

Abstract
Low-grade epilepsy-associated neuroepithelial tumors (LEATs) are responsible for drug-resistant chronic focal epilepsy, and are the second-most common reason for epilepsy surgery in children. LEATs are extremely responsive to surgical treatment, and therefore epilepsy surgery should be considered as a treatment option for LEATs. However, the optimal time for surgery remains controversial, and surgeries are often delayed. In this review, we reviewed published article on the factors associated with seizure and cognitive outcomes after epilepsy surgery for LEATs in children to help clinicians in their decision whether to pursue epilepsy surgery for LEATs. The achievement of gross total resection may be the most important prognostic factor for seizure freedom. A shorter duration of epilepsy, a younger age at surgery, and extended resection of temporal lobe tumors have also been suggested as favorable prognostic factors in terms of seizure control. Poor cognitive function in children with LEATs is associated with a longer duration of epilepsy and a younger age at seizure onset.
Keywords: Low-grade epilepsy-associated tumors, Epilepsy surgery, Prognosis, Cognition
Introduction
Low-grade epilepsy-associated neuroepithelial tumors (LEATs) are responsible for drug-resistant chronic focal epilepsy that presents with seizure onset during childhood or young adulthood [1]. LEATs comprise low-grade glial or glioneuronal tumors (GNTs) such as gangliogliomas (GGs), dysembryoplastic neuroepithelial tumors (DNTs), angiocentric astrocytomas, and isomorphic astrocytomas.
After leukemias, brain tumors are the most common tumors (20%–22%) in children [2]. Brain tumors are graded based on their histological appearance and molecular parameters. World Health Organization grades 1 and 2 are benign tumors, while grades 3 and 4 are malignant. Before biopsy or surgical resection, due to multiple and nonspecific clinical signs, tumor grade is mostly assumed based on analysis of tumor site and appearance on multiparametric magnetic resonance imaging (MRI) [3]. For example, a hemorrhagic tumor with peripheral edema containing multiple ectatic vessels or a hypercellular tumor that is iso- or hypointense compared to the cortex on T2-weighted imaging is more suggestive of high-grade tumors [3-5]. Seizure prevalence is higher in slow-growing benign brain tumors, and some suggested explanations include: (1) longer life expectancy of patients with low-grade tumors contributing to increased seizure frequency; (2) insufficient time for cells of high-grade tumors to reorganize, vascularize, and develop mechanisms necessary for epileptogenesis; and (3) slow-growing tumor cells may possess intrinsic epileptogenic properties [6-8].
As the propensity for malignant progression is very low in LEATs, seizure control may be the main treatment target. Unfortunately, there is a high incidence of drug-resistant seizures among LEAT patients; consequently, although LEATs account for only 2%–5% of all brain tumors and are the etiology of seizures in only 1%–3% of pediatric epilepsy patients, LEATs are the second-most common reason for epilepsy surgery in children [9-12]. In a European study of brain specimens from 9,523 patients who underwent epilepsy surgery, the histopathologic etiology was identified as a tumor in 24% of all patients. LEATs comprised 82% of the tumors, and 84% of the LEATs were GGs or DNTs (Table 1).
Table 1.
Histopathological classification of 1,846 low-grade epilepsy-associated neuroepithelial tumors obtained from patients undergoing epilepsy surgery [10]
| Tumor diagnosis | No. (%) | Age at seizure onset (yr) | Duration of epilepsy (yr) |
|---|---|---|---|
| GG | 986 (53.6) | 12.1±10.3 | 11.4±10.4 |
| DNT | 565 (30.6) | 14±10.9 | 12±10.7 |
| Pilocytic astrocytoma | 99 (5.4) | 14.1±9.9 | 12.3 ±11.4 |
| PXA | 43 (2.3) | 17.0±12.4 | 12.8±12.1 |
| Isomorphic astrocytoma | 17 (0.9) | 16.0±14.3 | 11.4±10.5 |
| Gangliocytoma | 16 (0.9) | 12.0±7.0 | 17.1±12.4 |
| Angiocentric glioma | 12 (0.7) | 7.7±4.8 | 6.9±6.0 |
| Low-grade tumor, not specified | 108 (5.9) | 14.6±13.2 | 11.5±10.1 |
Values are presented as number (%) or mean±standard devaition.
GG, ganglioglioma; DNT, dysembryoplastic neuroepithelial tumor; PXA, pleomorphic xanthoastrocytoma.
LEATs are extremely responsive to surgical treatment, and more than 80% of patients achieve seizure freedom after surgery [13-16]. Therefore, epilepsy surgery should be considered a treatment option for LEATs. However, the optimal surgical timing remains controversial, and surgeries are often delayed (Table 1), mostly due to late referral after lengthy trials of antiepileptic drugs (AEDs), with a mean duration from seizure onset to surgery (i.e., duration of epilepsy) of more than 10 years [10].
To help clinicians decide whether to pursue epilepsy surgery for LEATs, here we performed a systematic literature review of the factors associated with seizure and cognitive outcomes after epilepsy surgery for LEATs in children. Articles were extracted in July 2019 using PubMed searches of titles and abstracts with the following query terms: seizure or epilepsy; low-grade epilepsy-associated neuroepithelial tumor, long-term epilepsy-associated tumor, LEAT, ganglioglioma, dysembryoplastic neuroepithelial tumor, glioma, astrocytoma, xanthoastrocytoma, or tumor; surgery or resection; and child or pediatric. The inclusion criteria for the studies were: (1) epilepsy surgery in children with histopathologically confirmed LEATs, (2) seizure or epilepsy as the main symptom and reason for the surgery, and (3) mention of statistically significant predictive factors for seizure or cognitive outcomes. The exclusion criteria were: (1) inclusion of adults and children in the study and the reporting of data such that the child-specific data could not be distinguished from those for adults, (2) inclusion of high-grade tumors. Of 290 extracted articles, 86 were excluded after initial screening due to irrelevancy, while an additional 186 were excluded after full article review due to ineligibility. Ultimately, 18 studies were included; of them, 16 addressed factors associated with seizure outcome, and 6 addressed factors associated with cognitive outcome. All included studies were retrospective.
