

Abstract
The rapid growth and diffusion of digital media technologies has changed the landscape of market segmentation in the last two decades, including its use in promoting prosocial and behavior change. New, population-specific and culturally appropriate prevention strategies can leverage the potential of digital media to influence health outcomes, especially for the greatest users of digital technology, including youth and young adults. Health behavior change campaigns are increasingly shifting resources to social media, creating opportunities for innovative interventions and new research methods. This article examines three case studies of digital segmentation: (1) tobacco control from the Truth Initiative, (2) community-based public health programs from the Centers for Disease Control and Prevention, and (3) substance use (including opioids) and other risk behavior prevention from Public Good Projects. These case studies of recent digital segmentation efforts in the not-for-profit, government, and academic sectors show that it increases reach and frequency of messages delivered to priority populations. The practice of digital segmentation is rapidly growing, shows early signs of effectiveness, and may enhance future public health campaigns. Additional research could optimize its use and effectiveness in promoting prosocial and behavior change campaign outcomes.
Keywords: behavior change, digital media, mobile phones, public health, segmentation, social marketing
Commercial marketers have long recognized that not all consumers are alike. Consumers differ in terms of demographic characteristics, such as age or gender, geographic location (which may affect their access to products and services, as well as social environment), behavioral and lifestyle factors, and psychographic factors (psychological characteristics, beliefs, and attitudes). (Armstrong and Kotler 2005) define market segmentation as “dividing a market into distinct groups of buyers who have distinct needs, characteristics, or behavior and who might require separate products or marketing mixes” (p. 54). The purpose of segmentation is to align the marketer’s offer with the right consumer for whom the product or service is most relevant.
This approach has been widely applied in social marketing (i.e., the use of marketing theory, skills, and practices to achieve social change) for public health objectives (Evans, 2016; French & Gordon, 2015). For example, the Heart Truth campaign was created in response to the problem of heart disease in women (Long, Taubenheim, Wayman, Temple, & Ruoff, 2008). The Heart Truth developed a strategy for raising awareness of heart disease risks among 40 to 60 year olds and encouraged them to take action to reduce heart disease risk factors.
(Evans 2016) noted four criteria for effective segmentation: (1) tight definition based on a specific set of factors such as demographic and psychographic, (2) ability to measure the segments to estimate size and likely reach within the population to make a meaningful difference, (3) being reachable through communication in an affordable way, and (4) be substantial enough (large enough) to potentially have a meaningful public health impact.
The rapid growth and diffusion of digital media technologies has changed the landscape of segmentation in the last two decades (Evans, 2016). New, population-specific and culturally appropriate prevention strategies could leverage the potential of digital media to influence health outcomes, especially for the greatest users of digital technology, including youth and young adults. Health behavior change campaigns are increasingly shifting resources to social media such as YouTube, Twitter, Facebook, Instagram, and Snapchat, as these are the most widely used channels among youth and young adults (Pew Research Center, 2018). Recent studies show that social media can be an effective tool both to promote healthy behaviors and to counter unhealthy product marketing, such as tobacco industry product promotion, and may serve as effective campaign platforms (Duke et al., 2014). However, there is relatively little published data on exposure to and evaluations of large-scale health behavior change campaigns based on digital channels. Social marketing as a theoretical framework for social and behavior change suggests that digital channels will be a central strategy to maximize the reach and effectiveness of future campaigns (French & Gordon, 2015).
Health behavior change campaigns, especially those focused on high users of digital platforms, such as youth and young adult target audiences, are being encouraged to reallocate substantial resources to deliver messages online (Evans, 2016). Within digital platforms, primarily social networking services, interactivity or engagement—a measure of audience awareness, dialogue, or behavior—has been treated as a key performance indicator and a predictor of successful campaign outcomes (Hopp & Gallicano, 2016; Smith & Gallicano, 2015; Taylor & Kent, 2014). Recent work has operationalized engagement metrics into tiers: low (likes, awareness), medium (created or shared content), and high (subsequent offline activities; Neiger et al., 2012). Engagement is a function of both initial exposure to digital content and the process of behavioral retargeting—a form of online targeted advertising by which online advertising is targeted to consumers based on their previous Internet actions. Delivering traditional paid media (TV, radio, print, out of home), coupled with digital media, can increase the likelihood of audience exposure (Hornik, 2016). However, there are no standards associated with levels of paid digital media, audience exposure, and engagement over time (Hornik, 2016). As a result, additional information could help inform how and to what extent digital message exposure and engagement influences behavior over time, across platforms, and among multiple devices for the same individuals.
Why is this work significant? As more and more private and public sector marketing relies on digital platforms, the need to understand behavior in segments that predict consumer and program engagement and outcomes based on online behavioral characteristics increases. The traditional segmentation variables discussed earlier, while still relevant, will increasingly be just one part of a larger mosaic of predictive factors. Segmentation based on digital behavior will become more and more important in predicting engagement with online advertising and behavior change campaigns, and thus will be increasingly predictive of achieving campaign outcomes.
Digital segmentation—the ability to sort and reach audiences in a targeted manner using digital technologies—is still in its infancy as a public health practice but is growing rapidly. This article explores three case studies from the public, philanthropic, and not-for-profit sectors focused on the use of digital segmentation for behavioral and social change. We present examples of digital segmentation and message targeting from the truth campaign to prevent smoking among youth and young adults; communities funded by the Centers for Disease Control and Prevention (CDC) to address chronic disease; and the Public Good Projects’ (PGP) digital segmentation efforts across multiple subject areas, including opioid misuse. These case studies were chosen because they illustrate public health digital segmentation efforts, suggest future directions in the field, and point to the opportunity for research and digital campaign evaluations. While the cases are diverse, they share the common factor of illustrating the methods by which digital segmentation may be used for social and behavior change. Each was presented by an author of the current article at the 2018 Digital Health Promotion Summit held in Washington, D.C.
