

Supplemental Digital Content is available in the text.
Keywords: admission decision, hospital bed capacity, hospital length of stay, patient readmission, quality of healthcare, step-down unit, transitional care
Abstract
Objectives:
To examine whether and how step-down unit admission after ICU discharge affects patient outcomes.
Design:
Retrospective study using an instrumental variable approach to remove potential biases from unobserved differences in illness severity for patients admitted to the step-down unit after ICU discharge.
Setting:
Ten hospitals in an integrated healthcare delivery system in Northern California.
Patients:
Eleven-thousand fifty-eight episodes involving patients who were admitted via emergency departments to a medical service from July 2010 to June 2011, were admitted to the ICU at least once during their hospitalization, and were discharged from the ICU to the step-down unit or the ward.
Interventions:
None.
Measurements and Main Results:
Using congestion in the step-down unit as an instrumental variable, we quantified the impact of step-down unit care in terms of clinical and operational outcomes. On average, for ICU patients with lower illness severity, we found that availability of step-down unit care was associated with an absolute decrease in the likelihood of hospital readmission within 30 days of 3.9% (95% CI, 3.6–4.1%). We did not find statistically significant effects on other outcomes. For ICU patients with higher illness severity, we found that availability of step-down unit care was associated with an absolute decrease in in-hospital mortality of 2.5% (95% CI, 2.3–2.6%), a decrease in remaining hospital length-of-stay of 1.1 days (95% CI, 1.0–1.2 d), and a decrease in the likelihood of ICU readmission within 5 days of 3.6% (95% CI, 3.3–3.8%).
Conclusions:
This study shows that there exists a subset of patients discharged from the ICU who may benefit from care in an step-down unit relative to that in the ward. We found that step-down unit care was associated with statistically significant improvements in patient outcomes especially for high-risk patients. Our results suggest that step-down units can provide effective transitional care for ICU patients.
ICUs provide the highest level of care in a hospital setting but are often congested contributing to worsened health outcomes (1–4). Step-down units (SDUs) are sometimes used to provide an intermediate level of care for patients whose illness severity may not warrant ICU care, but who are not stable enough to be treated in the ward (5, 6). As such, they can improve ICU throughput. With one nurse for every three to four patients, SDUs provide a higher nurse-to-patient ratio than the general wards but are generally less expensive to operate than ICUs (7). Although considerable variation exists in how SDUs are used in practice (5), this report focuses on the originally intended role of SDUs, which is to provide transitional care for patients discharged from the ICU (8).
There is much debate within the medical community about the potential benefits of SDU care (5, 9). Some researchers have shown that receiving transitional care after discharge from an ICU can reduce the likelihood of adverse events (10). Several studies suggest that these units provide a cost-effective and safe transition from the ICU to the ward or home for very ill patients (11–13). Conversely, some studies show that SDU care is not associated with improved patient outcomes following ICU discharge (14) and argue that there is insufficient evidence of their cost-effectiveness (15, 16). Hence, many hospitals are uncertain about whether and how best to use an SDU.
The purpose of this study was to empirically investigate the impact of SDU care on patient outcomes after ICU discharge. Specifically, we examined whether transfer to an SDU, rather than to a ward, after an ICU stay affects in-hospital mortality (Mortality), hospital readmissions (HospReadm), ICU readmissions (ICUReadm), and remaining hospital length-of-stay (RemHospLOS). In contrast to our prior study, which focused on evaluating the impact of SDU care for various patient cohorts admitted from the emergency department (ED) (17), this study focused on patients who were discharged from the ICU and extended our prior analyses by stratifying patients based on severity of illness.
Estimating the impact of SDU admission is challenging because patients who are admitted to the SDU from the ICU are more likely to be sicker and thus have worse outcomes compared to patients who are discharged directly to the ward. Since we could not randomly assign patients to the SDU or the ward and compare patient outcomes, we relied on an observational study and used an instrumental variable (IV) approach to address potential unobserved treatment selection biases. We used SDU congestion as an IV to estimate the impact of SDU care by comparing differences in outcomes between patient groups with similar observable characteristics but who were discharged to different units due to congestion in the SDU.
