

Abstract
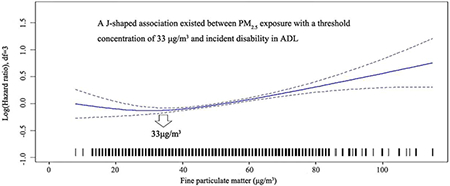
Currently the Chinese government has adopted World Health Organization interim target-1 values as the national ambient air quality standards values. However, the population-based evidence was insufficient, especially for the oldest old (aged 80+). We evaluated the association of fine particulate matters (PM2.5) exposure and incidence of disability in activities of daily living (ADL) in 15 453 oldest old in 886 counties/cities in China from 2002 to 2014 using Cox model with penalized splines and competing risk models to evaluate the linear or non-linear association. After adjusting for potential confounders, a J-shaped association existed between PM2.5 exposure with a threshold concentration of 33 μg/m3, and incident disability in ADL. Above this threshold, the risk magnitude significantly increased with increase of PM2.5 concentrations; compared to 33 μg/m3, the hazard ratio ranged from 1.03 (1.00-1.06) at 40 μg/m3 to 2.25 (1.54-3.29) at 110 μg/m3. The risk magnitude was not significantly changed below this threshold. Each 10 μg/m3 increase in PM2.5 exposure corresponded to a 7.7% increase in the risk of disability in ADL (hazard ratio 1.077, 95% CI 1.051-1.104). Men, smokers, and participants with cognitive impairment might be more vulnerable to PM2.5 exposure. The study provided limited population-based evidence for the oldest old and detected a threshold of 33 μg/m3, and supported that reduction to current World Health Organization interim target-1value (35 μg/m3) and Chinese national ambient air quality standards (35 μg/m3) or lower may be associated with lower risk of disability in ADL.
Keywords: PM2.5, disability, air pollution, oldest old, cohort study
Capsule:
A J-shaped association existed between long-term PM2.5 exposure with a threshold concentration of 33 μg/m3 and incident disability in ADL.
Graphical Abstract
1. Introduction
Worldwide, aging-related physical disability has become a critical health concern with the rapidly growing number of older adults, who comprise the largest group of people with disabilities1. In China, the population aged 60 years and older with physical disability is predicted to reach 64.02 million by 2020, and 140 million by 20502, 3. Regarded as a key indicator of overall health for older adults, disability represents a person’s ability to perform usual tasks and activities, which are essential for self-care and independent living4. Elevated exposure to air pollution, especially over a long-term duration, is associated with various adverse health problems, such as increased risks for cardiovascular and respiratory diseases5, 6. Given that physical disability is a common functional consequence of these subclinical pathologic processes and co-morbid chronic diseases, it is likely that exposure to air pollution also influences physical disability in older age.
Evidence is growing for an association between ambient air pollution exposure and physical functioning of older adults7–12. Despite this, several knowledge gaps are identified in the prior literature: (1) prior studies mainly focused on older adults younger than age 80 years, although it is likely that adults within an older cohort may be extremely vulnerable to the negative effects of air pollution exposure given functional organ decline13. (2) previous studies have mainly focused on either a composite air pollution index (API) or nitrogen oxides (NOx) but have not assessed fine matter with a diameter <2.5 μm (PM2.5) exposures, which are generally believed to be a primary driver of air pollution related adverse health. (3) Prior studies have been mostly conducted in developed countries where population exposures to PM2.5 are low, such as Europe and North America. China, the largest developing country with a relatively high level of exposure to air pollution14, is at a different stage of the epidemiologic transition, which means the conclusions drawn from developed countries may not reflect the situation in China. (4) In part, due to the lack of more accurate exposure data, prior studies have been conducted examining primarily community-level exposures partly. For the current analysis, we were able to access monitoring data throughout China, using satellite remote sensing combined with a nationwide networking of PM2.5 monitoring15. (5) Prior studies were mainly cross-sectional study in design, or only accounting for acute effects of short-term exposures, while disability in activities of daily living (ADL) would be expected to relate to chronic, progressive effects of long-term exposure to air pollution16. (6) Prior studies used different measures of disability; and an internationally accepted measure was not used, such as Katz index of independence in ADL 17.
