

Abstract
As COVID-19 delivered a devastating blow around Europe, unprecedented mental health issues have arisen. This study outlines the Greek translation and validation of the Fear of COVID-19 Scale (FCV-19S) in the general population. A sample of 3029 Greek-speaking individuals completed the FCV-19S, as part of a large online survey reporting on the aftermath of the coronavirus on the psychological health of Greeks. A total of 2970 participants completed all items without missing values, and their responses were included in the statistical analysis. The confirmatory factor analysis suggested an acceptable model fit. The internal consistency measured by Cronbach’s alpha = .87 for the whole scale. All hypothesized correlations were as expected, confirming the construct validity of the scale. The results of the analyses suggest that the psychometric properties of the Greek FCV-19S are sufficient.
Keywords: FCV-19S, Psychometric properties, Instrument, Greece, Pandemic, Validity
The novel coronavirus (COVID-19) pandemic has dramatically changed the daily functioning of most people. Routine overturn creates insecurity and uncertainty while social distancing at the same time weakens the individuals’ social network and triggers anxiety reactions (Kim et al. 2019).
Feelings of fear are expected when one is confronted with a potentially deadly virus. It may be useful to help develop strategies that will ensure safety. Excessive and prolonged fear though could lead to functionality reduction and impaired mental health. The fear of contracting the illness could lead to overreactions, like overprotection or rivalry toward non-compliers with measures or stigmatizing patients (Mowbray 2020; Shigemura et al. 2020).
Scientific discussions and research studies are focusing on identifying the potential implications of COVID-19 not only on physical health but on mental health as well. They also highlight that it is possible to predict more or less the expected consequences on mental and physical health of the most vulnerable segments of the population (Ahorsu et al. 2020; Kang et al. 2020; Pakpour and Griffiths 2020). One of the main goals of this effort is to identify individuals at risk and provide care for them. The need of valid self-completed instruments for screening purposes is more topical than ever since access to health care facilities may be limited or postponed due to the imposed measures. In mid-March, the Greek government specifically imposed an almost total lockdown on health care facilities allowing care for emergency cases only. Although this strategy was accredited internationally for having slowed the spread of the disease and having kept the number of deaths low (as of May 12, 2020, there have been 2744 confirmed COVID-19 cases and 152 deaths in Greece (Greek Minister of Health 2020)), psychology and psychiatry researchers lacked the opportunity to interview people at outpatients’ clinics so as to screen for anxiety or fear disorders related to the new virus.
The Fear of COVID-19 scale (FCV-19S) was designed in 2020 by Ahorsu et al. (2020) to assess the level of fear related to SARS-CoV-2. The scale has been found to be a useful tool for exploring COVID-19-related fear in Iran (Ahorsu et al. 2020), Italy (Soraci et al. 2020), Bangladesh (Sakib et al. 2020), Turkey (Satici et al. 2020), and Russia and Belarus (Reznik et al. 2020).
To investigate the broad aspects of fear in the Greek population, the translation and validation of the instrument is valuable, as it will allow researchers to draw useful conclusions. Therefore, the aims of the study were to translate and validate the Greek version of FCV-19S and to further explore its psychometric properties.
Methods
Translation and Cultural Adaptation
The adaptation process was developed in relation to the principal guidelines (Sousa and Rojjanasrirat 2011; Tsang et al. 2017; World Health Organization 2009). The forward translation was performed by two health care professionals fluent in English and the Greek version of the questionnaire was independently back-translated by one bilingual health care professional and one fluent in English: both blinded to the original English version. An expert panel consisting of two psychiatrists and two psychologists with experience in instrument development and translation compared all versions with the original scale in order to evaluate similarity in meaning and general linguistic clarity regarding the instructions, items, and response format, and to assure conceptual, semantic, and content equivalence of the items. A preliminary testing was conducted to further assess content adequacy and clarity of expression. Ten health care professionals working at Papageorgiou General Hospital (PGH) and twenty individuals (members of their families) were asked to reflect upon their understanding of each item and to rate the pre-final version of the translated scale using a dichotomous response choice (clear–not clear). The inter-rater agreement was 100% and no modifications were proposed. The final Greek version of the scale was administered on a larger sample of respondents to test its psychometric soundness.