MATERIALS AND METHODS
This project was approved by the Kaiser Permanente Northern California (KPNC) and Columbia University Institutional Review Boards for the Protection of Human Subjects.
Setting
Our study sample consisted of all adult (age ≥ 18 yr) inpatient episodes that were initiated between January 2010 and November 2011 in one of 10 KPNC hospitals. We restricted our sample to patients meeting these criteria: 1) admitted via the ED to a medical service; 2) admitted to the ICU during their hospitalization; and 3) admitted to an SDU or the ward following their first ICU stay. Since it is possible that SDU care may not provide the same benefit for all ICU patients, we additionally divided patients by severity level as measured by the Simplified Acute Physiology Score 3 (SAPS3) score (18–20). We defined “Low Severity Patients” as those with SAPS3 below the 33rd percentile (SAPS3 ≤ 42) and “High Severity Patients” as those with SAPS3 above the 66th percentile (SAPS3 ≥ 51). The SAPS3 score was updated at the time of each ICU admission.
For each hospital in our study, inpatient beds could be categorized by level of care: the ICU with 1–2 patients per nurse, the SDU with 2.5–4 patients per nurse, and the joint general medical/surgical ward (Ward) with up to five patients per nurse. Each hospital’s ICU was staffed with intensivists and each had an SDU staffed by hospitalists. The SDUs generally allowed for continuous oximetry and noninvasive ventilation.
Instrumental Variable Approach
The use of observational data to estimate the impact of SDU admission is vulnerable to treatment selection biases. This is because severity factors which are known to the physician at the time of the discharge decision, but are unobservable in the data, for example, poor perfusion or agitation, could affect both SDU admission and patient outcomes, making the SDU admission decisions endogenous. To reduce the aforementioned bias, we used an approach that mimics a randomized study by introducing an IV which is a factor that influences SDU admission decisions, but which otherwise does not affect patient outcomes (see [21] and [22]). Supplementary Figure 1 (Supplemental Digital Content 1, http://links.lww.com/CCX/A171) illustrates our econometric framework.
We employed SDU congestion as an instrument. We defined an SDU as being “busy” (SDU Busy = 1) if the number of available SDU beds 1 hour prior to ICU discharge was less than or equal to two. We used patient flow data to derive hourly occupancy levels for each SDU and defined its capacity as the maximum occupancy level observed for that unit over the 12-month time horizon in our study. For SDU congestion to be a valid instrument the following must hold: 1) SDU congestion affects SDU admission decisions and 2) SDU congestion is uncorrelated to the unobservable severity factors which affect patient outcomes. In other words, SDU congestion must affect patient outcomes only through its effect on the likelihood of SDU admission. For condition 1, we looked at the proportions of patients who were routed to the SDU when the SDU was congested versus not congested. As shown in Table 1, when the SDU was “busy,” the percentages of patients admitted to the SDU decreased substantially. The effect of SDU congestion on SDU admission is formally validated with the results of the admission decision model. For condition 2, we used SAPS3 as a proxy for unobservable severity factors. We performed two-sample Kolmogorov-Smirnov tests, the results of which suggest that the distribution of SAPS3 for patients who were discharged from the ICU when the SDU was busy is not statistically different from that when the SDU was not busy (p = 0.521 and 0.281 for low and high severity patients, respectively). Supplementary Figures 2 and 3 (Supplemental Digital Content 1, http://links.lww.com/CCX/A171) depict the distributions of SAPS3 for low and high severity patients who were discharged from the ICU when the SDU was busy and not busy. In addition, we conducted a sensitivity analysis for violations of Condition 2 (22).
TABLE 1.
Proportions of ICU Patients Who Were Routed to the Step-Down Unit and Ward When Step-Down Unit Was Busy Versus Step-Down Unit Was Not Busy

The Admission Decision Model
In the first stage of the two-stage IV approach, we regressed the endogenous variable, SDU admission, on the instrument, SDU congestion. In order to conduct risk-adjusted analysis, we also controlled for seasonality and patient characteristics including three illness severity scores, which were assigned at the time of hospital admission. A full list of covariates is provided in Supplementary Table 1 (Supplemental Digital Content 1, http://links.lww.com/CCX/A171).
