

Abstract
Importance:
Global cases of coronavirus disease 2019 infection continue to increase, and significant numbers of patients are critically ill, placing an immense burden on ICU resources. Understanding baseline resource needs and surge capacity in the ICU will be essential to meet current and projected healthcare needs. Continued appraisal of the state of readiness for healthcare systems at individual, regional and national levels will be paramount to ensure we are poised to continue the fight against coronavirus disease 2019.
Objectives:
This study queried U.S. ICU clinician perspectives on ICU preparedness and concerns regarding delivering coronavirus disease 2019 patient care.
Design, Setting, and Participants:
An anonymous web-based survey administered from March 18, 2020, to March 25, 2020 (email and newsletter) used survey methodology to query members of U.S. national critical care organizations.
Main Outcomes and Measures:
Through a 12-item descriptive questionnaire, ICU clinicians were assessed regarding preparedness, techniques employed to augment critical care capacity, and concerns related to caring for coronavirus disease 2019 patients.
Results:
A total of 4,875 ICU clinicians responded to the survey. Respondents included ICU nurses (n = 3,470, 71.3%), physicians (n = 664, 13.6%), advanced practice providers (nurse practitioners and physician assistants; n = 334, 6.9%), respiratory therapists (n = 236, 4.9%), and pharmacists (n = 79, 1.6%). Over half (n = 2,552, 52.5%) reported having cared for a presumed or confirmed coronavirus disease 2019 patient. The majority (n = 4,010, 82.9%) identified that their hospital was employing techniques to augment critical care capacity. However, 64.5% (n = 3,125) believed that their ICU facility and team were inadequately prepared to treat coronavirus disease 2019 patients. The majority (n = 4,547, 93.9%) anticipated ICU personal protective equipment shortages based upon their current use profile. The chief reported concerns include ICU resource shortages such as supplies, medications, beds, ICU staffing shortages, and patient surge leading to overcrowding.
Conclusions and Relevance:
This national ICU clinician survey indicates that hospitals are expanding ICU bed capacity to prepare for coronavirus disease 2019 patient surge. Importantly, amid this preparation, ICU clinicians harbor concerns regarding preparedness, staffing, and common use resources that merit specific education as well as resource allocation and utilization planning.
Keywords: coronavirus disease 2019, critical care clinician, intensive care unit, intensive care unit clinician, pandemic, preparedness
Coronavirus disease 2019 (COVID-19) is a newly-emerging, highly infectious disease caused by severe acute respiratory syndrome coronavirus 2 (1). The disease was first identified in 2019 in Wuhan China, and has since spread globally, resulting in the 2019–2020 COVID-19 pandemic (2). The WHO declared COVID-19 infection a Public Health Emergency of International Concern on January 30, 2020, and a pandemic on March 11, 2020 (3). As of April 12, 2020, there have been over 1.8 million confirmed cases spanning over 200 countries and territories, with over 112,000 deaths. Documented cases in the United States now surpass the total tally recorded in all other countries (4).
COVID-19 can result in acute hypoxemic respiratory failure requiring critical care in an estimated 5% of patients (5–7). Common reasons for ICU admission include hypoxemic respiratory failure, mechanical ventilation, hypotension requiring vasopressor rescue, or all three (8). The prevalence of hypoxemic respiratory failure in patients with COVID-19 is estimated at 19% of ICU patients with up to 12% requiring invasive mechanical ventilation in the ICU (6, 9). ICU patient mortality may reach 26% (10).
Worldwide, cases are increasing exponentially. Once local transmission occurs, it is estimated that the number of patients with COVID-19 in ICU settings doubles every 2 to 3 days. Furthermore, the rate of increase in ICU admissions may take more than 4 weeks to peak (11). Understanding baseline and surge ICU resource needs is essential to meet current and projected healthcare needs. These needs are multifaceted and include space (ICU rooms/beds), staff (including nurses, pharmacists, respiratory therapists, and intensivists), and supplies (medications, oxygen, ventilators, personal protective equipment [PPE], etc.). The Society of Critical Care Medicine (SCCM) recently published an update on U.S. ICU resource availability for COVID-19 (12). Specific information on ICU preparedness in a given city, region, or state is unfortunately opaque. This survey sought to improve the understanding of preparedness and clinician perception of the efficacy of those efforts during the early stages of pandemic care in the United States.