Participants and Survey Procedure
A sample of 2970 individuals aged 18 years and over completed the final version of the Greek FCV-19S as part of a larger online survey, hosted by Qualtrics, addressing the psychological impact of the coronavirus pandemic on the general population in Greece. Participants with minor missing information on the sociodemographic characteristics were included in the subsequent analyses as they provided complete values on the self-report measures. The recommended sample size for the psychometric validation was exceeded, i.e., respondent-to-item ratio of at least 10:1 sample size or a minimum requirement of 450 respondents (Boateng et al. 2018).
Measures
Demographic Information
Background information questions were included to obtain data about the participants consisting of gender, age, educational level, professional status, and residential area.
Fear of COVID-19 Scale
FCV-19S consists of seven items (e.g., item 1, “I am most afraid of coronavirus-19”; item 4, “I am afraid of losing my life because of coronavirus-19”) assessing fear toward COVID-19. It is a self-report measure rated on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). Total scores range from 7 to 35 with higher scores representing greater fear against the novel coronavirus disease. The original scale showed very good internal consistency (α = .82) (Ahorsu et al. 2020). Equally sufficient internal consistency was provided from the Italian version (α = .87), the Bangla version (α = .87), the Turkish version (α = .84), and the Russian version (α = .80) as well.
Generalized Anxiety Disorder Assessment
Generalized Anxiety Disorder Assessment (GAD-7) was developed by Spitzer et al. (2006) and consists of seven items (e.g., item 2, “Not being able to stop or control worrying”; item 7, “Feeling afraid as if something awful might happen”) assessing the severity of the generalized anxiety disorder corresponding to worry and anxiety symptoms. It is a self-report measure rated on a 4-point Likert-type scale (0 = not at all to 3 = nearly every day). The total score ranges from 0 to 20, with higher scores representing greater severity. A score above 10 is considered to be clinically significant (Spitzer et al. 2006). In this study, the reliability coefficient of the scale was found to be α = .79.
Brief Patient Health Questionnaire Depression Scale
Patient Health Questionnaire (PHQ-9) is a depression scale developed by Spitzer et al. (1999). The scale consists of nine items (e.g., item 2, “Feeling down, depressed, or hopeless”; item 4, “Feeling tired or having little energy”) and is proved to be a useful tool to recognize major depression and subclinical levels of depressive symptoms in the general population (Martin et al. 2006). It is a self-report measure rated on a 4-point Likert-type scale (0 = not at all to 3 = nearly every day). A score ranging from 0 to 4 indicates no or minimal depression; 5 to 9, mild depression; 10 to 14, moderate depression; 15 to 19, moderate severe depression; and 20 to 27, severe depression (Kroenke et al. 2001). In this study, the reliability coefficient of the scale was found to be α = .84.
Data Analysis
The demographic variables of the sample were summarized using descriptive statistics. Concurrent validity was assessed using Pearson’s product-moment correlation coefficient with respect to previously established measures. Reliability of the scale was explored by computing Cronbach’s alpha. Confirmatory factor analysis (CFA) was performed to assess the goodness of fit of the unidimensional factor structure of the scale proposed by the developers. Several indices were used to explore model fit, including root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker–Lewis Index (TLI), and standardized root mean square residual (SRMR). Data were analyzed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, N.Y., USA), and CAF was performed using AMOS 23.0 statistic package (Arbuckle 2014).
Results
Demographics
A total of 2970 participants took part in the study: 2153 females (72.5%) and 727 males (24.5%). The majority of the participants (52%) belonged to the age group of 18–30, almost half of the participants (45.4%) had a university degree, and the majority lived in a residential area (76.5%). A total of 23.1% continued to work during the quarantine with 8.2% of them health care professionals (Table 1).
Table 1.
