

Abstract
The aim of this study was to explore the root morphology and root canal configuration of first premolars among Shandong Chinese residents using cone-beam computed tomography (CBCT).
Randomly selected CBCT images were collected from 648 patients (44% women, 56% men). In total, 1268 maxillary and 1296 mandibular first premolars were analyzed. The number of roots and the canal configuration were recorded and identified based on Vertucci's classification.
The majority of the maxillary first premolars had 1 root (67.4%), followed by 2 roots (32%). A 2-canal configuration (89%) was the most prevalent observation. For mandibular first premolars, 98.8% had 1 root and 81% presented the type I configuration. There were no statistical differences in the number of roots or morphology in terms of the left/right side or sex (P > .05).
Among Chinese residents, the majority of maxillary first premolars had 1 root and 2 canals, whereas the most common anatomical configuration for mandibular first premolars was 1 root with 1 canal.
Keywords: CBCT, first premolars, racial diversity, root canal anatomy, root canal variation
Highlights
Root canal morphology of first premolars exhibited appreciable diversity.
Various root canal configurations of first premolars, including type 2-1-2-1, and the additional canals should deserve full attention.
Root canal morphology of first premolars exhibited no differences in terms of the left/right side or sex.
1. Introduction
Endodontic (root canal) treatment is the most fundamental and effective approach used for the management of pulpitis and periapical lesions. The clinical success of endodontic treatment involves the removal of inflamed or necrotic pulp tissues, cleaning and shaping of the root canals, followed by obturation of the prepared canals.[1,2,3,4,5] Root canal therapy of first premolars is frequently indicated due to the wedge-shaped defects leading to pulp exposure or a fractured malformed apex.[6] A wide range of variations in the root canal morphological configuration may complicate the endodontic treatment if any of the root canal is left untreated.[6,7] An untreated missing root canal can lead to the persistent presence of microorganisms and necrotic tissue inside the canal, accounting for a high rate of root canal failure. Therefore, a solid understanding of the root canal morphology and possible variations is an essential prerequisite to reduce the failure of endodontic treatment.
Among various classification systems, Vertucci's classification is used widely to study root canal morphology of various teeth.[8,9,10] In addition, different in vivo and in vitro methods are utilized to investigate root canal anatomy. Previously, transparent tooth staining technology and tissue slices of isolated teeth were widely employed.[11] However, more recently, cone-beam computed tomography (CBCT) has been introduced; this method can provide a high-precision 2-dimensional and 3-dimensional analysis of root canal anatomy without the need of any sample preparation or tooth destruction.[12]
The maxillary and mandibular first premolars have a highly diverse canal configuration that varies among races and geographic regions. Li et al[9] found that the most common anatomy of maxillary first premolars is 1 root with 2 canals (58.0%). The typical canal morphology is type IV (42.7%) in the Chinese population. In addition, Martins et al[13] have reported a higher prevalence of single-root configurations (83.2%) in maxillary first premolars in the Asian subpopulation, compared to whites with 48.7%. In mandibular first premolars, Dai et al[14] found that the incidence of a single-root canal is 58.2% to 88.5%, which varies in different regions and races. Therefore, the present study aimed to explore the root morphology and corresponding root canal configuration of first premolars among Shandong Chinese residents using CBCT.
2. Material and methods
2.1. Ethics approval
This study was approved by the Institutional Research Ethics Committee at the Qingdao Stomatological Hospital, China (approval number: QDSKQEC-91150427). All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
2.2. Subjects
Considering the Minors Protection Ordinance, the Ethics Committee restricted the use of CBCT to only include participants aged 18 years or older. The present study included 648 patients (288 women and 360 men; aged 18–65 years) attending the Department of Cariology and Endodontology, Qingdao Stomatological Hospital, China, between January 2016 and January 2018 and requiring CBCT examination for dental diagnosis/treatment planning (such as for the diagnosis of dentoalveolar trauma, management of impacted teeth, assessment of bone volume, and nonsurgical and surgical endodontic treatment planning). All patients were Han Chinese, the largest ethnic group in China. An informed consent was signed by all participants.
2.3. Selection criteria
The CBCT imaging data were analyzed to select maxillary first premolars (n = 1268) and mandibular first premolars (n = 1296) for further investigations. The following eligibility criteria were applied for all first premolars: complete root development with closed apices; no root resorption or calcification or any associated periapical pathology; no longitudinal fissures; no endodontic treatment, root canal fillings, or restorations; clear imaging data. Patients who had an extracted premolar for orthodontic treatment or due to any other reasons were excluded.