The Patient Outcome Models
In the second stage, our dependent variables were patient outcomes: Mortality, RemHospLOS, ICUReadm, and HospReadm. RemHospLOS is measured as the number of days between first ICU discharge and hospital discharge. We defined ICUReadm (ICUReadm—2 d, ICUReadm—5 d) as a subsequent stay in the ICU within 2 or 5 days after ICU discharge and prior to hospital discharge; that is, the ICUReadm must occur during the same hospital stay (23). We defined HospReadm (HospReadm—2 wk, HospReadm—30 d) as a new hospital admission within 2 weeks or 30 days following the index hospital discharge. We excluded patients who died in the HospReadm models.
The principal independent variable was SDU admission. As in the admission decision model, we controlled for patient characteristics and hospital fixed effects. Because congestion during a patient’s hospital stay could impact the patient’s outcomes (24), we also controlled for the daily average occupancy level (AvgOccStay) each patient experienced for all inpatient units he/she was admitted to after leaving the ICU and before hospital discharge. For ICUReadm, we calculated AvgOccStay based on the window between two consecutive ICU admissions. Because we do not have dynamic severity information, we cannot control for the severity of other patients treated in the same unit during the patient’s stay.
We estimated patient outcome models jointly with the admission decision model via maximum likelihood estimation. We used the bivariate probit model for our binary outcomes (Mortality, HospReadm, ICUReadm). For RemHospLOS, we used the treatment effect model. For comparison, we also estimated the patient outcome models without the IV. Stata 15.1 was used for statistical analyses (StataCorp, College Station, TX).
RESULTS
Patient Cohort
Our initial dataset consisted of 165,948 hospitalizations. Figure 1 depicts the data selection process. We restricted our study sample to patients admitted in the 12 months in the center of the 22-month period to avoid censored estimates of capacity and occupancy. We excluded surgical patients because the care pathways for them tend to be fairly standardized and protocol driven, making our statistical strategy more challenging for these patients. Our final patient cohort of 11,058 hospitalizations is characterized in Supplementary Table 2 (Supplemental Digital Content 1, http://links.lww.com/CCX/A171). We observed that patients who went to the SDU immediately following the ICU tended to be older and male, had more preexisting comorbidities (as measured by the Comorbidity Point Score 2 score), and spent more time in the ICU than those who went to the Ward. In our full dataset, 64.5% of patients (71.7%) in the ICU (SDU) were admitted via the ED to a medical service.
Figure 1.
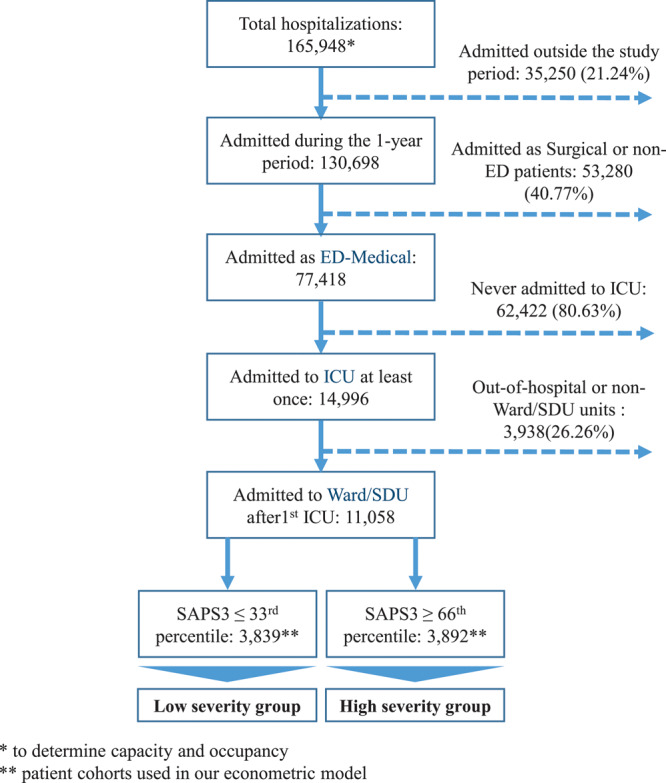
Data selection and severity categorization. ED = emergency department, SAPS3 = Simplified Acute Physiology Score 3, SDU = step-down unit.
