

Abstract
The current study is a retrospective epidemic report regarding dengue fever (DF) virus infection cases (2017) from fifteen districts of KPK, Pakistan. Medical records of 120 948 patients were reviewed retrospectively for demographic, clinical and laboratory data. The presence of dengue infection was confirmed by NS1-ELISA and RT-PCR, respectively. The total positive cases (of suspected DF samples) were 24 938 (20.6%), whereas seventy cases (0.28%) had a fatal outcome. Mean age ± SD of the dengue patients was 26 ± 19.8 years, while; the most affected age group was from 16 to 30 years (Chi-square: 12 820.125, p: 0.00). The infected males were 65.3%, and that of the female was 34.7%. All the dengue-infected patients were observed with symptoms of severe fever (100%), body aches (95%), gums and nose bleeding (5%), skin rashes (30%), vomiting (70%). The highest infection rate was found in district Peshawar and that of the lowest was in Bannu, Hungu and Luki Marwat. A high rate of dengue infection was found in post-monsoon months i.e. October (41%) and September (32%) of the year. The results proved that if the dengue outbreaks reveal further in KPK, it could alarmingly increase the mortality rate. Therefore, the Department of Public Health in KPK, Pakistan may take proper measures to avoid and control dengue epidemics in the future.
Key words: Dengue fever, infection, IDSRS, KPK, patients, symptoms, climate
Introduction
Dengue is a mosquito-borne viral ailment which infects over 100 million human population with an annual mortality rate of 30 000 globally (WHO 2013). Dengue virus (DENV) consists of single-stranded positive-sense RNA, belongs to genus Flavivirus, and family Flaviviridae (Durrani et al. 2014; Khan et al. 2018a). Commonly, four antigenically distinct serotypes of DENV have been reported, i.e. DENV 1 to DENV 4 (Durrani et al. 2014; Waseem et al. 2014; Suleman et al. 2017a; Suleman et al. 2017b; Khan et al. 2018b; Shams et al. 2018). According to recent reports from Pakistan, the major serotypes found in Punjab were DENV 2, 3 and 4; however, DENV 2 and 3 were found in Swat area of KPK province in 2013 with a high morbidity as well as mortality rate (Khan et al. 2017; Suleman et al. 2017a; Suleman et al. 2017b; Khan et al. 2018a). The serotype 3 has always predominated (Koo et al. 2013). Recently, serotype five (DENV 5) has been revealed via neutralization assays (Ghani et al. 2017; Morra et al. 2018).
The aforesaid viruses are transmitted by female of Aedes mosquito of order Diptera and Culicidae family, especially Aedes aegypti (primary vector) also known as yellow fever mosquito, and in lesser extent (Nasir et al. 2017; Qsim et al. 2017) Aedes albopictus (secondary vector) commonly known as Asian tiger mosquito. There are three main stages of dengue fever (DF): initially mild dengue fever (MDF), followed by severe dengue hemorrhagic fever (DHF), and the life-threatening dengue shock syndrome (DSS).
Dengue fever is endemic in Pakistan; however, highest incidences reported were almost post-monsoon (Rafique et al. 2017; Rafique et al. 2018). Since 2010, this country is facing some terrible epidemics of dengue accompanied by substantial human health issues and deaths. Local transmission of dengue has been reported since it would also have an important role in the reintroduction of the disease. The recent largest dengue pandemics were recorded for the first time in Lahore (2011) with 22 562 cases and 363 fatalities, and for the second time in Swat (2013) causing 8343 morbidities along with 57 deaths. Recently, in 2017 another huge dengue outbreak has been recorded in Peshawar with 23 541 cases (Hurtado-Díaz et al. 2007; Khan et al. 2018a; Rafique et al. 2018). Therefore, the present study is conducted for the recent outbreaks occurred in Khyber Pakhtunkhwa, Pakistan in 2017.
Experimental
Materials and Methods
Study area. The study was performed in Khyber Pakhtunkhwa (KPK), the Northwest province of Pakistan. According to 2017 census, its total area is 74 521 km2 and population is 30.523 million. The province shares boundaries with Afghanistan to the north-west, Gilgit-Baltistan to the north-east, Ex-Federal Administrative Tribal Areas (Ex-FATA) to the west and south, Azad Jammu and Kashmir to the east, Baluchistan to the south, and Islamabad Capital of the Country and Punjab to the South-East. Khyber Pakhtunkhwa is the third highest important populated region of the country (Khan et al. 2017).