Sample demographics, FCV-19S mean, and SD
| Frequency | % | M | SD | ||
|---|---|---|---|---|---|
| Gender | Male | 727 | 24.5 | 14.69 | 4.98 |
| Female | 2153 | 72.5 | 17.43 | 5.06 | |
| Total | 2880 | 97.0 | |||
| Missing | 90 | 3.0 | |||
| Total | 2970 | 100.0 | |||
| Age | 18–30 | 1551 | 52.2 | 16.01 | 5.07 |
| 31–45 | 758 | 25.5 | 11.13 | 5.20 | |
| 46–60 | 543 | 18.3 | 18.05 | 5.30 | |
| 61–75 | 95 | 3.2 | 18.73 | 5.22 | |
| > 75 | 10 | 0.3 | 19.70 | 6.03 | |
| Total | 2957 | 99.6 | |||
| Missing | 13 | 0.4 | |||
| Total | 2970 | 100.0 | |||
| Education | Elementary school | 12 | 0.4 | 20.50 | 5.61 |
| Middle school | 32 | 1.1 | 19.50 | 6.80 | |
| High school | 886 | 29.8 | 16.32 | 5.48 | |
| University | 1347 | 45.4 | 16.99 | 5.05 | |
| MSc | 610 | 20.5 | 16.76 | 4.99 | |
| PhD | 70 | 2.4 | 17.04 | 5.68 | |
| Total | 2957 | 99.6 | 16.78 | 5.23 | |
| Missing | 13 | 0.4 | 17.04 | 5.68 | |
| Total | 2970 | 100.0 | 16.78 | 5.23 | |
| Residential area | Urban | 2271 | 76.5 | 16.83 | 5.25 |
| Small city | 320 | 10.8 | 16.41 | 5.14 | |
| Rural | 349 | 11.8 | 16.76 | 5.20 | |
| Total | 2940 | 99.0 | 16.78 | 5.23 | |
| Missing | 30 | 1.0 | |||
| Total | 2970 | 100.0 | |||
| Professional status | HP | 264 | 8.9 | 16.97 | 5.48 |
| WP | 422 | 14.2 | 16.61 | 5.56 | |
| Other | 2265 | 76.2 | 16.80 | 5.18 | |
| Missing | 19 | 0.6 | |||
| Total | 2970 | 100.0 |
Females reported a higher level of fear (MFCV-19 = 17.43, SD = 5.06) than males (MFCV-19 = 14.69, SD = 4.98) with statistical significance (t = − 12.63, df = 2878, p < .001). The elderly (MFCV-19 = 19.70, SD = 6.03) had the highest scores among the age categories (F4,2956 = 21.96, p < .001). Those with lower education (MFCV-19 = 20.50, SD = 5.61) reported a greater amount of fear (F5,2951 = 4.84, p < .001). No statistically significant differences were found between the means of FCV-19S among people living in different residential areas (p > .001) or between subjects who have a professional status that requires them to continue working despite the quarantine vs those who stayed at home (p > .001).
Reliability Analysis
A Cronbach’s alpha coefficient was calculated for the FCV-19S, consisting of FCV1, FCV2, FCV3, FCV4, FCV5, FCV6, and FCV7. The items for FCV-19S had a Cronbach’s alpha coefficient based on standardized items of .87. Item–total correlations and intra-correlations are presented in Table 2.
Table 2.