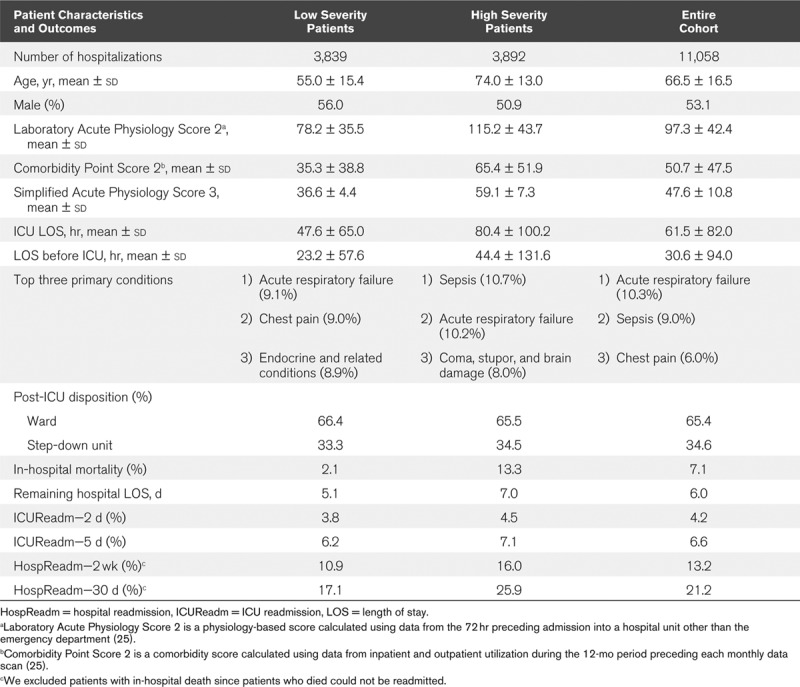
Patient characteristics and outcome variables for low and high severity patients are summarized in Table 2, while more detailed information on primary conditions is reported in Supplementary Table 3 (Supplemental Digital Content 1, http://links.lww.com/CCX/A171). On average, patients who were classified as “High Severity” based on their SAPS3 were older, had higher comorbidity and laboratory-based physiology scores, and spent more time in the ICU than those classified as “Low Severity.” Not surprisingly, high severity patients were more likely to be admitted to the SDU following their first ICU stay than low severity patients. Supplementary Table 4 (Supplemental Digital Content 1, http://links.lww.com/CCX/A171) summarizes patient outcomes for the patients in our cohort based on severity class and the unit which followed the first ICU stay. On average, patients who were discharged to the SDU had higher RemHospLOS, ICUReadm, and HospReadm as expected, whereas patients discharged to the Ward had slightly higher Mortality.
TABLE 2.
Patient Characteristic and Outcome Summary Statistics
Supplementary Table 5 (Supplemental Digital Content 1, http://links.lww.com/CCX/A171) summarizes the maximum and average occupancy level within each level of care across the 10 hospitals. Using this as an estimate for the capacity of each unit, we found that the average occupancy level in the ICU, SDU, and Ward were 61%, 67%, and 68%, respectively.
Estimated Effect of SDU Occupancy on SDU Admission
There were more than two available SDU beds upon ICU discharge for 89.4% of the patients. Supplementary Table 6 (Supplemental Digital Content 1, http://links.lww.com/CCX/A171) summarizes the results of the admission model. The effect of SDU congestion on the likelihood of SDU admission was negative and statistically significant. Decreasing the SDU occupancy level from having two or fewer available SDU beds to more than two available increased the chance of SDU admission from 15.9% to 35.2% for low severity patients and from 12.5% to 36.9% for high severity patients.
