

Abstract
Objective:
To evaluate the hypothesis that early-onset sepsis increases risk of death or neurodevelopmental impairment (NDI) among preterm infants; and that among infants without EOS, prolonged early antibiotics alters risk of death/NDI.
Study design:
Retrospective cohort study of infants born at NICHD Neonatal Research Network centers (2006-2014) at 22-26 weeks gestation and birth weight 401-1000 grams. EOS defined as growth of a pathogen from blood or cerebrospinal fluid culture ≤72 hours after birth. Prolonged early antibiotics was defined as antibiotics initiated ≤72 hours and continued ≥5 days without culture-confirmed infection, necrotizing enterocolitis or spontaneous perforation. Primary outcome was death before follow-up or NDI assessed 18-26 months corrected age. Poisson regression was used to estimate adjusted relative risk (aRR) and confidence interval (CI) for EOS outcomes. A propensity score (PS) for receiving prolonged antibiotics was derived from early clinical factors and used to match infants (1:1) with and without prolonged antibiotic exposure. Log binomial models were used to estimate aRR for outcomes in matched infants.
Results:
Among 6565 infants, those with EOS had higher aRR (95% CI) for death/NDI compared with infants managed with prolonged antibiotics [1.18 (1.06-1.32)] and to infants without prolonged antibiotics [1.23 (1.10-1.37)]. PS matching was achieved for 4362 infants. No significant difference in death/NDI [1.04 (0.98-1.11)] was observed with or without prolonged antibiotics among the matched cohort.
Conclusion:
EOS was associated with increased risk of death/NDI among extremely preterm infants. Among matched infants without culture-confirmed infection, prolonged early antibiotic administration was not associated with death/NDI.
The American Academy of Pediatrics recommends discontinuation of empiric antibiotics when blood cultures for early-onset sepsis (EOS) remain sterile after 48 hours’ incubation (1). However, neonatal providers frequently diagnose “culture-negative infection” when an infant’s perinatal history, clinical condition or laboratory testing suggest infection even when bacterial cultures are sterile (2). Antibiotics are continued in such cases to prevent the mortality and morbidity associated with culture-confirmed infection (3). The use of prolonged early antibiotics for presumed culture-negative infection varies widely across hospitals (4–7). We previously reported that the proportion of extremely preterm infants administered prolonged early antibiotics among Neonatal Research Network (NRN) centers ranges from 10-72% for infants identified as at low risk for EOS based on delivery characteristics, and from 20-80% among the remaining infants (8). In contrast, rates of culture-confirmed EOS ranged from 0-6.7% and 0-10.4% across sites, respectively (8). Wide center-level variation in prolonged antibiotic use provides the opportunity to investigate outcomes of clinically similar infants managed with different antibiotic regimens.
There is increasing appreciation of the impact of antibiotic exposures on the developing neonatal microbiome (9), including evidence for interaction of the microbiota with brain development and function (10,11). Extremely preterm infants have a high prevalence of both antibiotic administration and of neurological sequelae (7,12). In this study, our first objective was to assess the composite risk of death or neurodevelopmental impairment (NDI) at 18-26 months corrected age (CA) for infants with culture-confirmed EOS, compared with infants with sterile cultures managed with or without prolonged early antibiotics. Our next objective was to compare the risk of death or NDI between infants with sterile cultures managed with and without prolonged early antibiotics, using propensity score (PS) methods (13) to control for potential differences in illness severity.
METHODS
This is a retrospective cohort study of infants born at NRN centers between 01/01/2006 and 12/31/2014 and enrolled in a registry of high-risk infants maintained by the NRN. Eligibility criteria were: gestational age (GA) 22 0/7-26 6/7 weeks, birth weight (BW) 401-1000 grams, inborn and survival >12 hours. Infants with major birth defects (14) may differ in indications for early antibiotics and in outcomes compared with infants without birth defects and were excluded. The registry includes prospectively collected maternal pregnancy and delivery information; infant data from birth until death, discharge/transfer, or 120 days of age; and if hospitalized at 120 days, final date of discharge/transfer or death up to one year of age (15). Surviving infants were eligible for a follow-up assessment. The institutional review board at each center approved participation in the registry and follow-up, with written parental consent or waiver of consent determined by each center’s board.
EOS was defined as blood or cerebrospinal fluid (CSF) culture obtained ≤72 hours of age that grew pathogenic bacteria or fungi, for which the infant received antibiotics ≥5 days or died with intent to receive antibiotics ≥5 days. Micrococcus, Propionibacterium, Corynebacterium, Bacillus species, and coagulase-negative staphylococci were considered contaminants. Prolonged early antibiotics was defined as a “yes” response to the question “Did the infant receive antibiotics for ≥5 days, starting within the first 72 hours?”, and included intended use ≥5 days in an infant who died.
For both objectives, the primary composite outcome was death before follow-up or NDI in survivors. Death, NDI in survivors, and components of NDI were investigated as secondary outcomes. Surviving infants were evaluated at visits between 10/2007-8/2017 and were assessed at 18-22 months CA (births before 07/01/2012) or 22-26 months CA (births on or after 07/01/2012). Follow-up assessments included review of the medical history with the primary caretaker. The child’s vision and hearing status were determined by history, testing after discharge (if available), and examination at the visit. Neurologic examination and a developmental evaluation using the Bayley Scales of Infant Development, Third Edition (Bayley-3) were administered by certified examiners (16). Cerebral palsy (CP) was defined using the gross motor function classification system (GMFCS) as mild (level ≤1), moderate (level 2-3), or severe (level 4-5) (17). NDI was defined as one or more of the following: bilateral blindness (corrected vision <20/200 in both eyes), hearing impairment (permanent hearing loss affecting communication with or without amplification), GMFCS level ≥2 with or without CP, or a Bayley-3 cognitive composite score <85 (18).
Statistical Analyses:
Infants with missing exposure variables were excluded from all analyses. Neurodevelopmental outcomes were considered missing if assessment occurred at <14 or >30 months CA (2% of those assessed). All analyses were adjusted for maternal education, maternal insurance, maternal race/ethnicity, maternal hypertension, antepartum hemorrhage, antenatal steroids, maternal antibiotics received during the delivery admission, clinical chorioamnionitis, membrane rupture >18 hours, cesarean delivery, infant GA (categorical), BW (continuous), male sex, intubation at birth, temperature <60 minutes of birth, severe intraventricular hemorrhage (IVH) ≤7 days age and start of enteral feeds ≤3 days age (12,19–22). IVH classified by Papile criteria as grade 3 or 4 was considered severe (23).
Each study objective had additional exclusions and different analytic approaches. To assess the effect of EOS, infants who died ≤12 hours of age; infants with necrotizing enterocolitis (NEC, defined by modified Bell stage ≥ IIA (24,25)), spontaneous intestinal perforation (SIP, defined as intestinal perforation without proven NEC) at ≤3 days or infants with blood or CSF culture obtained at ≤3 days growing a contaminant were excluded. Poisson regression models with robust variance estimators (26) were used to assess risk of the primary outcome of death >12 hours and before follow-up or survival with NDI while adjusting for the covariates listed above as well as for study center.
Adjusted relative risks (aRR), 95% confidence intervals (CI), and p-values by the Wald chi-square test from these models were reported. To assess the effect of prolonged early antibiotics, infants who died or were diagnosed with NEC or SIP ≤5 days and infants with a blood or CSF culture obtained at ≤5 days growing a pathogen or contaminant were excluded. We used a PS-based analysis to adjust for imbalance of baseline characteristics in infants with and without prolonged early antibiotic exposure. A logistic regression model was fit to the dependent variable “prolonged early antibiotic exposure” to derive a propensity score defined as the probability of antibiotic use conditional on the covariates listed above as well as the highest respiratory support at 24 hours. Greedy nearest-neighbor matching without replacement using a caliper width of 0.2 of the standard deviation of the logit of the PS was used to match each infant managed with prolonged antibiotics with an infant managed without prolonged antibiotics but with similar PS (27). Adequacy of matching was assessed by comparing proportions and means of variables in the two groups before and after matching and by standardized mean differences (13,28). Absolute differences <0.10 were considered acceptable (28, 29). Composite of death >5 days of age and before follow-up or survival with NDI and secondary outcomes were assessed in the matched cohort using log binomial models to estimate relative risks (RR) and 95% CI while accounting for the paired nature of the matched sample by using generalized estimating equations methods (13). For secondary analyses, we constructed models that included post-matching adjustment for key confounders (GA, BW, male sex, severe IVH diagnosed ≤7 days and maternal education); study center; and for high frequency ventilation, a variable with residual imbalance after PS matching (30). Analyses were completed using SAS statistical software version 9.4 (SAS Institute, Cary, NC).
RESULTS
During the study period, 7631 infants with GA 22-26 weeks and BW 401-1000 grams were born at the 24 NRN centers and survived >12 hours. Of these, 238 infants with birth defects (3%), and 39 infants missing exposure variables were excluded, leaving 7354 (96%) infants in the base cohort before additional analysis-specific exclusions.