Epileptogenesis of LEATs
The reason why almost all GNTs, including GGs and DNTs, cause seizures is not entirely understood, and various epileptogenic mechanisms of LEAT-associated epilepsy have been suggested [17]. The LEAT itself can be intrinsically epileptogenic due to the presence of hyperexcitable dysplastic neurons or a high neuronal density within the tumor as evidenced by various results from immunocytochemical studies, such as the high expression of glutamate receptor subtypes, downregulation of several gamma-aminobutyric acid (GABA) receptors, and deregulation of cation-chloride cotransporters [18-22].
LEATs can also invade normal tissues, altering neurotransmitter expression and inflammatory reactions [23]. For example, the deregulation of glutamate uptake and release by glutamate receptors on glial cells, which results in increased extracellular glutamate concentrations and decreased glial glutamate transporter expressions, has been observed [19,20,24,25]. LEATs have also been noted to activate the innate and adaptive immune systems [26,27]. Proinflammatory molecules increase neuronal excitability by enhancing extracellular glutamate concentrations and modifying the functions of glutamate and GABA receptors [28]. Immune system activation also causes upregulation of major histocompatibility complex class I molecules in neuronal cells and activates the mammalian target of rapamycin pathway [26,27,29].
Adjacent cortical areas can also undergo dysplastic reorganization, leading to hyperexcitability [30,31]. Studies have shown that the afferentiation of adjacent cortical regions can lead to denervation hypersensitivity, modified synchronization of local networks, and overexpression of neurotransmitters in adjacent cortical areas [7,23,32].
Other suggested mechanisms for LEAT-related seizures include blood-brain barrier dysfunction, altered gap junction channels in glial cells, alterations in the surrounding neuronal network, altered regional metabolism and pH, regional hypoxic effects on the surrounding tissue, and an altered vascular supply [7,18,33-39]. Genetic predispositions for tumor-associated seizures have also been studied [7,40]. Therefore, the etiology of tumor-induced seizures is multifactorial and extends beyond the physical size of the tumor itself [41,42].
Factors associated with seizure outcomes after epilepsy surgery for LEATs
The following factors were mentioned at least once among the 16 studies that addressed seizure outcome as being predictive of seizure recurrence after surgery: younger age at seizure onset [43]; older age at surgery [44,45]; longer duration of epilepsy [44,46]; greater number of AEDs taken at the time of surgery [47]; presence of generalized seizure [48]; presence of generalized epileptiform discharges (EDs) in an electroencephalogram [49]; extratemporal or parietal location of the tumor [45]; presence of satellite lesions on a MRI scan [50]; lesionectomy of temporal tumors [43]; and subtotal tumor resection [15,45,46,51-55]. The included studies that examined seizure outcome are summarized in Table 2, and more detailed information regarding the tumor types included, parameters for seizure outcome assessment, and factors irrelevant to seizure outcome are shown in Supplementary Table 1.
Table 2.
Summary of articles addressing factors associated with seizure outcomes after epilepsy surgery for low-grade epilepsy-associated neuroepithelial tumors
| Study | No. of patients | Seizure-free rate | Factors associated with poor seizure outcome |
|---|---|---|---|
| Babini et al. (2013) [43] | 30 | 86.7% | Younger age at seizure onset |
| Tailored surgery (i.e., extended resection for epileptogenic foci) for temporal lobe tumors | |||
| Brahimaj et al. (2014) [47] | 18 | 44.4% | Greater number of AEDs tried before surgery |
| Daszkiewicz et al. (2018) [44] | 52 | 86.5% | Age of >6 yr at surgery |
| Duration of epilepsy >1 yr | |||
| Ehrstedt et al. (2017) [51] | 25 | 64.0% | Subtotal resection |
| Faramand et al. (2018) [15] | 92 | 80.4% | Subtotal resection |
| Garc a-Fern ndez et al. (2011) [52] | 21 | 85.7% | Subtotal resection |
| Khajavi et al. (1995) [53] | 15 | 66.7% | Subtotal resection |
| Khajavi et al. (1999) [46] | 34 | 73.5% | Older age at surgery |
| Subtotal resection | |||
| Ko et al. (2019) [54] | 58 | 87.9% | Subtotal resection |
| Minkin et al. (2008) [48] | 24 | 83.3% | Presence of generalized seizure |
| Nolan et al. (2004) [72] | 26 | 84.6% | Subtotal resection |
| Ogiwara et al. (2010) [66] | 30 | 90.0% | None |
| Packer et al. (1994) [45] | 50 | 72.0% | Parietal location of tumor |
| Subtotal resection | |||
| Duration of epilepsy >1 yr | |||
| Ramantani et al. (2014) [55] | 29 | 75.9% | Subtotal resection |
| Uliel-Sibony et al. (2011) [49] | 41 | 82.9% | Presence of generalized EDs in an EEG |
| Yang et al. (2019) [50] | 39 | 66.7% | Presence of satellite lesions on an MRI scan |
AED, antiepileptic drug; ED, epileptiform discharge; EEG, electroencephalogram; MRI, magnetic resonance imaging.