Estimated Effect of SDU Admission on Patient Outcomes
Table 3 summarizes the results for the low severity patients using our IV approach and using a simple probit model without an IV (non-IV approach). We did not find a statistically significant effect of SDU admission on Mortality, RemHospLOS, or ICUReadm. We did find a statistically significant effect (p < 0.01) of SDU admission on HospReadm following hospital discharge. To get a sense of the magnitude of the effect of a busy SDU, we estimated the average treatment effect of the SDU being busy versus not busy. Recall that a busy SDU was associated with a more than 50% decrease in likelihood of SDU admission for low severity patients. In turn, this translates to an increase in likelihood of HospReadm within 2 weeks (30 d) from 13.0% to 15.5% (20.2–24.1%). We do not present average treatment effects by assuming all patients are admitted to the SDU and comparing this to the case where all patients are admitted to the ward because there are some patients who will not be admitted to the SDU no matter how much capacity there is. When not using an IV, we found a negative and statistically significant coefficient for SDU admission on Mortality, a positive and statistically significant coefficient for SDU admission on RemHospLOS, and no statistically significant coefficient for ICU and HospReadm.
TABLE 3.
Estimated Effect of Step-Down Unit Admission on Patient Outcomes for Low Severity Patients
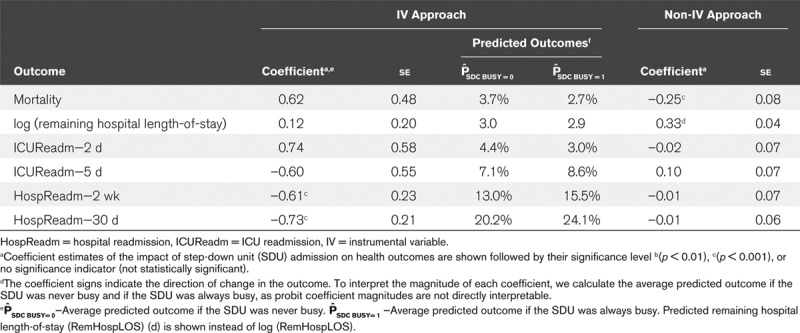
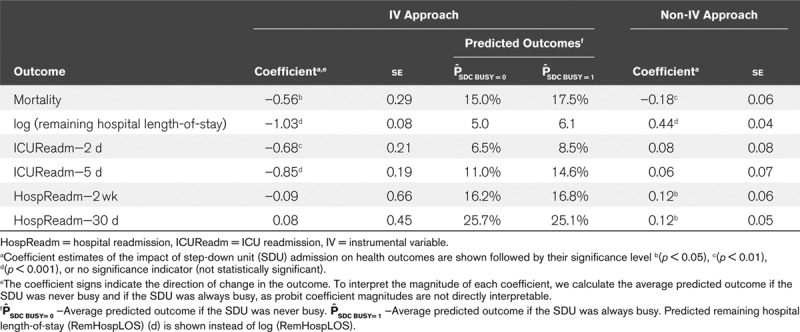
Table 4 summarizes the results for the high severity patients with our IV approach and without. We found a statistically significant effect of SDU admission on Mortality (p < 0.05), RemHospLOS (p < 0.001), and ICUReadm within 2 days (p < 0.01) and 5 days (p < 0.001). However, we did not find a statistically significant effect of SDU admission on HospReadm. Again, we estimated the average treatment effect of the SDU being busy versus not busy. We found that a busy SDU was associated with an absolute increase in hospital mortality of 2.5%, an increase in RemHospLOS of 1.1 hospital days, and an absolute increase in likelihood of ICUReadm within 2 days (5 d) of 1.9% (3.6%). When not using an IV, we found a negative and statistically significant coefficient for SDU admission on Mortality, a positive and statistically significant coefficient for SDU admission on RemHospLOS and HospReadm, and no statistically significant coefficient for ICUReadm.
TABLE 4.
Estimated Effect of Step-Down Unit Admission on Patient Outcomes for High Severity Patients
The results were quite robust to changes in the SAPS3 cutoffs for low and high severity (Supplementary Tables 7 and 8, Supplemental Digital Content 1, http://links.lww.com/CCX/A171), to various definitions of SDU congestion (Supplementary Tables 9 and 10, Supplemental Digital Content 1, http://links.lww.com/CCX/A171), and to using linear probability models for the discrete outcomes (Supplementary Tables 11–13, Supplemental Digital Content 1, http://links.lww.com/CCX/A171). Additionally, while we can never completely rule out the possibility of unobserved confounders impacting our results, our sensitivity analysis (Supplementary Figs. 4 and 5, Supplemental Digital Content 1, http://links.lww.com/CCX/A171) suggests that our results are very robust to potential unobserved confounders.