MATERIALS AND METHODS
Data acquisition occurred through a SCCM launched national web-based anonymous survey from March 18, 2020, to March 25, 2020. The survey invitation targeted members of the Critical Care Societies Collaborative, a grouping of four major U.S. critical care professional organizations including the American Association of Critical-Care Nurses, the American College of Chest Physicians, the American Thoracic Society, and SCCM. Based upon the key role played by ICU respiratory therapists, the survey was also sent to members of the American Association for Respiratory Care. Collectively these organizations represent over 150,000 critical care professionals including physicians, advanced practice providers, nurses, respiratory therapists, and pharmacists.
The 12-item questionnaire assessed ICU clinician perceptions of the degree to which they are prepared to treat COVID-19 patients within their healthcare systems. Additional elements assessed concerns related to caring for COVID-19 patients in the ICU, efforts to expand critical care space, and issues regarding the supply of PPE, medications, and staff. The survey was created using SurveyMonkey (SurveyMonkey Inc. San Mateo, CA; http://www.surveymonkey.com) and distributed via email and newsletter blasts. The study received institutional review board approval as a quality improvement initiative as the intent was to collect aggregate anonymous provider data about the implementation of practice for clinical purposes.
RESULTS
A total of 4,875 ICU clinicians responded to the survey. Respondents included ICU nurses (n = 3,470, 71.3%), physicians (n = 664, 13.6%), advanced practice providers (nurse practitioners and physician assistants; n = 334, 6.9%), respiratory therapists (n = 236, 4.9%), and pharmacists (n = 79, 1.6%). Other respondents included certified registered nurse anesthetists, physical therapists, dieticians, ICU directors, nurse managers and trainees in residency (n = 82, 1.7%) (Table 1 and Fig. 1). These clinicians represented ICU settings in the United States including all 50 states and Puerto Rico.
TABLE 1.
ICU Clinician Demographics (Overall Number of Responses = 4,875)
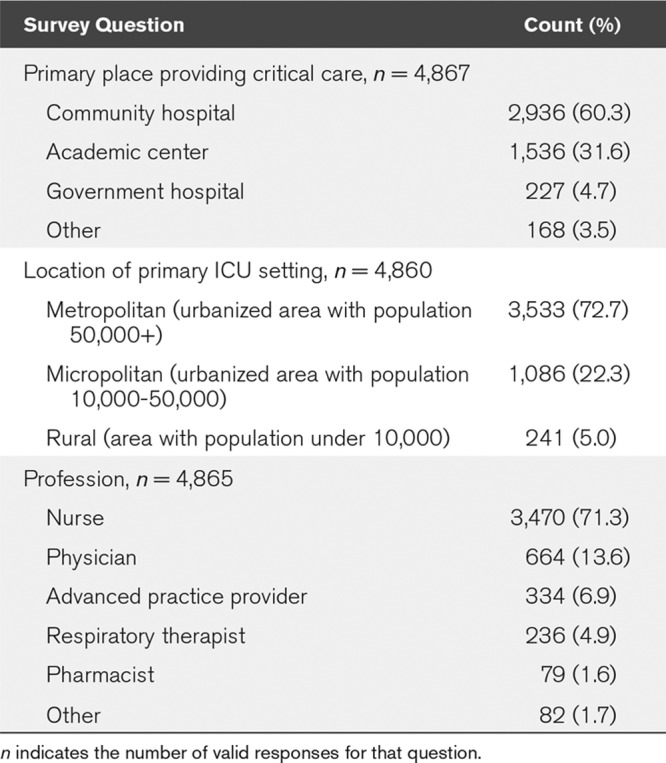
Figure 1.

ICU clinician survey respondents.
Respondents reported working in community (n = 2,936, 60.3%), academic (n = 1,536, 31.6%), and government (n = 227, 4.7%) settings. Practice locations included metropolitan and urbanized with a population more than 50,000 (n = 3,533, 72.7%), micropolitan and urbanized with a population of 10,000–50,000 (n = 1,086, 22.3%), and rural with a populations fewer than 10,000 (n = 241, 5.0%) (Table 1 and Fig. 2). Slightly more than half (2,552, 52.5%) reported having cared for a presumed or confirmed COVID-19 patient. Nearly 2 of 3 (n = 3,125, 64.5%) believed that that their ICU and critical care team are inadequately prepared to safely and effectively treat COVID-19 patients whether those patients are definitely infected, or still under investigation.