Case Studies
Case Study 1: Truth
Truth, the national mass media antitobacco campaign aimed at preventing tobacco use among youth ages 12 to 17 years, was launched in 2000 by Truth Initiative (formerly American Legacy Foundation; Vallone et al., 2017). Since its launch, truth primarily used television and radio advertisements to reach its intended audience. By 2014, the media landscape shifted dramatically with the rise of internet advertising, the growth of mobile devices, and increasing engagement with social media, prompting truth to seek new pathways to deliver its message (Verhoef, Kannan, & Inman, 2015).
To ensure that the target audience had multiple opportunities to take part in the movement, Truth Initiative employed an omni-channel marketing approach to the campaign. Unlike single-channel approaches such as television advertisements, omni-channel marketing uses the latest technology to deliver messages on multiple fronts, including mobile devices, through social media, and dedicated campaign websites (Verhoef et al., 2015). To best meet the needs of the target generation and evolving media landscape, the latest iteration of the truth campaign has gone beyond television advertisements to deliver digital messages through multiple platforms, including banner ads, online video ads, paid promotions on social media, truth-branded social media pages, and a campaign website (Vallone et al., 2018). Drawing from formative and psychological research showing that the target generation valued autonomy, identity formation, and connections with others, the campaign called on youth to join a social movement to end smoking (Hair et al., 2018). An evaluation of the campaign demonstrated a dose–response relationship between awareness of truth messages and changes in antitobacco attitudes, support for a social movement to end smoking, and intentions not to smoke (Vallone et al., 2018). Thus, it was imperative that youth not only see these ads but that they have the chance to frequently engage with the content.
Crucially, an omni-channel approach can integrate users’ online behavior in order to provide multiple opportunities, or touchpoints, for the target audience to take in the message (Verhoef et al., 2015). These touchpoints allow a marketer’s message to meet the customer where they are, so that whether the audience likes to discuss a social movement online through their social media accounts, prefers to watch YouTube videos, or seeks out content that asks them to join a larger cause, the message has the chance to get through to the audience (Vallone et al., 2016).
Audience Segmentation.
Using an audience-first approach, which first builds audience segments for the message, analyzes which messages connect most successfully to the target audience, and adjusts messaging based on analysis to make meaningful connections more quickly, the truth campaign sought to iteratively adjust messages for maximum impact, as shown in Figure 1 (Favatas, 2018).
Figure 1.
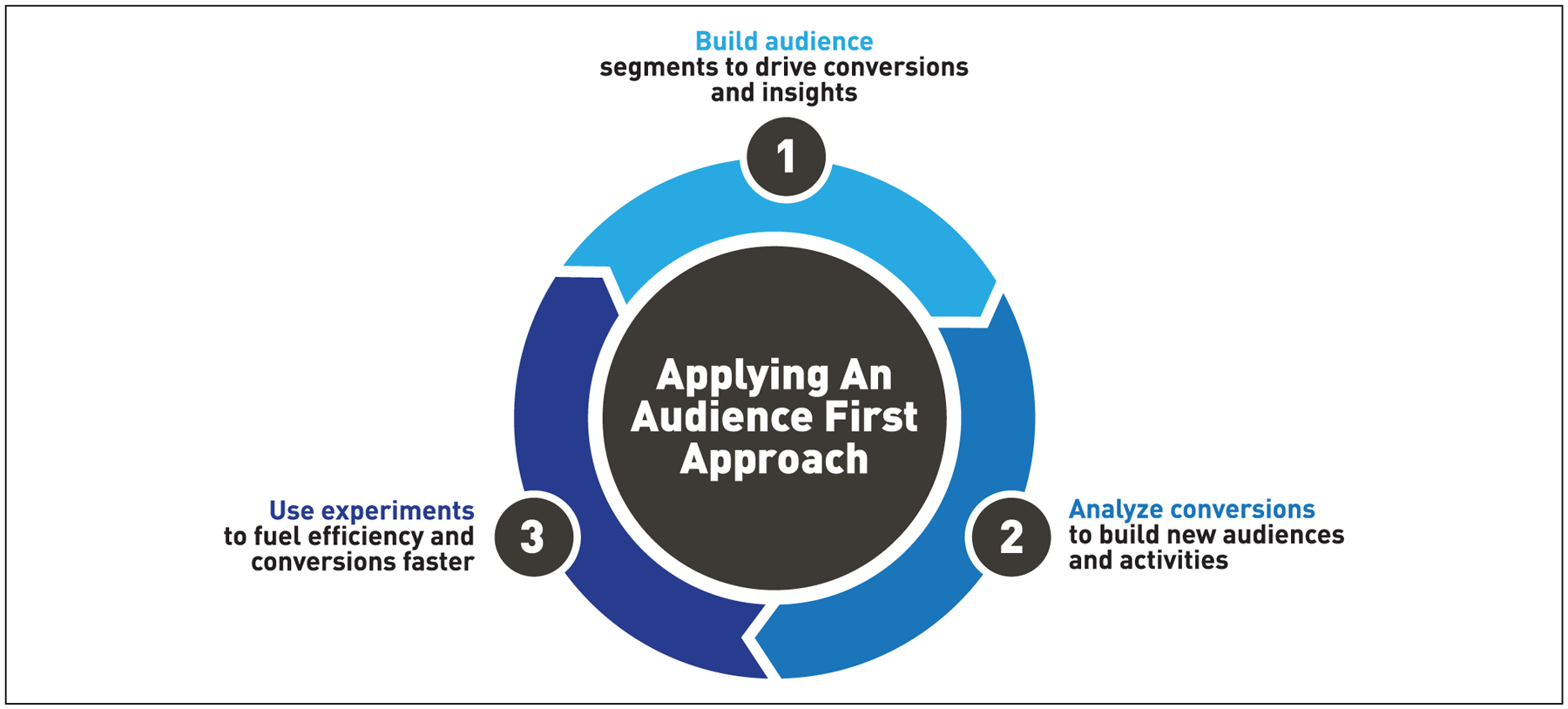
Audience-first model.