Currently, the Chinese government has adopted the World Health Organization (WHO) air quality interim target-1 values of 35 μg/m3 as the National Ambient Air Quality Standards (NAAQS) values15, 18, 19; these are expected to be updated when sufficient evidence from epidemiologic research conducted in Chinese populations becomes available. The concurrent rapid population aging and environmental degradation in China20 make it more urgent to study the role of air pollution in disability in ADL for oldest old (80+). With an attempt to contribute to the currently limited evidence, in this study, we analyzed data from a prospective cohort of the oldest old scattered across 866 community units (cities or counties) in 23 provinces of China, by exposure estimates derived from satellite observations; and determined disability in ADL by means of the Katz index and examined linear and non-linear dose-response relationships to explore the exposure limits most appropriate for the over 80 age group.
2. Materials and Methods
2.1. Study group
The study subjects were participants of the Chinese Longitudinal Healthy Longevity Survey (CLHLS). The study was chosen probabilistically to represent 85% of the total population of Chinese oldest old12,20 and a national range of exposures to PM9.5 in ambient air (Figure 1). All participants underwent triennial assessments during which they completed questionnaires and underwent evaluation of AD21. In 2002-2014, we enrolled 15 453 participants aged 80 and older (mean age, 92.3±7.3 years), with available geographic topography information, and independent ADL at baseline, including 8141 octogenarians (aged 80-89), 4472 nonagenarians (aged 90-99), and 2840 centenarians (aged 100 and older). Among 15453 participants, 7387, 3177, 4393, 496 participants were enrolled in 2002, 2005, 2008 and 2011 survey respectively; and 2326, 2441, 2836, and 1142 participants died before the incidence of disability in ADL in 2002, 2005, 2008 and 2011 survey respectively. Cohort members were followed from the date of recruitment until the date of disability in ADL, death, emigration, or 1 September 2014 (whichever came first). All procedures performed in studies were approved by the biomedical ethics committee of Peking University (IRB00001052-13074). Written informed consents were obtained from all participants included in the study by themselves or their proxy respondents.
Figure 1.
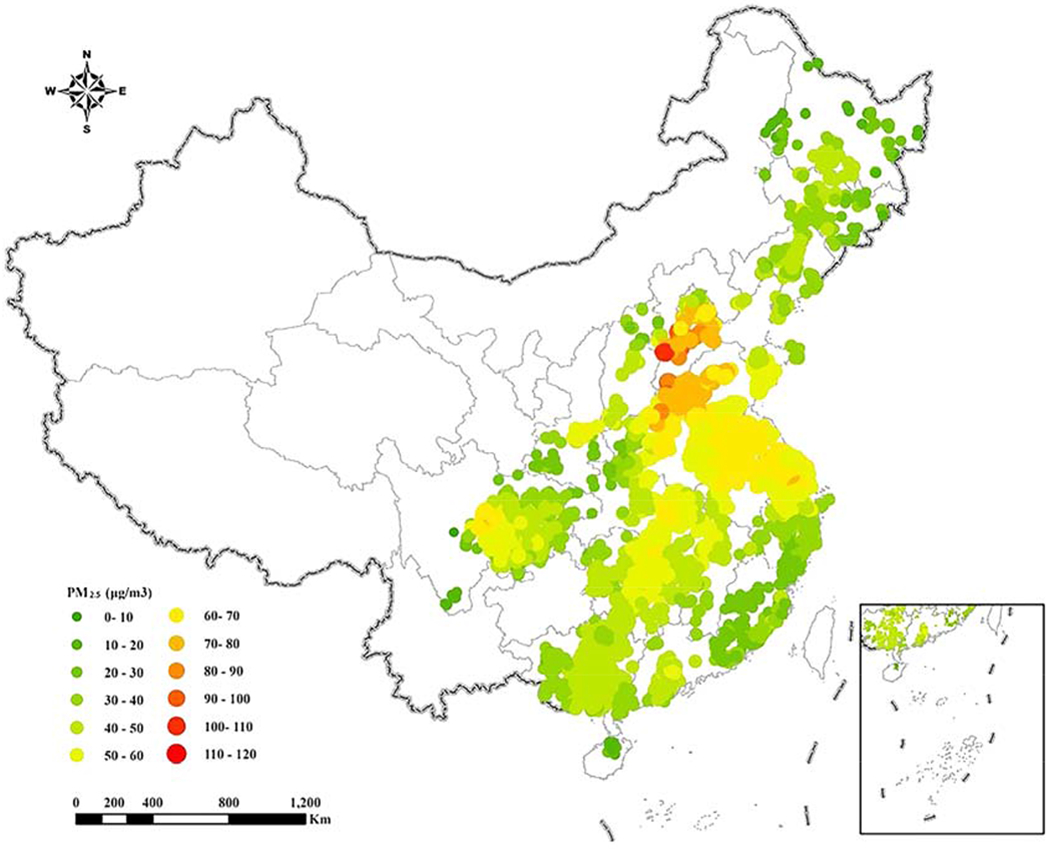
Annual average residential PM2.5 exposure with 0.01° spatial resolution (1.1x1.1 km) in 23 provinces of China at baseline for 15,453 participants
Annual average residential PM2.5 exposure at baseline ranged from 8.2 μg/m3 to 115.1 μg/m3, the mean annual PM2.5 exposure was 50.2 μg/m3 overall.
