

Abstract
Cardiac disease is increasingly diagnosed in pet rabbits, presumably because of their lengthening life span and the increased sophistication of their veterinary care. However, relatively little is known about the origins of and therapy for cardiac disease in pet rabbits. Dyspnea, murmurs, and arrhythmias are common clinical signs in rabbits with cardiac disease. However, rabbits with congestive heart failure may hide signs of illness until the disease has become severe. Unique physiologic characteristics (e.g., obligate nasal breathing and limited collateral circulation to the myocardium) predispose rabbits to collapse from stress and oxygen deprivation; therefore, oxygen supplementation and stabilization are priorities for the rabbit presenting in cardiorespiratory distress. The diagnostic workup for cardiac disease in rabbits is very similar to that for traditional pets and involves radiography, electrocardiography, and echocardiography. Cardiomyopathy and valvular degeneration are relatively common forms of cardiac disease in rabbits, while congenital anomalies are rare. Use and dosing of therapeutic agents is extrapolated from dogs and cats. Spontaneous arteriosclerosis is prevalent in rabbits, with an historical incidence of up to 40% in large breeds.
Keywords: arrhythmias, arteriosclerosis, cardiovascular disease, cardiomyopathy, congestive heart failure, rabbit, valvular disease
Cardiac disease has become increasingly recognized in pet rabbits, presumably because pet rabbits are living longer and increasingly sophisticated diagnostic and therapeutic modalities are used for their care. However, despite their frequent use as laboratory models for cardiac disease in people, reports of spontaneous heart disease in rabbits are sporadic, and case numbers are often low. As a result, relatively little is known about the pathogenesis and treatment of naturally occurring heart disease in pet rabbits.
Normal Cardiovascular Structure and Related Anatomy
The rabbit heart is unique in several ways: the tricuspid valve is composed of two rather than three cusps, the aortic nerve is not associated with chemoreceptors but only with baroreceptors, the pulmonary artery and its branches are heavily muscular, and a persistent left cranial vena cava is normally present and drains into the coronary sinus.4, 15, 17 In addition, the right and left auricles are relatively large compared with the rest of the atria, and the ostium of the coronary sinus is quite large.15, 27 Important clinically is the fact that the rabbit’s myocardium has limited collateral circulation and is therefore predisposed to ischemia mediated by coronary vasoconstriction.22
The rabbit’s thoracic cavity is extremely small compared to the rest of its body, and its heart occupies more of the thoracic area relative to other animals.25 The mediastinum and pericardium of the rabbit normally contain fat, which can mimic cardiomegaly in obese animals.26, 27
Examination of the Rabbit with Cardiovascular Disease
History
A thorough general history, including husbandry, diet, and past or present illnesses, should be obtained for rabbits suspected of having cardiac disease. Tachypnea, dyspnea, syncope, anorexia, weight loss, and malaise may be signs of heart disease in rabbits.26
Physical Examination
Take care to minimize the handling of a rabbit in cardiac distress; a complete physical examination and further diagnostic testing must sometimes be delayed until the rabbit is clinically stable. Stress can be minimized by examining the rabbit in a quiet room and moving slowly. Rabbits are a prey species and therefore very sensitive to external stimuli. If necessary, the rabbit may be sedated to minimize the risk of self-injury. Sedation can be achieved with midazolam (0.5–1 mg/kg intramuscularly [IM] or intravenously [IV]) (see also Chapter 37).26, 27, 29 Provide flow-by oxygen as needed if the rabbit is dyspneic or becomes tachypneic with handling. In rabbits suspected of having cardiac disease or respiratory distress, focus the initial examination on observing the respiratory rate and pattern, obtaining the heart rate and rhythm, auscultating the thorax, examining the mucous membranes, and palpating the pulses. The normal heart rate is 200–300 beats/min, and the normal respiratory rate is 30–60 breaths/min26, 27; however, the respiratory rate can approximate the heart rate in stressed animals. Rabbits are obligate nasal breathers; therefore, do not occlude the nares during restraint. Peripheral pulses can often be palpated at the central artery of the ear and should be strong and synchronous with the heartbeat.27 Two heart sounds (S1 and S2) are normally ausculted.27 Referred upper airway sounds often overlie heart sounds and can mimic a murmur; therefore perform auscultation until the respiratory and heart sounds can be resolved.26 Auscultation of any murmur should be followed by echocardiography.27
Rabbits with heart disease may have cyanotic or pale mucous membranes, arrhythmias, or heart murmurs. Rabbits in congestive heart failure often have tachycardia, tachypnea, and labored breathing; however, coughing is uncommon in the authors’ experience. Pulses may be irregular or weak. The entire thorax should be auscultated to localize heart murmurs and detect extra heart sounds (gallop sounds), arrhythmias, and abnormal lung sounds. A pediatric stethoscope allows better localization of heart sounds in rabbits and is preferred for cardiac auscultation, whereas a stethoscope with a larger diaphragm enhances auscultation of the lungs. Auscultatory findings vary among rabbits with congestive heart failure, and these findings are not pathognomonic. The clinician may hear muffled heart and lung sounds with pleural effusion and increased bronchial sounds or crackles with pulmonary edema. However, the absence of crackles should not be used to rule out pulmonary edema in this species. Most rabbits in congestive heart failure have an increased, superficial respiratory pattern. In addition, although heart and lung sounds can be muffled in rabbits with pleural effusion, similar findings can be detected in obese rabbits with significant subcutaneous and intrathoracic fat deposits.27
Diagnostic Methods
Diagnosis of cardiovascular disease is based on a complete history and physical examination, as well as findings of diagnostic tests. Thoracic radiographs, electrocardiography, echocardiography, and routine blood tests are useful in reaching a definitive diagnosis and developing a treatment plan.