Item–total correlations and intra-correlations
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||
|---|---|---|---|---|---|---|---|---|---|
| FCV-19S | Pearson correlation | 1 | |||||||
| Sig. (2-tailed) | |||||||||
| N | 2970 | ||||||||
| FCV1 | Pearson correlation | 0.773** | 1 | ||||||
| Sig. (2-tailed) | 0.000 | ||||||||
| N | 2970 | 2970 | |||||||
| FCV2 | Pearson correlation | 0.768** | 0.689** | 1 | |||||
| Sig. (2-tailed) | 0.000 | 0.000 | |||||||
| N | 2970 | 2970 | 2970 | ||||||
| FCV3 | Pearson correlation | 0.679** | 0.419** | 0.399** | 1 | ||||
| Sig. (2-tailed) | 0.000 | 0.000 | 0.000 | ||||||
| N | 2970 | 2970 | 2970 | 2970 | |||||
| FCV4 | Pearson correlation | 0.776** | 0.567** | 0.517** | 0.468** | 1 | |||
| Sig. (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | |||||
| N | 2970 | 2970 | 2970 | 2970 | 2970 | ||||
| FCV5 | Pearson correlation | 0.724** | 0.452** | 0.505** | 0.365** | 0.420** | 1 | ||
| Sig. (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | ||||
| N | 2970 | 2970 | 2970 | 2970 | 2970 | 2970 | |||
| FCV6 | Pearson correlation | 0.756** | 0.454** | 0.425** | 0.562** | 0.538** | 0.441** | 1 | |
| Sig. (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |||
| N | 2970 | 2970 | 2970 | 2970 | 2970 | 2970 | 2970 | ||
| FCV7 | Pearson correlation | 0.802** | 0.487** | 0.473** | 0.522** | 0.568** | 0.513** | 0.688** | 1 |
| Sig. (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | ||
| N | 2970 | 2970 | 2970 | 2970 | 2970 | 2970 | 2970 | 2970 | |
**Correlation is significant at the 0.01 level (2-tailed)
Confirmatory Factor Analysis
A CFA model was conducted to determine whether the latent variable, FCV-19S, adequately describes the data. Maximum likelihood estimation was performed to determine the standard errors for the parameter estimates. To identify influential points in the data, Mahalanobis distances were calculated and compared with a χ2 distribution. There were 2 observations detected as outliers. There were no variables that had an R2 > 0.90. The value of the determinant for the correlation matrix was 0.25, indicating that there was no multicollinearity in the data.
First, the reliability of the analysis was tested based on the sample size used to construct the model. Next, the results were evaluated using the Chi-square goodness of fit test and fit indices. Lastly, the squared multiple correlations (R2) for each endogenous variable were determined. The results of the CFA model are presented in Table 3. The node diagram is shown in Fig. 1.
Fig. 1.
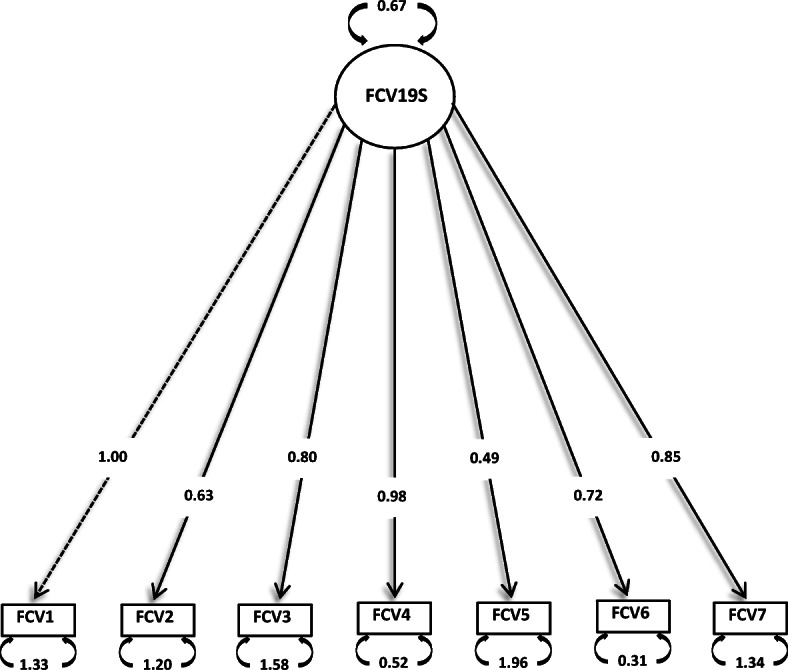
Node diagram for the CFA model
The RMSEA index was slightly greater than 0.10, RMSEA = 0.11, 90% CI = [0.10, 0.11], the CFI was 0.89, the TLI was 0.83 and the SRMR was between 0.05 and 0.08, and SRMR = 0.06, which implies that the model fits the data adequately.
The following observed variables had R2 values ≤ 0.20: FCV2 and FCV5. The R2 values, along with the error variances for each observed variable, are presented in Table 3. The resultant outcome indicated that the proposed model was a good fit.