2.2. Exposure assessment
At baseline, we obtained geographic topography information from the community questionnaire of the CLHLS. Data on estimates of PM2.5 came from the Atmospheric Composition Analysis Group from using satellite-, simulation- and monitor-based information22. Annual average residential PM2.5 exposure with 0.01° spatial resolution (1.1×1.1 km) at the participants’ home addresses was estimated according to the year of survey, from satellite observations by combining Aerosol Optical Depth (AOD) retrievals from multiple satellite products (MISR, MODIS Dark Target, MODIS and SeaWiFS Deep Blue, and MODIS MAIAC)22. The resultant PM2.5 estimates were highly consistent (R2=0.81) with out-of-sample cross-validated PM2.5 concentrations from monitors22. Nearly all of the locations (99.3%) were sufficiently complete and correct to allow geocoding to an exact location; exposures were not updated given that only very few (2.1%) participants moved to another address. The correlation matrix of estimated PM2.5 showed that the exposures from the year of 2002 to 2014 were highly correlated, the correlation coefficient ranged from 0.86 to 0.98 (Table 1), which suggested that the baseline PM2.5 may be a good estimation of the exposure from recruitment to event incidence. PM2.5 in the recruitment year of 2002, 2005, 2008 and 2011 was therefore used in the analysis. The improved ambient air pollution estimates from satellite monitoring may have lower exposure misclassification bias than the exposure estimates that relied only on fixed-location monitoring station.
Table 1.
The correlation matrix of PM2.5 exposure from the year of 2002 to 2014 (N = 453) †
| PM2.5 | 2002 | 2003 | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2002 | 1.00 | - | - | - | - | - | - | - | - | - | - | - | - |
| 2003 | 0.94 | 1.00 | - | - | - | - | - | - | - | - | - | - | - |
| 2004 | 0.94 | 0.89 | 1.00 | - | - | - | - | - | - | - | - | - | - |
| 2005 | 0.96 | 0.92 | 0.96 | 1.00 | - | - | - | - | - | - | - | - | |
| 2006 | 0.92 | 0.93 | 0.89 | 0.94 | 1.00 | - | - | - | - | - | - | - | - |
| 2007 | 0.94 | 0.96 | 0.89 | 0.93 | 0.94 | 1.00 | - | - | - | - | - | - | - |
| 2008 | 0.95 | 0.96 | 0.9 | 0.92 | 0.92 | 0.97 | 1.00 | - | - | - | - | - | - |
| 2009 | 0.94 | 0.94 | 0.88 | 0.9 | 0.9 | 0.95 | 0.98 | 1.00 | - | - | - | - | - |
| 2010 | 0.92 | 0.96 | 0.86 | 0.93 | 0.93 | 0.95 | 0.94 | 0.92 | 1.00 | - | - | - | - |
| 2011 | 0.95 | 0.94 | 0.88 | 0.93 | 0.93 | 0.96 | 0.96 | 0.96 | 0.96 | 1.00 | - | - | - |
| 2012 | 0.93 | 0.93 | 0.9 | 0.95 | 0.96 | 0.96 | 0.96 | 0.93 | 0.94 | 0.96 | 1.00 | - | - |
| 2013 | 0.93 | 0.96 | 0.84 | 0.91 | 0.93 | 0.95 | 0.95 | 0.95 | 0.96 | 0.98 | 0.95 | 1.00 | - |
| 2014 | 0.93 | 0.96 | 0.88 | 0.91 | 0.91 | 0.96 | 0.97 | 0.96 | 0.95 | 0.96 | 0.95 | 0.96 | 1.00 |
All the P value of the correlation coefficients were <0.001.
2.3. Outcome assessment
The internationally accepted Katz index of independence in ADL was used to assess disability17. Disability was identified if a participant needed help in any areas of the six daily tasks of dressing, eating, bathing, continence, toileting and cleaning themselves afterward, and indoor movement; a participant was considered independent if no help was required with any ADL. This resulted in scores ranging from 0 to 6; higher scores indicated better ADL. Participants who scored 5 or less were identified as disability in ADL; scored 6 were identified as normal ADL. The Katz index has been used in a variety of epidemiologic studies of aging, and has well-established reliability and validity23, more details on Katz index were described in Supplementary 1.