Radiography
Thoracic radiography provides critical information in the patient with cardiopulmonary disease—namely, cardiac shape and size, pulmonary pattern, vascular pattern, and other thoracic lesions. The vertebral heart score has been determined for New Zealand white rabbits (n = 50), and for cross, lop, and dwarf breeds (n = 27) by using the method described by Buchanan et al. for dogs.2, 9, 25 However, this measurement in rabbits is not commonly used in clinical practice in the United States.
Congestive heart failure and respiratory disease can be differentiated by evaluating thoracic radiographs. Radiographic findings supporting a diagnosis of cardiac disease are similar to those in other species: cardiac enlargement, pulmonary vascular enlargement, a pulmonary interstitial and alveolar pattern of pulmonary edema, and pleural effusion. However, in the normal rabbit, the cranial heart border is usually difficult to distinguish from the cranial mediastinum.9 Fig. 19.1, Fig. 19.2 show thoracic radiographs of a normal adult rabbit and a rabbit with congestive heart failure, respectively.
Fig. 19.1.
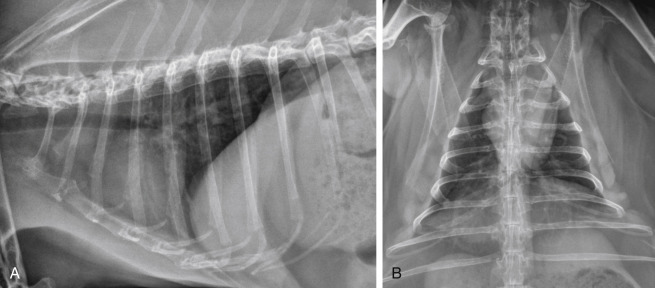
Normal thoracic radiographs of a 6-year-old rabbit
(A) Right lateral projection. (B) Ventrodorsal projection.
Fig. 19.2.
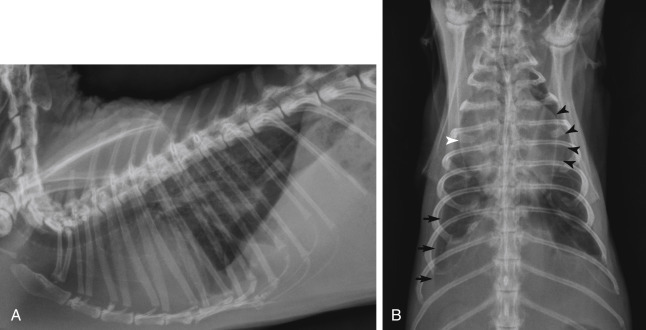
Severe generalized cardiomegaly with congestive heart failure in a 5-year-old male castrated Angora rabbit. (A) In the right lateral projection, the cardiac silhouette is generally enlarged. The carina is elevated owing to left atrial and ventricular enlargement. A marked bronchointerstitial pattern is present in the caudal dorsal lung lobes, which is compatible with pulmonary edema. The lung lobes are mildly retracted and the ventral border of the cardiac silhouette is obscured, indicating mild pleural effusion. (B) In the ventrodorsal projection, a markedly enlarged left auricle is present (black arrowheads). An enlarged right atrium is also present (white arrowhead). An increased bronchointerstitial pattern is evident in the caudal lung lobes, which is more pronounced on the right than the left. Retraction of the lung lobe indicates pleural effusion (black arrows).
Electrocardiography
Electrocardiography is a simple and practical diagnostic test in rabbits with suspected or confirmed cardiac disease. An electrocardiogram (ECG) is critical to diagnosing and managing arrhythmias or syncope. The ECG may also be a helpful addition to the cardiac database. However, one should not use an ECG to assess or detect chamber enlargement or hypertrophy. In most rabbits, the ECG can be recorded with the rabbit awake and under only minimal restraint.9 Record the ECG with the rabbit in sternal recumbency. Use toothless alligator-style electrodes to minimize skin trauma; then place medical-grade alcohol or electrode gel on the clips to enhance conduction. Record tracings with a vertical calibration of 2 cm/mV and a horizontal paper speed of 50 mm/s. Normal rabbit rhythm is sinus and does not include respiratory sinus arrhythmia.26 Spontaneous changes in the QRS complex have been observed in normal rabbits in serial ECG recordings.
Normal ECG values for a variety of pet rabbit breeds have been reported.20, 27 Reference ranges for ECGs are summarized in Table 19.1 .
TABLE 19.1.