EOS:
After exclusions, 6565 infants were analyzed (Figure 1; available at www.jpeds.com). The proportion of eligible infants who survived to follow-up but were excluded due to missing neurodevelopmental assessment was similar among infants with EOS (8/98, 8%), with prolonged antibiotics (345/2615, 13%) and without prolonged antibiotics (367/2700, 14%), p=0.29. Culture-confirmed EOS occurred in 153 infants (2.3%). Among infants without EOS, 3191 (48.6%) received prolonged early antibiotics and 3221 (49.1%) did not. Most maternal and neonatal characteristics differed among the three groups (Table 1). After adjusting for these characteristics, the composite outcome of death >12 hours or survival with NDI was increased for infants who had EOS (Table 2). Forty-one percent of infants with EOS died compared with 29% of culture-negative infants given prolonged early antibiotics and 28% without prolonged early antibiotics. Among survivors, risk of NDI was higher for infants with EOS compared with culture-negative infants who received prolonged early antibiotics and compared with infants who did not receive prolonged early antibiotics. Details of EOS infecting organisms are provided in Table 3; online. No difference was found in death/NDI among infants without EOS who were managed with and without prolonged antibiotics (Table 2).
Figure 1, online: Derivation of study cohorts.
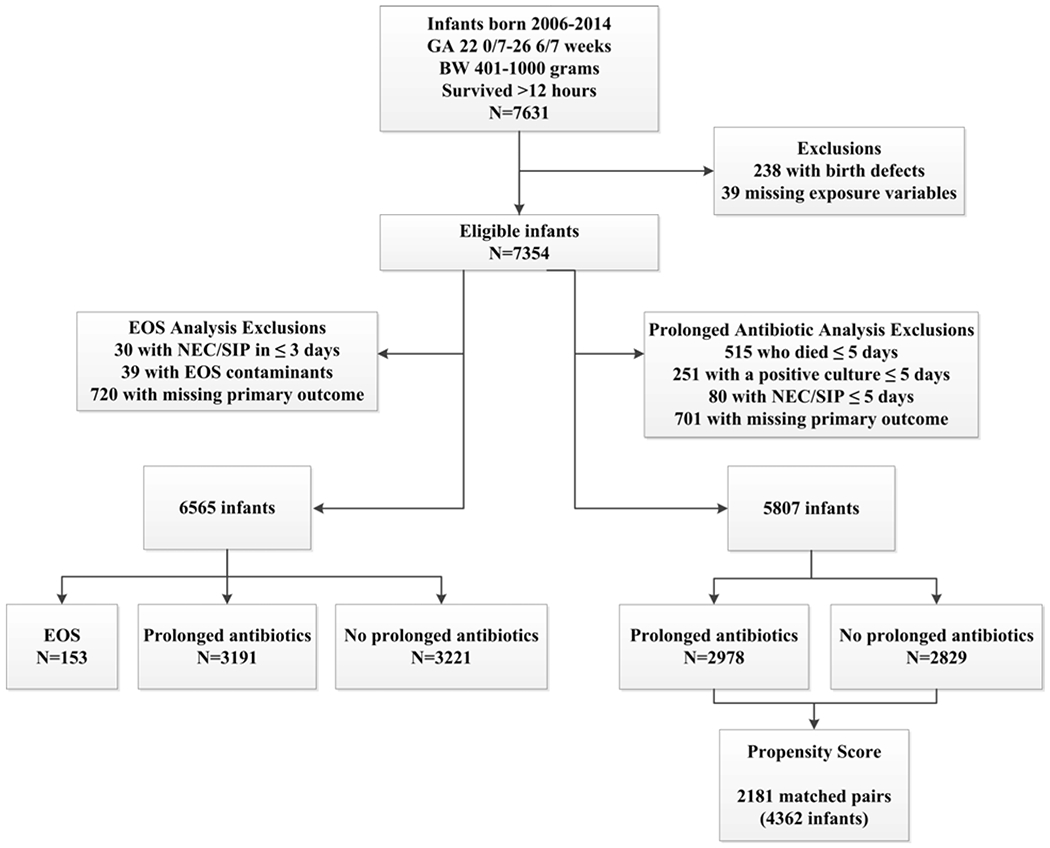
Figure 1, online legend: The 720 infants excluded from the EOS analysis due to missing outcome included 481 infants lost to follow-up, 140 with incomplete assessment, and 99 infants assessed outside of the allowable age. The 701 infants excluded from the prolonged antibiotic analysis due to missing outcome included 468 infants lost to follow-up, 135 with incomplete assessment, and 98 infants assessed outside of the allowable age. Abbreviations: GA, gestational age; BW, birth weight; NEC, necrotizing enterocolitis; SIP, spontaneous intestinal perforation; EOS, early onset sepsis.
Table 1:
Maternal and Neonatal Characteristics for EOS analysis
| n (column %) or mean (standard deviation)a | EOS N=153 | Prolonged antibiotics N=3191 | No prolonged antibiotics N=3221 | p-valueb |
|---|---|---|---|---|
| Maternal education | 0.008 | |||
| < High School degree | 16 (13.2) | 649 (22.8) | 598 (21.3) | |
| High School degree | 35 (28.9) | 835 (29.3) | 910 (32.4) | |
| > High School degree | 70 (57.9) | 1,361 (47.8) | 1,298 (46.3) | |
| Unknown/missing | 32 | 346 | 415 | |
| Maternal medical insurance | 0.007 | |||
| Private | 66 (44.9) | 1,276 (40.6) | 1,190 (37.2) | |
| Public/self-pay/other | 81 (55.1) | 1,864 (59.4) | 2,005 (62.8) | |
| Unknown/missing | 6 | 51 | 26 | |
| Maternal race/ethnicity | 0.03 | |||
| Black, non-Hispanic | 56 (37.3) | 1,381 (43.3) | 1,354 (42.2) | |
| White, non-Hispanic | 57 (38.0) | 1,160 (36.4) | 1,236 (38.6) | |
| Hispanic | 28 (18.7) | 473 (14.8) | 491 (15.3) | |
| Other | 9 (6.0) | 174 (5.5) | 125 (3.9) | |
| Maternal hypertension | 20 (13.1) | 647 (20.3) | 812 (25.2) | <0.001 |
| Antepartum hemorrhage | 32 (20.9) | 628 (19.7) | 709 (22.0) | 0.07 |
| Maternal clinical chorioamnionitis | 65 (43.0) | 769 (24.2) | 323 (10.1) | <0.001 |
| Maternal antibiotics during delivery admission | 130 (85.5) | 2,404 (75.9) | 2,274 (70.8) | <0.001 |
| Antenatal steroids | 132 (87.4) | 2,779 (87.4) | 2,839 (88.3) | 0.51 |
| Cesarean section | 87 (56.9) | 1,908 (59.8) | 2,159 (67.0) | <0.001 |
| Membrane rupture | <0.001 | |||
| >18 hours | 77 (52.0) | 983 (31.2) | 639 (20.1) | |
| ≤ 18 hours | 71 (48.0) | 2,164 (68.8) | 2,536 (79.9) | |
| Unknown/missing | 5 | 44 | 46 | |
| Male | 75 (49.0) | 1,643 (51.5) | 1,630 (50.7) | 0.70 |
| BW grams, mean (SD) | 713(131) | 700 (137) | 726 (140) | <0.001 |
| GA weeks, mean (SD) | 24.4 (1.1) | 24.6 (1.1) | 24.8 (1.0) | <0.001 |
| By GA week | <0.001 | |||
| 22 | 7 (4.6) | 63 (2.0) | 50 (1.6) | |
| 23 | 28 (18.3) | 475 (14.9) | 325 (10.1) | |
| 24 | 49 (32.0) | 915 (28.7) | 785 (24.4) | |
| 25 | 40 (26.1) | 959 (30.1) | 1,034 (32.1) | |
| 26 | 29 (19.0) | 779 (24.4) | 1,027 (31.9) | |
| Endotracheal intubation at birth | 141 (92.2) | 2,742 (86.0) | 2,571 (79.8) | <0.001 |
| Infant temperature within 60 minutes of birth | 0.04 | |||
| ≥ 96.5 F | 111 (77.6) | 2,127 (72.2) | 2,244 (74.9) | |
| < 96.5 F | 32 (22.4) | 819 (27.8) | 753 (25.1) | |
| Unknown/missing | 10 | 245 | 224 | |
| Severe IVH diagnosed within 7 days | <0.001 | |||
| Yes | 27 (18.8) | 328 (10.5) | 233 (7.6) | |
| No | 117 (81.3) | 2,789 (89.5) | 2,832 (92.4) | |
| No sonogram/missing | 9 | 74 | 156 | |
| Enteral feeds started within 3 days | 22 (14.4) | 805 (25.2) | 1,146 (35.6) | <0.001 |
| Survived > 24 hours, N | 146 | 3,170 | 3,144 | |
| Highest respiratory support at 24 hours | <0.001 | |||
| High-frequency ventilation | 56 (38.4) | 770 (24.3) | 325 (10.4) | |
| Conventional ventilation | 72 (49.3) | 1,810 (57.2) | 1,873 (59.7) | |
| NIMV | 3 (2.1) | 121 (3.8) | 172 (5.5) | |
| CPAP | 12 (8.2) | 389 (12.3) | 674 (21.5) | |
| Other/no support | 3 (2.1) | 75 (2.4) | 95 (3.0) |
BW, birth weight; CPAP, continuous positive airway pressure; GA, gestational age; IVH, intraventricular hemorrhage; NIMV, non-invasive intermittent mandatory ventilation;
Missing information is shown when missing for ≥1% of infants. Otherwise, information missing: maternal race/ethnicity, 21; maternal hypertension, 8; antepartum hemorrhage, 6; clinical chorioamnionitis, 20; antenatal antibiotics, 37; antenatal steroids, 18; cesarean section, 1; sex, 4; endotracheal intubation, 2; enteral feeds, 4; highest respiratory support at 24 h, 10 infants.
