiquimod 5% cream for pediatric plaque morphea: A prospective, multiple-baseline, open-label pilot study. Dermatology. 2011;223:363–9. doi: 10.1159/000335560. [DOI] [PubMed] [Google Scholar]
- 44.Joly P, Bamberger N, Crickx B, Belaich S. Treatment of severe forms of localized scleroderma with oral corticosteroids: Follow-up study on 17 patients. Arch Dermatol. 1994;130:663–4. [PubMed] [Google Scholar]
- 45.Koch SB, Cerci FB, Jorizzo JL, Krowchuk DP. Linear morphea: A case series with long-term follow-up of young, methotrexate-treated patients. J Dermatolog Treat. 2013;24:435–8. doi: 10.3109/09546634.2013.806769. [DOI] [PubMed] [Google Scholar]
- 46.Zulian F, Martini G, Vallongo C, Vittadello F, Falcini F, Patrizi A, et al. Methotrexate treatment in juvenile localized scleroderma: A randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2011;63:1998–2006. doi: 10.1002/art.30264. [DOI] [PubMed] [Google Scholar]
- 47.Kreuter A, Gambichler T, Breuckmann F, Rotterdam S, Freitag M, Stuecker M, et al. Pulsed high-dose corticosteroids combined with low-dose methotrexate in severe localized scleroderma. Arch Dermatol. 2005;141:847–52. doi: 10.1001/archderm.141.7.847. [DOI] [PubMed] [Google Scholar]
- 48.Kurzinski K, Torok KS. Cytokine profiles in localized scleroderma and relationship to clinical features. Cytokine. 2011;55:157–64. doi: 10.1016/j.cyto.2011.04.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Martini G, Ramanan AV, Falcini F, Girschick H, Goldsmith DP, Zulian F. Successful treatment of severe or methotrexate-resistant juvenile localized scleroderma with mycophenolate mofetil. Rheumatology. 2009;48:1410–3. doi: 10.1093/rheumatology/kep244. [DOI] [PubMed] [Google Scholar]
- 50.Kumar AB, Blixt EK, Drage LA, El-Azhary RA, Wetter DA. Treatment of morphea with hydroxychloroquine: A retrospective review of 84 patients at Mayo Clinic, 1996-2013. J Am Acad Dermatol. 2019;80:1658–63. doi: 10.1016/j.jaad.2019.01.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bali G1, Frühauf J, Wutte N, Aberer E. Cyclosporine reduces sclerosis in morphea: A retrospective study in 12 patients and a literature review. Dermatology. 2016;232:503–10. doi: 10.1159/000448171. [DOI] [PubMed] [Google Scholar]
- 52.Zhang A, Nocton J, Chiu Y. A case of pansclerotic morphea treated with tocilizumab. JAMA Dermatol. 2019;155:388–89. doi: 10.1001/jamadermatol.2018.5040. [DOI] [PubMed] [Google Scholar]
- 53.Roldan R, Morote G, Castro M del C, Miranda MD, Moreno JC, Collantes E. Efficacy of bosentan in treatment of unresponsive cutaneous ulceration in disabling pansclerotic morphea in children. J Rheumatol. 2006;33:2538–40. [PubMed] [Google Scholar]
- 54.Kim SR, Charos A, Damsky W, Heald P, Girardi M, King BA. Treatment of generalized deep morphea and eosinophilic fasciitis with the Janus kinase inhibitor tofacitinib. JAAD Case Rep. 2018;4:443–5. doi: 10.1016/j.jdcr.2017.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Dees C, Tomcik M, Palumbo-Zerr K, Distler A, Beyer C, Lang V, et al. JAK-2 as a novel mediator of the profibrotic effects of transforming growth factor β in systemic sclerosis. Arthritis Rheum. 2012;64:3006–15. doi: 10.1002/art.34500. [DOI] [PubMed] [Google Scholar]
- 56.Frumholtz L, Roux J, Bagot M, Rybojad M, Bouaziz JD. Treatment of generalized deep morphea with everolimus. JAMA Dermatol. 2016;152:1170–2. doi: 10.1001/jamadermatol.2016.2338. [DOI] [PubMed] [Google Scholar]
- 57.Ferguson ID, Weiser P, Torok KS. A case report of successful treatment of recalcitrant childhood localized scleroderma with infliximab and leflunomide. Open Rheumatol J. 2015;9:30–5. doi: 10.2174/18743129014090100030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Yamazaki-Nakashimada MA, Saez-de-Ocariz M, Maldonado-Colin G, García-Romero MT. Subcutaneous immunoglobulin for the treatment of deep morphoea in a child. Clin Exp Dermatol. 2018;43:303–5. doi: 10.1111/ced.13352. [DOI] [PubMed] [Google Scholar]
- 59.Wollina U, Looks A, Schneider R, Maak B. Disabling morphoea of childhood-beneficial effect of intravenous immunoglobulin therapy. Clin Exp Dermatol. 1998;23:292–3. doi: 10.1046/j.1365-2230.1998.00378.x. [DOI] [PubMed] [Google Scholar]
- 60.El-Mofty M, Mostafa W, Esmat S, Youssef R, Bousseila M, Nagi N, et al. Suggested mechanisms of action of UVA phototherapy in morphea: A molecular study. Photodermatol Photoimmunol Photomed. 2004;20:93–100. doi: 10.1111/j.1600-0781.2004.00080.x. [DOI] [PubMed] [Google Scholar]
- 61.Sartori-Valinotti JC, Tollefson MM, Reed AM. Updates on morphea: Role of vascular injury and advances in treatment. Autoimmune Dis. 2013;2013:467808. doi: 10.1155/2013/467808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Marrani E, Foeldvari I, Lopez JA, Cimaz R, Simonini G. Comparing ultraviolet light A photo (chemo) therapy with methotrexate protocol in childhood localized scleroderma: Evidence from systematic review and meta-analysis approach. Semin Arthritis Rheum. 2018;48:495–503. doi: 10.1016/j.semarthrit.2018.03.003. [DOI] [PubMed] [Google Scholar]
- 63.Buense R, Duarte IA, Bouer M. Localized scleroderma: Assessment of the therapeutic response to phototherapy. An Bras Dermatol. 2012;87:63–9. doi: 10.1590/s0365-05962012000100007. [DOI] [PubMed] [Google Scholar]
- 64.Schoch JJ, Schoch BS, Werthel JD, McIntosh AL, Davis DM. Orthopedic complications of linear morphea: Implications for early interdisciplinary care. Pediatr Dermatol. 2018;35:43–6. doi: 10.1111/pde.13336. [DOI] [PubMed] [Google Scholar]
- 65.Ardalan K, Zigler CK, Torok KS. Predictors of longitudinal quality of life in pediatric localized scleroderma. Arthritis Care Res (Hoboken) 2017;69:1082–7. doi: 10.1002/acr.23101. [DOI] [PMC free article] [PubMed] [Google Scholar]