Data collection. The study was a retrospective epidemic report regarding DF virus infection cases from fifteen districts of KPK, Pakistan. The data was collected from the Integrated Disease Surveillance and Response System (IDSRS) Directorate General Health Services, Peshawar, KPK, Pakistan with the prior approval of data by the statistical officer of IDSRS.
Clinical manifestations. The indoor patients admitted in different hospitals of the province were investigated for various signs and symptoms e.g. fever, body aches, nausea, vomiting, diarrhea, gum bleeding and bleeding of the nose, skin rashes, animals contact history, and platelet count at admission.
ELISA. The data collected was obtained from medical records. About 120 948 patients were reviewed retrospectively for demographic and clinical as well as laboratory data. The patients’ serum was investigated for the presence of non-structural protein-1 (NS1) antigen in order to identify DENV using ELISA, according to the guidelines of the manufacturer (Platelia Biorad Lab, Marnes-la-Coquette, France) (Lutfullah et al. 2017). In case of positive result, the treatment had been started immediately without any delay; however, in case of the weak positive or ambiguous result of NS1 antigen, the samples were processed with a thermal cycler.
PCR. To confirm the presence of dengue virus in the samples, the protocol adopted by Khan et al. (2017) was followed. Briefly, RNA was extracted and processed with RT-PCR using type-specific DENV primers (TS1-TS4) (Khan et al. 2018a). Both +ve and −ve controls (DENV-1, 2, 3 and 4) were used, respectively. The resultant amplified DNA products were determined on 2% agarose gels (Salman et al. 2015) (Biotium Inc., USA).
Data analysis. The data obtained in the current study was analyzed on the basis of: 1) geographical distribution in 15 Districts of KPK (Abbottabad, Banu, Buner, Dir lower, Hangu, Haripur, Karak, Kohat, Laki Marwat, Malakand, Mansehra, Mardan, Nowshera, Peshawar and Swabi), 2) month-wise (from July – December 2017), 3) age-wise (1–15, 16–30, 41–45, 46–60, and above 60) and 4) sociodemographically (gender-wise and clinical manifestation and outcome basis).
Results
In the current report of 120 948 suspected dengue cases, 24 938 were found positive for DENV that occurred in 15 different districts of Khyber Pakhtunkhwa (KPK) as a result of dengue outbreak in 2017. Preliminarily, out of total positive samples, > 90% of the patients were positive with the NS1 antigen ELISA; however, the remaining < 10% uncertain cases were confirmed with RT-PCR.
The most numerous cases were found positive in district Peshawar (23 541) with 65 deaths, followed by Mardan (369) with one death, and four death cases were reported from Abbottabad (142) (Table I). Male population was affected in a greater extent (65.33%) when compared to female (34.66%). Mostly, the affected patients were found in the age of 16–30 (45%, Chi-square: 12 820.125, p: 0.00), and subsequently of 31–45 (23%), and 1–15 years (20%). On the other hand, patients of age 45–60 and or above 60 years old were less affected (5–7%) (Table III).
Table I.
District-wise geographical distribution of dengue cases in the population.
| District | Suspected cases | Positive cases | Male | Female | No. of deaths |
|---|---|---|---|---|---|
| Abbottabad | 205 | 142 | 114 | 28 | 4 |
| Banu | 6 | 1 | 1 | 0 | 0 |
| Buner | 1102 | 143 | 104 | 39 | 0 |
| Dir lower | 6 | 6 | 5 | 1 | 0 |
| Hangu | 3 | 1 | 1 | 0 | 0 |
| Haripur | 211 | 64 | 42 | 42 | 0 |
| Karak | 12 | 9 | 6 | 3 | 0 |
| Kohat | 99 | 17 | 13 | 4 | 0 |
| Laki Marwat | 278 | 1 | 1 | 0 | 0 |
| Malakand | 667 | 240 | 165 | 75 | 0 |
| Mansehra | 782 | 72 | 49 | 23 | 0 |
| Mardan | 4295 | 369 | 260 | 109 | 1 |
| Nowshehra | 825 | 199 | 138 | 61 | 0 |
| Peshawar | 111979 | 23541 | 15302 | 8239 | 65 |
| Swabi | 478 | 133 | 93 | 40 | 0 |
| Total | 120948 | 24938 | 16294 | 8664 | 70 |
Table III.