In order to establish a baseline for message efficacy, Truth Initiative identified baseline segments, which included 25%, 50%, 75%, and 100% video completion, as well as media engagers (i.e., those who click on display or video units), and people who join the movement on signup forms on thetruth. com. Participants opted-in and the campaign anonymously monitored their level of engagement with truth content (Favatas, 2018). Since previous research established that changes in attitudes, knowledge, and beliefs translate into changes in behavior (Hair et al., 2018), it was important to measure the number of people who either complete watching the entire message or take a message-directed action, such as joining the campaign or posting about it to social media (Vallone et al., 2016).
Testing Completion.
Truth Initiative then designed a test to determine which video length and message would generate the highest number of video completions. Over a 2-week period, four million impressions, or unique video views, were observed and the percentage of video viewed (25%, 50%, 75%, 100%) was measured. Video messages were produced in both 15-second and 30-second versions and in two different creative themes for a total of four videos. Each audience member was exclusively sent only one video message and video length in order to test the efficacy of both message and length (Favatas, 2018).
Testing revealed that audiences reached higher completion rates with the shorter 15-second videos—a crucial finding in designing subsequent messages. Content creators were then able to front-load messages with the most important information so that even longer advertisements could ensure that key messages were more likely to be seen. Another key observation was that, for those exposed to the longer format videos (30 seconds), on average people completed at least 75% of the video before dropping off. This suggested during the test that subjects were willing to consume up to 22.5 seconds of a video, which opened up new opportunities to test longer format videos where a forced completed exposure is required (e.g., user cannot skip a video after 5 seconds).
Testing Conversion.
Truth Initiative also sought to understand the message content and call-to-action most likely to deliver the highest number of conversions, or follow-throughs on an intended action, such as visiting the truth campaign website or posting to social media. Researchers segmented audiences based on their percentage of video completion so that that those who watched 100% of a video and those that only completed 25% of a video were separated into their own groups and were then shown a video to determine which would be most effective for conversion. Eight advertisements used one of four key facts about the tobacco industry’s targeting of people with mental health issues or those in the military and tobacco use rates of those populations. Results showed that only two facts and two content messages comprised fully half of the study’s conversions. Messages focused on (1) the impact of smoking on a smoker’s lifespan, (2) the amount of money Big Tobacco earned, and (3) the high prevalence of smoking among populations living with mental health conditions were the most successful at driving conversions. Overall, messages highlighting the effects of smoking on individuals as well as detailing industry tactics were more impactful than messages which focused more narrowly on a subpopulation. Knowing which fact and message theme were mostly likely to spur a subsequent action was critical in designing future messages to ensure that engagement leads to changes in attitude.
Case Study 1 Conclusions.
Digital segmentation allowed Truth Initiative to capitalize on the type, content, and length of video most likely to attract a young audience, enlist them in the fight against tobacco, and, ultimately, encourage a shift in attitude and behavior that either prevents or discourages tobacco use. The next step is to examine how type, content, and video length are related to changing these attitudes and beliefs.
Case Study 2: Using Communication to Support Local Public Health Programs
From September 2014 through September 2017, the CDC funded 88 communities through two cooperative agreements, Racial and Ethnic Approaches to Community Health (REACH) and Partnerships to Improve Community Health (PICH). Communities focused on chronic disease prevention topics such as nutrition, physical activity, tobacco, and clinical and community linkages at the local level (CDC, 2014a, 2014b). Recognizing the importance of communication to public health programs (Frieden, 2014; National Association of County and City Health Officials, 2015), CDC asked communities to use communication to share messages, activities, and success about programs with public, partner, and stake holder audiences (CDC, 2014a, 2014b). To help communities successfully use communication, CDC provided guidance, resources, and technical assistance following a three-step approach (see Figure 2).
Figure 2.