DISCUSSION
Our work suggests that SDU care can benefit a subset of patients who are discharged from the ICU. The benefit of transitional care is most evident among ICU patients with higher illness severity whose characteristics are shown in Table 2. For these patients, we saw statistically significant reductions in mortality, RemHospLOS, and ICUReadm. Although we did not find that SDU care was associated with a decrease in HospReadm for high severity patients, we did find the effect in patients with lower illness severity. This may be due to competing failure rates between readmissions and postdischarge mortality; if high severity patients are more likely to die than low severity patients, they may appear to be less likely to be readmitted. Unfortunately, our data does not include postdischarge mortality, so we cannot test this hypothesis. Furthermore, since our results suggest that for many patients SDU care reduced ICUReadm, HospReadm, and RemHospLOS, the use of SDUs can potentially decrease hospital bed utilization and staffing costs in the long term. We note there exist SDU alternatives, such as flexible ICU beds, that have the potential to realize these benefits.
In contrast to our IV analysis, prior studies on the impact of SDU care primarily relied on before-and-after comparisons (15, 26–29) and direct comparisons between patients who were and were not discharged to an SDU (11, 30). Although several studies controlled for patient characteristics through multivariate regression (31) and propensity score matching (32), those studies considered only patient characteristics that were observable in patient records. These approaches do not address endogeneity bias caused by factors that are unobservable in the data but known to the physician. For instance, a physician may determine that a patient who has poor perfusion at the time of the discharge decision, despite having relatively stable vital signs and normal laboratory test results, should be discharged to the SDU. But because this patient is more critical than the average patient discharged to the ward, he/she is also more likely to have worse health outcomes.
In Tables 3 and 4, we observe a substantial difference between IV and non-IV estimates. Without an IV, the estimates suggest that SDU care increased RemHospLOS for both severity groups, and increased HospReadm for high severity patients. Additionally, despite the potential presence of endogeneity bias, the treatment effect for mortality for high severity patients was still negative, although smaller in magnitude. This provides strong evidence that SDU admission is associated with a reduction in mortality risk, as the results of both the IV and non-IV models support this finding. That said, the differences in magnitude and statistical significance of the estimate coefficients suggest that ignoring potential bias introduced when using observational data could result in underestimates of the potential benefit of SDU care, as well as produce mixed results where the estimated treatment effect may be in either direction. Thus, one likely explanation for the mixed evidence in the literature on the effect of SDU care is because these other studies do not explicitly address the potential for endogeneity biases.
This study has several limitations: 1) the IV approach estimates the average effect of SDU admission only for the subset of patients whose SDU admission decisions depends on the availability of SDU beds and not to the more than 60% of patients who were not admitted to the SDU when there were more than two beds available; 2) all study participants were members of a single integrated healthcare delivery system; 3) a large percentage of patients (60%) were admitted to the SDU from the ED, yet our study only provides insights into the benefits of SDU care for patients discharged from the ICU; 4) we do not have information on do not resuscitate or palliative status; and 5) our data were not taken from the most recent time period. Kaiser Permanente decided to remove all SDUs in Northern California several years ago and so it is not possible to redo this study using more recent data. More analysis would be necessary to understand how the impact of SDU care has evolved over time.
Our study also has several strong points. It covers 10 hospitals of different sizes, specialties, and locations, which helps to validate the robustness and generalizability of the results. Furthermore, our data include detailed information on every unit in which patients stayed, which allowed us to observe the entire care pathway of each patient, determine the time spent in each unit, and compute occupancy levels at any point of time in the study period.