Figure 2.
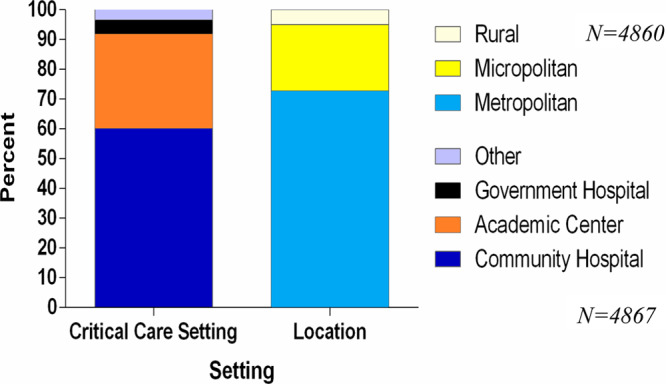
ICU clinician respondent’s work setting.
There was near uniform (n = 4,808, 98.7%) concern regarding aspects of ICU and clinician preparedness for COVID-19 patient care. These concerns included the lack of specific and consistent clinical guidance or treatment approaches (n = 2,613, 53.6%), insufficient clinician PPE use training (n = 2,120, 43.5%), anticipated ICU staffing shortages (n = 2,862, 58.7%), anticipated ICU resource shortages including routine use supplies, medications, and beds (n = 3,992, 81.9%), as well as patient surge and overcrowding (n = 2,984, 61.2%). Importantly, such concerns eclipsed any related to receiving pay or benefits during periods of quarantine following exposure to COVID-19 infected patients after direct care delivery (n = 1,591, 32.7%) (Table 2 and Fig. 3). Anticipated PPE shortages led the list of resource concerns for nearly all respondents (n = 4,547, 93.9%) (Fig. 4).
Figure 3.
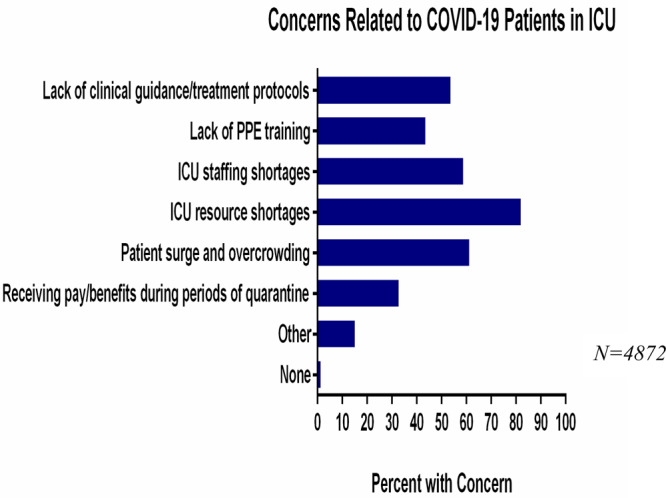
ICU clinician concerns regarding treating coronavirus disease 2019 (COVID-19) patients. PPE = personal protective equipment.
Figure 4.
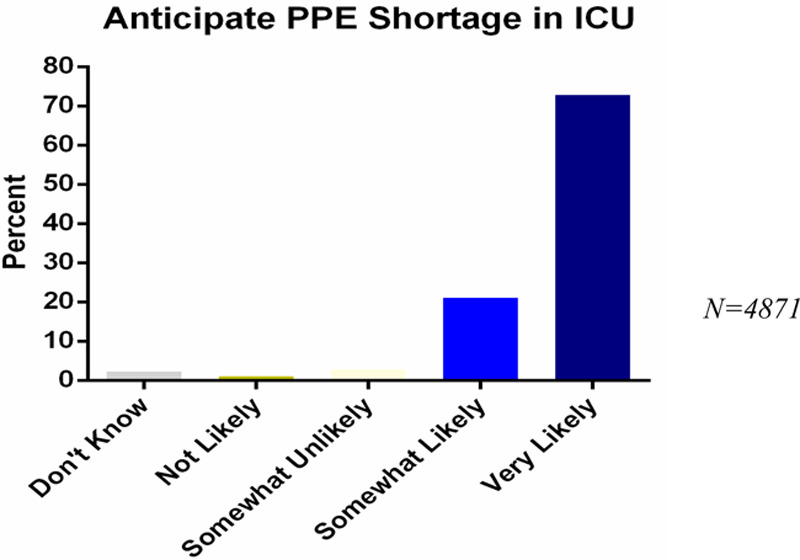
ICU clinician reports of anticipated personal protective equipment (PPE) shortages.