Concurrent Validity
Concurrent validity was explored by correlating the FCV-19S score with the GAD-7 self-reported anxiety score, and the PHQ-9 depression scale. High statistically significant correlation was found between FCV-19S and GAD-7 (r = 0.71, p < .001) and moderate correlation was found between FCV-19S and PHQ-9 (r = 0.47, p < .001) demonstrating a good concurrent validity (Table 4).
Discussion
This study aimed to examine the psychometric properties of the Greek FCV-19S among a large sample of individuals. The Greek FCV-19S demonstrated satisfactory psychometric properties with good internal consistency (α = .87). The factor pattern in the Greek translation is comparable with the original version (Ahorsu et al. 2020) and previous validation findings in Italy, Bangladesh, and Turkey (Sakib et al. 2020; Satici et al. 2020; Soraci et al. 2020), yet with rather modest factor loadings. The fit to the model however supported the unidimensionality of the scale, which implies that the sum of the item scores represents the severity of the perceived fear: i.e., a higher score indicates a more severe state of fear. It is worth noting that in the Russian version, exploratory factor analysis yields two factors representing physiological and emotional responses, respectively.
There was a significant positive correlation between the Greek FCV-19S and general anxiety (as assessed by GAD-7) and depression (as assessed by PHQ-9), as expected and previously reported (Ahorsu et al. 2020; Sakib et al. 2020; Satici et al. 2020; Soraci et al. 2020). This further demonstrates a potential pattern of comorbidity when screening against COVID-19 fear, portraying levels of cumulative negative affect. However, risk perceptions (e.g., probability of death, exposure to the virus), resulting in maladaptive psychological responses, are strongly related to the evaluations of threats, which vary among individuals from different countries, ages, gender, etc. (Gerhold 2020).
Meanwhile, a recent research proposed that the perceived fear against COVID-19, assessed by the FCV-19S, functions mainly as a protective factor that leads to better adjustment against the pandemic and predicts compliance with the preventive measures (Harper et al. 2020). Hence, it is known that the main function of fear and anxiety is to trigger appropriate adaptive responses in order to maintain survival; as such, the impact of the perceived fear can be seen more accurately in the long term (Ornell et al. 2020). The use of the FCV-19S could offer a better insight regarding the fear of COVID-19 to address individuals at risk and advise them accordingly.
Further observations in this study demonstrated that women, the elderly (over the age of 75), and participants with lower education displayed elevated fear of COVID-19 in accordance with other relevant studies (Gerhold 2020; Ma-Kellams and Wu 2020; Wang et al. 2020). A review of the gender differences in fear and anxiety suggests that there is substantial evidence indicating that women report greater fear (McLean and Anderson 2009), probably due to a broad range of biological influences, environmental factors, and socialization processes. Older people report higher levels of fear, as their physical vulnerability along with social isolation creates a very stressful combination (Girdhar et al. 2020; Meng et al. 2020). Lastly, less educated people may be more afraid because they cannot understand the medical terminology used extensively in connection with the virus, and therefore feel more uncertain.
Limitations
This study was not without limitations. First, although anonymous surveys appear to encourage disclosure and self-reporting data is considered a valuable resource of information for constructs otherwise difficult to obtain, the potential impact of self-reporting bias (Althubaiti 2016) should be acknowledged. Second, in online surveys, there is always a possibility for self-selection bias (Bethlehem 2010), which may indicate an overrepresentation of specific subgroups within the general population. Additionally, the sample in the current study did not include teenagers and children, and some characteristics were found predominant as for example the female gender. Future work may further seek to examine additional psychometric properties, including different types of reliability, validity, and measurement equivalence targeting as well as clinical settings.
Conclusion
This study outlines the Greek translation and validation of the newly developed Iranian FCV-19S in a large sample of adults. Psychometric properties of the Greek version of the FCV-19S are good, in line with the original scale and the adaptations in other languages. The findings support the reliability and construct-related validity of the Greek FCV-19S for assessing fear of the novel coronavirus among Greek-speaking individuals.