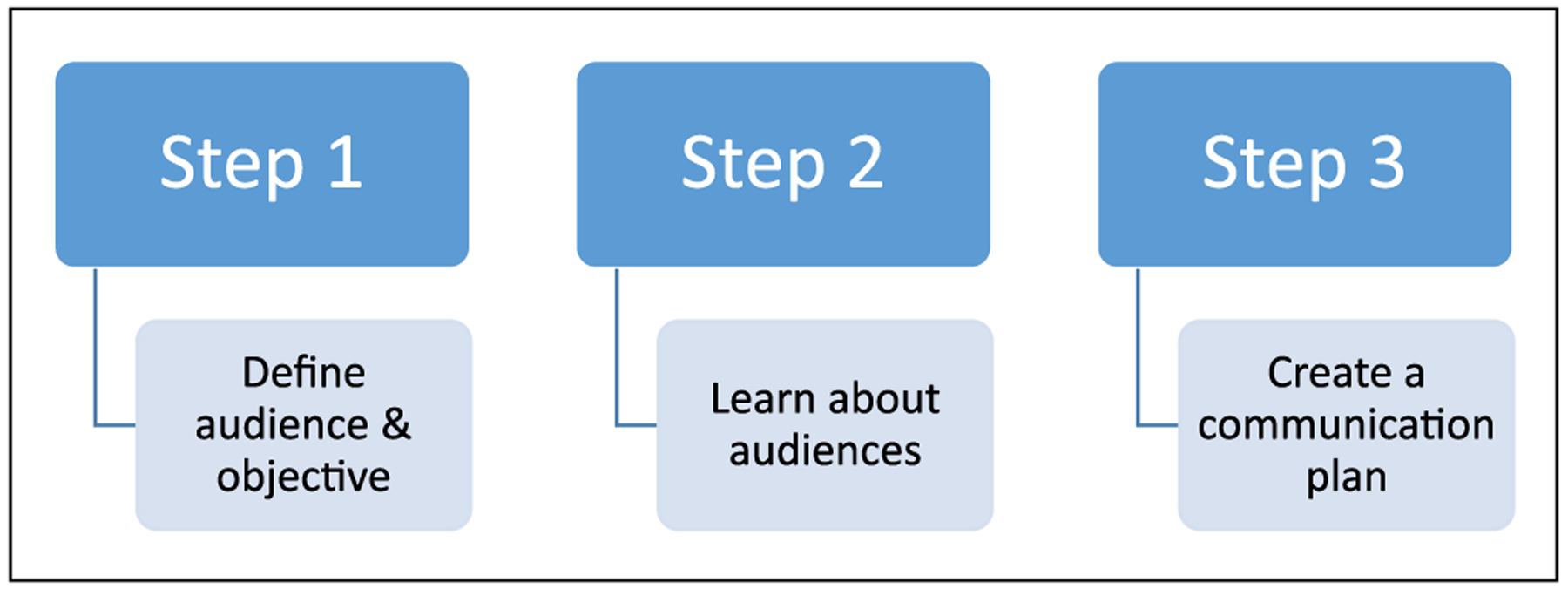
Approach to using communication to support community health work.
First, CDC asked communities to define their audiences and objectives. The intent was to identify and segment audiences by age, ethnicity, or other factors early in communication planning (Woolf et al., 2015). Communities also linked their communication activities to a larger program objective (e.g., Increase the number of SNAP recipients in Riverside who will have access to redeem SNAP benefits at farmers markets from 0 to 29,000 by September 2015). This ensured communication activities supported program efforts.
Second, CDC encouraged communities to learn about their audiences through focus groups, interviews, needs assessments, surveys, market research data, or other available data. Learning about audiences and their values, needs, or preferences informed communication activities and the overall program. Communities with limited resources and experience were also encouraged to work with partners to learn about their audiences. This was important since partners came from different sectors (e.g., academia, business, health care, local media outlets, transportation) and had different data or knowledge about audiences.
Third, CDC asked communities to create a communication plan. CDC provided a template or communication planning tool to help communities identify the program objective, communication objective, audience, activities, person or group responsible, financial and in-kind resources, and evaluation metrics (CDC, 2018). Communities created and used an annual communication plan to guide their communication activities. CDC also provided feedback on the plans and encouraged communities to review and update the plan throughout the year.
Here are a few REACH and PICH community examples of segmenting audiences for digital and social media efforts based on individual conversations and performance monitoring information. The Schenectady County Public Health Services (Schenectady County, NY) and Heart of Florida Health Center (Marion County, FL) both launched mobile phone applications to support healthy food efforts intended for low income and community residents. Marimn Health and the Coeur d’Alene Tribe in Idaho used Facebook to share videos using basic movements and cultural aspects of Pow Wow dancing to promote physical activity among Tribal members. The Cook County Department of Public Health (Cook County, IL) used geo-targeted advertisements to reach residents in specific areas of the county and provide information on healthy foods and physical activity. The Kent County Health Department (Kent County, MI) used digital and social media advertisements to increase Facebook page interactions and promote physical activity with community members. Solano County Public Health (Solano County, CA) used digital advertisements to reach moviegoers and promote healthy food and tobacco-free places in their community.
Communities also worked with partners on communication efforts. The Cabarrus Health Alliance (Cabarrus County, NC) worked with a local minor league baseball team to promote new healthy concessions. The baseball team posted information on their Facebook page to reach the audience, and this helped increase visits and followers to the health department’s Facebook page. The Cuyahoga County Board of Health (Cuyahoga County, OH) worked with radio stations to promote their work on shared-used facilities and healthy food. Radio stations used Facebook Live and Instagram to talk about the work; this helped reach the intended audience.
Case Study 2 Conclusions.
Using the three-step approach, PICH and REACH communities identified and segmented their audience(s) for digital and social media efforts. Communication plans helped connect communication efforts to program objectives. Working with partners offered another way to reach audiences through a different channel and trusted messenger. Using this approach, other communities can successfully plan and implement audience-specific digital and social media efforts to support program efforts.
Case Study 3: The Public Good Projects
Media sources (television, radio, print news and magazines, online news, online video, blogs, and social media) now produce quintillion bytes of data a day (DOMO, 2018; IBM, 2019). Cisco Systems estimates that monthly Internet traffic in North America will reach 44.7 EB (EB is short for Exabytes. One billion Gigabytes [GB] equals one Exabyte) by 2021 (Cisco Systems, 2017). This increase is the result of a 20% compound annual growth rate in Internet traffic, which is remarkable given that 90% of the world’s data was created in the last 2 years (IBM, 2019).