Age-based statistical analysis of dengue patients.
| Age Group | Frequencies (% age) | Test Statistics | |
|---|---|---|---|
| 1 to 15 | 4987 (20%) | Chi Square | 12820.125a |
| 16 to 30 | 11222(45%) | Degree of freedom | 4 |
| 31 to 45 | 5735 (23%) | Asymptotic significant value | 0 |
| 45 to 60 | 1748 (7%) | ||
| Above 60 | 1246 (5%) | ||
| Total | 24938(100%) | ||
- 0 cells (0%) have expected frequencies less than 5. The minimum cell frequency is 4987.6.
Clinical information. All the infected and hospitalized patients were observed with mild to severe fever (100%). The most common symptoms were body aches and pain (95%), followed by vomiting and diarrhea (70%), as well as skin rashes (30%). The patients had also hemorrhagic manifestations in the form of gum bleeding and bleeding from the nose (5%) (Table III).
Monthly distribution of dengue fever. The percentage of dengue viral infection was quite low in July and steadily increased in rainy months and the rate became much high in September and October (Table II). It might be owing to the well-established propagation of Aedes (primary and secondary vectors of dengue virus) in the monsoon period of the year. In July the infection rate was least (3%) while it slowly increased in August (16%). In September (32%) and October (41%), the infection rate of DF promptly increased owing to the rainy season, while in November (6%) and December (2%) there was a clear decrease again, which was depicted (Fig. 1).
Table II.
Sociodemographic and clinical presentation of dengue.
| Characteristics | DF (n = 24938) |
|---|---|
| Sociodemographic | |
| Age (years) (Means ± SD) | 26 ±19.8 |
| Male | 16294 (95.3%) |
| Female | 8664 (34.7%) |
| Clinical presentation | |
| Fever | 24938 (100%) |
| Body aches | 23691 (95%) |
| Vomiting/Nausea | 17457 (70%) |
| Skin rashes | 7481 (30%) |
| Bleeding | 1247 (5%) |
| Outcome | |
| Death | 70 (0.28%) |
Fig. 1.
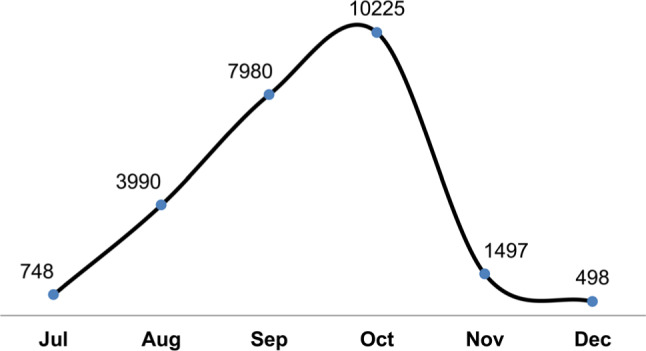
Month-wise dispersal of dengue infection.
Discussion
Most of the developing world is under high risk of dengue virus; hence, it is becoming a main public health issue, particularly in tropical regions (Hurtado-Díaz et al. 2007; Zafar et al. 2013; Kraemer et al. 2015;). In 2013 different regions of Khyber Pakhtunkhwa (KPK) faced permanent epidemics of DF, and the cases of deaths were also recorded. There were three possible reasons for the greater number of dengue cases reported from Peshawar. First, Peshawar is the capital of KPK province; hence, there are two governmental tertiary hospitals and a medical complex. The major health facilities are also available in this city. Second, in 2017, a dengue outbreak was reported from Peshawar; hence, the larger population was affected. Third, some remote areas, especially the Northern and southern hilly area, may be under-reported for dengue. On the other hand, the current study investigated the rate of dengue infection in other districts of Khyber Pakhtunkhwa (KPK). When studied in a similar way with the use of the Integrated Disease Surveillance and Response System (IDSRS), there were 24 938 dengue cases including 70 deaths reported from various districts of KPK. In other words, out of 70 death outcomes, 62 (88.6%) were male, while 8 (11.4%) were female.