Nearly all (4,707, 97%) reported activity specifically related to preparation for COVID-19 patient care. Specific measures included clinician communication about COVID-19 (n = 3,491, 71.9%), designating dedicated isolation rooms and areas (n = 3,414, 70.4%), activating an incident command team or similar to focus on COVID-19 activities (n = 3,029, 62.4%), creating internal COVID-19 online resources for staff education and guidance (n = 2,835, 58.4%), conducting general emergency preparedness training or drills within the last 90 days (n = 630, 13%), developing or updating a specific plan to augment ICU staffing (n = 1,350, 27.8%), and conducting a COVID-19 specific training or drill (n = 1,064, 21.9%) (Table 2 and Fig. 5).
TABLE 2.
ICU Preparedness for Coronavirus Disease 2019 (Overall Number of Responses = 4,875)
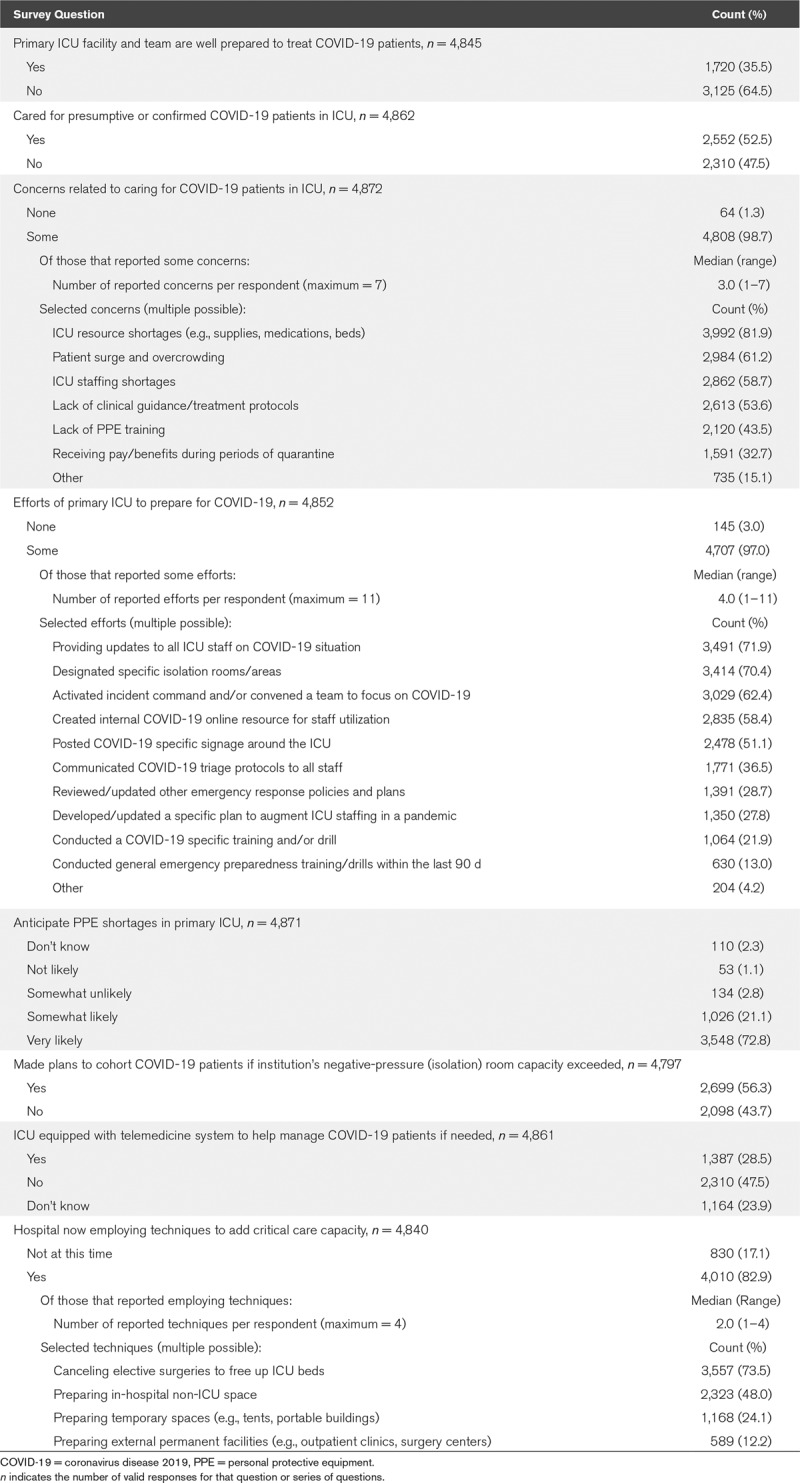
Figure 5.