Public health and health care have used “big data” from media sources (Akay, Dragomir, & Erlandsson, 2015). However, the majority of existing public health and health care research has focused on social media data, used by university-based health researchers to assess public opinion, organization’s social media use, evaluation of information accuracy, and disease surveillance (Fung, Tse, & Fu, 2015; Paul & Dredze, 2017; Tang, Bie, Park, & Zhi, 2018). The topic is of interest with approximately 2,100 peer-reviewed articles referencing “Twitter” or “Facebook” and “health” published since 2008 (National Center for Biotechnology Information, 2018). Many schools and programs of public health offer degree programs in Informatics, which may include social media data mining (Association of Schools & Programs of Public Health, 2018). PGP’s experience is that industries (e.g., retailers, hospitality, travel) routinely perform media monitoring and explore hypotheses (Betancourt, 2010).
Within academia, researchers commonly use Twitter data when looking for population-level insights (Sinnenberg et al., 2017), routinely employing between 1% and 10% of Twitter’s available data. Twitter allows third parties to download 1% of its data free of charge and makes these data easy for individuals to download without technical training. These two factors appear to have driven the field of media monitoring more than the need to show true representativeness, such as by triangulating data sources or using larger more robust datasets. Important research, such as the health information needs of the 2014 to 2016 Ebola outbreak (Odlum & Yoon, 2017), sentiment regarding diet and physical activity (Nguyen et al., 2017), real-time disaster response (Charles-Smith et al., 2015; Imran, Castillo, Lucas, Meier, & Vieweg, 2014), and illegal sales of opioids (Mackey, Kalyanam, Katsuki, & Lanckriet, 2017), have drawn conclusions from small percentages of one social media site’s data (Twitter). Broadcast television, radio, print news and magazines, online news, and social media sites beyond Twitter and Facebook are rarely studied.
Public Health Monitoring.
PGP collaborated with a variety of organizations, such as Kaiser Permanente; the West Orange Healthcare District; the National Academies of Sciences, Engineering, and Medicine; multiple state and local health departments; as well as the corporations Google, Facebook, and Zignal Labs, to advance public health monitoring techniques (The Public Good Projects, 2019a). PGP uses a combination of technologies to collect public data from websites, online video, social media (including 100% of Twitter), and other sources, to provide previously unavailable retrospective and real-time data for monitoring of issues important to public health. These data allow analysts to determine the public’s knowledge, attitudes, and behaviors related to a specific health topic, the source and spread of facts and misinformation, differences in discourse by location, and uncover shifts in conversation following major events. Analysts can report trends over time to examine and predict how issues evolve. Additionally, PGP is able to identify and monitor bots (automated computer programs) and botnets (multiple bots controlled by one or many outside sources; United States Computer Emergency Readiness Team, 2011), which may be used to spread misinformation.
PGP’s Opioid Monitoring.
From September 2017 to October 2018, PGP analyzed more than 14 million individual mentions of keywords related to the opioid crisis. These mentions were collected across all previously described media types. Keywords include brand and generic names of opioids, as well as “street names” of opioids, or slang terms referring to illicit opioids. Analyses were conducted using a combination of machine learning, natural language processing, and human coding using content analysis methodologies (i.e., interpreting and coding text material). PGP determined the United States public is predominately exposed to messaging that frames the opioid crisis in six distinct ways (The Public Good Projects, 2019b):
A policy debate occurring primarily among policy makers
The toll on families due to loss or addiction of a loved one
A criminal justice issue, focusing on punitive measures
The culpability of the health care system, and in particular, physicians
The culpability of the pharmaceutical industry
Frustration by those experiencing chronic pain, who believe they are reliant on opioids
Given that two of the six themes in the national dialogue relate to the culpability of the health care system and pharmaceutical industry, PGP concluded that erosion of trust in authorities and institutions may be of serious concern to those entrusted with the public’s welfare (The Public Good Projects, 2019b). In addition to these six frames, PGP stated that little information was tailored for rural populations. Analyses also showed 18 to 25 year olds were not exposed to or shared messages, but older populations saw and shared messages regarding chronic pain (The Public Good Projects, 2019b). PGP analyses also indicated opioids may be sold illegally across many social media and websites, with different strategies employed on different sites and channels. Finally, PGP concluded the public receives very little information providing tangible calls-to-action (The Public Good Projects, 2019b). This extends beyond calls to learn more and educate oneself on the dangers of opioids. The scale of the opioid crisis necessitates local solutions and local calls-to-action (e.g., reducing exposure to opioids, overdose response). If the majority of Americans are viewing the opioid crisis as a distant policy debate, which the data seem to support, efforts to localize and personalize may help slow the drug overdose epidemic.
Case Study 3 Conclusions.
Public media data can provide valuable information to researchers and health authorities regarding how public health topics are framed, who frames such topics, who receives messages related to those topics, and how those messages impact the conversation of the public and particular audience segments. Considering that such data are available, schools of public health and public health organizations may need to adapt course curriculums and professional training programs to bridge the skills gap between the public and private sectors. A limitation of the PGP example is that information is only on their website and a peer reviewed study or white paper is not available at this time. PGP states on their website that they are the only organization to continuously monitor multiple topics of public health concern across all publicly available media types. This monitoring is resource intensive and requires advanced public health and data science expertise.
Discussion
The three case studies show that digital segmentation for health promotion is becoming a widespread practice across the not-for-profit, government, and academic sectors. Community-based, regional, and national organizations in the United States are employing digital segmentation to customize, increase reach and frequency of exposure, and maximize impact of health promotion and disease prevention messages. These efforts are reaching priority populations ranging from low-income individuals, to multicultural audiences, to numerous groups facing health disparities. Digital segmentation is growing and becoming standard practice for public health.