2.4. Image acquisition
CBCT scanning of full dentition was accessed by a NewTom VG CBCT instrument (Quantitative Radiology, Verona, Italy). The exposure parameters for CBCT imaging were 110 kVp and 4.19 to 107.39 mAs, in accordance with the patient's size and field of view. The field of view was 15 cm × 15 cm or 12 cm × 8 cm. The minimum amount of radiation required to obtain an adequate image quality was used for the CBCT exposure. Subsequently, using a voxel size of 0.15 mm, the acquired images were reconstructed as DICOM data sets and imported into QR-NNT Version 2.19 software (AFP Imaging Corporation, USA) to analyze the cross-sectional data.
2.5. Image evaluation
Two competent endodontists with >10 years of experience in clinical endodontic practice simultaneously assessed the CBCT imaging data individually and compared the findings. In case of any disagreement, they discussed the data until a consensus was reached. The data were calibrated by analyzing 8.0% of the samples to determine the reliability of the evaluation. The teeth under investigation (first premolars) were centered, and the images were analyzed carefully in the sagittal, axial, and coronal views to record the following observations: the anatomical position of the premolars, the number and morphology of the roots; and the morphology of the root canal system according to Vertucci's classification (Fig. 1).[15] In addition, a number of root canal morphologies not included in Vertucci's classification were listed as additional root canals types and recorded according to their respective forms (Figs. 2345).
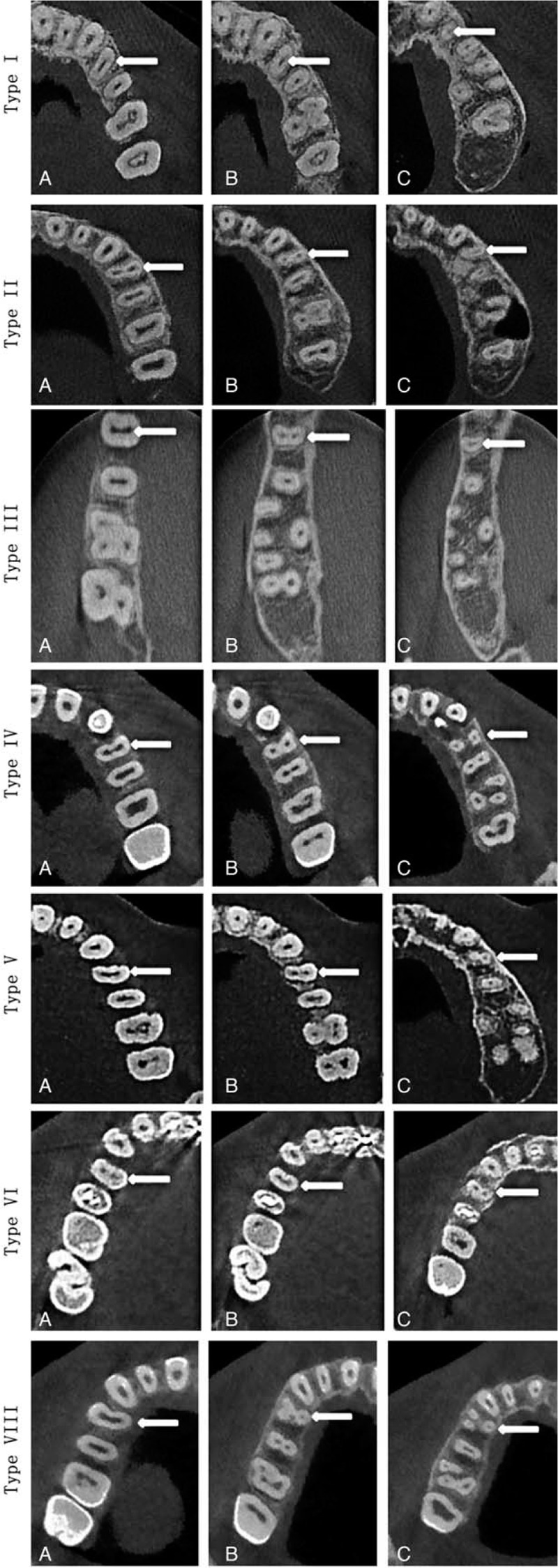
Figure 1.
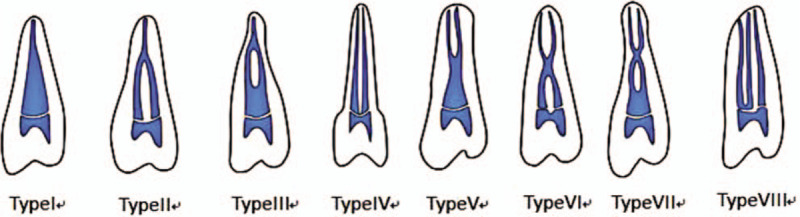
Schematic presentation of Vertucci's classification[33] used in the present study to classify the root canal morphology of first premolars: type I (1–1), type II (2–1), type III (1-2-1), type IV (2-2), type V (1-2-2), type VI (2-1-2), type VII (1-2-1-2), and type VIII (3-3).
