

Abstract
The treatment of type 3 acromioclavicular joint injuries has still controversial issues. In this retrospective study, we aimed to compare the radiological and functional outcomes of the suture anchor and double-button fixation methods for the treatment of type 3 acromioclavicular joint injuries.
This study included 20 patients who underwent suture anchor (9 patients) and double-button fixations (11 patients) for isolated type 3 acromioclavicular dislocation. Injuries were classified according to the Rockwood Classification System. Coracoclavicular(CC) distances and anterior translation have been measured pre-operatively and at the 12th month follow-up. Functional evaluation was performed using the DASH, and Constant–Murley scores of the patients were recorded at the12th-month follow-up.
The mean age of the patients was 37 (22–50) years in Group 1(double-button group) and 39 (24–56) years in Group 2(suture anchor group). All of the patients were male. There was no statistically significant difference between the DASH and Constant–Murley scores of the 2 groups (P > .05). The mean DASH score of the patients evaluated at the postoperative 12th month was 6.65 (0–38.3) in Group 1 and 2.48 (0–4.2) in Group 2. The mean Constant-Murley score of the patients evaluated at the postoperative 12th month was 89,6 (50–98) in Group 1 and 93,6 (90–98) in Group 2. Comparison of the pre- and post-operative CC distances and pre- and post-operative anterior translation distances of both groups revealed that there was no statistically significant difference between groups regarding postoperative CC distances and anterior translation distances (P > .05).
Suture anchor and double-button techniques are reliable treatment methods that are not superior to one another and can yield excellent functional outcomes
Keywords: acromioclavicular dislocation, double-button, stability, suture anchor, translation
1. Introduction
Acromioclavicular joint (ACJ) injuries are one of the most common injuries of the upper extremity.[1] ACJ injuries which roughly account for half of the athletic shoulder injuries are frequently observed in the young, athletic population as well as in all age groups after high energy trauma.[2,3]
Optimal management for Rockwood type 3 ACJ injuries is still controversial, and further sub-classification depending on the stability of the ACJ was proposed to assist clinical decision making.[4] Various techniques with different success rates, advantages, and disadvantages, have been proposed for the surgical treatment of ACJ injuries, such as pinning of the AC joint, coracoclavicular (CC) loop cerclage technique, hook plates, CC screws, CC ligament repairs, coracoid transfer, distal clavicle excision, muscle-ligament transfers, and various arthroscopically assisted techniques.[5–13] However, still, no single technique has been proved to be superior to others.[14]
The suture anchor technique defined by Jingwei et al is advocated to provide restoration of ACJ stability in both planes.[15] Also, double-button technique reported providing satisfactory stability via a simple technique.[16]
This study aims to compare the functional and radiological outcomes of the suture anchor and double-button methods for the fixation of type-3 ACJ injuries.
2. Materials and methods
This retrospective study was performed at our institution, which is a regional Level 1 trauma center. Shoulder trauma patients had been consulted by a single orthopedic surgeon experienced in shoulder surgery between 2014 and 2018. Patients with type 3 AC joint injuries were managed surgically unless there was a contraindication for surgery or the patient refused surgical treatment.
The patients had surgical fixation of the AC joint injuries with the use of either suture anchors or Biomet Zip-TightTM system depending on the availability of the fixation material. This resulted in 2 groups of consecutive patients who are the subjects of this study.
After ethical approval of the study by the Ethical Board of Erzurum Regional Research and Training hospital with the file number 19.02.18/37732058-514.13, charts of all patients who had suture anchor or double-button technique between January 2014 and September 2017 for acute type 3 ACJ injury were retrospectively reviewed. All of the patients were operated by the same surgeon experienced in shoulder trauma. The inclusion criteria were acute type 3 ACJ injury, the availability of at least 1 year follow-up and age between 18 and 60. Exclusion criteria were skeletally immature patients with open physis, and patients having concomitant injuries. The patients were randomly selected for the suture anchor and the double button fixation groups. Written informed consent was obtained from all of the patients regarding scientific research and medical interventions at the initial admission to the hospital.