CONCLUSIONS
Using patient data from 10 hospitals, we studied the use of SDUs and used econometric models to estimate the benefit of providing transitional care relative to that of the ward. Our work shows that for patients discharged from the ICU, SDU care was associated with improved patient outcomes for the subset of patients that we studied. We found that SDU admission after an ICU stay was associated with reduction in HospReadm rates for ICU patients with lower severity. For ICU patients with higher severity, we found evidence that SDU admission directly after an ICU stay was associated with a reduction in mortality rate, RemHospLOS, and ICUReadm rate. Our findings provide evidence that intermediate care with a nurse-to-patient ratio that is higher than that of the ward can measurably benefit ICU patients and can safely serve as a bridge from ICU to ward or home.
Supplementary Material
Footnotes
Supplemental digital content is available for this article. Direct URL citations appear in the HTML and PDF versions of this article on the journal’s website (http://journals.lww.com/ccejournal).
Mr. Lekwijit’s and Dr. Chan’s institutions received funding from the National Science Foundation/Agency for Healthcare Research and Quality. Drs. Chan’s and Escobar’s institutions received funding from National Science Foundation and Agency for Healthcare Research and Quality (Grant CMMI-1233547). Dr. Liu’s institution received funding from the National Institutes of Health (NIH) R35GM128672, and he received funding from the NIH. Drs. Escobar and Liu were also supported by the Permanente Medical Group and Kaiser Foundation Hospitals. Dr. Green has disclosed that she does not have any potential conflicts of interest.
REFERENCES
- 1.Brilli RJ, Spevetz A, Branson RD, et al. ; American College of Critical Care Medicine Task Force on Models of Critical Care Delivery. The American College of Critical Care Medicine Guidelines for the Defintion of an Intensivist and the Practice of Critical Care Medicine. Critical care delivery in the intensive care unit: Defining clinical roles and the best practice model. Crit Care Med. 2001; 29:2007–2019 [DOI] [PubMed] [Google Scholar]
- 2.Mathews KS, Long EF. A conceptual framework for improving critical care patient flow and bed use. Ann Am Thorac Soc. 2015; 12:886–894 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Herring AA, Ginde AA, Fahimi J, et al. Increasing critical care admissions from U.S. emergency departments, 2001-2009. Crit Care Med. 2013; 41:1197–1204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kim SH, Chan CW, Olivares M. Association among ICU congestion, ICU admission decision, and patient outcomes. Crit Care Med. 2016; 44:1814–1821 [DOI] [PubMed] [Google Scholar]
- 5.Prin M, Wunsch H. The role of stepdown beds in hospital care. Am J Respir Crit Care Med. 2014; 190:1210–1216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nasraway SA, Cohen IL, Dennis RC, et al. Guidelines on admission and discharge for adult intermediate care units. American College of Critical Care Medicine of the Society of Critical Care Medicine. Crit Care Med. 1998; 26:607–610 [DOI] [PubMed] [Google Scholar]
- 7.Sjoding MW, Valley TS, Prescott HC, et al. Rising billing for intermediate intensive care among hospitalized Medicare beneficiaries between 1996 and 2010. Am J Respir Crit Care Med. 2016; 193:163–170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gotsman MS, Schrire V. Acute myocardial infarction–an ideal concept of progressive coronary care. S Afr Med J. 1968; 42:829–832 [PubMed] [Google Scholar]
- 9.Vincent JL, Rubenfeld GD. Does intermediate care improve patient outcomes or reduce costs? Crit Care. 2015; 19:89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chaboyer W, James H, Kendall M. Transitional care after the intensive care unit: Current trends and future directions. Crit Care Nurse. 2005; 25:16–18, 20–22, 24–26 passim; quiz 29 [PubMed] [Google Scholar]
- 11.Harding AD. What can an intermediate care unit do for you? J Nurs Adm. 2009; 39:4–7 [DOI] [PubMed] [Google Scholar]
- 12.Stacy KM. Progressive care units: Different but the same. Crit Care Nurse. 2011; 31:77–83 [DOI] [PubMed] [Google Scholar]