Figure 2.
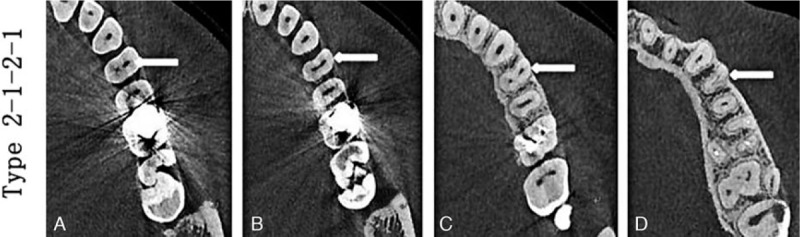
CBCT images (axial plane) revealing the type 2-1-2-1 root canal configuration at different levels of the root. (A) coronal; (B–C) middle third; and (D) apical third. CBCT = cone-beam computed tomography.
Figure 3.
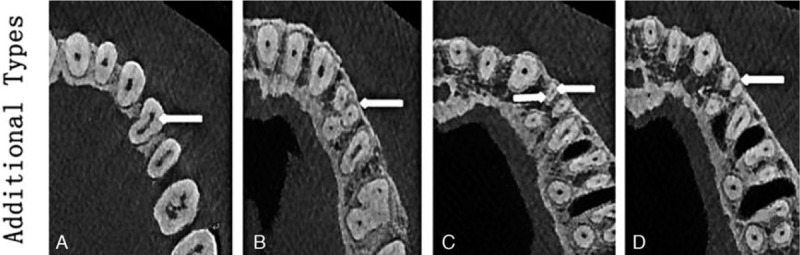
CBCT images (axial plane) reveal additional types of canals (arrows indicate the mesial-buccal root canal type 1-2-1) at different levels of the root. (A) coronal; (B–C) middle third; and (D) apical third. CBCT = cone-beam computed tomography.
Figure 4.
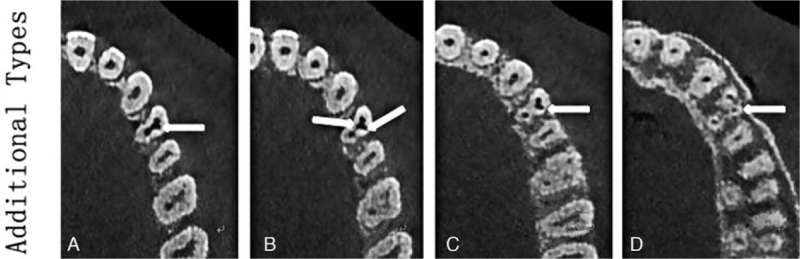
CBCT images (axial plane) reveal additional types of canals (arrows indicate the distal-buccal root canal type 2-1) at different levels of the root. (A) coronal; (B–C) middle third; and (D) apical third. CBCT = cone-beam computed tomography.
Figure 5.
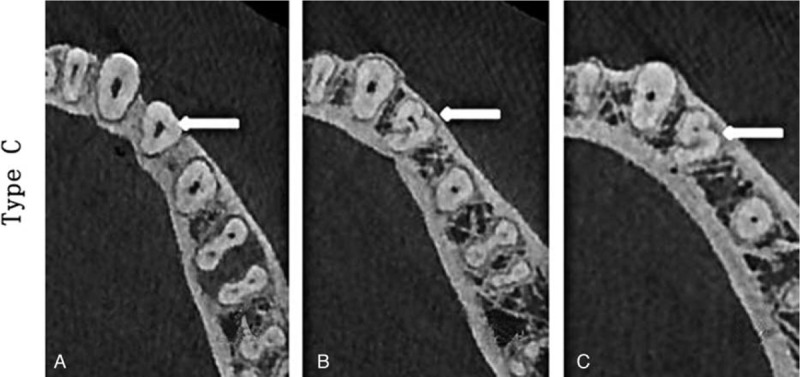
CBCT images (axial plane) showing the type C root canal configuration in a mandibular premolar at different levels of the root. (A) coronal; (B) middle third; and (C) apical third. CBCT = cone-beam computed tomography.
2.6. Statistical analysis
The data were statistically analyzed using SPSS 19.0 (SPSS, Inc., Chicago, IL). Cohen kappa test was applied to analyze the interexaminer and intraexaminer reliability. Other parameters (sex, right or left side) were analyzed by the χ2 test. A P value < .05 was considered statistically significant.