Twenty six patients who had surgical treatment for type 3 ACJ injuries and had a minimum follow-up period of 1 year were retrieved. One patient with open physis, 1 patient with bilateral ACJ injury, 1 with concomitant ipsilateral acromial fracture, 2 with concomitant ipsilateral proximal humeral fractures, and 1 with subarachnoid hemorrhage were excluded. Eleven of the remaining patients had double-button fixation, 9 had suture anchor fixation methods.
2.1. Surgical method and postoperative protocol
All patients underwent surgery under general anesthesia in the beach-chair position. The infraclavicular block was performed at the end of the operation to provide postoperative analgesia. All patients were administered 2 g of a first-generation cephalosporin preoperatively. Following the confirmation of the dislocated side with fluoroscopy, a longitudinal incision of approximately 3 to 5 cm was done from the medial side of the AC joint extending to the coracoid process. The dislocated AC joint was exposed with minimum soft tissue injury and by blunt dissection of soft tissues, and then the coracoid process was exposed.
2.2. Suture anchor method
A 5-mm suture anchor with 4 strands was placed by drilling toward the base of the coracoid process. Two holes were created on the coronal plane with a 2.7-mm drill over the clavicle at the region of the remnants of trapezoid and conoid ligaments. After the reduction of the AC joint, temporary fixation was performed with a 2-mm Kirschner wire. Strands of the suture anchor were passed through the holes in pairs and tied over the clavicle. Following the removal of the Kirschner wire, a 5-mm suture anchor with 4 strands was inserted into the distal part of the clavicle. The strands were passed through the holes drilled with the 2.7-mm drill over the acromion and clavicle and tied over the joint (Figs. 1–3). Following the completion of the fixation, the AC joint was examined for implant irritation and stability.
Figure 1.
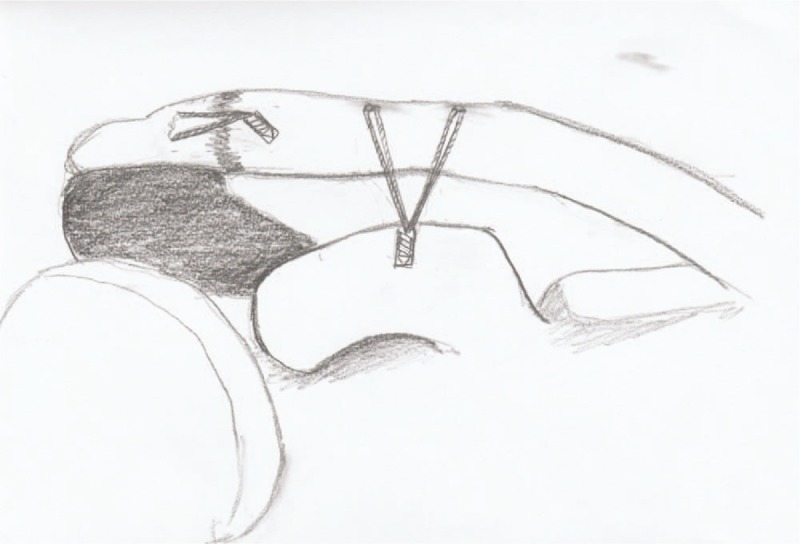
Suture anchor technique for AC injury fixation.
Figure 3.

Direct X-ray AP view of patient with type 3 AC injury after fixation with suture anchors.
Figure 2.

Direct X-ray AP view of patient with type 3 AC injury.
2.3. Double-button method
The double-button knotless suture anchor technique was performed using Biomet Zip-TightTM system. Temporary fixation of AC joint was performed with a 2-mm Kirschner wire, and then the sharp end of the guide was placed under the coracoid process. A Kirschner wire guide was advanced toward the base of the coracoid process over the clavicle. The holes on the clavicle and coracoid were opened with a 3.2-mm drill to be aligned on a single axis. The buttons were placed and tightened. After the adjustment of the tightness of the strands, the Kirschner wire was removed. The stability of the fixation and the presence of translation were assessed (Figs. 4–6).
Figure 4.