Degree of tumor resection
Gross total resection was the most frequently suggested favorable prognostic factor [15,45,46,49-55]. Fig. 1 shows an example of successful gross total resection of a LEAT (ganglioglioma) in a 7-year-old boy performed due to uncontrolled seizures after he took 3 AEDs for 1.3 years. Several studies that included large numbers of patients confirmed that gross total resection is among the strongest factors leading to seizure freedom after LEAT resection [41,56-58]. However, some studies have stated otherwise [49,50,59,60]. Gross total resection may not be possible if the tumor is located adjacent to eloquent areas or other functional cortical areas. Nevertheless, gross total resection should be the goal of surgery, and efforts should be made using multimodal approaches to maximize the extent of resection.
Fig. 1.
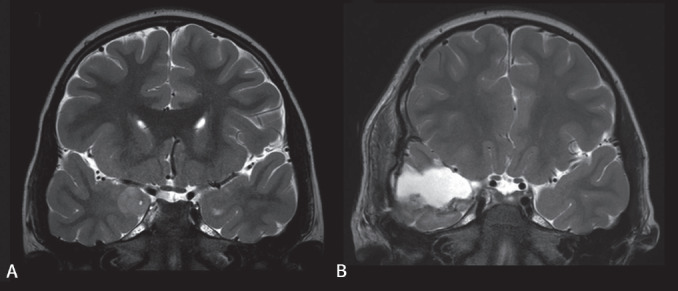
Brain magnetic resonance image of a patient with a low-grade epilepsy-associated neuroepithelial tumor (ganglioglioma) before (A) and after (B) gross total resection.
Duration of epilepsy
Two studies mentioned that a longer duration of epilepsy was a poor prognostic factor for seizure outcomes [44,45]. The same has been demonstrated in previous systematic reviews that examined adults or both adults and children [56,57,61]. Early seizures may promote progressive changes in synaptic plasticity and cerebral blood flow, with prolonged epilepsy making surrounding neurons more epileptic; thus, seizure control can become more difficult once a period of time has elapsed following seizure onset [56,62-65]. However, 8 studies found that epilepsy duration is not predictive of seizure outcome [15,43,46,49-52,55], while 2 studies suggested otherwise. Thus, more studies are needed to draw a definitive conclusion.
Age at surgery
Two studies found that an older age at surgery is predictive for persistent seizures [44,46], whereas 9 studies found no association between age at surgery and seizure outcome [15,43,45,47,48,50,52, 54,55,66]. In an Italian nationwide study of epilepsy surgery for LEATs that included a total of 282 adults and children, older age at surgery was the most significant predictor of persistent seizures, with a 4% increase in the probability of an unfavorable outcome for every year waited [16]. Since previous studies demonstrated no significant difference in surgical outcome between pediatric and adult patients with LEATs [16,56], the reason for the poor prognosis associated with older age at surgery may be the duration of epilepsy rather than the patient’s age itself.
Extent of resection
One article suggested that extended resection (i.e., removal of the tumor and surrounding epileptogenic zone) is helpful for achieving seizure freedom [43], whereas 6 other articles found no difference in seizure outcomes between lesionectomy alone and extended resection [46,47,49,52,53,66]. Thus, the matter of surgical strategy remains controversial. The discordance among previous studies also raises an important question regarding the use of additional corticectomy or additional amygdalohippocampectomy for temporal lobe tumors [14,16,23,56,60,67-69]. Extended resections are mainly performed for temporal tumors, while there is a lack of reports detailing outcomes for extratemporal tumors [43,67,69-71]. One indicator that endorses the application of extended tailored resection is the presence of adjacent dual pathology, such as focal cortical dysplasia or hippocampal sclerosis, that can cause seizures after lesionectomy [56]. Therefore, what can currently be said with confidence is that extended resection may be considered, particularly when treating temporal tumors with evidence of dual pathology [56].
Utilization of intraoperative electrocorticography
Intraoperative electrocorticography (ECoG) or 2-stage surgery is performed when delineation of the epileptogenic zone is needed due to the presence of multifocal epileptogenic foci or a tumor location adjacent to functional areas. All 3 studies that investigated the association between the utilization of intraoperative ECoG and seizure outcome found that it is not related to higher rates of seizure freedom [49,66,72]. Other large reviews reported the same conclusion. However, caution must be taken when interpreting these results, as intraoperative ECoG is more likely to be used in more difficult cases that involve multifocal epileptogenic foci or tumors located near eloquent areas [56,57]. Other studies advocate for the utilization of intraoperative ECoG during tailored surgery [73-76]. Therefore, the use of intraoperative ECoG is advised when extended resection is anticipated [73].
Factors associated with cognitive outcome after epilepsy surgery for LEATs
Studies that addressed factors associated with preoperative full-scale intelligence quotient (FSIQ), longer duration of epilepsy, and younger age at seizure onset are universally mentioned as poor prognostic factors for preoperative FSIQ [15,16,52,54,55]. An explanation of this finding is reduced brain plasticity and a limited degree of possible postoperative cognitive gains [77,78]. The studies addressing cognitive outcome are summarized in Table 3, and more detailed information regarding the cognitive parameters is shown in Supplementary Table 2.
Table 3.