The dengue cases in the current study were divided into five groups, based on the age of the patients. The highest dengue rate incidence was found in the following sequence; age 16–30 (45%), 31–45 (23%) and 1–15 years (20%), while the patients of the age 45–60 years and above were less affected (7–5%). These results are in correlation with those described in the documented dengue cases (134) in the patients of age 20–30 years (61.77%), and limitedly in children (Zafar et al. 2013). Moreover, some investigations performed in Singapore showed that the majority of infected patients were older (Gadhwal et al. 2016). In this regard, it has been concluded that adults of 16–30 years old in KPK are in the danger region to dengue infection and the risk may depend to the time spend outside (Khan et al. 2017). Simultaneously, in the present study, the infection rate was found the highest in the male population (65.33%) in comparison to female (34.66%). The same results in six Asian countries regarding the dengue infection rate in male-female were recorded (Ahmad et al. 2011; Gadhwal et al. 2016; Zubair et al. 2016). In another report, 71% rates of dengue RNA positive samples were found in male population of KPK and Punjab (Shahid et al. 2013). One study from KPK revealed that male to female ratio of dengue cases was 2:1 (Suleman et al. 2017a). The comparative studies also mentioned the same consequences of the dengue infection relative to male-female patients (> 15 years older) (Durrani et al. 2014; Khan et al. 2018b). The collected data and the results described in this study are compatible to those already documented in the literature (Ali et al. 2013; Hasan et al. 2013; Khalid et al. 2015; Ghani et al. 2017; Iqtadar et al. 2017). The dengue infection in Asian countries could be acquired during both outdoor and indoor activities. Based on outdoor and indoor activities, it has been concluded that male in KPK could be more affected with dengue infection in comparison to female (Khan et al. 2017; Suleman et al. 2017b). The up-to-date study is also scrutinized in a month-wise since the incidences of dengue infection were observed from July – December. The peak incidences were observed for dengue infection in the following periods of time: September – October (32–41%); July – August (16–3%) and November – December (6–2%). The peak incidence of dengue infection was seen in the post-monsoon season – in October (41%). The similar observation was found in the literature, where a steady increase was measured from August to October (Hasan et al. 2013; Khalid et al. 2015; Ghani et al. 2017;). This has also been previously shown by others (Khan et al. 2006; Khan et al. 2013; Arshad et al. 2015). The main reason for the highest ratio of incidences in post monsoon period may be the water stagnation, what plays a vital role in the reproduction of mosquitoes, vectors of dengue viruses.
Conclusions
From the current report, it may be concluded that DF and DHF are endemic in Khyber Pakhtunkhwa (KPK) in Pakistan; however, Peshawar is under the highest risk of morbidity and mortality. The most affected age group found was from 16 to 30 years. Male to female ratio of the DF was almost 2:1, whereas male to female ratio of mortality was about 9:1. About half of the dengue infection cases reported were in the month of October. In case of negligence of the preventive measures against the dengue outbreak, it may occur an alarming intensification of infections in the future. Therefore, the Department of Public Health in KPK may take a proper consideration to avoid and control dengue epidemics in the future.
The local governments of KPK may play important role in the eradication of dengue fever, therefore, besides the awareness, the proper training given to the teams consisted of young male and female volunteers on union council level is necessary. The emergency response kit may be provided to them and chairperson of the union council may conduct weekly meetings, specifically in monsoon season, in order to combat any disaster on an anticipatory basis. Integrated Disease Surveillance and Response System (IDSRS) with a geographic information system (GIS) are mandatory across the country. IDSRS-GIS will help the health authorities to identify the high-risk area and risk factors, followed by an adaptation of precautionary actions precedent in risk areas.
Footnotes
Conflict of interest
The authors do not report any financial or personal connections with other persons or organizations, which might negatively affect the contents of this publication and/or claim authorship rights to this publication.
ORCID
Muhammad Salman 0000-0002-7605-2806
Ethical approval
The study was approved from the ethical committee of Abdul Wali Khan University Mardan, Pakistan.