Electrocardiographic Values (Lead II) in Clinically Normal Rabbits
| New Zealand White Rabbits (awake)9 (N = 100: 44 M; 56 F) |
Client-Owned Fancy, Fur, and Cross Breeds (awake)20(N = 46: 24 M [8 intact]; 22 F [8 intact]) |
|||
|---|---|---|---|---|
| Parameter | Mean ± SD | Range | Mean ± SD | Range |
| Age, mo | — | 6 (all) | — | 2–84 |
| Body weight, kg | 2.62 ± 0.20 | 2.1–3.0 | — | 1.1–7.9 |
| Heart rate, beats/min | 243 ± 34 | 154– 330 | 264 ± 34 | 198–330 |
| P wave amplitude, mV | 0.05 ± 0.02 | 0.01–0.13 | 0.08 ± 0.02 | 0.04–0.12 |
| P wave duration, s | 0.032 ± 0.004 | 0.021–0.045 | 0.03 ± 0.01 | 0.01–0.05 |
| P-R interval, s | 0.050 ± 0.006 | 0.036–0.072 | 0.06 ± 0.01 | 0.04–0.08 |
| R wave amplitude, mV | 0.18 ± 0.09 | 0.04–0.42 | 0.21 ± 0.09 | 0.03–0.39 |
| QRS duration, s | 0.056 ± 0.004 | 0.043–0.066 | 0.04 ± 0.01 | 0.02–0.06 |
| Q-T interval, s | 0.143 ± 0.012 | 0.115–0.173 | 0.12 ± 0.02 | 0.08–0.16 |
| T wave amplitude, mV | 0.16 ± 0.07 | 0.01–0.51 | 0.11 ± 0.03 | 0.05–0.17 |
| Mean electrical axis | — | −60° to 180°a | 19° ± 31° | −43° to 80° |
In 85% of the rabbits, the mean electrical axis was −30° to 90°.
Echocardiography
Echocardiography provides a sensitive, accurate, noninvasive means of assessing cardiac structure and function. Most rabbits tolerate echocardiography without sedation, making it a practical diagnostic tool. However, in rabbits that are tachypneic or dyspneic, administer oxygen by face mask during restraint. The echocardiographic exam may be performed with the rabbit in lateral or sternal recumbency. Standard views used to evaluate dogs and cats can also be obtained with the rabbit. Because of the rabbit’s rapid heart rate and small size, optimal evaluation requires a high-frequency transducer (e.g., 7.5 MHz) and a high frame-rate ultrasound machine. Two-dimensional and M-mode echocardiography assess cardiac structure, chamber size, wall thickness, and motion as well as extracardiac structures, masses, and pleural effusion. Color-flow, spectral, and tissue Doppler echocardiography assess direction and velocity of blood flow, further defining cardiac conditions with more insight on systolic and diastolic function.
Relative structural measurements are similar to those in other mammalian species—e.g., the diameter of the left atrium is 1 to 1.5 times that of the aorta, the left and right atria are similar in size, and the diameter of the aorta and the pulmonary artery are equivalent.27 In addition, the thickness of the left ventricular free wall approximates that of the interventricular septum and is 2 to 3 times thicker than the right ventricular free wall.27 The coronary sinus, which encircles the atrioventricular junction, is normally quite large in the rabbit and should not be inadvertently interpreted as a congenital anomaly or a structural sign of right heart failure.27
Note that sedative drugs used for restraint, especially alpha-2 agonists such as dexmedetomidine and xylazine, may affect cardiac measurements. Reduced percent fractional shortening, reversal of the E/A ratio (peak velocity blood flow from gravity in early diastole [E wave] to peak velocity flow in late diastole due to atrial contraction [A wave]), decreased heart rate, and other changes have been documented with ketamine at a dose of 50 mg/kg IM and xylazine at 4 mg/kg IM.34 Sedation with ketamine (20 mg/kg) and midazolam (2 mg/kg) given subcutaneously has been shown to be less cardiodepressive.7 Normal echocardiographic values have been published for several breeds of rabbits (TABLE 19.2, TABLE 19.3 ).
TABLE 19.2.
M-mode and 2-dimensional Echocardiographic Measurements in Clinically Normal New Zealand White Rabbitsa,b
| Parameter | Awake(N = 100)9 | Sedatedc(N = 26)7 |
|---|---|---|
| Body weight, kg | 2.6 ± 0.2 | 2.3 ± 0.4 |
| Age, mo | 6 (all) | 4 - 5 |
| Sex | 44 M; 56 F | 26 M; 0 F |
| Heart rate, beats/min | 227 ± 36 | 263 ± 37 (Doppler) |
| IVSd, mm | 2.74 ± 0.51 | 2.65 ± 0.31 |
| IVSs, mm | 4.01 ± 0.70 | 3.63 ± 0.34 |
| LVIDd, mm | 13.28 ± 1.91 | 13.51 ± 1.05 |
| LVIDs, mm | 8.32 ± 1.47 | 8.64 ± 0.82 |
| LVFWd, mm | 2.78 ± 0.54 | 2.25 ± 0.29 |
| LVFWs, mm | 3.56 ± 0.52 | 3.15 ± 0.38 |
| FS, % | 37.17 ± 4.99 | 36.01 ± 4.31 |
| EF, % | 71.12 ± 6.32 | 69.58 ± 5.33 |
| LA, mm | 8.62 ± 1.02 (2D) | 7.49 ± 1.14 |
| Ao, mm | 7.90 ± 0.77 (2D) | 6.57 ± 0.46 |
| LA/Ao | 1.09 ± 0.10 (2D) | 1.15 ± 0.19 |
| EPSS, mm | — | 1.41 ± 0.25 |
Ao, aorta diameter; EF, ejection fraction; EPSS, E-point to septal separation; FS, fractional shortening; IM, intramuscularly; IVSd, interventricular septum in diastole; IVSs interventricular septum in systole; LA, left atrial diameter; LVIDd, left ventricular internal diameter in diastole; LVIDs, left ventricular internal diameter in systole; LVFWd, left ventricular free wall in diastole; LVFWs, left ventricular free wall in systole; SC, subcutaneously.