Summary of articles addressing factors associated with cognitive outcomes after epilepsy surgery for low-grade epilepsy-associated neuroepithelial tumors
| Study | No. of patients | Parameters | Value | Factors associated with poor cognitive outcome |
|---|---|---|---|---|
| Faramand et al. (2018) [15] | 22 | Postoperative FSIQ | Seizure-free (n=14): 92.4 (range, 73–116) | Younger age at seizure onset |
| Low seizure severity (n=5): 105.0 (range, 71–126) | Persistent seizure after surgery | |||
| High seizure severity (n=3): 75.3 (range, 70–80) | High seizure severity after surgery | |||
| Faramand et al. (2018) [15] | 90 | Preoperative FSIQ | 81 (IQR, 71–95) | Younger age at seizure onset |
| Longer duration of epilepsy | ||||
| 41 | Postoperative FSIQ | 86 (IQR, 71–100) | Low preoperative FSIQ | |
| García-Fernández et al. (2011) [52] | 21 | Preoperative FSIQ | 85.2±21.9 | Younger age at seizure onset |
| Drug-resistant epilepsy before surgery | ||||
| Postoperative FSIQ | 88.6±17.7 | None | ||
| Giulioni et al. (2017) [16] | Unknown | Preoperative NP test | Normal vs. pathologic (deficit) | Longer duration of epilepsy |
| Ko et al. (2019) [54] | 58 | Preoperative FSIQ | 78.9±27.1 | Longer duration of epilepsy |
| 42 | Postoperative FSIQ | 80.9±28.7 | Low preoperative FSIQ | |
| Ramantani et al. (2014) [55] | 25 | Preoperative FSIQ | 93.0±21.8 | Longer duration of epilepsy |
| Preoperative VIQ | 95.9±13.8 | Longer duration of epilepsy | ||
| Preoperative PIQ | 101.2±15.5 | Younger age at seizure onset | ||
| 24 | Postoperative FSIQ | 91.7±21.6 | Low preoperative FSIQ |
Values are presented as mean (range), median (interquartile range), or mean±standard deviation.
FSIQ, full-scale intelligence quotient; NP, neuropsychological; VIQ, verbal intelligence quotient; PIQ, performance intelligence quotient.
Postoperative cognitive function has been shown to significantly depend on preoperative cognitive function [15,54,55]. García-Fernández et al. [52]. reported that none of the various cognitive domains of a postoperative neuropsychological test performed 1 year after resection showed significant decline; on the contrary, there were statistically significant improvements in several cognitive domains (Supplementary Table 2). Ramantani et al. [55]. also reported that, at the group level, there was significant intraindividual improvement in verbal intelligence quotient (IQ) and performance IQ as well as a trend toward FSIQ improvement after epilepsy surgery. Finally, a study by Faramand et al. [15]. showed that postoperative FSIQ improved in 61% of children, declined in 36.5% of children, and was unchanged in 2.5% of children. The study by García-Fernández et al. [52]. mentioned above also showed poorer preoperative cognitive function in children with drug-resistant epilepsy, suggesting that it can be beneficial for surgery to occur before drug-resistant epilepsy develops.
Overall, earlier surgery can prevent low postoperative FSIQ in children, particularly young children, and that improved cognitive function can be expected following epilepsy surgery.
Conclusion
LEATs usually develop in children and young adults who present with seizures that are highly drug-resistant. Surgical treatment, however, is extremely effective, resulting in seizure freedom in approximately 70%–80% of cases. The achievement of gross total resection may be the most important prognostic factor for seizure freedom. Shorter duration of epilepsy, younger age at surgery, and extended resection of temporal lobe tumors have also been suggested as favorable prognostic factors for seizure control.
Poor cognitive function in children with LEATs is strongly associated with longer duration of epilepsy and younger age at seizure onset. Therefore, surgical treatment should be considered as an early option in children with LEATs prior to the diagnosis of drug-resistant epilepsy to protect the cognitive function of LEAT patients by averting recurrent seizures and the administration of multiple AEDs.
Footnotes
No potential conflict of interest relevant to this article was reported.
Supplementary materials
Supplementary Tables 1 and 2 can be found via https://doi.org/10.3345/kjp.2019.01151.
Detailed summary of literatures on factors associated with seizure outcome in epilepsy surgery of low-grade epilepsy-associated neuroepithelial tumors
Detailed summary of literatures on factors associated with cognitive outcome in epilepsy surgery of low-grade epilepsy-associated neuroepithelial tumors
References
- 1.Holthausen H, Blümcke I. Epilepsy-associated tumours: what epileptologists should know about neuropathology, terminology, and classification systems. Epileptic Disord. 2016;18:240–51. doi: 10.1684/epd.2016.0851. [DOI] [PubMed] [Google Scholar]
- 2.Bauchet L, Rigau V, Mathieu-Daudé H, Fabbro-Peray P, Palenzuela G, Figarella-Branger D, et al. Clinical epidemiology for childhood primary central nervous system tumors. J Neurooncol. 2009;92:87–98. doi: 10.1007/s11060-008-9740-0. [DOI] [PubMed] [Google Scholar]