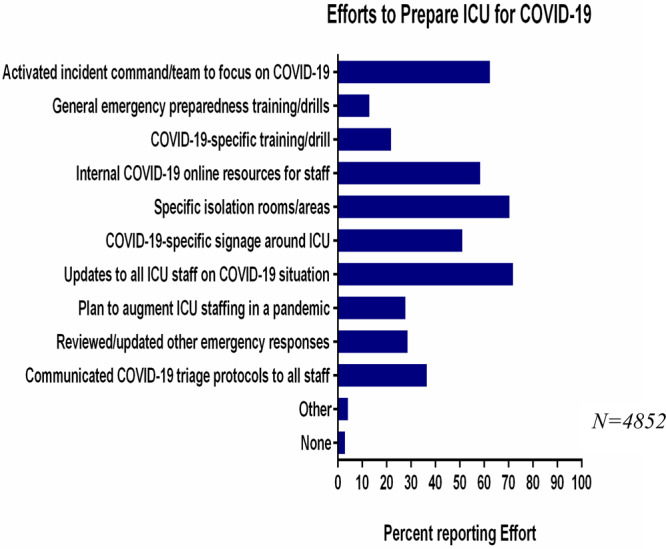
ICU clinician reports of efforts to prepare for coronavirus disease 2019 (COVID-19) patients.
More than half (2,699, 56.3%) noted that their ICU planned to cohort COVID-19 patients should negative-pressure room capacity be exceeded (Table 2). A majority of respondents (n = 4,010, 82.9%) reported the use of techniques to add critical care bed capacity. Specifically employed measures included rescheduling elective surgeries to increase ICU bed availability (n = 3,557, 73.5%), preparing in-hospital non-ICU spaces to accommodate ICU-level care (n = 2,323, 48%), preparing temporary spaces for patient intake or for the care of noncritically ill patients (e.g., tents, portable buildings, n = 1,168 [24.1%]), as well as leveraging external permanent facilities as remote care centers (e.g., free-standing outpatient clinics, ambulatory surgery centers, n = 589 [12.2%]) (Fig. 6). Less than half of respondents (n = 2,310, 47.5%) report being equipped with a telemedicine system to augment care capacity and oversight.
Figure 6.
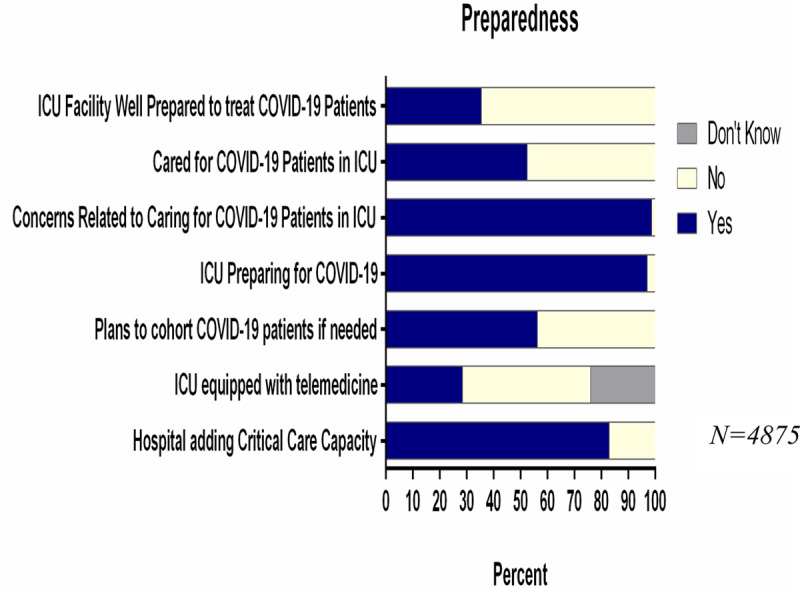
ICU clinician perceptions of level of preparedness for managing coronavirus disease 2019 (COVID-19) patients.