Values are mean ± standard deviation except for age and sex.
All values are M-mode derived unless indicated otherwise (2D).
Sedated with ketamine (20 mg/kg SC) and midazolam (2 mg/kg SC).
TABLE 19.3.
Doppler Echocardiographic Measurements, Including Tissue Doppler Imaging (TDI) Derived Values, in Clinically Normal New Zealand White Rabbitsa
| Parameter | Awake(N = 100)9 | Awake(N = 20)34 | Sedated7(N = 26) |
|---|---|---|---|
| Body weight, kg | 2.62 ± 0.20 | 2.92 | 2.3 ± 0.4 |
| Age, mos | 6 (all) | 4 | 4 – 5 |
| Sex | 44 M; 56 F | 10 M; 10 F | 26 M; 0 F |
| Heart rate, beats/min | 227 ± 36 | 234 ± 26 | 263 ± 37 (Doppler) |
| Aomax, m/s | 0.75 ± 0.14 | 0.75 ± 0.20 | 0.86 ± 0.12 |
| PAmax, m/s | 0.79 ± 0.16 | — | 0.78 ± 0.12 |
| Mitral E-wave, m/s | 0.64 ± 0.13 | 0.72 ± 0.14 | 0.78 ± 0.15 |
| Mitral A-wave, m/s | 0.52 ± 0.10 | 0.51 ± 0.15 | 0.55 ± 0.11 |
| Mitral E/A | 1.23 ± 0.25 | 1.44 ± 0.28 | 1.44 ± 0.16 |
| IVRT, ms | 36.29 ± 12.77 | 38 ± 5 | 31.42 ± 6.19 |
| DT E, ms | 64.95 ± 17.67 | — | — |
| IVCT, ms | — | 24 ± 11 | 25.00 ± 3.68 |
| LVET, ms | — | 126 ± 14 | 95.72 ± 10.21 |
| Tei index | — | 0.57 ± 0.20 | 0.60 ± 0.10 |
| TDI Lat E′, m/s | — | 0.067 ± 0.019 | 0.16 ± 0.05 |
| TDI Sep E′, m/s | — | 0.050 ± 0.017 | 0.11 ± 0.04 |
| TDI Lat A′, m/s | — | 0.039 ± 0.007 | 0.09 ± 0.03 |
| TDI Sep A′, m/s | — | 0.032 ± 0.009 | 0.08 ± 0.02 |
| TDI Lat S′, m/s | — | 0.055 ± 0.013 | 0.11 ± 0.02 |
| TDI Sep S′, m/s | — | 0.053 ± 0.010 | 0.10 ± 0.02 |
| TDI Lat E′/A′ | — | — | 1.83 ± 0.43 |
| TDI Sep E′/A′ | — | — | 1.55 ± 0.44 |
| Mitral E/TDI Lat E′ (E/E′ lateral) | — | — | 5.24 ± 1.55 |
| Mitral E/TDI Sep E′ (E/E′ septal) | — | — | 7.75 ± 2.69 |
bSedated with ketamine (20 mg/kg SC) and midazolam (2 mg/kg SC).
cSedated with ketamine (2 mg/kg IM) and medetomidine (0.15 mg/kg IM).
Aomax, maximal aortic outflow velocity; DT E, E-wave deceleration time; IM, intramuscularly; IVCT, isovolumetric contraction time; IVRT, isovolumetric relaxation time; LVET, left ventricular ejection time; Mitral A, peak transmitral late diastolic (atrial contraction) velocity; Mitral E, peak transmitral early diastolic velocity; PAmax, maximal pulmonary artery outflow velocity; SC, subcutaneously; TDI Lat A′, peak late diastolic mitral annular velocity from lateral wall; TDI Lat E′, peak early diastolic mitral annular velocity from lateral wall; TDI Lat S′, peak systolic mitral annular velocity from lateral wall; TDI Sep A′, peak late diastolic mitral annular velocity from septal wall; TDI Sep E′, peak early diastolic mitral annular velocity from septal wall; TDI Sep S′, peak systolic mitral annular velocity from septal wall.
Values are mean ± standard deviation except age and sex.