3. Results
All first premolars (1268 maxillary and 1296 mandibular) were carefully evaluated and 28 teeth (maxillary and mandibular) were excluded for not meeting the inclusion criteria (16 were endodontically treated and 12 had severely calcified canals). The Cohen kappa values showed satisfactory results for the interexaminer (0.906 and 0.887) and intraexaminer (0.919 and 0.894) agreements. The procedure was reliable for the evaluations and measurements performed by the 2 observers.
3.1. Numbers and anatomy of the root canals
For the maxillary first premolars, the majority of teeth were single-rooted (67.4%), whereas the minority of teeth had multiple roots (32%), and this difference was significant. The present study found only 7 (0.5%) maxillary first premolars with three roots (Table 1). For the mandibular first premolars, we observed a clear dominance of single-rooted premolars (98.2%), followed by a significantly lower number of premolars with 2 roots (1.2%). The present study detected no mandibular first premolars with ≥3 roots (Table 1).
Table 1.
Distribution of the number of roots and various configuration types in maxillary and mandibular first premolars; n (%).

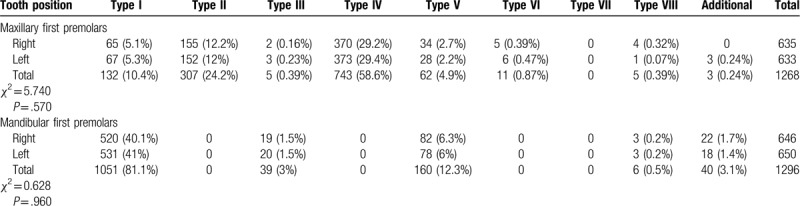
In terms of the canal configuration of the maxillary first premolars, the majority of roots had 2 root canals (89%) with various Vertucci types (type II: 24.2%, type III: 0.39%, type IV: 58.6%, type V: 4.9%, type VI: 0.87%), followed by 1 canal