Practice Setting Differences
Practice setting appeared to influence the specific approach to preparation. Metropolitan practices more commonly established specific isolation rooms or areas, internally generated online education and guidance resources, developed clinician communication focused on COVID-19, and activated practices to augment beds and ICU clinician staffing. More ICU clinicians working in metropolitan areas (72.7%) reported caring for presumed or confirmed COVID-19 patients, compared with 22.9% in micropolitan and 4.4% in rural settings.
Facility Differences
Similar to geographic differences, facility orientation (academic, community, federal) also impacted preparation efforts. Academic centers (71.6%) more commonly activated a leadership team to address COVID-19 activities compared with only 58% of community facilities. More, but still relatively few, academic centers (34.1%) developed or updated a plan to augment ICU staffing in a pandemic. Despite the paucity of academic centers engaged in staff expansion efforts, the percentage exceeded that of community hospitals (25%).
A total of 70.5% of academic centers created internal COVID-19 online resources for staff utilization, compared with 42.9% of federal hospitals. More federal hospitals (21%) conducted general emergency preparedness training or drills within the last 90 days compared with only 11% of community hospitals. Similarly, more federal hospitals (31%) conducted COVID-19 specific training or drills compared with 19% of community sites.
Professional Differences
Physicians were more likely to believe that their facility and ICU team were well-prepared to care for COVID-19 patients (51%) compared with nurses (30%). Similarly, physicians (41.4%) were less concerned regarding the lack of uniform clinical guidance and treatment strategy compared with nurses (57.3%); respiratory therapists were similar to physicians with regard to such concerns (40.9%). More physicians (52.1%) reported that the ICU had developed or updated a plan to augment ICU staffing in a pandemic compared with 21.4% of nurses. It is not clear if this represents differences in practice settings, perception, or information sharing.
With respect to ICU resource shortages (e.g., supplies, medications, beds), 86.1% of pharmacists and 83.2% of nurses expressed concerns compared with 72.3% of respiratory therapists. More physicians (74.2%) identified concerns over patient surge and overcrowding compared with 58.5% of nurses and 55.3% of respiratory therapists. More nurses (37.6%) expressed concern regarding salary and benefits during periods of quarantine compared with only 17.3% of physicians.
Working With Presumed or Confirmed COVID-19 Patients
More nurses (70.2%) reported working with presumed or confirmed COVID-19 patients compared with 14.7% of physicians, 6.9% of advanced practice providers, 5.2% of respiratory therapists, and 2.1% of pharmacists.
Most (73.4%) of those who cared for a presumed or confirmed COVID-19 patient in the ICU work in an institution that updated all ICU staff on COVID-19 related information. A nearly similar proportion (72.1%) of those with presumed or confirmed COVID-19 patient care work in an institution with designated isolation rooms or areas; 58.5% of such respondents noted plans for COVID-19 patient cohorting when patient volume exceeded the number of negative pressure rooms. Concerns regarding surge and patient overcrowding were more commonly reported in those who had cared for a COVID-19 positive or presumed positive patient (57.6%) compared with those without contact (42.4%).
Only 28.1% of those who cared for a presumed or confirmed COVID-19 patient were equipped with an ICU telemedicine support system.
DISCUSSION/IMPLICATIONS
This survey reflects the perceptions and concerns of a spectrum of ICU team members with regard to preparation for COVID-19 patient care during the early unfolding of the pandemic within the United States. Although some facilities have disaster plans already in place for mass casualty care, as well as natural or man-made disaster, the scope of pandemic care engendered by COVID-19 as it sweeps across the world, is of unprecedented scale. Therefore, the typical preparations that would come with enacting a disaster plan may not meet the needs for the surge volume or the location for surge care for which facilities may be previously prepared. Although facilities share their preparation activities, it is the perception of the staff working within the facility that offer a lens through which to view the completeness and timeliness of those preparations. Herein lies the value of this particular survey.