Blood Pressure Measurement
Hypotension is not uncommon in rabbits anesthetized with inhalant agents.11 Doppler-measured arterial blood pressure reportedly correlates well with direct peripheral (auricular artery) blood pressure measurement in the rabbit.11 Using the technique described for a dog or a cat, place a 8.2-MHz frequency ultrasonic Doppler flow detector transducer over a branch of the radial artery on the medial aspect of the carpus, and use a pediatric blood pressure cuff with a width 40%–50% of the circumference of the limb.11 The systolic blood pressure in the clinic is generally 120–180 mmHg.27 Indirect blood pressure measurements <80 mmHg indicate hypotension.11 Rabbits demonstrate circadian patterns in heart rate, as well as both systolic and diastolic blood pressure, with all three parameters being higher at night.31
Diseases and Management
Although the prevalence of cardiovascular disease in rabbits is unknown, the incidence generally increases with age—for example, over 4 years of age.27, 38 Large breeds, such as New Zealand white rabbits, may be overrepresented.38
To date, there are no cardiac drugs approved by the U.S. Food and Drug Administration for use in rabbits. Recommended dosages published in the literature are primarily based on extrapolation from dogs and cats, the authors’ clinical experience, or both.27 Drugs should always be dosed on a milligram-per-kilogram basis, and oral drugs should be given in liquid, not tablet, form.
Congestive Heart Failure
Congestive heart failure is the clinical condition in which pulmonary edema, pleural effusion, hepatomegaly, or all three develop as a result of structural or functional cardiac disease. As a prey species, rabbits may hide signs of illness or debilitation; thus, rabbits with congestive heart failure may be presented after heart disease has become advanced.27 Any rabbit with respiratory abnormalities, particularly in the absence of upper respiratory signs, should be evaluated for heart disease. In some instances, aggressive fluid therapy for treatment of ileus or other abnormalities may result in abnormal breathing and radiographic signs of congestive heart failure.26
The goal of therapy for congestive heart failure is to relieve congestion, control future retention of sodium and fluids, and improve cardiac performance. Various management strategies are used during the acute stage. A common initial treatment protocol is to place the patient in a quiet cage with supplemental oxygen and administer parenteral furosemide (1–4 mg/kg IV or IM every 4–12 hours); nitroglycerin 2% ointment (1/8 inch applied transdermally every 6–12 hours) can be applied to the inner pinna for vasodilation to reduce preload. In a rabbit with pleural effusion, perform therapeutic pleurocentesis if the rabbit is dyspneic.
Long-term therapy of congestive heart failure should include a diuretic (furosemide 1–3 mg/kg by mouth [PO] every 8–24 hours) combined with treatment directed at the underlying precipitating cause.27 Knowledge of the cardiac disease process is the basis of specific treatment of the underlying condition. An angiotensin-converting enzyme (ACE) inhibitor, such as enalapril maleate (0.25–0.5 mg/kg PO every 24–48 hours, begun every 24 hours), is often added to furosemide for the treatment of rabbits with congestive heart failure. Pimobendan (0.1–0.3 mg/kg PO every 12–24 hours), which has both inotropic and vasodilatory properties as well as antiinflammatory effects, may also be used for treatment of systolic dysfunction and myocardial failure.27 During acute and chronic management, it is critical that clinical and radiographic signs, hydration status, appetite, and body weight, as well as serum or plasma blood urea nitrogen, creatinine, and electrolyte concentrations be monitored.
Congenital Heart Disease
Congenital heart disease is rarely reported in rabbits. A ventricular septal defect in an unnamed breed and suspected cor triatriatum dexter in a dwarf lop were both diagnosed with echocardiography.28 , 38 A ventricular septal defect, pulmonary hypertension, and a valvular cyst identified at necropsy have been described in a New Zealand white rabbit.18
Arrhythmias
Although relatively rare, arrhythmias such as atrial fibrillation and ventricular premature complexes have been identified in pet rabbits with underlying cardiomyopathies and congestive heart failure.21, 26, 27 In a rabbit with a clinically relevant arrhythmia, the treatment protocol should be based on ECG findings and clinical signs.
For anesthesia-induced bradycardia, glycopyrrolate may be more effective than atropine sulfate in increasing heart rate, in large part because some rabbits produce atropinesterases.24 , 38 For syncope associated with bradycardia, oral theophylline or pacemaker implantation may be indicated. Although wireless-powered microimplant pacemakers have been used experimentally in New Zealand white rabbits,13 clinical use of a pacemaker has not yet been reported in a pet rabbit.
Supraventricular tachycardias may be treated with oral digoxin or diltiazem. If digoxin is used, monitor the rabbit’s appetite as well as stool production and measure blood levels by ≤8 hours after the last dose.27 The dose may need to be reduced or digoxin discontinued if the rabbit becomes anorexic or develops ileus.38 Use of diltiazem can result in hypotension, so closely monitor rabbits treated with this agent. Ventricular tachyarrhythmias may respond to boluses of intravenous lidocaine.27 , 38 Using dosages determined for dogs, sotalol and mexiletine have also been used anecdotally in rabbits.38
Empirical dosages are published for lidocaine, atropine, and glycopyrrolate (see the Appendix). Other antiarrhythmic drugs have been used at dosages published for cats or ferrets.