configuration (type I: 10.4%) and 3 canals (type VIII: 0.39%) (Table 1, Fig. 6). Whereas for the mandibular first premolars, the majority of teeth had a Vertucci's type I configuration (81%), which was significantly more common than the other types of canal configurations that altogether contributed about 18.5% (Table 1, Fig. 7). Additionally, no significant difference (P > .05) in the number of roots of the first premolars was observed between sexes (Table 2) or side (Table 3). Similarly, no significant difference (P > .05) was observed in the distribution of morphology/type of the root canal in terms of sex across the midline (Tables 4 and 5).
Figure 6.
Representative CBCT images (axial plane) showing various root forms of maxillary first premolars (arrows) at different levels of the root: (A) coronal; (B) middle third; and (C) apical third. CBCT = cone-beam computed tomography.
Figure 7.
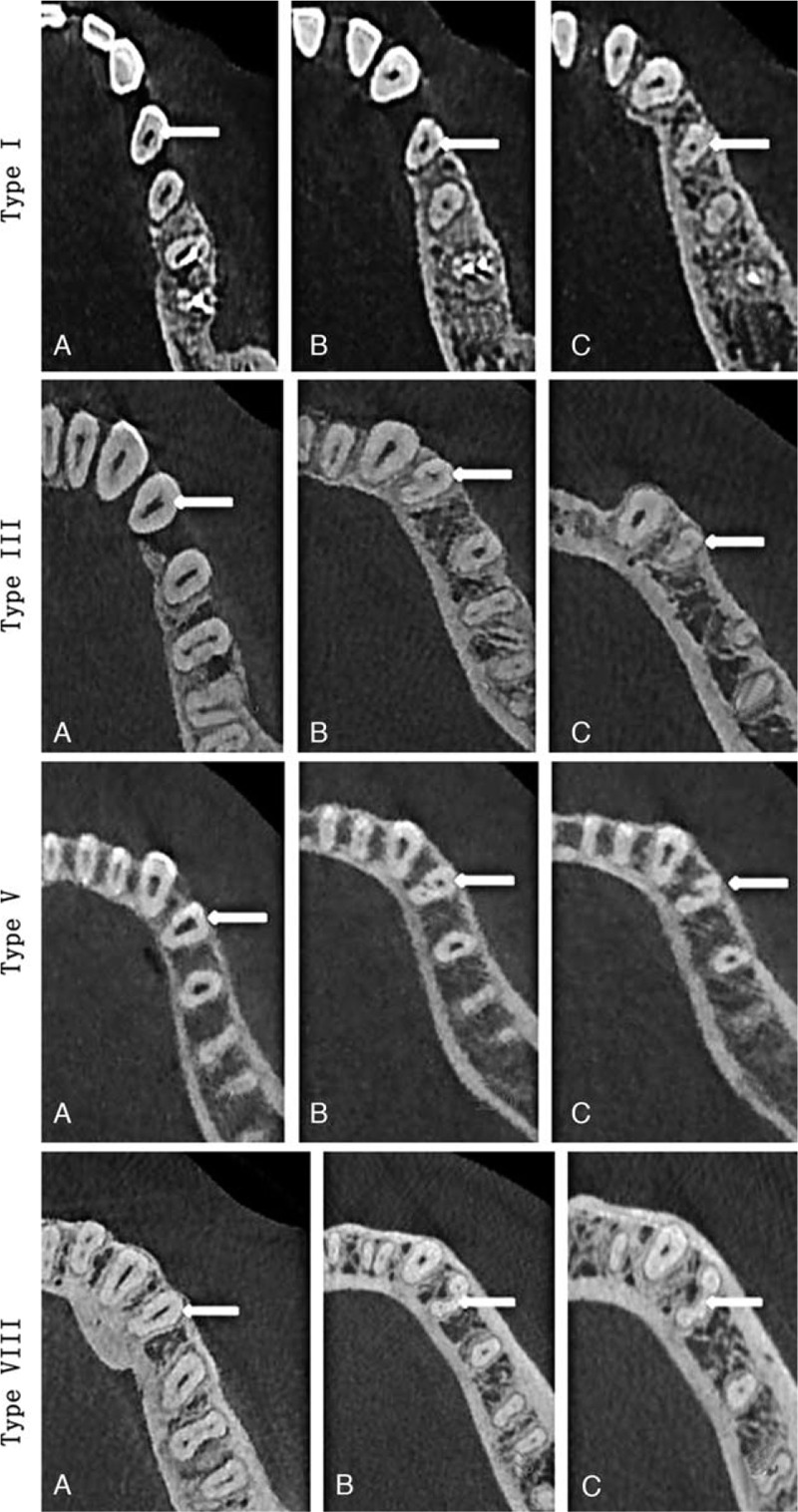
CBCT images (axial plane) showing various root forms of mandibular first premolars (arrows) at different levels of the root: (A) coronal; (B) middle third; and (C) apical third. CBCT = cone-beam computed tomography.
Table 2.
Prevalence of the number of roots of first premolars by sex.
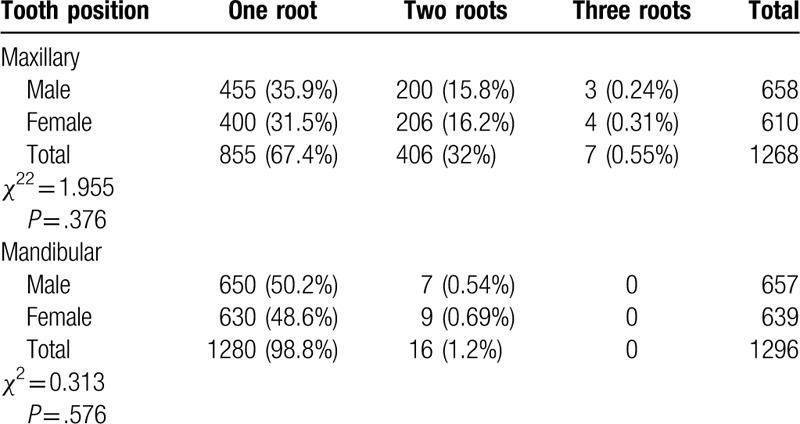
Table 3.
Prevalence of the number of roots of first premolars by tooth position.
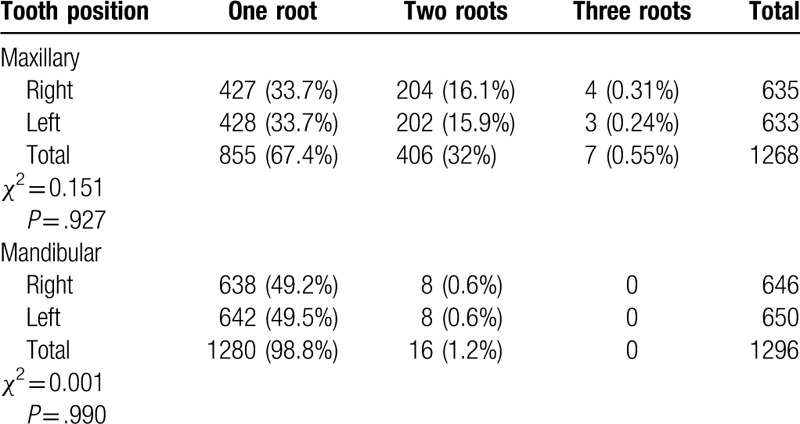
Table 4.
Prevalence of the morphology of the root canal types according to sex.