Our results note that healthcare workers are much more concerned about facility preparation to respond to the realities of patient care than they are about their salary or benefits. This is characteristic of the intensive care professional, regardless of primary training—patients come first. Although financial compensation did not seem to be a significant factor in COVID-19 readiness, nurses were significantly more likely to report concern regarding salary and benefits during periods of quarantine compared with physicians. Noting the salary differential between physicians and nurses, this could reflect perceptions of the financial implications of being unable to work after inadvertent exposure to a COVID-19 patient that leads to quarantine at home.
With a highly transmissible disease such as COVID-19, direct patient care easily becomes a threat to personal safety of the medical provider. Through this inherent personal risk, concerns regarding facility resources surface. It is unsurprising that concerns regarding PPE, medications and space are raised across the spectrum of team members. The remainder of facility preparation reflects facility orientation and perhaps, staff expectations, despite the apparent need for increased uniformity. Nurses were less likely to identify that their facility and ICU team were well prepared to care for COVID-19 patients compared with physicians. Nurses were also less likely to report that the ICU had developed a plan to augment ICU staffing compared with physicians. It is not clear if this represents differences in practice settings, perception, or information sharing.
Academically oriented facilities appear to engage in a wider scope of facility preparation compared with community or federal facilities among the respondents. It is important to note that these differences may simply reflect the breadth of resources available to academic facilities that are generally tertiary or quaternary referral centers. It is easier to do more with a broader array of individuals and a more robust panel of clinicians and other resources. Such resources include but are not limited to information technology and medical informatics support, both of which are readily leveraged in facility preparedness. Although none of those elements were directly captured by survey elements, each of those are typically different between facility types and favor academic centers with resource array availability.
At the time of this survey, not all respondents had provided COVID-19 patient care. Once care is rendered to a person under investigation, or an individual presumed or confirmed COVID-19 positive, that experience informs one’s perception of preparation adequacy and raises concerns regarding resources. It is relevant to note that most respondents were critical care nurses, reflecting the usual composition of the ICU team in terms of numbers and direct contact time. Furthermore, while the bedside nurse generally remains as a fixed asset within a particular ICU, other team members including physicians, respiratory therapists, and to a lesser extent, advanced practice providers and pharmacists may have other responsibilities within a facility. Those team members more likely rotate through the ICU instead of having it be their sole site of work. Therefore, the seemingly asymmetric exposure to COVID-19 patients between nurses and physicians may reflect the reality of workflow and ICU exposure.
An important concern is the availability of negative pressure airborne infection isolation rooms (AIIRs) throughout a facility. Although the initial influx of COVID-19 positive patients may be managed in (AIIRs), it is expected that the surge volume will overwhelm the number of such rooms. The conversion of traditional rooms to those with negative pressure capability requires resources that do not impact PPE, medications, nor ICU staff but enable care to proceed with enhanced safety. Such enhancements do bear a financial and labor cost but may help preserve the limited supply of healthcare workers who are essential during pandemic care.
Equally important to address is the apparent lack of telemedicine—and in particular, telecritical care support services. Academic centers that are supported by fellows and in-house high-level trainees may not commonly use such services but may find a key role for telecritical care especially as they craft ICUs in nontraditional spaces. Roving telecritical care carts, and even robots, may increase safety and enable advanced guidance even while there is no intensivist physically present. Community and federal facilities may find similar benefit as ICU volume and care requirements exceed their usual tenor and pace. Telecritical care may become a priority during pandemic care, and current services may also find themselves overwhelmed. Like in-person critical care, remote telecritical care also leverages a team-based approach (13).