Myocardial Disease
Numerous myocardial diseases have been reported in rabbits, and cardiomyopathy is a common postmortem finding in older rabbits.28 Giants breeds may be most susceptible.38 Hypertrophic, restrictive, and dilated forms of cardiomyopathy have all been reported,38 and anecdotally, dilated cardiomyopathy appears to be the form of cardiomyopathy diagnosed most frequently in rabbits.23, 26
The primary causes of cardiomyopathy in rabbits are generally unknown.38 Vitamin E deficiency produces a muscular dystrophy in which the myocardium may be affected.3 Taurine deficiency has not been reported in rabbits.26 However, in a study of 5-month-old albino rabbits with experimentally induced aortic regurgitation and subsequent congestive heart failure, daily supplementation with taurine dosed at 100 mg/kg significantly improved myocardial contractility and decreased mortality.35 There are no published reports of pet rabbits being supplemented with taurine.26
Although infectious myocarditis is rare in pet rabbits, organisms reported to be associated with myocarditis in this species include Pasteurella multocida, Salmonella species, Clostridium piliforme, Encephalitozoon cuniculi, and coronavirus.1, 5, 6, 16Although infection with a coronavirus is used to create a rabbit model of dilated cardiomyopathy, no naturally occurring cases have been reported.1, 4 In experimental studies, myocardial disease has also been induced by inoculation of Trypanosoma cruzi 30 and administration of doxorubicin.37
The alpha-agonist drug detomidine has been associated with myocardial necrosis and fibrosis in New Zealand white rabbits.14 A similar ischemia-mediated process is suggested in association with ketamine/xylazine administration in Dutch belted rabbits.22 Rabbits subjected to intermittent crowding developed an apparent stress-induced cardiomyopathy, which was fatal in 34 of 44 experimental animals.39
Valvular Disease
Mitral and tricuspid insufficiencies are not uncommon and have been identified in pet rabbits, particularly as animals age.23 , 25 , 38 Valvular insufficiencies may be associated with primary valve degeneration, cardiomyopathy, or infection. Progression of the condition leads to volume overload and potential congestive heart failure. A focal murmur is the most common clinical finding. Valvular disease is diagnosed with two-dimensional and Doppler echocardiography (Fig. 19.3 ). Echocardiographic findings most often include thickening of one or both atrioventricular valves, dilation of cardiac chambers, and turbulent regurgitation of blood detected by Doppler scanning.
Fig. 19.3.
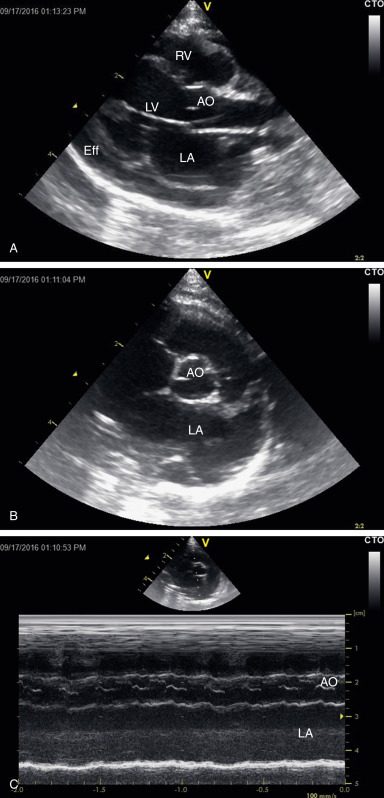
Standard echocardiographic views in rabbits with cardiac disease
(A) Right parasternal long-axis view of a rabbit with dilated cardiomyopathy and pericardial effusion, which is a manifestation of congestive heart failure. Note the dilated left atrium and left ventricle, and the thin left ventricular walls. (B) Right parasternal short-axis view at the level of the heart base in a rabbit with dilated cardiomyopathy. Note the dilated left atrium and auricle. (C) M-mode derived from a right parasternal short-axis view of a rabbit with dilated cardiomyopathy, showing aortic root and left atrial dimensions. LV, Left ventricle; LA, left atrium; RV, right ventricle; RA, right atrium; Ao, aorta; eff, pericardial effusion.
Dental Disease and Abscessation
Vegetative endocarditis due to Haemophilus parainfluenzae was diagnosed post mortem in a 4-year-old rabbit that had presented with a 2-week history of progressive lethargy and weight loss.22a A continuous IV/VI parasternal murmur and an arrhythmia had been ausculted on physical examination. The ECG findings revealed atrial fibrillation conducted with a left bundle branch morphology, and echocardiography showed vegetative and aortic endocarditis and a secondary aortocavitary fistula. Bacteremia was suspected secondary to severe dental disease.