P-value by chi-square test (categorical variables) or T test (continuous variables).
Table 2.
Study Outcomes in EOS Analysis
| EOS n (%) | Prolonged antibiotics n (%) | No prolonged antibiotics n (%) | Adjusted RRa (95% CI) p-value | |||
|---|---|---|---|---|---|---|
| EOS vs. Prolonged antibiotics | EOS vs. No prolonged antibiotics | Prolonged vs. No prolonged antibiotics | ||||
| Infants, N | 153 | 3,191 | 3,221 | |||
| Death/ NDI | 104 (68.0) | 1,732 (54.3) | 1,640 (50.9) | 1.18 (1.06-1.32) 0.003 | 1.23 (1.10-1.37) <0.001 | 1.04 (0.99-1.08) 0.11 |
| Death | 63 (41.2) | 921 (28.9) | 888 (27.6) | 1.16 (0.97-1.40) 0.11 | 1.16 (0.96-1.40) 0.12 | 1.00 (0.93-1.07) 0.97 |
| NDI Evaluation, N | 90 | 2,270 | 2,333 | |||
| NDI | 41 (45.6) | 811 (35.7) | 752 (32.2) | 1.26 (0.99-1.60) 0.06 | 1.34 (1.05-1.71) 0.02 | 1.06 (0.98-1.16) 0.14 |
| Bayley 3 cognitive composite score <85 | 38 (42.2) | 745 (33.1) | 695 (30.0) | 1.26 (0.98-1.63) 0.07 | 1.34 (1.04-1.74) 0.02 | 1.06 (0.97-1.16) 0.17 |
| GMFCS level ≥2 | 15 (16.7) | 234 (10.3) | 193 (8.3) | 1.50 (0.91-2.46) 0.11 | 1.74 (1.05-2.88) 0.03 | 1.16 (0.95-1.41) 0.14 |
| Bilateral blindnessb | 0 (0.0) | 39 (1.7) | 29 (1.2) | − 0.40 | − 0.62 | 1.39 (0.86-2.23) 0.18 |
| Hearing impairmentb | 2 (2.2) | 75 (3.3) | 59 (2.5) | 0.67 (0.17-2.69) 0.77 | 0.88 (0.22-3.54) 1.0 | 1.31 (0.93-1.83) 0.14 |
| Blindness or hearing impairmentc | 2 (2.2) | 106 (4.7) | 86 (3.7) | 0.50 (0.12-2.01) 0.33 | 0.56 (0.14-2.29) 0.42 | 1.12 (0.84-1.50) 0.44 |
RR adjusted for study center, maternal education (<, =, > high school, missing), maternal insurance (private, public/other), maternal race/ethnicity (non-Hispanic black, non-Hispanic white, Hispanic, other), maternal hypertension, antepartum hemorrhage, chorioamnionitis, antenatal antibiotics and steroids, cesarean, membrane rupture >18 hours, GA (22–26), BW (continuous), male sex, intubation, temperature ≤60 minutes, enteral feeds ≤3 days, severe IVH ≤7 days. Statistical significance determined by the Wald chi-square test.
RR of bilateral blindness not estimated for EOS comparisons. Unadjusted p-values and RRs for bilateral blindness and hearing impairment are shown.
Study center could not be included in the model fit to the combined outcome blindness or hearing impairment as some centers had no children with either outcome.
Table 3,
online: EOS causing organisms
| Organism(s)--Blood | Organism(s)--CSFa | n (column %) |
|---|---|---|
| Gram positive | 42 (27.5) | |
| Viridans streptococci | 1 (0.7) | |
| Group B strep | 28 (18.3) | |
| Staph aureus | 3 (2.0) | |
| Viridans streptococci | 3 (2.0) | |
| Enterococcus | 2 (1.3) | |
| MRSA | 2 (1.3) | |
| Strep pneumoniae | 2 (1.3) | |
| Alpha hemolytic strep | 1 (0.7) | |
| Gram negative | 100 (65.4) | |
| E. coli | 1 (0.7) | |
| E. coli | 65 (42.5) | |
| E. coli | E. coli | 7 (4.6) |
| Haemophilus | 10 (6.5) | |
| Klebsiella | 4 (2.6) | |
| Acinetobacter | 2 (1.3) | |
| Capnocytophaga | 2 (1.3) | |
| Citrobacter | 2 (1.3) | |
| Morganella morganii | 2 (1.3) | |
| Bacteroides | 1 (0.7) | |
| Campylobacter | 1 (0.7) | |
| Eikenella corrodens | 1 (0.7) | |
| Pseudomonas aeruginosa | 1 (0.7) | |
| Sphingomonas paucimobilis | 1 (0.7) | |
| Fungi | 2 (1.3) | |
| Candida albicans | 1 (0.7) | |
| Saccharomyces | 1 (0.7) | |
| Polymicrobial | 6 (3.9) | |
| Acinetobacter baumannii, Acinetobacter lwoffii, Micrococcus | 1 (0.7) | |
| E. coli, CONS | 1 (0.7) | |
| E. coli, Group B strep | 1 (0.7) | |
| E. coli, Strep viridans | 1 (0.7) | |
| Neisseria, Haemophilus | 1 (0.7) | |
| Strep bovis, Corynebacterium | 1 (0.7) | |
| Not specified | 3 (2.0) | |
| Missing | 2 (1.3) | |
| Other bacteria (699) | 1 (0.7) | |
| Total number of cases | 153 |
Three of the 10 infants with a positive CSF culture had meningitis alone (1 Viridans streptococci, 1 E. coli, 1 Acinetobacter plus Micrococcus); 7 had E. coli on both blood and CSF cultures.
Prolonged early antibiotic use:
After exclusions, 5807 infants were analyzed (Figure 1). Of these, 2978 infants (51%) received prolonged early antibiotics and 2829 (49%) did not. Propensity scores generated for the two groups showed good overlap (Figure 2; available at www.jpeds.com) and PS matching resulted in 2181 pairs (75% of the eligible cohort). After matching, differences in means and proportions of baseline characteristics were reduced between the groups and standardized mean differences of <0.10 were achieved in all variables except high-frequency ventilation at 24 hours (Table 4). Fifty percent of infants with prolonged early antibiotic exposure died >5 days or survived with NDI compared with 48% of matched infants without exposure to prolonged early antibiotics [RR 1.04 (95% CI: 0.98-1.11), P = .18] (Table 5). Estimated relative risk of death alone, NDI in survivors and components of NDI were also similar. Post-matching adjustment did not substantially alter these comparisons.
Figure 2,
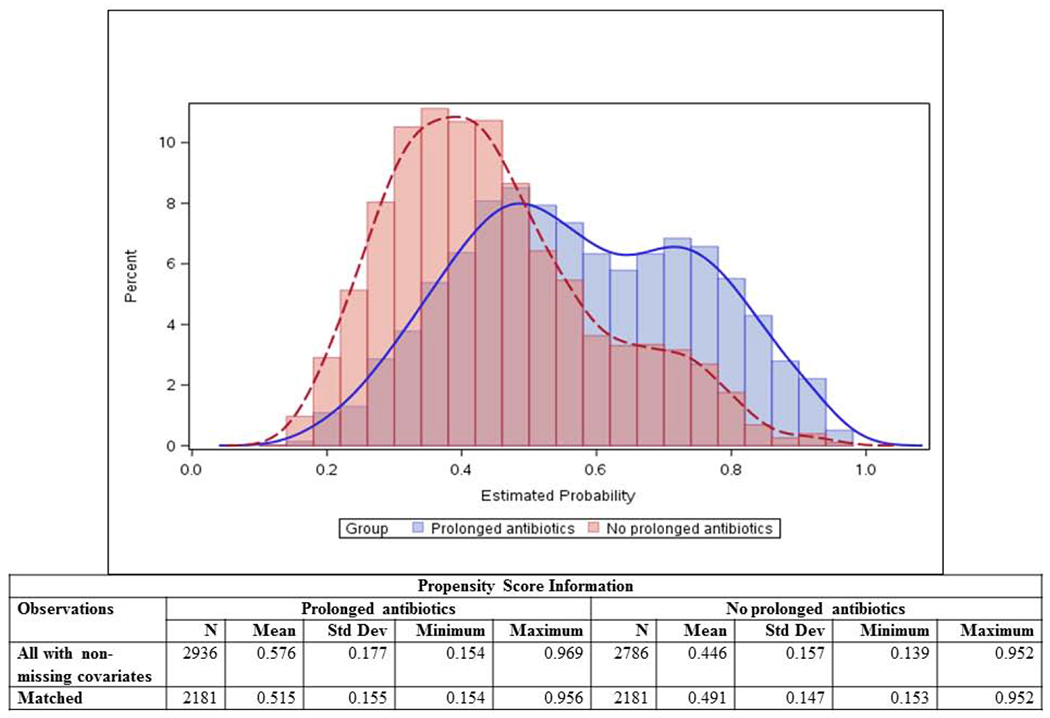
online: Distribution of propensity score generated from demographics and early clinical presentation.
Table 4.