- 3.Koob M, Girard N. Cerebral tumors: specific features in children. Diagn Interv Imaging. 2014;95:965–83. doi: 10.1016/j.diii.2014.06.017. [DOI] [PubMed] [Google Scholar]
- 4.Porto L, Jurcoane A, Schwabe D, Hattingen E. Conventional magnetic resonance imaging in the differentiation between high and low-grade brain tumours in paediatric patients. Eur J Paediatr Neurol. 2014;18:25–9. doi: 10.1016/j.ejpn.2013.07.004. [DOI] [PubMed] [Google Scholar]
- 5.Forbes JA, Chambless LB, Smith JG, Wushensky CA, Lebow RL, Alvarez J, et al. Use of T2 signal intensity of cerebellar neoplasms in pediatric patients to guide preoperative staging of the neuraxis. J Neurosurg Pediatr. 2011;7:165–74. doi: 10.3171/2010.11.PEDS10312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chen DY, Chen CC, Crawford JR, Wang SG. Tumor-related epilepsy: epidemiology, pathogenesis and management. J Neurooncol. 2018;139:13–21. doi: 10.1007/s11060-018-2862-0. [DOI] [PubMed] [Google Scholar]
- 7.van Breemen MS, Wilms EB, Vecht CJ. Epilepsy in patients with brain tumours: epidemiology, mechanisms, and management. Lancet Neurol. 2007;6:421–30. doi: 10.1016/S1474-4422(07)70103-5. [DOI] [PubMed] [Google Scholar]
- 8.Hildebrand J, Lecaille C, Perennes J, Delattre JY. Epileptic seizures during follow-up of patients treated for primary brain tumors. Neurology. 2005;65:212–5. doi: 10.1212/01.wnl.0000168903.09277.8f. [DOI] [PubMed] [Google Scholar]
- 9.Harvey AS, Cross JH, Shinnar S, Mathern GW, ILAE Pediatric Epilepsy Surgery Survey Taskforce Defining the spectrum of international practice in pediatric epilepsy surgery patients. Epilepsia. 2008;49:146–55. doi: 10.1111/j.1528-1167.2007.01421.x. [DOI] [PubMed] [Google Scholar]
- 10.Blumcke I, Spreafico R, Haaker G, Coras R, Kobow K, Bien CG, et al. Histopathological findings in brain tissue obtained during epilepsy surgery. N Engl J Med. 2017;377:1648–56. doi: 10.1056/NEJMoa1703784. [DOI] [PubMed] [Google Scholar]
- 11.Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, et al. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–30. doi: 10.3322/canjclin.56.2.106. [DOI] [PubMed] [Google Scholar]
- 12.Ullrich NJ, Pomeroy SL, Kapur K, Manley PE, Goumnerova LC, Loddenkemper T. Incidence, risk factors, and longitudinal outcome of seizures in long-term survivors of pediatric brain tumors. Epilepsia. 2015;56:1599–604. doi: 10.1111/epi.13112. [DOI] [PubMed] [Google Scholar]
- 13.Chan CH, Bittar RG, Davis GA, Kalnins RM, Fabinyi GC. Long-term seizure outcome following surgery for dysembryoplastic neuroepithelial tumor. J Neurosurg. 2006;104:62–9. doi: 10.3171/jns.2006.104.1.62. [DOI] [PubMed] [Google Scholar]
- 14.Giulioni M, Gardella E, Rubboli G, Roncaroli F, Zucchelli M, Bernardi B, et al. Lesionectomy in epileptogenic gangliogliomas: seizure outcome and surgical results. J Clin Neurosci. 2006;13:529–35. doi: 10.1016/j.jocn.2005.07.017. [DOI] [PubMed] [Google Scholar]
- 15.Faramand AM, Barnes N, Harrison S, Gunny R, Jacques T, Tahir MZ, et al. Seizure and cognitive outcomes after resection of glioneuronal tumors in children. Epilepsia. 2018;59:170–8. doi: 10.1111/epi.13961. [DOI] [PubMed] [Google Scholar]
- 16.Giulioni M, Marucci G, Pelliccia V, Gozzo F, Barba C, Didato G, et al. Epilepsy surgery of "low grade epilepsy associated neuroepithelial tumors": a retrospective nationwide Italian study. Epilepsia. 2017;58:1832–41. doi: 10.1111/epi.13866. [DOI] [PubMed] [Google Scholar]
- 17.Aronica E, Crino PB. Epilepsy related to developmental tumors and malformations of cortical development. Neurotherapeutics. 2014;11:251–68. doi: 10.1007/s13311-013-0251-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wolf HK, Birkholz T, Wellmer J, Blümcke I, Pietsch T, Wiestler OD. Neurochemical profile of glioneuronal lesions from patients with pharmacoresistant focal epilepsies. J Neuropathol Exp Neurol. 1995;54:689–97. doi: 10.1097/00005072-199509000-00011. [DOI] [PubMed] [Google Scholar]
- 19.Wolf HK, Buslei R, Blümcke I, Wiestler OD, Pietsch T. Neural antigens in oligodendrogliomas and dysembryoplastic neuroepithelial tumors. Acta Neuropathol. 1997;94:436–43. doi: 10.1007/s004010050730. [DOI] [PubMed] [Google Scholar]
- 20.Aronica E, Yankaya B, Jansen GH, Leenstra S, van Veelen CW, Gorter JA, et al. Ionotropic and metabotropic glutamate receptor protein expression in glioneuronal tumours from patients with intractable epilepsy. Neuropathol Appl Neurobiol. 2001;27:223–37. doi: 10.1046/j.0305-1846.2001.00314.x. [DOI] [PubMed] [Google Scholar]
- 21.Fassunke J, Majores M, Tresch A, Niehusmann P, Grote A, Schoch S, et al. Array analysis of epilepsy-associated gangliogliomas reveals expression patterns related to aberrant development of neuronal precursors. Brain. 2008;131(Pt 11):3034–50. doi: 10.1093/brain/awn233. [DOI] [PubMed] [Google Scholar]