Authors’ Contributions
Study planning: V. Holeva, Parlapani
Study plan validation: Z. Nasika, I. Diakogiannis
Project implementation: C. Varvara, E. Spyridopoulou
Data interpretation: E. Parlapani, V. Holeva
Data analysis: S. Sakka, S. Kostikidou
Writing the first draft: V. Tsipropoulou
Review and edit: V.A. Nikopoulou
Final approval: I. Diakogiannis
Data Availability
Data will be available on request.
Compliance with Ethical Standards
Ethical approval was granted from the PGH Review Board (no. 563/2020) and the study was conducted in accordance with the Declaration of Helsinki. The participation in the survey was entirely voluntary, anonymous, and confidential. All the respondents provided informed consent for their participation, data extraction, and publication of the results prior to their enrollment.
Disclaimer
The authors involved in this research communication do not have any relationships with other people or organizations that could inappropriately influence (bias) the findings.
Conflict of Interest
The authors declare that they have no conflict of interest.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Ahorsu, D. K., Lin, C. Y., Imani, V., Saffari, M., Griffiths, M. D., & Pakpour, A. H. (2020). The fear of COVID-19 scale: development and initial validation. International Journal of Mental Health and Addiction, 1–9. 10.1007/s11469-020-00270-8. [DOI] [PMC free article] [PubMed]
- Althubaiti A. Information bias in health research: definition, pitfalls, and adjustment methods. Journal of Multidisciplinary Healthcare. 2016;9:211–217. doi: 10.2147/JMDH.S104807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arbuckle JL. Amos (version 23.0) [computer program] Chicago: IBM SPSS; 2014. [Google Scholar]
- Bethlehem J. Selection bias in Web surveys. International Statistical Review. 2010;78(2):161–188. doi: 10.1111/j.1751-5823.2010.00112.x. [DOI] [Google Scholar]
- Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Frontiers in Public Health. 2018;6:149. doi: 10.3389/fpubh.2018.00149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gerhold, L. (2020). COVID-19: risk perception and coping strategies. 10.31234/osf.io/xmpk4.
- Girdhar R, Srivastava V, Sethi S. Managing mental health issues among elderly during COVID-19 pandemic. Journal of Geriatric Care and Research. 2020;7(1):29–32. [Google Scholar]
- Greek Minister of Health (2020). Press release on coronavirus COVID-19. Retrieved from https://www.moh.gov.gr/articles/ministry/grafeio-typoy/press-releases/7167-enhmerwsh-diapisteymenwn-syntaktwn-ygeias-apo-ton-yfypoyrgo-politikhs-prostasias-kai-diaxeirishs-krisewn-niko-xardalia-kai-ton-ekproswpo-toy-ypoyrgeioy-ygeias-gia-to-neo-koronoio-kathhghth-swthrh-tsiodra-12-5-2020.
- Harper, C. A., Satchell, L. P., Fido, D., & Latzman, R. D. (2020). Functional fear predicts public health compliance in the COVID-19 pandemic. International Journal of Mental Health and Addiction. 10.1007/s11469-020-00281-5. [DOI] [PMC free article] [PubMed]
- Kang L, Li Y, Hu S, Chen M, Yang C, Yang B. The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. The Lancet Psychiatry. 2020;7(3):E14. doi: 10.1016/S2215-0366(20)30047-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, Y. G., Moon, H., Kim, S. Y., Lee, Y. H., Jeong, D. W., Kim, K., ... & Park, H. C. (2019). Inevitable isolation and the change of stress markers in hemodialysis patients during the 2015 MERS-CoV outbreak in Korea. Scientific Reports, 9, 5676. 10.1038/s41598-019-41964-x. [DOI] [PMC free article] [PubMed]
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine. 2001;16(9):606–613. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ma-Kellams C, Wu MS. Gender, behavioral inhibition/activation, and emotional reactions to negative natural and social events. Personality and Individual Differences. 2020;157:109809. doi: 10.1016/j.paid.2019.109809. [DOI] [Google Scholar]
- Martin A, Rief W, Klaiberg A, Braehler E. Validity of the brief patient health questionnaire mood scale (PHQ-9) in the general population. General Hospital Psychiatry. 2006;28(1):71–77. doi: 10.1016/j.genhosppsych.2005.07.003. [DOI] [PubMed] [Google Scholar]