Smaller Standardized Difference for Maternal and Neonatal Characteristics After Propensity Score Matchinga.
| Original Sample | Matched Sample | |||||
|---|---|---|---|---|---|---|
| Prolonged antibiotics n=2936 | No prolonged antibiotics n=2786 | Standardized difference | Prolonged antibiotics n=2181 | No prolonged antibiotics n=2181 | Standardized difference | |
| Maternal education | ||||||
| < High School degree | 597 (20.3) | 533 (19.1) | 0.030 | 442 (20.3) | 439 (20.1) | 0.003 |
| High School degree | 788 (26.8) | 813 (29.2) | 0.052 | 605 (27.7) | 618 (28.3) | 0.013 |
| > High School degree | 1,280 (43.6) | 1,176 (42.2) | 0.028 | 929 (42.6) | 924 (42.4) | 0.005 |
| Maternal medical insurance | ||||||
| Private | 1,174 (40.0) | 1,029 (36.9) | 0.063 | 826 (37.9) | 828 (38.0) | 0.002 |
| Maternal race/ethnicity | ||||||
| Black, non-Hispanic | 1,278 (43.5) | 1,194 (42.9) | 0.014 | 965 (44.2) | 972 (44.6) | 0.006 |
| White, non-Hispanic | 1,063 (36.2) | 1,072 (38.5) | 0.047 | 786 (36.0) | 779 (35.7) | 0.007 |
| Hispanic | 433 (14.7) | 418 (15.0) | 0.007 | 330 (15.1) | 336 (15.4) | 0.008 |
| Maternal hypertension | 591 (20.1) | 733 (26.3) | 0.147 | 501 (23.0) | 518 (23.8) | 0.019 |
| Antepartum hemorrhage | 571 (19.4) | 597 (21.4) | 0.049 | 432 (19.8) | 442 (20.3) | 0.011 |
| Maternal clinical chorioamnionitis | 719 (24.5) | 269 (9.7) | 0.402 | 323 (14.8) | 269 (12.3) | 0.067 |
| Maternal antibiotics during delivery admission | 2,243 (76.4) | 1,992 (71.5) | 0.112 | 1,606 (73.6) | 1,583 (72.6) | 0.024 |
| Antenatal steroids | 2,586 (88.1) | 2,504 (89.9) | 0.057 | 1,930 (88.5) | 1,936 (88.8) | 0.009 |
| Cesarean section | 1,764 (60.1) | 1,887 (67.7) | 0.160 | 1,370 (62.8) | 1,407 (64.5) | 0.035 |
| Membrane rupture >18 hours | 927 (31.6) | 569 (20.4) | 0.256 | 563 (25.8) | 527 (24.2) | 0.038 |
| GA week | ||||||
| 22 | 47 (1.6) | 30 (1.1) | 0.046 | 24 (1.1) | 26 (1.2) | 0.008 |
| 23 | 414 (14.1) | 226 (8.1) | 0.191 | 246 (11.3) | 216 (9.9) | 0.044 |
| 24 | 836 (28.5) | 652 (23.4) | 0.116 | 589 (27.0) | 568 (26.0) | 0.022 |
| 25 | 900 (30.7) | 923 (33.1) | 0.053 | 708 (32.5) | 706 (32.4) | 0.002 |
| BW grams, mean (SD) | 705 (137) | 735 (138) | 0.223 | 716 (137) | 721 (137) | 0.043 |
| Male | 1,509 (51.4) | 1,371 (49.2) | 0.044 | 1,118 (51.3) | 1,105 (50.7) | 0.012 |
| Endotracheal intubation at birth | 2,520 (85.8) | 2,192 (78.7) | 0.188 | 1,826 (83.7) | 1,815 (83.2) | 0.013 |
| Infant temperature within 60 minutes of birth | ||||||
| ≥ 96.5 F | 1,977 (67.3) | 1,998 (71.7) | 0.095 | 1,507 (69.1) | 1,505 (69.0) | 0.002 |
| < 96.5 F | 741 (25.2) | 612 (22.0) | 0.077 | 519 (23.8) | 528 (24.2) | 0.010 |
| Highest respiratory support at 24 hours | ||||||
| High-frequency ventilation | 689 (23.5) | 230 (8.3) | 0.426 | 317 (14.5) | 230 (10.5) | 0.112 |
| Conventional ventilation | 1,684 (57.4) | 1,652 (59.3) | 0.039 | 1,366 (62.6) | 1,402 (64.3) | 0.033 |
| NIMV | 117 (4.0) | 166 (6.0) | 0.091 | 101 (4.6) | 111 (5.1) | 0.021 |
| CPAP | 375 (12.8) | 650 (23.3) | 0.277 | 340 (15.6) | 378 (17.3) | 0.046 |
| Severe IVH diagnosed within 7 days | 252 (8.6) | 120 (4.3) | 0.175 | 142 (6.5) | 117 (5.4) | 0.047 |
| Enteral feeds started within 3 days | 773 (26.3) | 1,091 (39.2) | 0.276 | 635 (29.1) | 649 (29.8) | 0.014 |
BW, birth weight; CPAP, continuous positive airway pressure; GA, gestational age; IVH, intraventricular hemorrhage; NIMV, non-invasive intermittent mandatory ventilation; SD, standard deviation.
N (%) are shown for all variables except BW reported as mean and standard deviation. Standardized differences are shown as absolute value. The original sample includes 5722 infants with all non-missing values of the covariates included in the propensity score model from the total 5807 infants in the complete cohort. Categorical variables with missing values for ≥1% of infants were entered in the model with a level indicating missing in order to minimize the number of observations excluded due to missing values (maternal education, 10% missing; maternal medical insurance, 1%; membrane rupture >18 hours, 1%; infant temperature within 60 minutes of birth, 7%; severe IVH diagnosed with 7 days, 1%).
Table 5.
Study Outcomes in Propensity-Score Matched Sample
| Prolonged antibiotics | No prolonged antibiotics | RR (95% CI)a | p-valuea | |
|---|---|---|---|---|
| Infants, n | 2,181 | 2,181 | ||
| Death/NDI, n (%) - with adjustment for key covariatesb | 1,091 (50.0) | 1,047 (48.0) | 1.04 (0.98-1.11) 1.05 (0.99-1.11) | 0.18 0.09 |
| Death before follow-up, n (%) - with adjustment for key covariatesb | 512 (23.5) | 469 (21.5) | 1.09 (0.98-1.22) 1.07 (0.97-1.19) | 0.12 0.17 |
| Survived to follow-up and evaluated, n | 1,669 | 1,712 | ||
| NDI, n (%) - with adjustment for key covariatesb | 579 (34.7) | 578 (33.8) | 1.03 (0.94-1.13) 1.05 (0.96-1.16) | 0.57 0.25 |
| Bayley 3 cognitive composite score <85 - with adjustment for key covariatesb | 530 (32.0) | 533 (31.4) | 1.02 (0.92-1.13) 1.05 (0.96-1.16) | 0.70 0.29 |
| GMFCS level ≥2 - with adjustment for key covariatesb | 162 (9.7) | 155 (9.1) | 1.07 (0.87-1.33) 1.17 (0.95-1.45) | 0.50 0.14 |
| Bilateral blindness | 27 (1.6) | 24 (1.4) | 1.15 (0.67-1.97) | 0.61 |
| Hearing impairment | 58 (3.5) | 49 (2.9) | 1.22 (0.85-1.76) | 0.29 |
| Blindness or hearing impairment - with adjustment for key covariatesb,c | 79 (4.8) | 71 (4.2) | 1.15 (0.84-1.56) 1.16 (0.85-1.58) | 0.38 0.36 |
Relative risks (RR) and confidence intervals (CI) from log binomial (for primary comparisons) or Poisson regression models (for models with post-match adjustment) using methods that account for the matched pair design with statistical significance determined by the Wald chi-square test. Poisson models were used due to convergence problems with log binomial models when covariates were added.
Covariates used in post-matching adjustment included important confounders (study center, maternal education, infant GA, BW, male sex, severe IVH diagnosed within 7 days of birth), as well as highest respiratory support at 24 hours of life due to some evidence of residual imbalance after matching based on a standardized mean difference between groups >0.10 for one level (High-Frequency ventilation, 0.112).
Study center could not be included in the model fit to the combined outcome blindness or hearing impairment as some centers had no children with either outcome.
DISCUSSION
In this study, infants who had culture-confirmed EOS were more likely to die or survive with NDI as assessed at 18-26 months CA compared with infants without EOS who did or did not receive prolonged early antibiotics, when accounting for multiple confounders and other predictors of this outcome. When we compared infants without EOS, NEC, or SIP, we found the composite outcome of death or NDI at 18-26 months CA was 4% more likely to occur in infants managed with prolonged antibiotics with the confidence limits crossing zero and ranging from a 2% lower risk to an 11% higher risk. For this comparison, we used a propensity score matched cohort, and also employed post-matching adjustment to rigorously address the issue of confounding. We also made this comparison using the full cohort from which our PS analysis was derived, and found similar results. Our results demonstrate that risk of death/NDI for infants with culture-confirmed EOS is higher compared with infants without this diagnosis. This finding is likely no surprise to neonatal clinicians. Perhaps less expected is our observation that among those without culture-confirmed EOS, the administration of prolonged antibiotics was not associated with any significant difference in outcomes of death and/or NDI. One straightforward explanation is that the infants receiving prolonged antibiotics did not have bacterial infection and antibiotics made no difference to their outcomes. Another possible explanation is that any advantage or disadvantage offered by prolonged antibiotics administration does not impact mortality or NDI as measured in this study.