- 22.Aronica E, Boer K, Redeker S, Spliet WG, van Rijen PC, Troost D, et al. Differential expression patterns of chloride transporters, Na+-K+-2Cl--cotransporter and K+-Cl--cotransporter, in epilepsy-associated malformations of cortical development. Neuroscience. 2007;145:185–96. doi: 10.1016/j.neuroscience.2006.11.041. [DOI] [PubMed] [Google Scholar]
- 23.Zaghloul KA, Schramm J. Surgical management of glioneuronal tumors with drug-resistant epilepsy. Acta Neurochir (Wien) 2011;153:1551–9. doi: 10.1007/s00701-011-1050-1. [DOI] [PubMed] [Google Scholar]
- 24.Seifert G, Carmignoto G, Steinhäuser C. Astrocyte dysfunction in epilepsy. Brain Res Rev. 2010;63:212–21. doi: 10.1016/j.brainresrev.2009.10.004. [DOI] [PubMed] [Google Scholar]
- 25.Ye ZC, Rothstein JD, Sontheimer H. Compromised glutamate transport in human glioma cells: reduction-mislocalization of sodium-dependent glutamate transporters and enhanced activity of cystine-glutamate exchange. J Neurosci. 1999;19:10767–77. doi: 10.1523/JNEUROSCI.19-24-10767.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Aronica E, Gorter JA, Redeker S, Ramkema M, Spliet WG, van Rijen PC, et al. Distribution, characterization and clinical significance of microglia in glioneuronal tumours from patients with chronic intractable epilepsy. Neuropathol Appl Neurobiol. 2005;31:280–91. doi: 10.1111/j.1365-2990.2004.00636.x. [DOI] [PubMed] [Google Scholar]
- 27.Prabowo AS, Iyer AM, Anink JJ, Spliet WG, van Rijen PC, Aronica E. Differential expression of major histocompatibility complex class I in developmental glioneuronal lesions. J Neuroinflammation. 2013;10:12. doi: 10.1186/1742-2094-10-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Vezzani A, French J, Bartfai T, Baram TZ. The role of inflammation in epilepsy. Nat Rev Neurol. 2011;7:31–40. doi: 10.1038/nrneurol.2010.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Boer K, Troost D, Timmermans W, van Rijen PC, Spliet WG, Aronica E. Pi3K-mTOR signaling and AMOG expression in epilepsy-associated glioneuronal tumors. Brain Pathol. 2010;20:234–44. doi: 10.1111/j.1750-3639.2009.00268.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rajneesh KF, Binder DK. Tumor-associated epilepsy. Neurosurg Focus. 2009;27:E4. doi: 10.3171/2009.5.FOCUS09101. [DOI] [PubMed] [Google Scholar]
- 31.Rudà R, Trevisan E, Soffietti R. Epilepsy and brain tumors. Curr Opin Oncol. 2010;22:611–20. doi: 10.1097/CCO.0b013e32833de99d. [DOI] [PubMed] [Google Scholar]
- 32.Bartolomei F, Bosma I, Klein M, Baayen JC, Reijneveld JC, Postma TJ, et al. How do brain tumors alter functional connectivity? A magnetoencephalography study. Ann Neurol. 2006;59:128–38. doi: 10.1002/ana.20710. [DOI] [PubMed] [Google Scholar]
- 33.Steinhäuser C, Seifert G. Glial membrane channels and receptors in epilepsy: impact for generation and spread of seizure activity. Eur J Pharmacol. 2002;447:227–37. doi: 10.1016/s0014-2999(02)01846-0. [DOI] [PubMed] [Google Scholar]
- 34.Aronica E, Gorter JA, Jansen GH, Leenstra S, Yankaya B, Troost D. Expression of connexin 43 and connexin 32 gap-junction proteins in epilepsy-associated brain tumors and in the perilesional epileptic cortex. Acta Neuropathol. 2001;101:449–59. doi: 10.1007/s004010000305. [DOI] [PubMed] [Google Scholar]
- 35.Schmitz AK, Grote A, Raabe A, Urbach H, Friedman A, von Lehe M, et al. Albumin storage in neoplastic astroglial elements of gangliogliomas. Seizure. 2013;22:144–50. doi: 10.1016/j.seizure.2012.10.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Alkonyi B, Mittal S, Zitron I, Chugani DC, Kupsky WJ, Muzik O, et al. Increased tryptophan transport in epileptogenic dysembryoplastic neuroepithelial tumors. J Neurooncol. 2012;107:365–72. doi: 10.1007/s11060-011-0750-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Calatozzolo C, Pollo B, Botturi A, Dinapoli L, Carosi M, Salmaggi A, et al. Multidrug resistance proteins expression in glioma patients with epilepsy. J Neurooncol. 2012;110:129–35. doi: 10.1007/s11060-012-0946-9. [DOI] [PubMed] [Google Scholar]
- 38.You G, Sha Z, Jiang T. The pathogenesis of tumor-related epilepsy and its implications for clinical treatment. Seizure. 2012;21:153–9. doi: 10.1016/j.seizure.2011.12.016. [DOI] [PubMed] [Google Scholar]
- 39.Shamji MF, Fric-Shamji EC, Benoit BG. Brain tumors and epilepsy: pathophysiology of peritumoral changes. Neurosurg Rev. 2009;32:275–84. doi: 10.1007/s10143-009-0191-7. [DOI] [PubMed] [Google Scholar]
- 40.Berntsson SG, Malmer B, Bondy ML, Qu M, Smits A. Tumor-associated epilepsy and glioma: are there common genetic pathways? Acta Oncol. 2009;48:955–63. doi: 10.1080/02841860903104145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ranger A, Diosy D. Seizures in children with dysembryoplastic neuroepithelial tumors of the brain--A review of surgical outcomes across several studies. Childs Nerv Syst. 2015;31:847–55. doi: 10.1007/s00381-015-2675-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Lee JW, Wen PY, Hurwitz S, Black P, Kesari S, Drappatz J, et al. Morphological characteristics of brain tumors causing seizures. Arch Neurol. 2010;67:336–42. doi: 10.1001/archneurol.2010.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Babini M, Giulioni M, Galassi E, Marucci G, Martinoni M, Rubboli G, et al. Seizure outcome of surgical treatment of focal epilepsy associated with low-grade tumors in children. J Neurosurg Pediatr. 2013;11:214–23. doi: 10.3171/2012.11.PEDS12137. [DOI] [PubMed] [Google Scholar]