This study has several limitations including a low response rate—perhaps influenced by the ongoing pandemic, asymmetry between specialties and a nonuniform exposure rate of exposure to COVID-19 patient care. Nonetheless, it does represent the breadth of facilities, team members and their concerns. Although the survey was geared to U.S. ICU clinicians, some respondents may have also practiced in other countries. Although zip codes were collected, the country of practice was not assessed. The data provides insight into how facility preparation is progressing as the COVID-19 pandemic spreads across the United States. As this is an early investigation, it is expected that the data will shift as patient surge directly influences facility response, and colors healthcare worker perception and practice. We did not assess individual adaptation but instead inquired about facility level changes and clinician perceptions. As such, there is no hard data on activity and its efficacy regarding patient care or outcomes. Such data will require sufficient experience in providing COVID-19 patient care to understand the impact of specific approaches on care quality and outcome. Instead, we investigated what concerns clinicians harbor as they prepare to be potentially overwhelmed in a way for which no prior training has resulted in sufficient preparation. In this way, our data outlines areas for future inquiry to determine whether concerns articulated at this point were valid, or if ones unanticipated were more relevant.
CONCLUSIONS
ICU clinicians of all types are preparing to manage patients at risk of, or with confirmed COVID-19 infection. Common concerns include the adequacy of facility and team preparation, as well as ICU resource availability such as PPE, medications, and staff. The number and scope of facility activities appear to reflect facility orientation, and perhaps available resources, with academic facilities outperforming community and federal ones. As anticipated, ICU clinicians placed patient care concerns well ahead of personal ones. Structural enhancements such as increasing the availability of negative pressure rooms and the expansion of telecritical care services within hospitals may support healthcare professionals as well as patient safety. This early survey offers areas of specific inquiry that may be reinvestigated as COVID-19 patient care sweeps across the United States.
ACKNOWLEDGMENTS
Society of Critical Care Medicine, Fundamentals of Disaster Management Committee members are acknowledged for their work in survey question development.
Footnotes
Dr. Maves is a United States military service member. This work was prepared as part of his official duties. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Title 17 U.S.C. §105 provides that “Copyright protection under this title is not available for any work of the United States Government.” Title 17 U.S.C. §101 defines a U.S. Government work as a work prepared by a military service member or employee of the U.S. Government as part of that person’s official duties. The opinions and assertions contained herein are those of the authors and do not reflect the official views or position of the Department of the Navy, Department of Defense, nor of the U.S. Government.
REFERENCES
- 1.World Health Organization. Naming the Coronavirus Disease (COVID-19) and the Virus That Causes It. Available at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it. Accessed April 6, 2020
- 2.World Health Organization. Q&A on Coronaviruses (COVID-19). Available at: https://www.who.int/news-room/q-a-detail/q-a-coronaviruses. Accessed April 6, 2020
- 3.World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. World Health Organization (WHO Press release) Available at: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---23-march-2020. Accessed April 6, 2020 [Google Scholar]
- 4.Johns Hopkins University. John Hopkins Coronavirus Resource Center. 2020. Available at: https://coronavirus.jhu.edu/map.html. Accessed April 10, 2020
- 5.Alhazzani W, Møller MH, Arabi YM, et al. Surviving sepsis campaign: Guidelines on the management of critically ill adults with coronavirus disease 2019 (COVID-19). Crit Care Med. 2020 Mar 27. online ahead of print [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Murthy S, Gomersall CD, Fowler RA. Care for critically ill patients with COVID-19. JAMA. 2020; 323:1499–1500 [DOI] [PubMed] [Google Scholar]
- 7.Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020; 323:1239–1242 [DOI] [PubMed] [Google Scholar]
- 8.Bhatraju PK, Ghassemieh BJ, Nichols M, et al. Covid-19 in critically ill patients in the Seattle Region — case series. N Engl J Med. 2020 Mar 30. online ahead of print [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hui DS, I Azhar E, Madani TA, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—the latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. 2020; 91:264–266 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA. 2020; 323:1574–1581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Grasselli G, Pesenti A, Cecconi M. Critical care utilization for the COVID-19 outbreak in Lombardy, Italy: Early experience and forecast during an emergency response. JAMA. 2020; 323:1545–1546 [DOI] [PubMed] [Google Scholar]
- 12.Halpern NA, Tan KS. United States Resource Availability for COVID-19. Society of Critical Care Medicine. Available at: https://sccm.org/Blog/March-2020/United-States-Resource-Availability-for-COVID-19. Accessed April 6, 2020.
- 13.Lilly CM, Mullen M. Critical care surge management: A role for ICU telemedicine and emergency department collaboration. Crit Care Med. 2019; 47:1271–1273 [DOI] [PubMed] [Google Scholar]