Although epidemiologic studies address EOS-attributable mortality (31–34), information on the impact of culture-confirmed EOS on neurodevelopmental outcomes among preterm infants is scarce. A study from Israel demonstrated that very-low birth weight (VLBW, BW <1500 grams) infants with EOS are more likely to have brain injury compared with uninfected infants, but this report had no information on post-discharge outcomes (35). A prior study conducted among extremely preterm infants cared for in NRN centers from 1993-2001 found an increased risk of death or NDI among infants with culture-confirmed infection (34). The contribution of EOS to these findings is difficult to determine because the analysis combined cases of EOS and late-onset sepsis (LOS), and <3% of the infected study cohort had EOS alone. In a French study of infants born at 22-32 weeks gestation, those who had both EOS and LOS had a higher risk of CP at 5 years of age than uninfected infants (36). No difference was observed among those who had EOS alone, although this finding was based on evaluation of only 11 children. Our study demonstrates the negative overall impact of EOS in a large cohort of extremely preterm infants: 68% of those with EOS died or survived with NDI compared with 53% of infants without culture-confirmed EOS.
Because culture-confirmed EOS is universally treated with antibiotics, the potential impacts of the infection itself versus the antibiotics used cannot be separated. In contrast, provider and institutional variation in early antibiotic administration duration in the absence of culture-confirmed EOS provides the opportunity to assess the impact of prolonged early antibiotics after adjustment for patient-level risk factors. Multiple prior studies have reported adverse hospital outcomes among preterm infants administered prolonged early antibiotics (37–39). A study of extremely preterm infants born 1998-2001 and cared for at NRN centers reported that prolonged early antibiotic administration was associated with increased odds for in-hospital death (37), although a similar study of those born 2008-2014 reported less frequent use of prolonged early antibiotics and a smaller association between treatment and death (adjusted odds ratio 1.17 [95% CI: 0.99–1.40] p=0.07) (5). Initial antibiotic duration among VLBW infants admitted to centers in the Canadian Neonatal Network (CNN) was associated with increased odds of a composite outcome of mortality or significant morbidity (severe neurologic injury, retinopathy of prematurity, NEC, LOS or bronchopulmonary dysplasia), although the association with death at >7 days was not significant (40).
Few studies have explored the impact of prolonged antibiotics on outcomes after hospital discharge among preterm infants. CNN investigators assessed the relationship of antibiotic utilization rate (AUR), defined as total days of antibiotics divided by the length of stay, with death and severe NDI at 18-21 months among infants born at <29 weeks’ gestation (41). They measured antibiotics administered in the absence of standard indications as quartiles of AUR (41). Comparing infants with the highest quartile of AUR to infants with the lowest quartile of AUR, this study found elevated adjusted odds for the composite outcome of death or NDI and for death alone, but not for NDI among survivors. A limitation of this study is that mortality effects length of stay which may in turn influence the association between high AUR and death. We restricted our analysis of prolonged early antibiotic exposure to infants who survived >5 days to ensure the exposure could occur in all eligible infants. We found no evidence that prolonged early antibiotics either contribute to or protect against the composite or individual outcomes of death or NDI. The differing results for the outcome of death may be driven by the different approaches in the two studies.
Confounding by indication is a common concern in retrospective studies addressing the impact of antibiotic administration. It is likely that in many cases, infants who receive prolonged early antibiotics for culture-negative infection are sicker than those infants who do not. Prior studies approached this by adjusting for covariates in a regression model. Using this approach, we found no difference in outcomes between infants without EOS conditional on prolonged antibiotic use. We then applied a different approach to allow visualization of the balance of early clinical status among infants receiving prolonged antibiotics or not. We used propensity scores to match infants on multiple demographic and clinical characteristics that may influence management decisions and ultimately contribute to a child’s risk of the composite outcome. This approach allowed us to focus on the 75% of infants among whom there is the most clinical variation in care, as it eliminates infants for whom most clinicians administered prolonged antibiotics, as well as those for whom most clinicians did not. Characteristics such as younger gestational age, maternal chorioamnionitis, and prolonged rupture of membranes that were more frequent among infants who received prolonged early antibiotics were better balanced in the matched cohort. We additionally conducted post-match adjustment of key variables and variables with residual imbalance after matching. Despite these adjustments, we cannot entirely rule out an impact of residual confounding.
Our study has additional limitations. In the database we used for this study, information about early antibiotics did not include type, indication and total duration of use. We did not collect additional laboratory data that can influence persistent antibiotic use, nor did we have information regarding probiotic use. Using the PS to match infants with and without prolonged antibiotic exposure provides balance on the characteristics considered, but unmeasured characteristics may still be unequally distributed between the groups resulting in biased estimates. As noted, approximately 25% of the cohort could not be matched (Table 6; online), largely due to a lack of practice variation among these infants.
Table 6,
online: Characteristics of unmatched infants
| n (column %) or mean (standard deviation)a | Prolonged antibiotics n=797 | No prolonged antibiotics n=648 | p-valueb |
|---|---|---|---|
| Maternal education | 0.001 | ||
| < High School degree | 164 (22.8) | 101 (17.6) | |
| High School degree | 193 (26.8) | 205 (35.7) | |
| > High School degree | 363 (50.4) | 269 (46.8) | |
| Unknown/missing | 77 | 73 | |
| Maternal medical insurance | <0.001 | ||
| Private | 360 (46.9) | 220 (34.1) | |
| Public/self-pay/other | 408 (53.1) | 425 (65.9) | |
| Unknown/missing | 29 | 3 | |
| Maternal race/ethnicity | <0.001 | ||
| Black, non-Hispanic | 326 (41.0) | 233 (36.8) | |
| White, non-Hispanic | 296 (37.2) | 306 (48.3) | |
| Hispanic | 109 (13.7) | 87 (13.7) | |
| Other | 64 (8.1) | 8 (1.3) | |
| Unknown/missing | 2 | 14 | |
| Maternal hypertension | 98 (12.4) | 221 (34.3) | <0.001 |
| Antepartum hemorrhage | 149 (18.7) | 166 (25.7) | 0.001 |
| Maternal clinical chorioamnionitis | 402 (50.9) | 7 (1.1) | <0.001 |
| Maternal antibiotics during delivery admission | 651 (84.0) | 430 (67.0) | <0.001 |
| Unknown/missing | 22 | 6 | |
| Antenatal steroids | 684 (86.9) | 602 (93.8) | <0.001 |
| Unknown/missing | 10 | 6 | |
| Cesarean section | 420 (52.8) | 513 (79.2) | <0.001 |
| Membrane rupture | <0.001 | ||
| >18 hours | 374 (47.6) | 54 (8.5) | |
| ≤ 18 hours | 412 (52.4) | 583 (91.5) | |
| Unknown/missing | 11 | 11 | |
| GA weeks, mean (SD) | 24.3 (1.1) | 25.3 (0.8) | <0.001 |
| By GA week | <0.001 | ||
| 22 | 25 (3.1) | 4 (0.6) | |
| 23 | 174 (21.8) | 11 (1.7) | |
| 24 | 262 (32.9) | 96 (14.8) | |
| 25 | 201 (25.2) | 230 (35.5) | |
| 26 | 135 (16.9) | 307 (47.4) | |
| BW grams, mean (SD) | 673 (130) | 785 (130) | <0.001 |
| Male | 414 (52.0) | 285 (44.2) | 0.003 |
| Endotracheal intubation at birth | 731 (91.8) | 414 (64.0) | <0.001 |
| Infant temperature within 60 minutes of birth | <0.001 | ||
| ≥ 96.5 F | 495 (68.1) | 525 (84.8) | |
| < 96.5 F | 232 (31.9) | 94 (15.2) | |
| Unknown/missing | 70 | 29 | |
| Highest respiratory support at 24 hours | <0.001 | ||
| High-frequency ventilation | 385 (48.6) | 1 (0.2) | |
| Conventional ventilation | 338 (42.7) | 276 (42.9) | |
| NIMV | 17 (2.1) | 55 (8.5) | |
| CPAP | 38 (4.8) | 282 (43.8) | |
| Other/no support | 14 (1.8) | 30 (4.7) | |
| Severe IVH diagnosed within 7 days | <0.001 | ||
| Yes | 114 (14.4) | 4 (0.6) | |
| No | 679 (85.6) | 637 (99.4) | |
| No sonogram/missing | 4 | 7 | |
| Enteral feeds started within 3 days | 147 (18.5) | 454 (70.4) | <0.001 |
BW, birth weight; CPAP, continuous positive airway pressure; EOS, early-onset sepsis; GA, gestational age; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis; NIMV, non-invasive intermittent mandatory ventilation; SIP, spontaneous intestinal perforation.
The number of infants with unknown/missing information is shown for characteristics with information missing for ≥1% of infants. Otherwise, information was missing for: maternal hypertension, 7; antepartum hemorrhage, 4; maternal clinical chorioamnionitis, 12; cesarean section, 1; male sex, 4; endotracheal intubation, 2; highest respiratory support at 24 h, 9; enteral feeds within 3 days, 4 infants.
p-value by chi-square test (categorical variables) or T test (continuous variables).
We do not interpret the lack of association in our study as ‘safety’ of prolonged antibiotics but as an absence of benefit. Death and NDI are not appropriate outcomes to gauge safety; they are the key metrics of anticipated benefit. We did not have the data to compare interim outcomes such as drug side effects, alterations in microbiota or longer-term outcomes such as atopy and allergies to inform true safety. To our knowledge, no study addressing the impact of antibiotics administered to preterm infants has reported a benefit of prolonged antibiotics when used in the absence of culture-confirmed infection. Yet neonatal providers continue to express concerns about poor detection rates of microbiological cultures and rely on inflammatory biomarkers to guide antibiotic duration. Given the existing evidence of potential harm from antibiotic-associated dysbiosis and the lack of demonstrable benefit, we must question the practice of prolonged antibiotic use among extremely preterm infants when optimally-collected microbiological cultures are sterile.