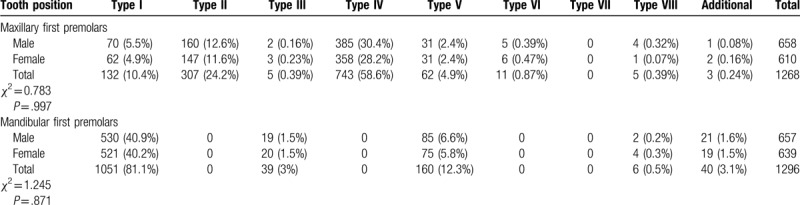
Table 5.
Prevalence of the morphology of the root canal types according to tooth position.
3.2. Additional canal types
A complex canal type (2-1-2-1) was detected in three maxillary first premolar roots; this type had two canals leaving the pulp chamber, rejoining and dividing again into 2 separate canals, and rejoining to form one canal before exiting through the apical foremen (Fig. 2). An additional canal type is shown in Fig. 3; in this type, the mesial-buccal root canal is divided into 2 canals in the mid-root and fused into a single canal before exiting through the apical foramen (Fig. 3A–D). Fig. 4A–D shows another example of an additional root canal in the pulp cavity as well as the central canal and the distal-buccal root canal fused into one at the exit site. The C-shaped canal configuration was observed in 3% of mandibular first premolars (Fig. 5).
4. Discussion
In this study, we analyzed the root anatomy and root canal morphologies of first premolars among Shandong Chinese residents using CBCT. A sound knowledge of root morphology and probability of variation in the root canal configuration is considered important for the clinical success of endodontic procedures as undetected root canals may lead to treatment failure. Therefore, the current study chose to analyze the mandibular and maxillary first premolars specifically to explore their diversity in a Chinese population. For this purpose, we analyzed a large sample size of CBCT imaging data from 648 patients to reduce the sampling bias.
The current study showed that maxillary and mandibular first premolars among Shandong China residents presented with a variety of Vertucci types of canal configurations, with similarities and differences to other reported studies[16,17] in different populations. The number of roots and the morphology of the root canals were the same in both sexes, agreeing with a previous study.[18]
We revealed a higher frequency of 1-rooted maxillary first premolars (67.4%), followed by 2 roots in 32%, and 3 roots in 0.55% of teeth. The 2-canal configuration was the most prevalent observation (89%), whereas one canal was observed in 10.4% and 3 canals were seen in 0.39% of teeth. Previous studies[13,15,19,20,21] suggest that the rate of single-root maxillary first premolars is 31.5% to 79% and that of one root canal is 1.5% to 28.1%. The frequency of 2 roots ranges from 21% to 68.5% and that of 2 root canals ranges from 68.8% to 98.5%. The rates of 3 roots and 3 root canals in maxillary first premolars range from 0% to 6%, whereas we detected 0.55% in the present study.
For mandibular first premolars, our data showed a wide diversity in terms of the number of root canals (1 to 3) and configuration, including the occasional detection of C-shaped root canals. We found 1 root canal in 81% and multiple canals in 19% of root canals. The incidence of a single root canal ranges from 58.2% to 88.5%, in different regions and races. Cleghorn et al[22] pointed out that mandibular first premolars have a single root canal in 68.1% and 2 root canals in 31.9% of Iranian patients. Meanwhile, Lu et al[23] found a single root canal in 54% of mandibular first premolars among Taiwanese patients.
A significant range of diversity in the tooth anatomy of both maxillary and mandibular first premolars includes the possibility of the rare type 2-1-2-1 and type C canal configurations, which was similar to a previous study.[9] Interestingly, the present study detected a C-shaped root canal in 40 (3%) mandibular first premolars. In general, the incidence of a C-shaped root canal is relatively low in mandibular first premolars in both Chinese and other studies.[24,25] A previous study has shown that the complexity of the root canals of mandibular first premolars may be closely related to the existence of root grooves.[26] The root grooves are usually located near the mesial root surface with an average depth of >0.5 mm, and the incidence of multiple root canals is reported to be as high as 78.7%.[27]
Another study[28] has found that additional canals may occur when preoperative radiographs show a sharp thinning, bifurcation, interruption, or double periapical imaging at the middle of the root canal. It is of great value to diagnose the above situations using periapical radiography with a variable angle projection technique or CBCT. CBCT is a nondestructive scanning technique without sample size limitations.[29] In addition, it is convenient to view different sections of teeth to observe the root canal morphology.[30] Currently, micro-CT is widely used to observe the fine anatomical structure of teeth. Dou et al[31] have used micro-CT to investigate the root anatomy and root canal morphology of mandibular first premolars in a southwestern Chinese population and have reported that almost all of the samples were single-rooted (99.4%). Moreover, 64.04% of the teeth possessed type I canal systems, whereas 34.27% had 2 canals and 1.69% had 3 canals. Guerreiro et al[32] used micro-CT and found that the anatomical variations of the mandibular first premolars were closely related to the radicular groove region. Although micro-CT has a higher resolution for observing teeth, it is not available for routine clinical use because of the confined scanning area.