- 44.Daszkiewicz P, Kowalczyk P, Roszkowski M. Surgical treatment of neuronal-glial tumors of mesial-basal part of temporal lobe: Long term outcome and control of epilepsy in pediatric patients. Neurol Neurochir Pol. 2018;52:2–8. doi: 10.1016/j.pjnns.2017.04.001. [DOI] [PubMed] [Google Scholar]
- 45.Packer RJ, Sutton LN, Patel KM, Duhaime AC, Schiff S, Weinstein SR, et al. Seizure control following tumor surgery for childhood cortical low-grade gliomas. J Neurosurg. 1994;80:998–1003. doi: 10.3171/jns.1994.80.6.0998. [DOI] [PubMed] [Google Scholar]
- 46.Khajavi K, Comair YG, Wyllie E, Palmer J, Morris HH, Hahn JF. Surgical management of pediatric tumor-associated epilepsy. J Child Neurol. 1999;14:15–25. doi: 10.1177/088307389901400102. [DOI] [PubMed] [Google Scholar]
- 47.Brahimaj B, Greiner HM, Leach JL, Horn PS, Stevenson CB, Miles L, et al. The surgical management of pediatric brain tumors causing epilepsy: consideration of the epileptogenic zone. Childs Nerv Syst. 2014;30:1383–91. doi: 10.1007/s00381-014-2427-2. [DOI] [PubMed] [Google Scholar]
- 48.Minkin K, Klein O, Mancini J, Lena G. Surgical strategies and seizure control in pediatric patients with dysembryoplastic neuroepithelial tumors: a single-institution experience. J Neurosurg Pediatr. 2008;1:206–10. doi: 10.3171/PED/2008/1/3/206. [DOI] [PubMed] [Google Scholar]
- 49.Uliel-Sibony S, Kramer U, Fried I, Fattal-Valevski A, Constantini S. Pediatric temporal low-grade glial tumors: epilepsy outcome following resection in 48 children. Childs Nerv Syst. 2011;27:1413–8. doi: 10.1007/s00381-011-1454-5. [DOI] [PubMed] [Google Scholar]
- 50.Yang J, Kim SK, Kim KJ, Chae JH, Lim BC, Wang KC, et al. Satellite lesions of DNET: implications for seizure and tumor control after resection. J Neurooncol. 2019;143:437–45. doi: 10.1007/s11060-019-03174-3. [DOI] [PubMed] [Google Scholar]
- 51.Ehrstedt C, Moreira NC, Casar-Borota O, Strömberg B, Ahlsten G. Glioneuronal tumors in childhood - Before and after surgery. A long-term follow-up study. Epilepsy Behav. 2017;72:82–8. doi: 10.1016/j.yebeh.2017.02.012. [DOI] [PubMed] [Google Scholar]
- 52.García-Fernández M, Fournier-Del Castillo C, Ugalde-Canitrot A, Pérez-Jiménez Á, Álvarez-Linera J, De Prada-Vicente I, et al. Epilepsy surgery in children with developmental tumours. Seizure. 2011;20:616–27. doi: 10.1016/j.seizure.2011.06.003. [DOI] [PubMed] [Google Scholar]
- 53.Khajavi K, Comair YG, Prayson RA, Wyllie E, Palmer J, Estes ML, et al. Childhood ganglioglioma and medically intractable epilepsy. A clinicopathological study of 15 patients and a review of the literature. Pediatr Neurosurg. 1995;22:181–8. doi: 10.1159/000120899. [DOI] [PubMed] [Google Scholar]
- 54.Ko A, Kim SH, Kim SH, Park EK, Shim KW, Kang HC, et al. Epilepsy surgery for children with low-grade epilepsy-associated tumors: factors associated with seizure recurrence and cognitive function. Pediatr Neurol. 2019;91:50–6. doi: 10.1016/j.pediatrneurol.2018.10.008. [DOI] [PubMed] [Google Scholar]
- 55.Ramantani G, Kadish NE, Anastasopoulos C, Brandt A, Wagner K, Strobl K, et al. Epilepsy surgery for glioneuronal tumors in childhood: avoid loss of time. Neurosurgery. 2014;74:648–57. doi: 10.1227/NEU.0000000000000327. [DOI] [PubMed] [Google Scholar]
- 56.Englot DJ, Berger MS, Barbaro NM, Chang EF. Factors associated with seizure freedom in the surgical resection of glioneuronal tumors. Epilepsia. 2012;53:51–7. doi: 10.1111/j.1528-1167.2011.03269.x. [DOI] [PubMed] [Google Scholar]
- 57.Englot DJ, Berger MS, Barbaro NM, Chang EF. Predictors of seizure freedom after resection of supratentorial low-grade gliomas. A review. J Neurosurg. 2011;115:240–4. doi: 10.3171/2011.3.JNS1153. [DOI] [PubMed] [Google Scholar]
- 58.Southwell DG, Garcia PA, Berger MS, Barbaro NM, Chang EF. Long-term seizure control outcomes after resection of gangliogliomas. Neurosurgery. 2012;70:1406–13. doi: 10.1227/NEU.0b013e3182500a4c. [DOI] [PubMed] [Google Scholar]
- 59.Kirkpatrick PJ, Honavar M, Janota I, Polkey CE. Control of temporal lobe epilepsy following en bloc resection of low-grade tumors. J Neurosurg. 1993;78:19–25. doi: 10.3171/jns.1993.78.1.0019. [DOI] [PubMed] [Google Scholar]
- 60.Blümcke I, Wiestler OD. Gangliogliomas: an intriguing tumor entity associated with focal epilepsies. J Neuropathol Exp Neurol. 2002;61:575–84. doi: 10.1093/jnen/61.7.575. [DOI] [PubMed] [Google Scholar]