Some additional themes about digital segmentation practice emerge from the case studies. First, digital segmentation enables public health organizations to increase reach and frequency of exposure to messages over time, making them highly relevant for emerging and acute health crises. The Truth Initiative case showed that large number of digital impressions can be generated in a matter of weeks to combat threats such as smoking. Maximizing impressions can spread awareness of health threats and potentially create diffusion effects that can assist public health in combating emergent crises (Neiger et al., 2012).
Second, digital segmentation, and tracking of exposure among segmented populations, enables public health organizations to gain valuable audience insights. Media consumption, propensity to view online content, time spent viewing videos, and engagement metrics (digital media behavior and subsequent online and offline outcomes) can all be monitored. The PGP case demonstrated other ways to gain insights from real-time public data, thus potentially leading to improved programming and content. This information can help public health organizations improve public health knowledge, increase prevention and health promoting behaviors, and combat the effects of competing messages delivered from industry through digital channels (Stephen, 2016). Such industry efforts may reduce public trust in digital marketing, and countermarketing using digital segmentation may have the added benefit of counteracting this erosion of trust. Audience insight is a cornerstone of social marketing, and digital segmentation shows significant promise to advance the state of science in how to effectively reach and influence multiple audiences for pro-social and behavior change (Google Developers, 2018).
Third, digital segmentation creates opportunities for synergies between public health organizations and the digital technology industry. Each of the case studies highlights different ways in which the implementing organizations leveraged technology platforms such as Google, Facebook, Twitter, as well as partners in health care (e.g., Kaiser Permanente), and in local communities using digital segmentation to achieve programmatic objectives. Collaborations between public health and digital technology companies offer future opportunities to increase the reach and effectiveness of health interventions, and to expand and deepen the potential impact of corporate social responsibility and philanthropic efforts (Wang, Tong, Takeuchi, & George, 2016).
There are important ethical considerations for public health organizations using digital segmentation. The same audience insights that can improve digital programming and content also have potential to compromise individuals’ privacy, including the most vulnerable among us. As seen in recent efforts by foreign and domestic U.S. actors to influence public opinion, attitudes, and behaviors ranging from health to civic engagement, digital audience insights cut both ways (Director of National Intelligence, 2018). Public Health has a significant opportunity to lead future efforts to ensure that digital segmentation is used for prosocial objectives, which will promote public trust in their use and serve a constructive purpose in improving social change programs and promoting constructive online dialogue. The CDC community-engagement examples highlight important strategies and approaches to building community buy-in and co-creation of digital segmentation and sharing of insights for mutual benefit.
One approach to building support for, and effective use of, digital segmentation strategies is to promote their inclusion in professional health-related conference programs and online forums. Content presented on digital segmentation should include discussion of its ethical use. These efforts may serve to enhance message source credibility of public health digital marketing (Kumkale, Albarracín, & Seignourel, 2010).
Finally, more rigorous digital media research and campaign evaluations could aid understanding and refinement. There is a dearth of longitudinal, experimental, and quasiexperimental studies that (1) effectively measure the dosage and exposure of segmented audiences to digital media and (2) evaluate health and behavioral outcomes in relation to digital segmentation efforts. A recent meta-analysis demonstrated there was a positive relationship between social media use and civic participation cross-sectionally (Boulianne, 2015). Yet this effect was not found in a longitudinal study design. Others have pointed to a need to focus efforts beyond “likes” and toward individual and/or network characteristics as predictors of engagement (Jobs & Gilfoil, 2014; John, Emrich, Gupta, & Norton, 2017; Liang & Fu, 2015). Overall, additional information can inform how and to what extent digital message exposure and engagement influences behavior over time, across platforms, and among multiple devices for the same individuals.
Conclusions
Digital segmentation, widely practiced in commercial marketing and near omnipresent online, is now rapidly growing as a standard public health practice. The use of digital segmentation may enhance health behavior change campaigns. Recent digital segmentation efforts in the not-for-profit, government, and academic sectors show that it increases reach and frequency of messages delivered to priority populations. There is an opportunity to enhance optimization its use and effectiveness in promoting health behavior change campaign outcomes.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplement Note
This article is part of the Health Education & Behavior supplement issue, “Advancing the Science and Translation of Digital Health Information and Communication Technology.” The printing and dissemination of the supplement was supported by the Office of Behavioral and Social Sciences Research, National Institutes of Health (Contract No. HHSN276201800167P). No federal funds were used in the development of these supplement manuscripts, and the views and findings expressed in them are those of the authors and are not meant to imply endorsement or reflect the views and policies of the U.S. Government. The entire supplement is available open access at https://journals.sagepub.com/toc/hebc/46/2_suppl.