Furthermore, an adequate access opening and root canal file preflexion would also help to find extra root canals, so we suggest that the pulp access opening should be extended in special cases from the traditional oval to various shapes, depending on the location of the extra root canals as determined by CBCT. At the same time, the use of magnifying microscopy during the root canal treatment may help to explore the extra root canals.
The present study reflected the internal root morphology of first premolars among Shandong residents and provided a theoretical basis for the clinical treatment to some extent. The findings of anatomical types of root canals were closely related to the sample size and the experimental method. However, there are a few limitations that must be mentioned. The present study was a single-center study, and the sample size could have been larger. In addition, the spatial resolution of CBCT used in this study was lower than that of micro-CT and nano-CT, which may affect the results to some extent. Further multicenter studies using advanced techniques such as micro-CT may mitigate the limitations of the present study.
5. Conclusions
Patient ethnicity is an incontrovertible factor that affects the root canal anatomy. The root canal anatomy of maxillary and mandibular first premolars among Chinese residents revealed a wide range of variations. The majority of maxillary first premolars had 1 root and 2 root canals, whereas the most common anatomical configuration for mandibular first premolars was 1 root with 1 root canal. Occasionally, additional canal types exist, which deserve the full attention of clinicians.
Acknowledgments
The authors especially acknowledge the cooperation of the Department of Epidemiology and Health Statistics, School of Public Health, Qingdao University.
Author contributions
Conceptualization: Di Wu, Dan-qing Hu, Bing-chang Xin, Jing-yuan Su.
Data curation: Di Wu, Dan-qing Hu, Bing-chang Xin, De-gang Sun, Zhi-pu Ge, Jing-yuan Su.
Formal analysis: De-gang Sun, Jing-yuan Su.
Funding acquisition: De-gang Sun, Jing-yuan Su.
Investigation: Di Wu.
Methodology: Di Wu.
Software: Zhi-pu Ge.
Visualization: Bing-chang Xin, De-gang Sun, Jing-yuan Su.
Writing – original draft: Di Wu, Dan-qing Hu, Bing-chang Xin, De-gang Sun, Jing-yuan Su.
Writing – review & editing: Di Wu, Dan-qing Hu, Zhi-pu Ge, Jing-yuan Su.
Footnotes
Abbreviation: CBCT = cone-beam computed tomography.
How to cite this article: Wu D, Hu Dq, Xin Bc, Sun Dg, Ge Zp, Su Jy. Root canal morphology of maxillary and mandibular first premolars analyzed using cone-beam computed tomography in a Shandong Chinese population. Medicine. 2020;99:20(e20116).
The authors report no conflicts of interest.
All data generated or analyzed during this study are included in this published article [and its supplementary information files.
References
- [1].Song M, Kim HC, Lee W, et al. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. J Endodont 2011;37:1516–9. [DOI] [PubMed] [Google Scholar]
- [2].Ng YL, Mann V, Rahbaran S, et al. Outcome of primary root canal treatment: systematic review of the literature—part 1. Effects of study characteristics on probability of success. Int Endodont J 2007;40:921–39. [DOI] [PubMed] [Google Scholar]
- [3].Vertucci FJ. Root canal morphology and its relationship to endodontic procedure. Endodontic Topics 2010;10:3–29. [Google Scholar]
- [4].Sjogren U, Hagglund B, Sundqvist G, et al. Factors affecting the long-term results of endodontic treatment. J Endodont 1990;16:498–504. [DOI] [PubMed] [Google Scholar]
- [5].Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endodont 1979;5:83–90. [DOI] [PubMed] [Google Scholar]
- [6].Ahmad IA, Alenezi MA. Root and root canal morphology of maxillary first premolars: a literature review and clinical considerations. J Endodont 2016;42:861–72. [DOI] [PubMed] [Google Scholar]
- [7].de Pablo OV, Estevez R, Peix Sanchez M, et al. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endodont 2010;36:1919–31. [DOI] [PubMed] [Google Scholar]
- [8].Mothanna A, Muhammad SZ. Evaluation of root canal morphology of maxillary molars using cone beam computed tomography. Pak J Med Sci 1900;31:426–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Li YH, Bao SJ, Yang XW, et al. Symmetry of root anatomy and root canal morphology in maxillary premolars analyzed using cone-beam computed tomography. Arch Oral Biol 2018;94:84–92. [DOI] [PubMed] [Google Scholar]
- [10].Zafar MS, Alrahabi M. Cone beam computed tomography for exploring morphology of mandibular first molar. British Journal of Medicine and Medical Research 2015;6:514–21. [Google Scholar]