2.4. Statistical analysis
To explore the linear or non-linear associations of PM2.5 with disability in ADL, Cox models with penalized splines were conducted24. Based on the corrected Akaike Information Criterion (AIC), 3 degrees of freedom for PM2.5 (coded as a continuous variable) were selected for the association analyses. Cox models with penalized splines showed a statistically significant J-shaped association for PM2.5 with disability in ADL. Participants with 33 μg/m3 had the minimum risk of disability in ADL based on the estimated parameters of penalized splines (J-shaped exposure-response function) after adjustment for the confounders. The hazard ratios (HRs) and 95% confidence intervals (CI) were evaluated for every 10μg/m3 interval of PM2.5 concentrations for 10, 20, 30, 40, 50, 60, 70, 80, 90, 100 and 110 μg/m3 in Cox models with penalized splines adjusting for the confounders, with reference to 33 μg/m3. A number of potential confounding factors were measured, including age (continuous), sex, residence, current marital status, living pattern, educational level, occupation, source of income, parity, playing cards, smoking status, alcohol consumption, physical activity, hypertension, heart disease, cerebrovascular disease, diabetes mellitus, respiratory disease and cognitive impairment at baseline, based on the existing literature25, and included in the final model specification. Living pattern has been defined as “living with family members” or “living alone or at nursing home”. Educational level was classified as illiterate and literate since most Chinese adults aged 80 and older didn’t receive any formal education. Occupation was categorized as farmer or non-farmer. Source of income was categorized as pension or other. Parity was the number of children and used as continuous variable. Smoking status was defined into three categories: current, former, and never. Alcohol drinking status was defined into three categories: current, former, and never. Data on the prevalence of chronic diseases such as heart disease, cerebrovascular disease, diabetes mellitus, and respiratory disease were collected. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) at baseline enrollment were measured to determine the presence of hypertension (SBP≥140 mmHg, DBP≥90 mmHg). Cognitive impairment was defined as the score of mini-mental status examination lower than 24. In the final analytic database, although less than 0.7% of individuals had missing data for any individual covariates, multiple imputation methods were used to impute missing values of covariates.
To correctly estimate the marginal probability of disability in ADL in the presence of mortality, competing risk models were constructed to estimate risk of disability in ADL for each 10 μg/m3 increase in PM2.5 adjusted for the above confounders. Using Cox models with penalized splines, we evaluated potential modifiers of an effect between PM2.5 and disability in ADL such as sex, smoking status, residence, cognitive function, subgroup analyses in men and women, smokers and non-smokers, urban participants and rural participants, participants with cognitive impairment and normal cognition. Additionally, interactions between those modifiers and PM2.5 for disability in ADL were tested.
To assess the robustness of the observed associations, a number of sensitivity analyses were conducted. (1) The predicted PM2.5 concentrations were averaged at each of her/his residential locations from recruitment to event incidence, characterizing the historic long-term exposures. (2) Models were repeated for the participants who did not move to another address during the follow-up survey, even though address changes were only observed in very few of participants. (3) Crude models and models adjusted only for sex and age were also constructed, for adjusted variables may be plausible intermediates on the causal pathway. (4) Analyses were conducted excluding the participants lost to follow-up. (5) Models were conducted with a relatively “healthy” designation, by excluding individuals diagnosed with the comorbidities (heart disease, cerebrovascular disease, diabetes mellitus, and respiratory disease).
A P-value threshold of 0.05 was used to assess statistical significance. All analyses were carried out using SAS version 9.4 (SAS Inc., Cary, NC, USA) and R 3.4.2 (R foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Study participants
In total, the analysis included data from 15 453 individuals (Table 2). The mean age of the participants was 92.3±7.3 years; 43.9% were men and 18.0% lived in urban areas at baseline. Annual average residential PM2.5 exposure at baseline ranged from 8.2 μg/m3 to μg/m3 (Figure 1). The mean annual PM2.5 exposure was as follows: 50.2 μg/m3 overall; 49.5 μg/m3 for rural residents; 53.4μg/m3 for urban residents; 49.9 μg/m3 for participants with independent ADL; and 51.4 μg/m3 for participants with disability in ADL. The mean (standard deviation, SD) of the follow-up time for included participants was 4.6 (3.1) years. Over a follow-up period of 71 396 person-years, 3373 (21.8%) incident cases of disability in ADL were ascertained.