References
- Akay A, Dragomir A, & Erlandsson B (2015, December 18). Mining social media big data for health. IEEE Pulse. Retrieved from https://pulse.embs.org/november-2015/mining-socialmedia-big-data-for-health [Google Scholar]
- Armstrong G, & Kotler P (2005). Marketing: An introduction (7th ed.). Upper Saddle River, N.J: Prentice Hall. [Google Scholar]
- Association of Schools & Programs of Public Health. (2018). Academic program finder. Retrieved from https://www.aspph.org/program-finder/
- Betancourt L (2010, March 2). How companies are using your social media data. Retrieved from https://mashable.com/2010/03/02/data-mining-social-media
- Boulianne S (2015). Social media use and participation: A metaanalysis of current research. Information, Communication & Society, 18, 524–538. doi: 10.1080/1369118X.2015.1008542 [DOI] [Google Scholar]
- Centers for Disease Control and Prevention. (2014a). Partnerships to Improve Community Health (PICH) awardees, CDC RFA-DP14–1417. Retrieved from https://www.grants.gov/web/grants/view-opportunity.html?oppId=255772
- Centers for Disease Control and Prevention. (2014b). PPHF 2014: Racial and Ethnic Approaches to Community Health (REACH)—Financed in part by Prevention and Public Health Funding, FOA DP14–1419PPHF14. Retrieved from https://www.grants.gov/web/grants/view-opportunity.html?oppId=257868
- Centers for Disease Control and Prevention. (2018, July 12). Crosscutting resources—Communication planning tool. Retrieved from https://www.cdc.gov/nccdphp/dnpao/state-local-programs/crosscutting-resources.html#CommunicationMaterials
- Charles-Smith LE, Reynolds TL, Cameron MA, Conway M, Lau EH, Olsen JM, … Corley CD (2015). Using social media for actionable disease surveillance and outbreak management: A systematic literature review. PLoS One, 10, e0139701. doi: 10.1371/journal.pone.0139701 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cisco Systems. (2017). Cisco Visual Networking Index: Forecast and methodology, 2017–2022 white paper. Retrieved from https://www.cisco.com/c/en/us/solutions/collateral/serviceprovider/visual-networking-index-vni/complete-white-paperc11-481360.html
- Director of National Intelligence. (2018). Background to “Assessing Russian Activities and Intentions in Recent US Elections”: The analytic process and cyber incident attribution. Retrieved from https://www.dni.gov/files/documents/ICA_2017_01.pdf
- DOMO. (2018). Data Never Sleeps 5.0. Retrieved from https://www.domo.com/learn/data-never-sleeps-5
- Duke JC, Lee YO, Kim AE, Watson KA, Arnold KY, Nonnemaker JM, & Porter L (2014). Exposure to electronic cigarette television advertisements among youth and young adults. Pediatrics, 134, e29–e36. doi: 10.1542/peds.2014-0269 [DOI] [PubMed] [Google Scholar]
- Evans WD (2016). Social marketing research for global public health: Methods and technologies. New York, NY: Oxford University Press. [Google Scholar]
- Favatas D (2018). How Truth Initiative delivers impactful omnichannel experiences to drive change Paper presented at Digital Health Promotion: Executive Leadership Summit. Washington, DC. [Google Scholar]
- French J, & Gordon R (2015). Strategic social marketing. Thousand Oaks, CA: Sage. [Google Scholar]
- Frieden TR (2014). Six components necessary for effective public health program implementation. American Journal of Public Health, 104, 17–22. doi: 10.2105/AJPH.2013.301608 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fung ICH, Tse ZTH, & Fu KW (2015). The use of social media in public health surveillance. Western Pacific Surveillance and Response Journal, 6(2), 3–6. doi: 10.5365/wpsar.2015.6.1.019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Google Developers. (n.d.). Cookie matching. Real-time bidding protocol web site Retrieved from https://developers.google.com/ad-exchange/rtb/cookie-guide
- Hair EC, Cantrell J, Pitzer L, Bennett MA, Romberg AR, Xiao H, & Vallone D (2018). Estimating the pathways of an antitobacco campaign. Journal of Adolescent Health, 63, 401–406. doi: 10.1016/j.jadohealth.2018.04.008 [DOI] [PubMed] [Google Scholar]
- Hopp T, & Gallicano TD (2016). Development and test of a multidimensional scale of blog engagement. Journal of Public Relations Research, 28, 127–145. doi: 10.1080/1062726X.2016.1204303 [DOI] [Google Scholar]
- Hornik R (2016). Measuring campaign message exposure and public communication environment exposure: Some implications of the distinction in the context of social media. Communication Methods & Measures, 10, 167–169. doi: 10.1080/19312458.2016.1150976 [DOI] [PMC free article] [PubMed] [Google Scholar]
- IBM. (2019). 2019 marketing trends. Retrieved from https://www.ibm.com/watson/marketing/resources/2019-marketing-trends/
- Imran M, Castillo C, Lucas J, Meier P, & Vieweg S (2014). AIDR: Artificial intelligence for disaster response In Proceedings of the 23rd International Conference on World Wide Web (WWW ‘14 Companion; pp. 159–162). New York, NY: Association for Computer Machinery. doi: 10.1145/2567948.2577034 [DOI] [Google Scholar]
- Jobs CG, & Gilfoil DM (2014). A social media advertising adoption model for reallocation of traditional advertising budgets. Academy of Marketing Studies Journal, 18, 235–248. [Google Scholar]
- John LK, Emrich O, Gupta S, & Norton MI (2017). Does “liking” lead to loving? The impact of joining a brand’s social network on marketing outcomes. Journal of Marketing Research, 54, 144–155. doi: 10.1509/jmr.14.0237 [DOI] [Google Scholar]