Supplementary Material
Acknowledgments:
We thank our medical and nursing colleagues and the infants and their parents who agreed to take part in this study.
Conducted and supported by the National Institutes of Health, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the National Center for Research Resources, and the National Center for Advancing Translational Sciences who provided grant support for the Neonatal Research Network’s generic database and follow-up studies through cooperative agreements. While NICHD staff had input into the study design, conduct, analysis, and manuscript drafting, the comments and views of the authors do not necessarily represent the views of NICHD, the National Institutes of Health, the Department of Health and Human Services, or the U.S. Government. Participating NRN sites collected data and transmitted it to RTI International, the data coordinating center (DCC) for the network, which stored, managed and analyzed the data for this study. On behalf of the NRN, RTI International had full access to all of the data in the study, and with the NRN Center Principal Investigators, takes responsibility for the integrity of the data and accuracy of the data analysis.SM is supported by the NICHD (K23HD088753-01A1). R.G. has received support from industry for research services (https://dcri.org/about-us/conflict-of-interest/). The other authors declare no conflicts of interest.
Abbreviations:
- aRR
Adjusted relative risk
- BW
Birth weight
- CA
Corrected age
- CI
Confidence interval
- CP
Cerebral palsy
- CPAP
Continuous positive airway pressure
- CSF
Cerebrospinal fluid
- EOS
Early-onset sepsis
- GA
Gestational age
- GMFCS
Gross motor function classification system
- IVH
Intraventricular hemorrhage
- LOS
Late-onset sepsis
- NDI
Neurodevelopmental impairment
- NEC
Necrotizing enterocolitis
- NICHD
Eunice Kennedy Shriver National Institute of Child Health and Human Development
- NRN
Neonatal Research Network
- PS
Propensity score
- ROM
Rupture of membranes
- SIP
Spontaneous intestinal perforation
Appendix (online)
Additional members of the NICHD Neonatal Research Network NRN Steering Committee Chairs: Alan H. Jobe, MD PhD, University of Cincinnati (2003-2006); Michael S. Caplan, MD, University of Chicago, Pritzker School of Medicine (2006-2011);
Richard A. Polin, MD, Division of Neonatology, College of Physicians and Surgeons, Columbia University, (2011-present).
Alpert Medical School of Brown University and Women & Infants Hospital of Rhode Island (UG1 HD27904) – Abbott R. Laptook, MD; Martin Keszler, MD; Betty R. Vohr, MD; Angelita M. Hensman, MS RNC-NIC; Barbara Alksninis, PNP; Kristin M. Basso, MaT BSN; Emily Little, BSN RN; Robert Burke, MD; Melinda Caskey, MD; Laurie Hoffman, MD; Katharine Johnson, MD; Mary Lenore Keszler, MD; Andrea M. Knoll; Theresa M. Leach, MEd CAES; Emilee Little, RN BSN; Elisabeth C. McGowan, MD; Elisa Vieira, RN BSN; Victoria E. Watson, MS CAS; Suzy Ventura.
Case Western Reserve University, Rainbow Babies & Children’s Hospital (UG1 HD21364, M01 RR80) – Michele C. Walsh, MD MS; Anna Maria Hibbs, MD MSCE; Deanne E. Wilson-Costello, MD; Nancy S. Newman, BA RN; Allison H. Payne, MD MS; Bonnie S. Siner, RN; Monika Bhola, MD; Gulgun Yalcinkaya, MD.
Children’s Mercy Hospital, University of Missouri Kansas City School of Medicine (UG1 HD68284) – William E. Truog, MD; Eugenia K. Pallotto, MD MSCE; Howard W. Kilbride MD; Cheri Gauldin, RN BS CCRC; Anne Holmes RN MSN MBA-HCM CCRC; Kathy Johnson RN, CCRC; Allison Scott, RNC-NIC BSN CCRC.
Cincinnati Children’s Hospital Medical Center, University Hospital, and Good Samaritan Hospital (UG1 HD27853, M01 RR8084) – Brenda B. Poindexter, MD MS; Kurt Schibler, MD; Edward F. Donovan, MD; Cathy Grisby, BSN CCRC; Kate Bridges, MD; Barbara Alexander, RN; Estelle E. Fischer, MHSA MBA; Stephanie Merhar, MD MS; Holly L. Mincey, RN BSN; Jody Hessling, RN; Teresa L. Gratton, PA; Lenora Jackson, CRC; Kristin Kirker, CRC; Greg Muthig, BS; Jean J. Steichen, MD; Stacey Tepe, BS; Kimberly Yolton, PhD.
Duke University School of Medicine, University Hospital, University of North Carolina, and Duke Regional Hospital (UG1 HD40492, UL1 TR1117, M01 RR30, UL1 TR1111) – Ronald N. Goldberg, MD; Ricki F. Goldstein, MD; Patricia L. Ashley, MD PhD; William F. Malcolm, MD; Kathy J. Auten, MSHS; Kimberley A. Fisher, PhD FNP-BC IBCLC; Sandra Grimes, RN BSN; Kathryn E. Gustafson, PhD; Melody B. Lohmeyer, RN MSN; Joanne Finkle, RN JD; Matthew M. Laughon, MD MPH; Carl L. Bose, MD; Janice Bernhardt, MS RN; Gennie Bose, RN; Cindy Clark, RN; Linda Manor, RPh; Diane Warner, MD MPH; Janice Wereszczak, NNP.
Emory University, Children’s Healthcare of Atlanta, Grady Memorial Hospital, and Emory University Hospital Midtown (UG1 HD27851, M01 RR39) –David P. Carlton, MD; Ira Adams-Chapman, MD; Ellen C. Hale, RN BS CCRC; Yvonne Loggins, RN BSN; Ann Blackwelder, RN MN; Lynn C. Wineski, RN MS; Maureen Mulligan LaRossa, RN; Sheena L. Carter, PhD. Eunice Kennedy Shriver National Institute of Child Health and Human Development – Rosemary D. Higgins, MD; Stephanie Wilson Archer, MA.
Indiana University, University Hospital, Methodist Hospital, Riley Hospital for Children, and Wishard Health Services (UG1 HD27856, M01 RR750) – Gregory M. Sokol, MD; Brenda B. Poindexter, MD MS; Anna M. Dusick, MD (deceased); Lu-Ann Papile, MD; Susan Gunn, NNP CCRC; Faithe Hamer, BS; Heidi M. Harmon, MD MS; Dianne E. Herron, RN CCRC; Abbey C. Hines, PsyD; Carolyn Lytle, MD MPH; Heike M. Minnich, PsyD HSPP; Lucy Smiley CCRC; Leslie Dawn Wilson, BSN CCRC.
McGovern Medical School at The University of Texas Health Science Center at Houston, Children’s Memorial Hermann Hospital, Memorial Hermann Southwest Hospital, and Lyndon Baines Johnson General Hospital/Harris County Hospital District (UG1 HD87229, U10 HD21373) – Kathleen A. Kennedy, MD MPH; Jon E. Tyson, MD MPH; Georgia E. McDavid, RN; Nora I. Alaniz, BS; Elizabeth Allain, MS; Julie Arldt-McAlister, RN BSN; Katrina Burson, RN BSN; Susan E. Dieterich, PhD; Allison G. Dempsey, PhD; Andrea F. Duncan, MD; Elizabeth Eason, MD; Patricia W. Evans, MD; Carmen Garcia, RN CCRP; Charles Green, PhD; Beverly Foley Harris, RN BSN; Margarita Jiminez, MD MPH; Janice John, CPNP; Patrick M. Jones, MD; M. Layne Lillie, RN BSN; Anna E. Lis, RN BSN; Carrie M. Mason, MA LPA; Karen Martin, RN; Sara C. Martin, RN BSN; Shannon McKee EdS; Brenda H. Morris, MD; Shawna Rodgers, RN BSN; Saba Siddiki, MD; Maegan C. Simmons, RN; Daniel Sperry, RN; Patti L. Pierce Tate, RCP; Sharon L. Wright, MT(ASCP).
Nationwide Children’s Hospital and the Ohio State University Medical Center (UG1 HD68278) –Leif D. Nelin, MD; Sudarshan R. Jadcherla, MD; Patricia Luzader, RN; Christine A. Fortney, PhD RN; Gail E. Besner, MD; Nehal A. Parikh, MD
RTI International (U10 HD36790) – Abhik Das, PhD; Dennis Wallace, PhD; Marie G. Gantz, PhD; W. Kenneth Poole, PhD (deceased); Jamie E. Newman, PhD MPH; Jeanette O’Donnell Auman, BS; Margaret M. Crawford, BS; Jenna Gabrio, MPH; Carolyn M. Petrie Huitema, MS; Kristin M. Zaterka-Baxter, RN BSN.
Stanford University, Dominican Hospital, El Camino Hospital, and Lucile Packard Children’s Hospital (UG1 HD27880, M01 RR70) – Krisa P. Van Meurs, MD; David K. Stevenson, MD; Susan R. Hintz, MD MS Epi; Marian M. Adams, MD; M. Bethany Ball, BS CCRC; Barbara Bentley, PhD; Elizabeth Bruno, PhD; Maria Elena DeAnda, PhD; Anne M. DeBattista, RN PNP; Lynne C. Huffman, MD; Magdy Ismael, MD MPH; Jean G. Kohn, MD MPH; Casey Krueger, PhD; Andrew Palmquist, RN; Melinda S. Proud, RCP; Nicholas H. St. John, PhD; Hali Weiss, MD.