Vascular Disease
Spontaneous arteriosclerosis of the aorta and other arteries has been observed in nearly all rabbit breeds, with historical incidence ranging from 13% in Dutch breeds to 40% or greater in Flemish giant, chinchilla, New Zealand white, and English spot breeds.8, 19 Arterial walls and other soft tissues mineralize; the aortic arch and descending thoracic aorta are most commonly affected. Radiopaque vessels, caused by calcification, may be visible on radiographs.19, 32 Clinical signs, if present, may include lethargy, anorexia, and weight loss. The cause is unknown; however, such variation of incidence by breed suggests a genetic predisposition.8, 19
Hypervitaminosis D, resulting from errors in feed formulation, can result in excessive absorption of dietary calcium and subsequent calcification of blood vessel walls and other soft tissues.10, 33 It has also been suggested that aortic mineralization can occur in hypercalcemic rabbits secondary to renal disease and compromised calcium excretion.10
Pulmonary hypertension associated with high altitude has been reported in a rabbit.12 Lesions included right ventricular hypertrophy and pulmonary artery proliferation from hypoxia. Based on research, rabbits with pulmonary hypertension may respond to phosphodiesterase type-5 inhibitors, particularly vardenafil.36 Systemic hypertension is reportedly rare but may occur with renal failure.27 Rabbits tolerate enalapril well; however, anecdotal reports suggest that they are particularly susceptible to the hypotensive effects of benazepril.29
References
- 1.Alexander L.K., Small J.D., Edwards S., Baric R.S. An experimental model for dilated cardiomyopathy after rabbit coronavirus infection. J Infect Dis. 1992;166(5):978–985. doi: 10.1093/infdis/166.5.978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Buchanan J.W., Bücheler J. Vertebral scale system to measure canine heart size in radiographs. J Am Vet Med Assoc. 1995;206(2):194–199. [PubMed] [Google Scholar]
- 3.Cheeke P.R. In: The Biology of the Laboratory Rabbit. Manning P.J., Ringler D.H., Newcomer C.E., editors. Academic Press; San Diego: 1994. Nutrition and nutritional diseases; pp. 321–333. [Google Scholar]
- 4.Cruise L.J., Brewer N.R. In: The Biology of the Laboratory Rabbit. Manning P.J., Ringler D.H., Newcomer C.E., editors. Academic Press; San Diego: 1994. Anatomy; pp. 47–51. [Google Scholar]
- 5.DeLong D., Manning P.J. In: The Biology of the Laboratory Rabbit. Manning P.J., Ringler D.H., Newcomer C.E., editors. Academic Press; San Diego: 1994. Bacterial diseases; pp. 129–170. [Google Scholar]
- 6.DiGiacoma R.F., Maré C.J. In: The Biology of the Laboratory Rabbit. Manning P.J., Ringler D.H., Newcomer C.E., editors. Academic Press; San Diego: 1994. Viral diseases; pp. 171–204. [Google Scholar]
- 7.Fontes-Sousa A.P., Moura C., Carneiro C.S., et al. Echocardiographic evaluation including tissue Doppler imaging in New Zealand white rabbits sedated with ketamine and midazolam. Vet J. 2009;181:326–331. doi: 10.1016/j.tvjl.2008.02.022. [DOI] [PubMed] [Google Scholar]
- 8.Gaman E.M., Feigenbaum A.S., Schenk E.A. Spontaneous aortic lesions in rabbits: part 3. Incidence and genetic factors. J Atheroscler Res. 1967;7(2):131–141. doi: 10.1016/s0368-1319(67)80075-9. [DOI] [PubMed] [Google Scholar]
- 9.Giannico A.T., Garcia D.A.A., Lima L., et al. Determination of normal echocardiographic, electrocardiographic, and radiographic cardiac parameters in the conscious New Zealand white rabbit. J Exotic Pet Med. 2015;24(2):223–234. [Google Scholar]
- 10.Harcourt-Brown F. Butterworth-Heinemann; Oxford: 2002. Textbook of Rabbit Medicine. [Google Scholar]
- 11.Harvey L., Knowles T., Murison P.J. Comparison of direct and Doppler arterial blood pressure measurements in rabbits during isoflurane anaesthesia. Vet Anaesth Analg. 2013;39(2):174–184. doi: 10.1111/j.1467-2995.2011.00685.x. [DOI] [PubMed] [Google Scholar]
- 12.Heath D., Williams D., Rios-Dalenz J., et al. Pulmonary vascular disease in a rabbit at high altitude. Int J Biometeorol. 1990;34:20–23. doi: 10.1007/BF01045815. [DOI] [PubMed] [Google Scholar]
- 13.Ho J.S., Yeh A.J., Neofytou E., et al. Wireless power transfer to deep-tissue microimplants. http://www.pnas.org/content/111/22/7974 [DOI] [PMC free article] [PubMed]
- 14.Hurley R.J., Marini R.P., Avison D.L., et al. Evaluation of detomidine anesthetic combinations in the rabbit. Lab Anim Sci. 1994;44:472–478. [PubMed] [Google Scholar]
- 15.James T.N. Anatomy of the cardiac conduction system in the rabbit. Circ Res. 1967;20:638–648. doi: 10.1161/01.res.20.6.638. [DOI] [PubMed] [Google Scholar]