- 61.Yang I, Chang EF, Han SJ, Barry JJ, Fang S, Tihan T, et al. Early surgical intervention in adult patients with ganglioglioma is associated with improved clinical seizure outcomes. J Clin Neurosci. 2011;18:29–33. doi: 10.1016/j.jocn.2010.05.002. [DOI] [PubMed] [Google Scholar]
- 62.Blume WT. The progression of epilepsy. Epilepsia. 2006;47 Suppl 1:71–8. doi: 10.1111/j.1528-1167.2006.00665.x. [DOI] [PubMed] [Google Scholar]
- 63.Breier JI, Mullani NA, Thomas AB, Wheless JW, Plenger PM, Gould KL, et al. Effects of duration of epilepsy on the uncoupling of metabolism and blood flow in complex partial seizures. Neurology. 1997;48:1047–53. doi: 10.1212/wnl.48.4.1047. [DOI] [PubMed] [Google Scholar]
- 64.Ben-Ari Y, Dudek FE. Primary and secondary mechanisms of epileptogenesis in the temporal lobe: there is a before and an after. Epilepsy Curr. 2010;10:118–25. doi: 10.1111/j.1535-7511.2010.01376.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Hauser WA, Lee JR. Do seizures beget seizures? Prog Brain Res. 2002;135:215–9. doi: 10.1016/s0079-6123(02)35021-0. [DOI] [PubMed] [Google Scholar]
- 66.Ogiwara H, Nordli DR, DiPatri AJ, Alden TD, Bowman RM, Tomita T. Pediatric epileptogenic gangliogliomas: seizure outcome and surgical results. J Neurosurg Pediatr. 2010;5:271–6. doi: 10.3171/2009.10.PEDS09372. [DOI] [PubMed] [Google Scholar]
- 67.Giulioni M, Rubboli G, Marucci G, Martinoni M, Volpi L, Michelucci R, et al. Seizure outcome of epilepsy surgery in focal epilepsies associated with temporomesial glioneuronal tumors: lesionectomy compared with tailored resection. J Neurosurg. 2009;111:1275–82. doi: 10.3171/2009.3.JNS081350. [DOI] [PubMed] [Google Scholar]
- 68.Pelliccia V, Deleo F, Gozzo F, Sartori I, Mai R, Cossu M, et al. Early and late epilepsy surgery in focal epilepsies associated with long-term epilepsy-associated tumors. J Neurosurg. 2017;127:1147–52. doi: 10.3171/2016.9.JNS161176. [DOI] [PubMed] [Google Scholar]
- 69.Cossu M, Fuschillo D, Bramerio M, Galli C, Gozzo F, Pelliccia V, et al. Epilepsy surgery of focal cortical dysplasia-associated tumors. Epilepsia. 2013;54 Suppl 9:115–22. doi: 10.1111/epi.12455. [DOI] [PubMed] [Google Scholar]
- 70.Giulioni M, Marucci G, Martinoni M, Volpi L, Riguzzi P, Marliani AF, et al. Seizure outcome in surgically treated drug-resistant mesial temporal lobe epilepsy based on the recent histopathological classifications. J Neurosurg. 2013;119:37–47. doi: 10.3171/2013.3.JNS122132. [DOI] [PubMed] [Google Scholar]
- 71.Bonney PA, Glenn CA, Ebeling PA, Conner AK, Boettcher LB, Cameron DM, et al. Seizure freedom rates and prognostic indicators after resection of gangliogliomas: a review. World Neurosurg. 2015;84:1988–96. doi: 10.1016/j.wneu.2015.06.044. [DOI] [PubMed] [Google Scholar]
- 72.Nolan MA, Sakuta R, Chuang N, Otsubo H, Rutka JT, Snead OC, 3rd, et al. Dysembryoplastic neuroepithelial tumors in childhood: long-term outcome and prognostic features. Neurology. 2004;62:2270–6. doi: 10.1212/01.wnl.0000130495.69512.6f. [DOI] [PubMed] [Google Scholar]
- 73.Santos MV, de Oliveira RS, Machado HR. Approach to cortical dysplasia associated with glial and glioneuronal tumors (FCD type IIIb) Childs Nerv Syst. 2014;30:1869–74. doi: 10.1007/s00381-014-2519-z. [DOI] [PubMed] [Google Scholar]
- 74.Lombardi D, Marsh R, de Tribolet N. Low grade glioma in intractable epilepsy: lesionectomy versus epilepsy surgery. Acta Neurochir Suppl. 1997;68:70–4. doi: 10.1007/978-3-7091-6513-3_13. [DOI] [PubMed] [Google Scholar]
- 75.Qiu B, Ou S, Song T, Hu J, You L, Wang Y, et al. Intraoperative electrocorticography-guided microsurgical management for patients with onset of supratentorial neoplasms manifesting as epilepsy: a review of 65 cases. Epileptic Disord. 2014;16:175–84. doi: 10.1684/epd.2014.0662. [DOI] [PubMed] [Google Scholar]
- 76.Sugano H, Shimizu H, Sunaga S. Efficacy of intraoperative electrocorticography for assessing seizure outcomes in intractable epilepsy patients with temporal-lobe-mass lesions. Seizure. 2007;16:120–7. doi: 10.1016/j.seizure.2006.10.010. [DOI] [PubMed] [Google Scholar]
- 77.O'Leary DS, Lovell MR, Sackellares JC, Berent S, Giordani B, Seidenberg M, et al. Effects of age of onset of partial and generalized seizures on neuropsychological performance in children. J Nerv Ment Dis. 1983;171:624–9. doi: 10.1097/00005053-198310000-00006. [DOI] [PubMed] [Google Scholar]
- 78.Vendrame M, Alexopoulos AV, Boyer K, Gregas M, Haut J, Lineweaver T, et al. Longer duration of epilepsy and earlier age at epilepsy onset correlate with impaired cognitive development in infancy. Epilepsy Behav. 2009;16:431–5. doi: 10.1016/j.yebeh.2009.08.008. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Detailed summary of literatures on factors associated with seizure outcome in epilepsy surgery of low-grade epilepsy-associated neuroepithelial tumors
Detailed summary of literatures on factors associated with cognitive outcome in epilepsy surgery of low-grade epilepsy-associated neuroepithelial tumors