Tufts Medical Center, Floating Hospital for Children (U10 HD53119, M01 RR54) – Ivan D. Frantz III, MD; John M. Fiascone, MD; Brenda L. MacKinnon, RNC; Anne Furey, MPH; Ellen Nylen, RN BSN; Elisabeth C. McGowan, MD.
University of Alabama at Birmingham Health System and Children’s Hospital of Alabama (UG1 HD34216, M01 RR32) – Waldemar A. Carlo, MD; Namasivayam Ambalavanan, MD; Myriam Peralta-Carcelen, MD MPH; Monica V. Collins, RN BSN MaEd; Shirley S. Cosby, RN BSN; Fred J. Biasini, PhD; Kristen C. Johnston, MSN CRNP; Kathleen G. Nelson, MD; Cryshelle S. Patterson, PhD; Vivien A. Phillips, RN BSN; Sally Whitley, MA OTR-L FAOTA.
University of California - Los Angeles, Mattel Children’s Hospital, Santa Monica Hospital, Los Robles Hospital and Medical Center, and Olive View Medical Center (UG1 HD68270) – Uday Devaskar, MD; Meena Garg, MD; Isabell B. Purdy, PhD CPNP; Teresa Chanlaw, MPH; Rachel Geller, RN BSN.
University of California – San Diego Medical Center and Sharp Mary Birch Hospital for Women and Newborns (U10 HD40461) – Neil N. Finer, MD; Yvonne E. Vaucher, MD MPH; David Kaegi, MD; Maynard R. Rasmussen, MD; Kathy Arnell, RNC; Clarence Demetrio, RN; Martha G. Fuller, PhD RN MSN; Wade Rich, BSHS RRT.
University of Iowa and Mercy Medical Center (UG1 HD53109, M01 RR59) – Tarah T. Colaizy, MD MPH; Michael J. Acarregui, MD; Jane E. Brumbaugh, MD; Jonathan M. Klein, MD; John M. Dagle, MD; Diane L. Eastman, RN CPNP MA; Karen J. Johnson, RN BSN; Jacky R. Walker, RN; John A. Widness, MD; Dan L. Ellsbury, MD; Donia B. Campbell, RNC-NIC; Tracy L. Tud, RN.
University of Miami, Holtz Children’s Hospital (U10 HD21397, M01 RR16587) – Shahnaz Duara, MD; Charles R. Bauer, MD; Ruth Everett-Thomas, RN MSN; Sylvia Fajardo-Hiriart, MD; Arielle Rigaud, MD; Maria Calejo, MS; Silvia M. Frade Eguaras, MA; Michelle Harwood Berkowits, PhD; Andrea Garcia, MS; Helina Pierre, BA; Alexandra Stoerger, BA.
University of New Mexico Health Sciences Center (UG1 HD53089, M01 RR997) – Kristi L. Watterberg, MD; Jean R. Lowe, PhD; Janell F. Fuller, MD; Robin K. Ohls, MD; Conra Backstrom Lacy, RN; Andrea F. Duncan, MD MScr; Rebecca A. Thomson, RN BSN; Carol H. Hartenberger, MPH RN; Sandra Brown, RN BSN; Elizabeth Kuan, RN BSN.
University of Pennsylvania, Hospital of the University of Pennsylvania, Pennsylvania Hospital, and Children’s Hospital of Philadelphia (UG1 HD68244) – Barbara Schmidt, MD MSc; Haresh Kirpalani, MB MSc; Soraya Abbasi, MD; Aasma S. Chaudhary, BS RRT; Erik A. Jensen, MD MSCE; Toni Mancini, RN BSN CCRC; Noah Cook, MD; Dara M. Cucinotta, RN; Judy C. Bernbaum, MD; Marsha Gerdes, PhD; Hallam Hurt, MD; Saritha Vangala, RN MSN.
University of Rochester Medical Center, Golisano Children’s Hospital, and the University at Buffalo Women’s and Children’s Hospital of Buffalo (UG1 HD68263, U10 HD40521, M01 RR44, UL1 TR42) – Carl T. D’Angio, MD; Dale L. Phelps, MD; Ronnie Guillet, MD PhD; Satyan Lakshminrusimha, MD; Michelle Andrews-Hartley, MD; Julie Babish Johnson, MSW; Kyle Binion, BS; Melissa Bowman, RN NP; Erica Burnell, RN; Cait Fallone, MA; Osman Farooq, MD; Stephanie Guilford, BS; Cassandra A. Horihan, MS; Julianne Hunn, BS; Diane Hust, MS RN CS; Rosemary L. Jensen; Emily Kushner, MA; Deanna Maffett, RN; Joan Merzbach, LMSW; Gary J. Myers, MD; Constance Orme; Diane Prinzing; Linda J. Reubens, RN CCRC; Anne Marie Reynolds, MD, MPH; Mary Rowan, RN; Michael G. Sacilowski, MAT CCRC; Ann Marie Scorsone, MS CCRC; Holly I.M. Wadkins, MA; Ashley Williams, MS Ed; Karen Wynn, RN; Kelley Yost, PhD; William Zorn, PhD; Lauren Zwetsch, RN MS PNP.
University of Texas Southwestern Medical Center at Dallas, Parkland Health & Hospital System, and Children’s Medical Center Dallas (UG1 HD40689, M01 RR633) – Myra H. Wyckoff, MD; Luc P. Brion, MD; Roy J. Heyne, MD; Walid A. Salhab, MD; Charles R. Rosenfeld, MD; Diana M. Vasil, MSN BSN RNC-NIC; Lijun Chen, PhD RN; Alicia Guzman; Gaynelle Hensley, RN; Melissa H. Leps, RN; Nancy A. Miller, RN; Janet S. Morgan, RN; Lara Pavageau, MD; Sally S. Adams, MS RN CPNP; Catherine Twell Boatman, MS CIMI; Elizabeth T. Heyne, MS MA PAC PsyD; Linda A. Madden, RN CPNP; Lizette E. Lee, RN.
University of Utah Medical Center, Intermountain Medical Center, LDS Hospital, and Primary Children’s Medical Center (UG1 HD87226, U10 HD53124, M01 RR64, UL1 RR25764) – Roger G. Faix, MD; Bradley A. Yoder, MD; Karen A. Osborne, RN BSN CCRC; Cynthia Spencer, RNC BSN; Kimberlee Weaver-Lewis, RN MS; Shawna Baker, RN; Karie Bird, RN BSN; Jill Burnett, RNC BSN; Michael Steffen, MS CPM; Jennifer J. Jensen, RN BSN; Sarah Winter, MD; Karen Zanetti, RN.
Wake Forest University, Baptist Medical Center, Forsyth Medical Center, and Brenner Children’s Hospital (U10 HD40498, M01 RR7122) – T. Michael O’Shea, MD MPH; Robert G. Dillard, MD; Lisa K. Washburn, MD; Barbara G. Jackson, RN, BSN; Nancy Peters, RN; Korinne Chiu, MA; Deborah Evans Allred, MA LPA; Donald J. Goldstein, PhD; Raquel Halfond, MA; Carroll Peterson, MA; Ellen L. Waldrep, MS; Cherrie D. Welch, MD MPH; Melissa Whalen Morris, MA; Gail Wiley Hounshell, PhD.
Wayne State University, Hutzel Women’s Hospital and Children’s Hospital of Michigan (UG1 HD21385) – Seetha Shankaran, MD; Athina Pappas, MD; John Barks, MD; Rebecca Bara, RN BSN; Katherine Abramczyk; Prashant Agarwal, MD; Monika Bajaj, MD; Elizabeth Billian, RN MBA; Sanjay Chawla, MD; Mary Christensen, RT; Lilia C. De Jesus, MD; Debra Driscoll, RN BSN; Melissa February, MD; Laura A. Goldston, MA; Mary E. Johnson, RN BSN; Geraldine Muran, RN BSN; Girija Natarajan, MD; Jeannette E. Prentiss, MD; Beena G. Sood, MD MS; Stephanie A. Wiggins, MS; Diane White RT; Eunice Woldt, RN MSN.
Yale University, Yale-New Haven Children’s Hospital, and Bridgeport Hospital (U10 HD27871, ULTR142) – Richard A. Ehrenkranz, MD (deceased); Harris Jacobs, MD; Christine G. Butler, MD; Patricia Cervone, RN; Sheila Greisman, RN; Monica Konstantino, RN BSN; JoAnn Poulsen, RN; Janet Taft, RN BSN; Joanne Williams, RN BSN; Elaine Romano, MSN.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Portions of this study were presented at the Pediatric Academic Societies annual meeting, May 5-8, 2018, Toronto, Canada.
Data Sharing: Data reported in this paper may be requested through a data use agreement. Further details are available at https://neonatal.rti.org/index.cfm?fuseaction=DataRequest.Home.