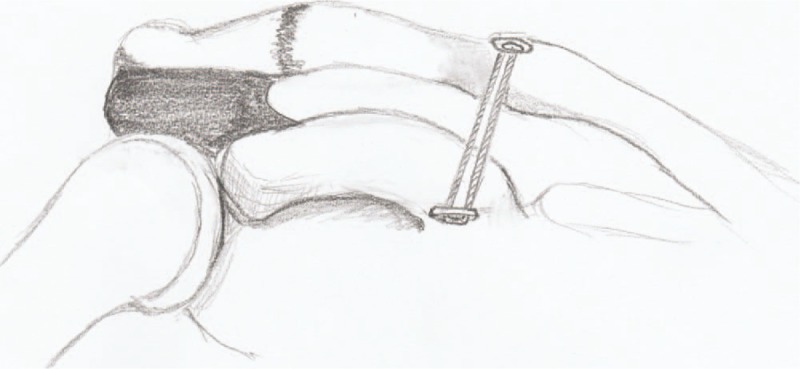
Double-Button technique for AC injury fixation.
Figure 6.

Direct X-ray AP view of patient with type 3 AC injury after fixation with double buttons.
Figure 5.

Direct X-ray AP view of patient with type 3 AC injury.
The follow-up, functional, and radiologic evaluation of the patients had been performed by the same orthopedic surgeon who operated the patients. Patients had been kept in a sling for 1 month after the operation, allowing only passive range of motion (ROM) exercises. In the following weeks, patients progressed to active motion until full ROM is achieved, and strengthening exercises were begun afterward. Patients were routinely followed up with anteroposterior and axial radiographs obtained at 1st, 3rd, 6th, and 12th months postoperatively unless there was a complication that required intervention and close follow-up. Additionally, 3D CT images of the patients were obtained only at the postoperative 12th-month follow-up for the evaluation of the ACJ in both vertical and horizontal planes. Depending on the radiographic evaluation, ACJ injuries were graded, and distances between the clavicle and coracoid process (C-C distance) were measured. Functional scores were evaluated the Disabilities of the Arm, Shoulder, and Hand (DASH), and Constant–Murley scores of the patients were recorded at the 12th-month follow-up. Complications such as infections, loss of fixation, reoperation, and implant failures observed during the follow-ups were also recorded.
2.4. Statistical analysis
Statistical analyses were performed by IBM SPSS.20 computer software. Data were presented as mean, number, percent, and standard deviation. Shapiro–Wilk test was used to determine whether the data were normally distributed or not. Mann–Whitney U, Fisher exact, Chi-Squared, and the Student t test were performed for comparison between the groups. The level of significance was set at P < .05.
3. Results
Baseline characteristics of the patients (age, gender, dislocated side, trauma etiology, time from admission to operation, operation time, fluoroscopy time, and duration of follow-up) are noted in Table 1.
Table 1.
Baseline characteristics of patients.
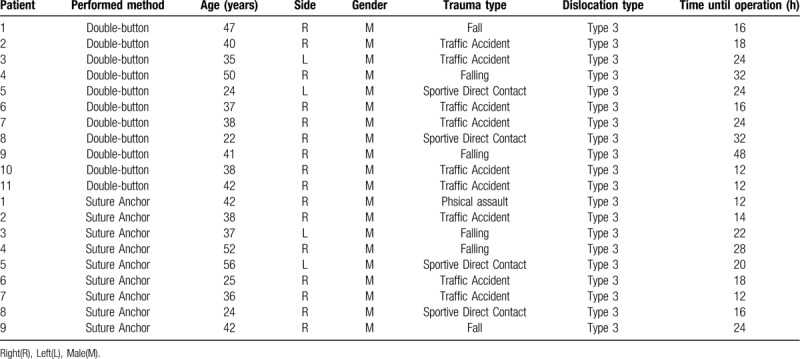
Eleven patients who underwent double-button fixation were designated as Group 1, and 9 patients who underwent suture anchor fixation were designated as Group 2. All patients included in the study were male. The mean age of the patients was 37 (22–50) years in Group 1 and 39 (24–56) years in Group 2. Group 1 consisted of 9 patients with the right shoulder, 2 patients with left shoulder injuries. Group 2 consisted of 7 patients with right shoulder, 2 patients with left shoulder injuries. Etiologically, out of the 20 patients, the cause of injury was fall in 6 patients, traffic accidents in 9 patients, athletic injuries in 4 patients, and physical assault in 1 patient. All patients included in the study had type 3 ACJ injuries. The mean time to the operation was 23 (12–48) hours in Group 1 and 18 (12–28) hours in Group 2. The mean duration of follow-up was 13,8 (12–21) months in Group 1 and 12,7 (12–16) months in Group 2.