- [11].Jain A, Bahuguna R. Root canal morphology of mandibular first premolar in a gujarati population—an in vitro study. Dent Res J (Isfahan) 2011;8:118–22. [PMC free article] [PubMed] [Google Scholar]
- [12].Felsypremila G, Vinothkumar TS, Kandaswamy D. Anatomic symmetry of root and root canal morphology of posterior teeth in Indian subpopulation using cone beam computed tomography: a retrospective study. Eur J Dentistry 2015;9:500–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Martins JNR, Gu Y, Marques D, et al. Differences on the root and root canal morphologies between Asian and white ethnic groups analyzed by cone-beam computed tomography. J Endodont 2018;44:1096–104. [DOI] [PubMed] [Google Scholar]
- [14].Hai-feng D, Ya-wen L, Ya-qian L, et al. Investigation on the root canal configuration of the mandibular first premolars with radicular groove by micro-computer tomography. Acta Univ Med Nanjing 2018;38:838–42. [Google Scholar]
- [15].Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589–99. [DOI] [PubMed] [Google Scholar]
- [16].Hai-bo Zhang, Chang-lian Du. Study on root canal system of maxillary first premolar. J Clin Stomatol 2014;12:721. [Google Scholar]
- [17].Liu N, Li X, Liu N, et al. A micro-computed tomography study of the root canal morphology of the mandibular first premolar in a population from southwestern China. Clin Oral Investigat 2013;17:999–1007. [DOI] [PubMed] [Google Scholar]
- [18].Yang L, Chen X, Tian C, et al. Use of cone-beam computed tomography to evaluate root canal morphology and locate root canal orifices of maxillary second premolars in a Chinese subpopulation. J Endodont 2014;40:630–4. [DOI] [PubMed] [Google Scholar]
- [19].Loh HS. Root morphology of the maxillary first premolar in Singaporeans. Aust Dent J 1998;43:399–402. [DOI] [PubMed] [Google Scholar]
- [20].Zhang DH, Da-Ming WU, You-Nong WU, et al. Root form and canal morphology of maxillary first premolars. Acta Univ Med Nanjing 2011;31:213-5.234. [Google Scholar]
- [21].Kai C, Ping W, Zhang M. Morphology of roots and canals in maxillary first premolars. J Pract Stomatol 2005;21:121–3. [Google Scholar]
- [22].Cleghorn BM, Christie WH, Dong CC. The root and root canal morphology of the human mandibular first premolar: a literature review. J Endodont 2007;33:509–16. [DOI] [PubMed] [Google Scholar]
- [23].Lu TY, Yang SF, Pai SF. Complicated root canal morphology of mandibular first premolar in a Chinese population using the cross section method. J Endodont 2006;32:932–6. [DOI] [PubMed] [Google Scholar]
- [24].Liao Q, Han JL, Xu X. [Analysis of canal morphology of mandibular first premolar]. Shanghai Kou Qiang Yi Xue 2011;20:517–21. [PubMed] [Google Scholar]
- [25].Sikri VK, Sikri P. Mandibular premolars: aberrations in pulp space morphology. Indian J Dent Res 1994;5:9–14. [PubMed] [Google Scholar]
- [26].Fan B, Yang J, Gutmann JL, et al. Root canal systems in mandibular first premolars with C-shaped root configurations. Part I: microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endodont 2008;34:1337–41. [DOI] [PubMed] [Google Scholar]
- [27].Gu Y, Zhang Y, Liao Z. Root and canal morphology of mandibular first premolars with radicular grooves. Arch Oral Biol 2013;58:1609–17. [DOI] [PubMed] [Google Scholar]
- [28].Sun Y, Lu TY, Chen YC. The best radiographic method for determining root canal morph- ology in mandibular first premolars: a study of Chinese descendants in Taiwan. J Dent Sci 2016;11:175–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Neelakantan P, Subbarao C, Subbarao CV. Comparative evaluation of modified canal staining and clearing technique, cone-beam computed tomography, peripheral quantitative computed tomography, spiral computed tomography, and plain and contrast medium-enhanced digital radiography in studying root canal morphology. J Endodont 2010;36:1547–51. [DOI] [PubMed] [Google Scholar]
- [30].Bulut DG, Kose E, Ozcan G, et al. Evaluation of root morphology and root canal configuration of premolars in the Turkish individuals using cone beam computed tomography. Eur J Dent 2015;9:551–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Dou L, Li D, Xu T, et al. Root anatomy and canal morphology of mandibular first premolars in a Chinese population. Sci Rep 2017;7:750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Guerreiro D, Shin JM, Pereira M, et al. Radicular groove accessory canal morphology in mandibular first premolars: micro-computed tomographic study. J Endodont 2019;45:554–9. [DOI] [PubMed] [Google Scholar]
- [33].Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dental Assoc 1978;97:47–50. [DOI] [PubMed] [Google Scholar]