Literature
- Ahmad N, Fazal H, Ayaz M, Abbasi BH, Mohammad I, Fazal L. Dengue fever treatment with Carica papaya leaves extracts. Asian Pac J Trop Biomed. 2011;1(4):330–333. doi: 10.1016/S2221-1691(11)60055-5 Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ali A, Rehman H, Nisar M, Rafique S, Ali S, Hussain A, Nausheen, Idrees M, Sabri S, Zada H, et al. . Seroepidemiology of dengue fever in Khyber Pakhtunkhawa, Pakistan. Int J Infect Dis. 2013;17(7):e518–e523. doi: 10.1016/j.ijid.2013.01.007 Medline [DOI] [PubMed] [Google Scholar]
- Arshad K, Sheikh S, Naqvi SU, Sarwar I, Javaid S, Asghar M, Butt MA. Frequency of splenomegaly in dengue fever in children. J Ayub Med Coll Abbottabad. 2015;27(2):356–359. Medline [PubMed] [Google Scholar]
- Durrani MR, Iqbal MD, Munir N, Jamal A. Dengue hemorrhagic fever-epidemic in Karachi, Pakistan (2006–2016) experience at a tertiary care centre. Pak J Surg. 2017;33(1):53–58. [Google Scholar]
- Gadhwal AK, Ankit BS, Chahar C, Tantia P, Sirohi P, Agrawal RP. Effect of Carica papaya leaf extract capsule on platelet count in patients of dengue fever with thrombocytopenia. J Assoc Physicians India. 2016;64(6):22–26. Medline [PubMed] [Google Scholar]
- Ghani E, Mushtaq S, Khan SA. 2017 Multiplex polymerase chain reaction-based serotype analysis of dengue virus during 2015 dengue outbreak in Pakistan. East Mediterr Heal J. 2017;23(9):594–597. Medline [DOI] [PubMed] [Google Scholar]
- Hasan SR, Riaz M, Jafri FA. Characteristics and outcome of dengue infection; clinical perspective from a secondary care hospital of Karachi. Pak J Med Sci. 2013;29(1):115–118. Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurtado-Díaz M, Riojas-Rodríguez H, Rothenberg SJ, Gomez-Dantés H, Cifuentes E. Short communication: impact of climate variability on the incidence of dengue in Mexico. Trop Med Int Health. 2007;12(11):1327–1337. doi: 10.1111/j.1365-3156.2007.01930.x Medline [DOI] [PubMed] [Google Scholar]
- Iqtadar S, Akbar N, Mehmood M, Abaidullah S. Clinical audit of dengue related deaths in 2011 at Mayo Hospital Lahore Pakistan. Pak J Med Sci. 2017;33(5):1070–1073. doi: 10.12669/pjms.335.13051 Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khalid B, Ghaffar A. Environmental risk factors and hotspot analysis of dengue distribution in Pakistan. Int J Biometeorol. 2015;59(11):1721–1746. doi: 10.1007/s00484-015-0982-1 Medline [DOI] [PubMed] [Google Scholar]
- Khan E, Siddiqui J, Shakoor S, Mehraj V, Jamil B, Hasan R. Dengue outbreak in Karachi, Pakistan, 2006: experience at a tertiary care center. Trans R Soc Trop Med Hyg. 2007;101(11):1114–1119. doi: 10.1016/j.trstmh.2007.06.016 Medline [DOI] [PubMed] [Google Scholar]
- Khan J, Ghaffar A, Khan SA. The changing epidemiological pattern of dengue in Swat, Khyber Pakhtunkhwa. PLoS One. 2018a;13(4):e0195706. doi: 10.1371/journal.pone.0195706 Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan J, Khan I, Ali I, Iqbal A, Salman M. The role of vertical transmission of dengue virus among field-captured Aedes aegypti and Aedes albopictus mosquitoes in Peshawar, Khyber Pakhtunkhwa, Pakistan. Pak J Zoo. 2017;49(3):777–784. doi: 10.17582/journal.pjz/2017.49.3.777.784 [DOI] [Google Scholar]
- Khan J, Khan I, Ghaffar A, Khalid B. Epidemiological trends and risk factors associated with dengue disease in Pakistan (1980–2014): a systematic literature search and analysis. BMC Public Health. 2018b;18(1):745. doi: 10.1186/s12889-018-5676-2 Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan MI, Anwar E, Agha A, Hassanien NS, Ullah E, Syed IA, Raja A. Factors predicting severe dengue in patients with dengue Fever. Mediterr J Hematol Infect Dis. 2013;5(1):e2013014. doi: 10.4084/mjhid.2013.014 Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koo C, Nasir A, Hapuarachchi H, Lee KS, Hasan Z, Ng LC, Khan E. Evolution and heterogeneity of multiple serotypes of dengue virus in Pakistan, 2006–2011. Virol J. 2013;10(1):275. doi: 10.1186/1743-422X-10-275 Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraemer MUG, Perkins TA, Cummings DAT, Zakar R, Hay SI, Smith DL, Reiner RC Jr. Big city, small world: density, contact rates, and transmission of dengue across Pakistan. J R Soc Interface. 