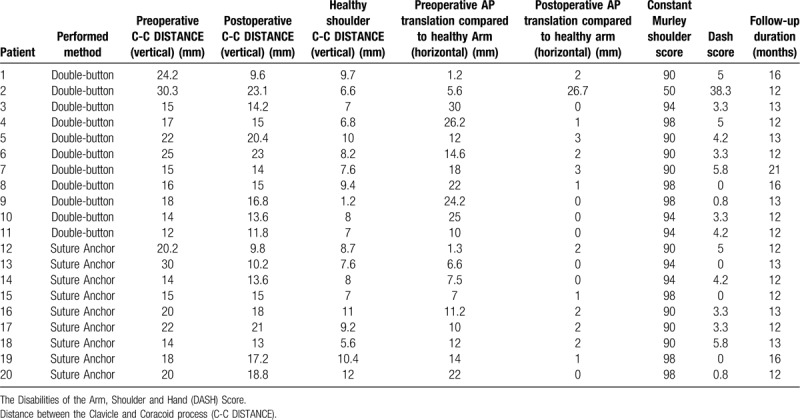
ACJ injuries were evaluated according to the Rockwood Classification System.[17] The mean preoperative distance between the clavicle and coracoid process (C-C distance) in Group 1 was 19 (12–30) mm. The mean C-C distance at the postoperative 12th-month follow-up was 16 (9.6–23.1) mm. This distance in the intact shoulder of the patients in this group was recorded as 7.4 (7–9.7) mm. The mean preoperative C-C distance in Group 2 was 19 (14–30) mm. The mean C-C distance at the postoperative 12th-month follow-up was 15.7 (9.8–18.8) mm. This distance in the intact shoulder of the patients in this group was recorded as 8.83 (7–10.4) mm. There was no statistically significant difference in terms of the postoperative C-C distance between the 2 groups (P > .05).
Translation of distal clavicle on the horizontal plane was measured and recorded in both groups in comparison to the intact shoulder in the preoperative period and at the postoperative 12th-month follow-up. Translation in the posterior direction was not observed in any of the patients. Anterior translation compared to the intact shoulder in Group 1 was recorded as 17.16 (1.2–26.2) mm in the preoperative period and 3.51 (0–26.7) mm in the postoperative period. This translation was recorded as 8.32 (1.3–22) mm in the preoperative period and 1.11 (0–2) mm in the postoperative period in Group 2. There was no statistically significant difference in terms of the postoperative anterior translation between the 2 groups (P > .05).
The mean DASH score of the patients evaluated at the postoperative 12th month was 6.65 (0–38.3) in Group 1 and 2.48 (0–4.2) in Group 2. There was no statistically significant difference between the DASH scores of the 2 groups (P > .05). The mean Constant–Murley score of the patients evaluated at the postoperative 12th month was 89,6 (50–98) in Group 1 and 93,6 (90–98) in Group 2. There was no statistically significant difference between the Constant–Murley scores of the 2 groups (P > .05) All postoperative outcomes of the patients are presented in Table 2 (Table 2).
Table 2.
Functional and radiological results of patients.
No infection was observed in both groups. Revision surgery was performed with a Kirschner wire after observation of fixation loss in 1 patient in Group 1 at a 1st-month follow-up. The wires in this patient were removed 20 days after 3 weeks of immobilization with Velpeau bandage.