- 16.Koller L.D. Spontaneous Nosema cuniculi infection in laboratory rabbits. J Am Vet Med Assoc. 1969;155(7):1108–1114. [PubMed] [Google Scholar]
- 17.Kozma C., Macklin W., Cummins L.M., et al. In: The Biology of the Laboratory Rabbit. Weisbroth S.H., Flatt R.E., Krause S.E., editors. Academic Press; New York: 1974. Anatomy; pp. 50–72. [Google Scholar]
- 18.Li X., Murphy J.C., Lipman N.S. Eisenmenger’s syndrome in a New Zealand white rabbit. Lab Anim Sci. 1995;45:618–620. [PubMed] [Google Scholar]
- 19.Lindsey J.R., Fox R.R. In: The Biology of the Laboratory Rabbit. Manning P.J., Ringler D.H., Newcomer C.E., editors. Academic Press; San Diego: 1994. Inherited diseases and variations; pp. 293–319. [Google Scholar]
- 20.Lord B., Boswood A., Petrie A. Electrocardiography of the normal domestic pet rabbit. Vet Rec. 2010;167:961–965. doi: 10.1136/vr.c3212. [DOI] [PubMed] [Google Scholar]
- 21.Lord B., Devine C., Smith S. Congestive heart failure in two pet rabbits. J Small Anim Prac. 2011;52:46–50. doi: 10.1111/j.1748-5827.2010.01016.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Marini R.P., Li X., Harpster N.K., et al. Cardiovascular pathology possibly associated with ketamine/xylazine anesthesia in Dutch belted rabbits. Lab Anim Sci. 1999;49:153–160. [PubMed] [Google Scholar]
- MartelArquette A, Tjostheim S.S, Carlson J,, Mans C, et al. Aortocavitary fistula secondary to vegetative endocarditis in a rabbit. J Vet Cardiol. 2019;21:49–56. doi: 10.1016/j.jvc.2018.08.003. [DOI] [PubMed] [Google Scholar]
- 23.Mitchell E.B., Zehnder A.M., Hsu A., Hawkins M.G. Pimobendan: treatment of heart failure in small mammals. Proceed 29th Annu AAV Conf & Expo with AEMV. 2008:71–79. [Google Scholar]
- 24.Olson M.E., Vizzutti D., Morck D.W., et al. The parasympathetic effects of atropine sulfate and glycopyrrolate in rats and rabbits. Can J Vet Res. 1994;58:254–258. [PMC free article] [PubMed] [Google Scholar]
- 25.Onuma M., Ono S., Ishida T., et al. Radiographic measurement of cardiac size in 27 rabbits. J Vet Med Sci. 2010;72(4):529–531. doi: 10.1292/jvms.09-0390. [DOI] [PubMed] [Google Scholar]
- 26.Orcutt C. In: BSAVA Manual of Rabbit Medicine. Meredith A., Lord B., editors. BSAVA; Quedgeley, UK: 2014. Cardiovascular disorders. [Google Scholar]
- 27.Pariaut R. Cardiovascular physiology and diseases of the rabbit. Vet Clin North Am Exot Anim Pract. 2009;12:135–144. doi: 10.1016/j.cvex.2008.08.004. [DOI] [PubMed] [Google Scholar]
- 28.Redrobe S. Imaging techniques in small mammals. Sem Avian Exot Pet Med. 2001;10:195. [Google Scholar]
- 29.Reusch B. Investigation and management of cardiovascular disease in rabbits. In Pract. 2005;27:418–425. [Google Scholar]
- 30.Rossi M.A. Microvascular changes as a cause of chronic cardiomyopathy in Chagas’ disease. Am Heart J. 1990;120:233–236. doi: 10.1016/0002-8703(90)90191-y. [DOI] [PubMed] [Google Scholar]
- 31.Sato K., Chatani F., Sato S. Circadian and short-term variabilities in blood pressure and heart rate measured by telemetry in rabbits and rats. J Auton Nerv Syst. 1995;54(3):235–246. doi: 10.1016/0165-1838(95)00016-q. [DOI] [PubMed] [Google Scholar]
- 32.Shell L.G., Saunders G. Arteriosclerosis in a rabbit. J Am Vet Med Assoc. 1989;194:679–680. [PubMed] [Google Scholar]
- 33.Stevenson R.G., Palmer N.C., Finley G.G. Hypervitaminosis D in rabbits. Can Vet J. 1976;17(2):54–57. [PMC free article] [PubMed] [Google Scholar]
- 34.Stypmann J., Engelen M.A., Breithardt A.K., et al. Doppler echocardiography and tissue Doppler imaging in the healthy rabbit: differences of cardiac function during awake and anaesthetised examination. Int J Cardiol. 2007;115:164–170. doi: 10.1016/j.ijcard.2006.03.006. [DOI] [PubMed] [Google Scholar]
- 35.Takihara K., Azuma J., Awata N., et al. Beneficial effect of taurine in rabbits with chronic congestive heart failure. Am Heart J. 1986;112(6):1278–1284. doi: 10.1016/0002-8703(86)90360-1. [DOI] [PubMed] [Google Scholar]
- 36.Toque H.A., Teixeira C.E., Priviero F.B., et al. Varendafil, but not sildenafil or tadalafil, has calcium-channel blocking activity in rabbit isolated pulmonary artery and human washed platelets. Br J Pharmacol. 2008;154:787–796. doi: 10.1038/bjp.2008.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Van Vleet J.F., Ferrans V.J. Clinical and pathologic features of chronic adriamycin toxicosis in rabbits. Am J Vet Res. 1980;41:1462–1469. [PubMed] [Google Scholar]
- 38.Varga M. 2nd ed. Butterworth-Heinemann; Edinburgh: 2014. Cardiorespiratory disease. Textbook of Rabbit Medicine. [Google Scholar]
- 39.Weber H.W., Van Der Walt J.J. Cardiomyopathy in crowded rabbits: a preliminary report. S Afr Med J. 1973;47(35):1591–1595. [PubMed] [Google Scholar]