2015;12(111):20150468. doi: 10.1098/rsif.2015.0468 Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lutfullah G, Ahmed J, Aftab Khan HI, Ahmad J. Evaluation of Non-Structural Protein-1 (NS1) positive patients of 2013 dengue outbreak in Khyber Pakhtunkhwa, Pakistan. Pak J Med Sci. 2017; 33(1):172–176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morra ME, Altibi AMA, Iqtadar S, Minh LHN, Elawady SS, Hallab A, Elshafay A, Omer OA, Iraqi A, Adhikari P, et al. . Definitions for warning signs and signs of severe dengue according to the WHO 2009 classification: systematic review of literature. Rev Med Virol. 2018;28(4):e1979. doi: 10.1002/rmv.1979 [DOI] [PubMed] [Google Scholar]
- Nasir S, Jabeen F, Abbas S, Nasir I, Debboun M. Effect of climatic conditions and water bodies on population dynamics of the dengue vector, Aedes aegypti (Diptera: culicidae). J Arthropod Borne Dis. 2017;11(1):50–59. Medline [PMC free article] [PubMed] [Google Scholar]
- Qsim M, Ashfaq UA, Yousaf MZ, Masoud MS, Rasul I, Noor N, Hussain A. Genetically modified Aedes aegypti to control dengue: A review. Crit Rev Eukaryot Gene Expr. 2017;27(4):331–340. [DOI] [PubMed] [Google Scholar]
- Rafique I, Saqib MA, Munir MA, Siddiqui S, Malik IA, Rao MH, Ahmed J, Bashir S, Khan O, Firdous R, et al. . Dengue knowledge and its management practices among physicians of major cities of Pakistan. J Pak Med Assoc. 2015;65(4):392–396. Medline [PubMed] [Google Scholar]
- Rafique I, Saqib MAN, Munir MA, Qureshi H, Taseer IH, Iqbal R, Ahmed W, Akhtar T, Rizwanullah. Asymptomatic dengue infection in adults of major cities of Pakistan. Asian Pac J Trop Med. 2017;10(10):1002–1006. doi: 10.1016/j.apjtm.2017.09.013 Medline [DOI] [PubMed] [Google Scholar]
- Salman M, Ali A, Jabbar A, Sarwar Y, Rahman M, Iqbal M, Haque A. Simplest identification, O-specific polysaccharide purification and antigenic evaluation of Salmonella enterica serovar Typhi Vi negative isolate. EXCLI J. 2015;14:1078–1084. Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shahid M, Amin I, Afzal S, Fatima Z, Zahid S, Ashraf U, Idrees M. Prevalence and molecular detection of dengue virus in 2013 outbreak in KPK and Punjab, Pakistan. Pak J Zool. 2017; 49(3):1119–1122. doi: 10.17582/journal.pjz/2017.49.3.sc4 [DOI] [Google Scholar]
- Shams N, Amjad S, Yousaf N, Ahmed W, Seetlani NK, Farhat S. Dengue knowledge in indoor dengue patients from low socioeconomic class; aetiology, symptoms, mode of transmission and prevention. J Ayub Med Coll Abbottabad. 2018;30(1):40–44. Medline [PubMed] [Google Scholar]
- Suleman M, Faryal R, Alam MM, Khurshid A, Sharif S, Shaukat S, Angez M, Umair M, Sufian MM, Arshad Y, et al. . Outbreak of dengue virus type-3 in Malakand, Pakistan 2015; A laboratory perspective. Acta Trop. 2017a;169:202–206. doi: 10.1016/j.actatropica.2017.02.011 Medline [DOI] [PubMed] [Google Scholar]
- Suleman M, Faryal R, Alam MM, Sharif S, Shaukat S, Aamir UB, Khurshid A, Angez M, Umair M, Sufian MM, et al. . Dengue virus serotypes circulating in Khyber Pakhtunkhwa province, Pakistan, 2013–2015. Ann Lab Med. 2017b;37(2):151–154. doi: 10.3343/alm.2017.37.2.151 Medline [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waseem T, Latif H, Shabbir B. An unusual cause of acute abdominal pain in dengue fever. 2014. Am J Emerg Med. 32(7):819: 3–4. [DOI] [PubMed] [Google Scholar]
- WHO Dengue in Pakistan. Weekly Epidemiological Monitor. World Health Organization. 2013. Dec 29;6(52). [Google Scholar]
- Zafar H, Hayyat A, Akhtar N, Rizwan SF. Prevalence of undifferentiated fever in adults of Rawalpindi having primary dengue fever. J Pak Med Assoc. 2013;63(6):770–771. Medline [PubMed] [Google Scholar]
- Zubair M, Ashraf M, Ahsan A, Nazir NU, Hanif H, Khan HA. Dengue viral infections in Pakistan and other Asian countries: a comprehensive review. J Pak Med Assoc. 2016;66(7):884–888. Medline [PubMed] [Google Scholar]