4. Discussion
Both of the surgical techniques achieved satisfactory functional as well as radiological outcomes in the treatment of type 3 ACJ injuries. The suture anchor method was proposed to provide better anteroposterior stability. However, comparing the anterior translation distance of the groups, at last, follow up, there was no significant difference between the groups, and the overall functional outcomes were similar.
The primary purpose of surgical treatment for AC injuries is to reduce the AC joint and provide adequate stability for keeping reduction. There is still no consensus on the best technique and, there are more than 50 different methods for the treatment of ACJ injuries reported in the literature.[18]
Jerosch et al compared 8 different fixation methods and reported that a single coracoid sling procedure results in anterior displacement and fixation with an anchor placed in the base of the coracoid process, and the hole created in the medial clavicle is a system that best restores the anatomy.[19] Dimakopulos et al reported that horizontal stability is just as important as vertical stability and that they achieved good results because the CC cerclage method that they used provided adequate stabilization in both planes.[20] Breslow et al compared suture anchor and suture cerclage methods and achieved similar results with both methods; however, damage to the neurovascular structures was less likely, and the operation time was shorter with suture anchor method.[21] Jingwei et al achieved excellent results with a method in which they performed AC fixation with CC fixation in order to obtain horizontal stability, which is also similar to the suture anchor method used in our study.[15]
Chernchujit et al used arthroscopy-assisted AC and CC fixation methods and emphasized that the AC joint must be stabilized in both vertical and horizontal planes. Particular studies also reported that CC ligaments provide approximately two-thirds of the force preventing the vertical translation, whereas joint capsule and AC ligaments prevent horizontal displacement.[22–24] Other studies have shown that an essential structure preventing translation in the anterior and superior direction is the conoid ligament, which is one of the CC ligaments.[25,26]
Beris et al argued that sufficient strength against displacement in both anterior and superior directions could be acquired with double button fixation techniques alone, without applying additional fixation to the AC joint. They stated that the fixation loss in first-generation materials is usually because of the bone erosion in the clavicle due to the use of small buttons, the proximal button size was increased; thus, erosion was decreased, and satisfactory results were obtained. The most important aspect of this method is the anatomic location of the hole in the coracoid. A hole that is not opened precisely at the center of the coracoid in the coronal plane and as close to the base as possible, will negatively affect the anterior stabilization of the fixation, can cause the coracoid process to be broken, and lead to displacement in the vertical plane.[27]
While performing fixation, attention is almost always paid to vertical stability, whereas horizontal stability is often overlooked. Lack of adequate stabilization in the vertical or horizontal planes after AC joint dislocation can cause chronic pain and limitation in the shoulder functions of the patient in the long-term. Adequate fixation in both planes while choosing the surgical technique would prevent pain and degenerative changes in the AC joint that may occur in the future.[28–30]
We think that the satisfactory functional outcomes achieved in both groups with different surgical methods are associated with the achievement of horizontal stability as well as the vertical stability during the application of suture anchor and double-button methods. We believe that prospective, clinical, or biomechanical studies evaluating larger comparison groups are needed to determine the single best method of ACJ injuries.
Although both methods seem to have yielded similar success, there was a reduction loss in 1 patient in the group that underwent fixation using the double-button method. We believe that this complication was due to fixation with inadequate thread tightness during the application of the method and lack of surgical experience because this was the first patient in the series. Thus, we believe that when deciding the surgical method for type 3 AC injuries along with the knowledge that these 2 methods have similar results, it would be beneficial that the operating surgeon prefers the method that he or she is most experienced with.
Being a single-center study, the same surgeon operating all of the patients, comparatively homogenous groups of patients are strengths of our study. The limitations of our study include the small number of patients, relatively shorter follow-up time, and problems associated with the retrospective design. Prospective, randomized controlled, and multi-center studies on a more extensive patient series will provide more information on the treatment of type 3 AC joint injuries.
5. Conclusion
Both of the techniques resulted in satisfactory outcomes for the patients without being superior to one another. Surgeons can prefer both of these techniques reliably in the surgical treatment of patients with type 3 ACJ injuries.