- 13.Tosteson AN, Goldman L, Udvarhelyi IS, et al. Cost-effectiveness of a coronary care unit versus an intermediate care unit for emergency department patients with chest pain. Circulation. 1996; 94:143–150 [DOI] [PubMed] [Google Scholar]
- 14.Bellomo R, Goldsmith D, Uchino S, et al. A before and after trial of the effect of a high-dependency unit on post-operative morbidity and mortality. Crit Care Resusc. 2005; 7:16–21 [PubMed] [Google Scholar]
- 15.Keenan SP, Massel D, Inman KJ, et al. A systematic review of the cost-effectiveness of noncardiac transitional care units. Chest. 1998; 113:172–177 [DOI] [PubMed] [Google Scholar]
- 16.Hanson CW, III, Deutschman CS, Anderson HL, III, et al. Effects of an organized critical care service on outcomes and resource utilization: A cohort study. Crit Care Med. 1999; 27:270–274 [DOI] [PubMed] [Google Scholar]
- 17.Chan CW, Green LV, Lekwijit S, et al. Assessing the impact of service level when customer needs are uncertain: An empirical investigation of hospital step-down units. Manag Sci. 2018; 65:751–775 [Google Scholar]
- 18.Christensen S, Johansen MB, Christiansen CF, et al. Comparison of Charlson comorbidity index with SAPS and APACHE scores for prediction of mortality following intensive care. Clin Epidemiol. 2011; 3:203–211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mbongo CL, Monedero P, Guillen-Grima F, et al. Performance of SAPS3, compared with APACHE II and SOFA, to predict hospital mortality in a general ICU in Southern Europe. Eur J Anaesthesiol. 2009; 26:940–945 [DOI] [PubMed] [Google Scholar]
- 20.Strand K, Flaatten H. Severity scoring in the ICU: A review. Acta Anaesthesiol Scand. 2008; 52:467–478 [DOI] [PubMed] [Google Scholar]
- 21.Wooldridge J. Econometric Analysis of Cross Section and Panel Data. 2010, Cambridge, MA: MIT Press [Google Scholar]
- 22.Baiocchi M, Cheng J, Small DS. Instrumental variable methods for causal inference. Stat Med. 2014; 33:2297–2340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Brown SE, Ratcliffe SJ, Halpern SD. An empirical derivation of the optimal time interval for defining ICU readmissions. Med Care. 2013; 51:706–714 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kc DS, Terwiesch C. An econometric analysis of patient flows in the cardiac intensive care unit. Manuf Serv Oper Manag. 2012; 14:50–65 [Google Scholar]
- 25.Escobar GJ, Gardner MN, Greene JD, et al. Risk-adjusting hospital mortality using a comprehensive electronic record in an integrated health care delivery system. Med Care. 2013; 51:446–453 [DOI] [PubMed] [Google Scholar]
- 26.Armstrong K, Young J, Hayburn A, et al. Evaluating the impact of a new high dependency unit. Int J Nurs Pract. 2003; 9:285–293 [DOI] [PubMed] [Google Scholar]
- 27.Davies J, Tamhane R, Scholefield C, et al. Does the introduction of HDU reduce surgical mortality? Ann R Coll Surg Engl. 1999; 81:343–347 [PMC free article] [PubMed] [Google Scholar]
- 28.Franklin CM, Rackow EC, Mamdani B, et al. Decreases in mortality on a large urban medical service by facilitating access to critical care. An alternative to rationing. Arch Intern Med. 1988; 148:1403–1405 [PubMed] [Google Scholar]
- 29.Eachempati SR, Hydo LJ, Barie PS. The effect of an intermediate care unit on the demographics and outcomes of a surgical intensive care unit population. Arch Surg. 2004; 139:315–319 [DOI] [PubMed] [Google Scholar]
- 30.McIlroy DR, Coleman BD, Myles PS. Outcomes following a shortage of high dependency unit beds for surgical patients. Anaesth Intensive Care. 2006; 34:457–463 [DOI] [PubMed] [Google Scholar]
- 31.Peelen L, de Keizer NF, Peek N, et al. The influence of volume and intensive care unit organization on hospital mortality in patients admitted with severe sepsis: A retrospective multicentre cohort study. Crit Care. 2007; 11:R40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ranzani OT, Zampieri FG, Taniguchi LU, et al. The effects of discharge to an intermediate care unit after a critical illness: A 5-year cohort study. J Crit Care. 2014; 29:230–235 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.