- Kumkale GT, Albarracín D, & Seignourel PJ (2010). The effects of source credibility in the presence or absence of prior attitudes: Implications for the design of persuasive communication campaigns. Journal of Applied Social Psychology, 40, 1325–1356. doi: 10.1111/j.1559-1816.2010.00620.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liang H, & Fu KW (2015). Testing propositions derived from twitter studies: Generalization and replication in computational social science. PLoS One, 10, e0134270. doi: 10.1371/journal.pone.0134270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Long T, Taubenheim A, Wayman J, Temple S, & Ruoff B (2008). “The Heart Truth:” Using the power of branding and social marketing to increase awareness of heart disease in women. Social Marketing Quarterly, 14, 3–29. doi: 10.1080/15245000802279334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mackey TK, Kalyanam J, Katsuki T, & Lanckriet G (2017). Twitter-based detection of illegal online sale of prescription opioid. American Journal of Public Health, 107, 1910–1915. doi: 10.2105/AJPH.2017.303994 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Association of County and City Health Officials. (2015). Best practices for comprehensive tobacco control programs at the local level: A guide for local health departments based on 2014 national recommendations. Retrieved from https://www.naccho.org/uploads/downloadable-resources/Best-Practices-Tobacco-Programs-Local-Level-2015.pdf
- National Center for Biotechnology Information. (2018). Bethesda, MD: National Library of Medicine. Retrieved from https://www.ncbi.nlm.nih.gov/ [Google Scholar]
- Neiger BL, Thackeray R, Van Wagenen SA, Hanson CL, West JH, Barnes MD, & Fagen MC (2012). Use of social media in health promotion: Purposes, key performance indicators, and evaluation metrics. Health Promotion Practice, 13, 159–164. doi: 10.1177/1524839911433467 [DOI] [PubMed] [Google Scholar]
- Nguyen QC, McCullough M, Meng HW, Paul D, Li D, Kath S, … Li F (2017). Geotagged US tweets as predictors of county-level health outcomes, 2015–2016. American Journal of Public Health, 107, 1776–1782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odlum M, & Yoon S (2017). Health information needs and health seeking behavior during the 2014–2016 Ebola outbreak: A Twitter content analysis. PLoS Currents, 10. doi: 10.1371/currents.outbreaks.fa814fb2bec36e29b718ab6af66124fa [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paul MJ, & Dredze M (2017). Social monitoring for public health. Synthesis Lectures on Information Concepts, Retrieval, and Services, 9, 1–183. [Google Scholar]
- Pew Research Center. (2018). Social media use in 2018. Retrieved from http://assets.pewresearch.org/wp-content/uploads/sites/14/2018/03/01105133/PI_2018.03.01_Social-Media_FINAL.pdf
- The Public Good Projects. (2019a). Public health monitoring. Retrieved from https://publicgoodprojects.org/modals/approach/media-monitoring
- The Public Good Projects (2019b). Opioid crisis. Retrieved from https://publicgoodprojects.org/modals/work/opioid-crisis
- Sinnenberg L, Buttenheim AM, Padrez K, Mancheno C, Ungar L, & Merchant RM (2017). Twitter as a tool for health research: A systematic review. American Journal of Public Health, 107, e1–e8. doi: 10.2105/AJPH.2016.303512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith BG, & Gallicano TD (2015). Terms of engagement: Analyzing public engagement with organizations through social media. Computers in Human Behavior, 53, 82–90. doi: 10.1016/j.chb.2015.05.060 [DOI] [Google Scholar]
- Stephen AT (2016). The role of digital and social media marketing in consumer behavior. Current Opinion in Psychology, 10, 17–21. doi: 10.1016/j.copsyc.2015.10.016 [DOI] [Google Scholar]
- Taylor M, & Kent ML (2014). Dialogic engagement: Clarifying foundational concepts. Journal of Public Relations Research, 26, 384–398. doi: 10.1080/1062726X.2014.956106 [DOI] [Google Scholar]
- Tang L, Bie B, Park SE, & Zhi D (2018). Social media and outbreaks of emerging infectious diseases: A systematic review of literature. American Journal of Infection Control, 46, 962– 972. doi: 10.1016/j.ajic.2018.02.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- United States Computer Emergency Readiness Team. (2011, August 24). Security Tip (ST06–001): Understanding hidden treats: Rooktkits and botnets [web log comment]. Retrieved from https://www.us-cert.gov/ncas/tips/ST06-001
- Vallone D, Cantrell J, Bennett M, Smith A, Rath JM, Xiao H, …. Hair EC. (2018). Evidence of the impact of the truth yinishIt campaign. Nicotine and Tobacco Research, 20, 543– 551. doi: 10.1093/ntr/ntx119 [DOI] [PubMed] [Google Scholar]
- Vallone D, Greenberg M, Xiao H, Bennett M, Cantrell J, Rath J, & Hair E (2017). The effect of branding to promote healthy behavior: Reducing tobacco use among youth and young adults. International Journal of Environmental Research and Public Health, 14(12), E1517. doi: 10.3390/ijerph14121517 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vallone D, Smith A, Kenney T, Greenberg M, Hair E, Cantrell J, … Koval R (2016). Agents of social change: a model for targeting and engaging Generation Z across platforms: How a nonprofit rebuilt an advertising campaign to curb smoking by teens and young adults. Journal of Advertising Research, 56, 414–425. doi: 10.2501/JAR-2016-046 [DOI] [Google Scholar]
- Verhoef PC, Kannan P, & Inman JJ (2015). From multichannel retailing to omni-channel retailing: Introduction to the special issue on multi-channel retailing. Journal of Retailing, 91, 174–181. doi: 10.1016/j.jretai.2015.02.005 [DOI] [Google Scholar]
- Wang H, Tong L, Takeuchi R, & George G (2016). Corporate social responsibility: An overview and new research directions. Academy of Management Journal, 59, 534–544. doi: 10.5465/amj.2016.5001 [DOI] [Google Scholar]
- Woolf SH, Purnell JQ, Simon SM, Zimmerman EB, Camberos GJ, Haley A, & Fields RP (2015). Translating evidence into population health improvement: Strategies and barriers. Annual Review of Public Health, 18, 463–482. doi: 10.1146/annurev-publhealth-082214-110901 [DOI] [PMC free article] [PubMed] [Google Scholar]