Acknowledgments
We would like to thank Prof. Dr. Mehmet Topal for assistance with statistical analysis and Kelly Dye for reviewing the article as a native speaker of English language.
Author contributions
Conceptualization: Murat Topal, Ahmet Köse.
Data curation: Murat Topal, Ahmet Köse.
Investigation: Murat Topal.
Methodology: Murat Topal, Ahmet Köse.
Writing – original draft: Murat Topal, Ahmet Köse.
Writing – review & editing: Murat Topal, Ahmet Köse.
Footnotes
Abbreviations: AC = acromioclavicular, ACJ = acromioclavicular joint, CC = coracoclavicular, CC DISTANCE = Distance Between the Clavicle and Coracoid Process, DASH = The Disabilities of the Arm, Shoulder, and Hand, ROM = range of motion.
How to cite this article: Topal M, Köse A. Surgical management of Rockwood type 3 acromioclavicular joint injuries: a retrospective comparison of outcomes of suture anchor fixation and double-button fixation techniques. Medicine. 2020;99:21(e20312).
The study was approved by the ethics committee of our institution (ethics committee of EBEAH. / 19.02.18/37732058-514.13) and was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent was obtained from all individual participants included in the study. Patients signed informed consents on conduction of diagnostic procedures and medical interventions.
The authors declare that they have no conflict of interest.
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
References
- [1].Kocher MS, Dupré MM, Feagin JA. Shoulder injuries from alpine skiing and snowboarding. Sports Med 1998;25:201–11. [DOI] [PubMed] [Google Scholar]
- [2].Pallis M, Cameron KL, Svoboda SJ, et al. Epidemiology of acromioclavicular joint injury in young athletes. Am J Sports Med 2012;40:2072–7. [DOI] [PubMed] [Google Scholar]
- [3].Babhulkar A, Pawaskar A. Acromioclavicular joint dislocations. Curr Rev Musculoskelet Med 2014;7:33–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Beitzel K, Mazzocca AD, Bak K, et al. ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries. Arthroscopy 2014;30:271–8. [DOI] [PubMed] [Google Scholar]
- [5].Mazzocca AD, Santangelo SA, Johnson ST, et al. A biomechanical evaluation of an anatomical coracoclavicular ligament reconstruction. Am J Sports Med 2006;34:236–46. [DOI] [PubMed] [Google Scholar]
- [6].De Tullio V, Orsi R, Celenza M. Surgical treatment of Allman type III acromio-clavicular dislocation. A long-term follow-up study. Acta Orthop Belg 1994;60:300–2. [PubMed] [Google Scholar]
- [7].Sim E, Schwarz N, Höcker K, et al. Repair of complete acromioclavicular separations using the acromioclavicular-hook plate. Clin Orthop Relat Res 1995;314:134–42. [PubMed] [Google Scholar]
- [8].Sundaram N, Patel D, Porter D. Stabilization of acute acromioclavicular dislocation by a modified Bosworth technique: a long-term follow-up study. Injury 1992;23:189–93. [DOI] [PubMed] [Google Scholar]
- [9].Tienen TG, Oyen JF, Eggen PJ. A modified technique of reconstruction for complete acromioclavicular dislocation. Am J Sports Med 2003;31:655–9. [DOI] [PubMed] [Google Scholar]
- [10].Greiner S, Braunsdorf J, Perka C, et al. Mid to long-term results of open acromioclavicular-joint reconstruction using polydioxansulfate cerclage augmentation. Arch Orthop Trauma Surg 2009;129:735–40. [DOI] [PubMed] [Google Scholar]
- [11].Walz L, Salzmann G, Eichhorn S, et al. The anatomic reconstruction of AC joint dislocations using 2 TightRope®-a biomechanical study. Am J Sports Med Rev 2007. [DOI] [PubMed] [Google Scholar]