REFERENCES
- (1).Puopolo KM, Benitz WE, Zaoutis TE, COMMITTEE ON FETUS AND NEWBORN, COMMITTEE ON INFECTIOUS DISEASES. Management of Neonates Born at <34 6/7 Weeks’ Gestation With Suspected or Proven Early-Onset Bacterial Sepsis. Pediatrics 2018;142:101542/peds.2018–2896. [Google Scholar]
- (2).Piantino J, Schreiber M, Alexander K, Hageman J. Culture Negative Sepsis and Systemic Inflammatory Response Syndrome in Neonates. NeoReviews 2013;14:e294–305. [Google Scholar]
- (3).Cantey JB, Wozniak PS, Sanchez PJ. Prospective surveillance of antibiotic use in the neonatal intensive care unit: results from the SCOUT study. Pediatr Infect Dis J 2015;34:267–272. [DOI] [PubMed] [Google Scholar]
- (4).Schulman J, Profit J, Lee HC, Duenas G, Bennett MV, Parucha J, et al. Variations in Neonatal Antibiotic Use. Pediatrics 2018;142:101542/peds.2018–0115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (5).Greenberg RG, Chowdhury D, Hansen NI, Smith PB, Stoll BJ, Sanchez PJ, et al. Prolonged duration of early antibiotic therapy in extremely premature infants. Pediatr Res 2019;85:994–1000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (6).Schulman J, Dimand RJ, Lee HC, Duenas GV, Bennett MV, Gould JB. Neonatal intensive care unit antibiotic use. Pediatrics 2015;135:826–833. [DOI] [PubMed] [Google Scholar]
- (7).Flannery DD, Ross RK, Mukhopadhyay S, Tribble AC, Puopolo KM, Gerber JS. Temporal Trends and Center Variation in Early Antibiotic Use Among Premature Infants. JAMA Network Open 2018;1:e180164–e180164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (8).Puopolo KM, Mukhopadhyay S, Hansen NI, Cotten CM, Stoll BJ, Sanchez PJ, et al. Identification of Extremely Premature Infants at Low Risk for Early-Onset Sepsis. Pediatrics 2017;140:101542/peds.2017–0925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (9).Fouhy F, Guinane CM, Hussey S, Wall R, Ryan CA, Dempsey EM, et al. High-throughput sequencing reveals the incomplete, short-term recovery of infant gut microbiota following parenteral antibiotic treatment with ampicillin and gentamicin. Antimicrob Agents Chemother 2012;56:5811–5820. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (10).Leclercq S, Mian FM, Stanisz AM, Bindels LB, Cambier E, Ben-Amram H, et al. Low-dose penicillin in early life induces long-term changes in murine gut microbiota, brain cytokines and behavior. Nat Commun 2017;8:15062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (11).Tang AT, Choi JP, Kotzin JJ, Yang Y, Hong CC, Hobson N, et al. Endothelial TLR4 and the microbiome drive cerebral cavernous malformations. Nature 2017;545:305–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (12).Adams-Chapman I, Heyne RJ, DeMauro SB, Duncan AF, Hintz SR, Pappas A, et al. Neurodevelopmental Impairment Among Extremely Preterm Infants in the Neonatal Research Network. Pediatrics 2018:141:101542/peds.2017–3091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (13).Austin PC. A critical appraisal of propensity-score matching in the medical literature between 1996 and 2003. Stat Med 2008;27:2037–2049. [DOI] [PubMed] [Google Scholar]
- (14).Adams-Chapman I, Hansen NI, Shankaran S, Bell EF, Boghossian NS, Murray JC, et al. Ten-year review of major birth defects in VLBW infants. Pediatrics 2013;132:49–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (15).Stoll BJ, Hansen NI, Bell EF, Walsh MC, Carlo WA, Shankaran S, et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA 2015;314:1039–1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (16).Bayley N Manual for the Bayley Scales of Infant and Toddler Development, Third edition San Antonio, TX: Hartcourt; 2006. [Google Scholar]
- (17).Palisano RJ, Avery L, Gorter JW, Galuppi B, McCoy SW. Stability of the Gross Motor Function Classification System, Manual Ability Classification System, and Communication Function Classification System. Dev Med Child Neurol 2018;60:1026–1032. [DOI] [PubMed] [Google Scholar]
- (18).Younge N, Goldstein RF, Bann CM, Hintz SR, Patel RM, Smith PB, et al. Survival and Neurodevelopmental Outcomes among Periviable Infants. N Engl J Med 2017;376:617–628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (19).Agarwal PK, Shi L, Rajadurai VS, Zheng Q, Yang PH, Khoo PC, et al. Factors affecting neurodevelopmental outcome at 2 years in very preterm infants below 1250 grams: a prospective study. J Perinatol 2018;38:1093–1100. [DOI] [PubMed] [Google Scholar]
- (20).You J, Shamsi BH, Hao MC, Cao CH, Yang WY. A study on the neurodevelopment outcomes of late preterm infants. BMC Neurol 2019;19:108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (21).Bonnevier A, Brodszki J, Bjorklund LJ, Kallen K. Underlying maternal and pregnancy-related conditions account for a substantial proportion of neonatal morbidity in late preterm infants. Acta Paediatr 2018; doi: 10.1111/apa.14321. [DOI] [PubMed] [Google Scholar]
- (22).Synnes A, Luu TM, Moddemann D, Church P, Lee D, Vincer M, et al. Determinants of developmental outcomes in a very preterm Canadian cohort. Arch Dis Child Fetal Neonatal Ed 2017. ;102:F235–F234. [DOI] [PubMed] [Google Scholar]
- (23).Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr 1978. ;92:529–534. [DOI] [PubMed] [Google Scholar]
- (24).Bell MJ. Neonatal necrotizing enterocolitis. N Engl J Med 1978. February 2;298(5):281–282. [PubMed] [Google Scholar]
- (25).Walsh MC, Kliegman RM. Necrotizing enterocolitis: treatment based on staging criteria. Pediatr Clin North Am 1986;33:179–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (26).Zou G A modified poisson regression approach to prospective studies with binary data. Am J Epidemiol 2004;159:702–706. [DOI] [PubMed] [Google Scholar]
- (27).Austin PC. A comparison of 12 algorithms for matching on the propensity score. Stat Med 2014. ;33:1057–1069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (28).Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med 2009;28:3083–3107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (29).Stuart EA. Matching methods for causal inference: A review and a look forward. Stat Sci 2010. ;25:1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (30).D’Agostino RB Jr, D’Agostino RB Sr. Estimating treatment effects using observational data. JAMA 2007; 297:314. [DOI] [PubMed] [Google Scholar]
- (31).Weston EJ, Pondo T, Lewis MM, Martell-Cleary P, Morin C, Jewell B, et al. The burden of invasive early-onset neonatal sepsis in the United States, 2005–2008. Pediatr Infect Dis J 2011. ;30:937–941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (32).Stoll BJ, Hansen NI, Sanchez PJ, Faix RG, Poindexter BB, Van Meurs KP, et al. Early onset neonatal sepsis: the burden of group B Streptococcal and E. coli disease continues. Pediatrics 2011. ;127:817–826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (33).Schrag SJ, Farley MM, Petit S, Reingold A, Weston EJ, Pondo T, et al. Epidemiology of Invasive Early-Onset Neonatal Sepsis, 2005 to 2014. Pediatrics 2016;138:101542/peds.2016–2013. [DOI] [PubMed] [Google Scholar]
- (34).Stoll BJ, Hansen NI, Adams-Chapman I, Fanaroff AA, Hintz SR, Vohr B, et al. Neurodevelopmental and growth impairment among extremely low-birth-weight infants with neonatal infection. JAMA 2004. November 17;292(19):2357–2365. [DOI] [PubMed] [Google Scholar]
- (35).Klinger G, Levy I, Sirota L, Boyko V, Lerner-Geva L, Reichman B, et al. Outcome of early-onset sepsis in a national cohort of very low birth weight infants. Pediatrics 2010;125:e736–40. [DOI] [PubMed] [Google Scholar]
- (36).Mitha A, Foix-L’Helias L, Arnaud C, Marret S, Vieux R, Aujard Y, et al. Neonatal infection and 5-year neurodevelopmental outcome of very preterm infants. Pediatrics 2013;132:e372–80. [DOI] [PubMed] [Google Scholar]
- (37).Cotten CM, Taylor S, Stoll B, Goldberg RN, Hansen NI, Sanchez PJ, et al. Prolonged duration of initial empirical antibiotic treatment is associated with increased rates of necrotizing enterocolitis and death for extremely low birth weight infants. Pediatrics 2009;123:58–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- (38).Ting JY, Synnes A, Roberts A, Deshpandey A, Dow K, Yoon EW, et al. Association Between Antibiotic Use and Neonatal Mortality and Morbidities in Very Low-Birth-Weight Infants Without Culture-Proven Sepsis or Necrotizing Enterocolitis. JAMA Pediatr 2016;170:1181–1187. [DOI] [PubMed] [Google Scholar]
- (39).Cantey JB, Pyle AK, Wozniak PS, Hynan LS, Sanchez PJ. Early Antibiotic Exposure and Adverse Outcomes in Preterm, Very Low Birth Weight Infants. J Pediatr 2018;203:62–67. [DOI] [PubMed] [Google Scholar]
- (40).Ting JY, Roberts A, Sherlock R, Ojah C, Cieslak Z, Dunn M, et al. Duration of Initial Empirical Antibiotic Therapy and Outcomes in Very Low Birth Weight Infants. Pediatrics 2019;143:101542/peds.2018–2286. [DOI] [PubMed] [Google Scholar]
- (41).Ting JY, Synnes A, Roberts A, Deshpandey AC, Dow K, Yang J, et al. Association of Antibiotic Utilization and Neurodevelopmental Outcomes among Extremely Low Gestational Age Neonates without Proven Sepsis or Necrotizing Enterocolitis. Am J Perinatol 2018;35:972–978. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.