- McLean P, Anderson ER. Brave men and timid women? A review of the gender difference in fear and anxiety. Clinical Psychology Review. 2009;29(6):496–505. doi: 10.1016/j.cpr.2009.05.003. [DOI] [PubMed] [Google Scholar]
- Meng H, Xu Y, Dai J, Zhang Y, Liu B, Yang H. The psychological effect of COVID-19 on the elderly in China. Psychiatry Research. 2020;112983:112983. doi: 10.1016/j.psychres.2020.112983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mowbray, H. (2020). In Beijing, coronavirus 2019-nCoV has created a siege mentality. BMJ, 368. 10.1136/bmj.m516. [DOI] [PubMed]
- Ornell, F., Schuch, J. B., Sordi, A. O., & Kessler, F. H. P. (2020). “Pandemic fear” and COVID-19: mental health burden and strategies. Brazilian Journal of Psychiatry.10.1590/1516-4446-2020-0008. [DOI] [PMC free article] [PubMed]
- Pakpour, A. H., & Griffiths, M. D. (2020). The fear of CoVId-19 and its role in preventive behaviors. Journal of Concurrent Disorders. Advance online publication. https://concurrentdisorders.ca/2020/04/03/the-fear-of-covid-19-and-its-role-in-preventive-behaviors/.
- Reznik, A., Gritsenko, V., Konstantinov, V., Khamenka, N., & Isralowitz, R. (2020). COVID-19 fear in Eastern Europe: validation of the fear of COVID-19 scale. International Journal of Mental Health and Addiction. 10.1007/s11469-020-00283-3. [DOI] [PMC free article] [PubMed]
- Sakib, N., Mamun, M. A., Bhuiyan, A. I., Hossain, S., Al Mamun, F., Hosen, I., et al. (2020). Psychometric Validation of the Bangla Fear of COVID-19 Scale: confirmatory factor analysis and Rasch analysis. International Journal of Mental Health and Addiction. 10.1007/s11469-020-00289-x. [DOI] [PMC free article] [PubMed]
- Satici, B., Gocet-Tekin, E., Deniz, M. E., & Satici, A. S. (2020). Adaptation of the Fear of COVID-19 Scale: its association with psychological distress and life satisfaction in Turkey. International Journal of Mental Health Addiction. Advance online publication. 10.1007/s11469-020-00294-0. [DOI] [PMC free article] [PubMed]
- Shigemura J, Ursano RJ, Morganstein JC, Kurosawa M, Benedek DM. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: mental health consequences and target populations. Psychiatry and Clinical Neurosciences. 2020;74(4):281–282. doi: 10.1111/pcn.12988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soraci, P., Ferrari, A., Abbiati, F. A., Del Fante, E., De Pace, R., Urso, A., & Griffiths, M. D. (2020). Validation and psychometric evaluation of the Italian version of the Fear of COVID-19 Scale. International Journal of Mental Health and Addiction. 10.1007/s11469-020-00277-1. [DOI] [PMC free article] [PubMed]
- Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: a clear and user-friendly guideline. Journal of Evaluation in Clinical Practice. 2011;17(2):268–274. doi: 10.1111/j.1365-2753.2010.01434.x. [DOI] [PubMed] [Google Scholar]
- Spitzer RL, Kroenke K, Williams JB, Patient Health Questionnaire Primary Care Study Group Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Jama. 1999;282(18):1737–1744. doi: 10.1001/jama.282.18.1737. [DOI] [PubMed] [Google Scholar]
- Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives of Internal Medicine. 2006;166(10):1092–1097. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi Journal of Anaesthesia. 2017;11(5):80–89. doi: 10.4103/sja.SJA_203_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang C, Pan R, Wan X, Tan Y, Xu L, Ho CS, Ho RC. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. International Journal of Environmental Research and Public Health. 2020;17(5):1729. doi: 10.3390/ijerph17051729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization. (2009). Process of translation and adaptation of instruments. Retrieved May 12, 2020, from https://www.who.int/substance_abuse/research_tools/translation/en/.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data will be available on request.