- [12].Lee S, Bedi A. Shoulder acromioclavicular joint reconstruction options and outcomes. Curr Rev Musculoskeletal Med 2016;9:368–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Lafosse L, Baier GP, Leuzinger J. Arthroscopic treatment of acute and chronic acromioclavicular joint dislocation. Arthroscopy 21:1017.e1011-1017. e1018. [DOI] [PubMed] [Google Scholar]
- [14].Frank RM, Cotter EJ, Leroux TS, et al. Acromioclavicular joint injuries: evidence-based treatment. JAAOS 2019;27:e775–88. [DOI] [PubMed] [Google Scholar]
- [15].Jingwei Z, Min L, Xianfeng H, et al. Operative treatment of acromioclavicular joint dislocation: a new technique with suture anchors. Chin J Traumatol 2014;17:187–92. [PubMed] [Google Scholar]
- [16].Lim YW, Sood A, van Riet RP, et al. Acromioclavicular joint reduction, repair and reconstruction using metallic buttons-early results and complications. Tech Shoulder Elbow Surg 2007;8:213–21. [Google Scholar]
- [17].Marsh JL, Slongo TF, Agel J, et al. Fracture and dislocation classification compendium - 2007: Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma 2007;21: 10 Suppl: S1–33. [DOI] [PubMed] [Google Scholar]
- [18].Tang G, Zhang Y, Liu Y, et al. Comparison of surgical and conservative treatment of Rockwood type-III acromioclavicular dislocation: a meta-analysis. Medicine 2018;97(4.): [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Jerosch J, Filler T, Peuker E, et al. Which stabilization technique corrects anatomy best in patients with AC-separation? An experimental study. Knee Surg Sports Traumatol Arthrosc 1999;7:365–72. [DOI] [PubMed] [Google Scholar]
- [20].Dimakopoulos P, Panagopoulos A, Syggelos SA, et al. Double-loop suture repair for acute acromioclavicular joint disruption. Am J Sports Med 2006;34:1112–9. [DOI] [PubMed] [Google Scholar]
- [21].Breslow MJ, Jazrawi LM, Bernstein AD, et al. Treatment of acromioclavicular joint separation: suture or suture anchors? J Shoulder Elbow Sur 2002;11:225–9. [DOI] [PubMed] [Google Scholar]
- [22].Fukuda K, Craig E, An K-N, et al. Biomechanical study of the ligamentous system of the acromioclavicular joint. JBJS 1986;68:434–40. [PubMed] [Google Scholar]
- [23].Harris RI, Wallace AL, Harper GD, et al. Structural properties of the intact and the reconstructed coracoclavicular ligament complex. J Sports Med 2000;28:103–8. [DOI] [PubMed] [Google Scholar]
- [24].Chernchujit B, Tischer T, Imhoff AB. Arthroscopic reconstruction of the acromioclavicular joint disruption: surgical technique and preliminary results. Arch Orthop Trauma Surg 2006;126:575–81. [DOI] [PubMed] [Google Scholar]
- [25].Costic RS, Labriola JE, Rodosky MW, et al. Biomechanical rationale for development of anatomical reconstructions of coracoclavicular ligaments after complete acromioclavicular joint dislocations. Am J Sports Med 2004;32:1–8. [DOI] [PubMed] [Google Scholar]
- [26].Harris RI, Vu DH, Sonnabend DH, et al. Anatomic variance of the coracoclavicular ligaments. J Shoulder Elbow Surg 2001;10:585–8. [DOI] [PubMed] [Google Scholar]
- [27].Beris A, Lykissas M, Kostas-Agnantis I, et al. Management of acute acromioclavicular joint dislocation with a double-button fixation system. Injury 2013;44:288–92. [DOI] [PubMed] [Google Scholar]
- [28].Post M. Current concepts in the diagnosis and management of acromioclavicular dislocations. Clin Orthop Relat Res 1985;200:234–47. [PubMed] [Google Scholar]
- [29].Rawes M, Dias J. Long-term results of conservative treatment for acromioclavicular dislocation. J Bone Joint 1996;78:410–2. [PubMed] [Google Scholar]
- [30].Calvo E, López-Franco M, Arribas IM. Clinical and radiologic outcomes of surgical and conservative treatment of type III acromioclavicular joint injury. J Shoulder Elbow Surg 2006;15:300–5. [DOI] [PubMed] [Google Scholar]