Table 2.
Baseline characteristics of the study participants by disability in ADL status (N = 15,453).
| Characteristics | All | Independent ADL | Disability in ADL | P value |
|---|---|---|---|---|
| Number of participants* | 15453 (100) | 12080 (78.2) | 3373 (21.8) | |
| Age (year)# | 92.3±7.3 | 91.9±7.2 | 93.8±7.4 | <0.001 |
| Sex | <0.001 | |||
| Men* | 6790 (43.9) | 5507 (45.6) | 1283 (38.0) | |
| Women* | 8663 (56.1) | 6573 (54.4) | 2090 (62.0) | |
| Residence | <0.001 | |||
| Urban* | 2781 (18.0) | 2016 (16.7) | 765 (22.7) | |
| Rural* | 12672 (82.0) | 10064 (83.3) | 2608 (77.3) | |
| Marital status | 0.022 | |||
| In marriage* | 4083 (26.4) | 3140 (26.0) | 943 (28.0) | |
| Not in marriage* | 11370 (73.6) | 8940 (74.0) | 2430 (72.0) | |
| Education | 0.009 | |||
| Illiteracy* | 10420 (67.4) | 8083 (66.9) | 2337 (69.3) | |
| Literacy* | 5033 (32.6) | 3997 (33.1) | 1036 (30.7) | |
| Living pattern | <0.001 | |||
| Live with family members* | 12325 (79.8) | 9544 (79.0) | 2781 (82.4) | |
| Live alone or at nursing home* | 3128 (20.2) | 2536 (21.0) | 592 (17.6) | |
| Tobacco smoking | <0.001 | |||
| Current* | 10454 (67.7) | 8077 (66.9) | 2377 (70.5) | |
| Former* | 2929 (19.0) | 2372 (19.6) | 557 (16.5) | |
| Never* | 2070 (13.4) | 1631 (13.5) | 439 (13.0) | |
| Alcohol drinking | <0.001 | |||
| Current* | 10630 (68.8) | 8193 (67.8) | 2437 (72.3) | |
| Former* | 3364 (21.8) | 2718 (22.5) | 646 (19.2) | |
| Never* | 1459 (9.4) | 1169 (9.7) | 290 (8.6) | |
| Regular exercise | 5329 (34.5) | 4090 (33.9) | 1239 (36.7) | 0.002 |
| Hypertension* | 7827 (51.3) | 5992 (49.6) | 1835 (54.4) | |
| Heart disease* | 937 (6.1) | 670 (5.5) | 267 (7.9) | <0.001 |
| Diabetes* | 178 (1.2) | 130 (1.1) | 48 (1.4) | 0.095 |
| Cerebrovascular disease* | 415 (2.7) | 292 (2.4) | 123 (3.6) | <0.001 |
| Respiratory disease* | 1615 (10.5) | 1321 (10.9) | 294 (8.7) | <0.001 |
| Cognitive impairment* | 3488 (22.6) | 2751 (22.8) | 737 (21.8) | 0.257 |
| PM2.5 (ug/m3)# | 50.2±13.4 | 49.9±13.2 | 51.4±14.3 | <0.001 |
ADL: activities of daily living; PM2.5: fine particulate matter with diameter <2.5 μm
Indicating categories variables displayed as sample size (%)
Indicating continuous variables displayed as mean±SD.
3.2. Association between PM2.5 and disability in ADL
Using a Cox model with penalized splines adjusted for potential confounders, a J-shaped association was observed between PM2.5 exposure and disability in ADL with a threshold concentration of 33 μg/m3. Above this threshold, the risk magnitude significantly increased with increase of PM2.5 concentrations; not significantly changed blow this threshold. Compared to 33 μg/m3, the hazard ratios for different PM2.5 thresholds of exposure of 10, 20, 30, 40, 50, 60, 70, 80, 90, 100 and 110 μg/m3 were 1.09(0.86-1.39), 1.02(0.89-1.17), 0.99 (0.93-1.06), 1.03 (1.00-1.06), 1.11 (1.09-1.14), 1.23 (1.20-1.27), 1.38 (1.31-1.45), 1.54 (1.41-1.71), 1.75 (1.48-2.07), 1.98 (1.53-2.58) and 2.25 (1.54-3.29) respectively (Figure 2). The value at which the curve becomes significantly non-zero was 40 μg/m3. The competing risk models showed that each 10 μg/m3 increase in PM2.5 exposure corresponded to a 7.7% increase in the risk of disability in ADL (HR 1.077 [1.051-1.104]).
Figure 2.
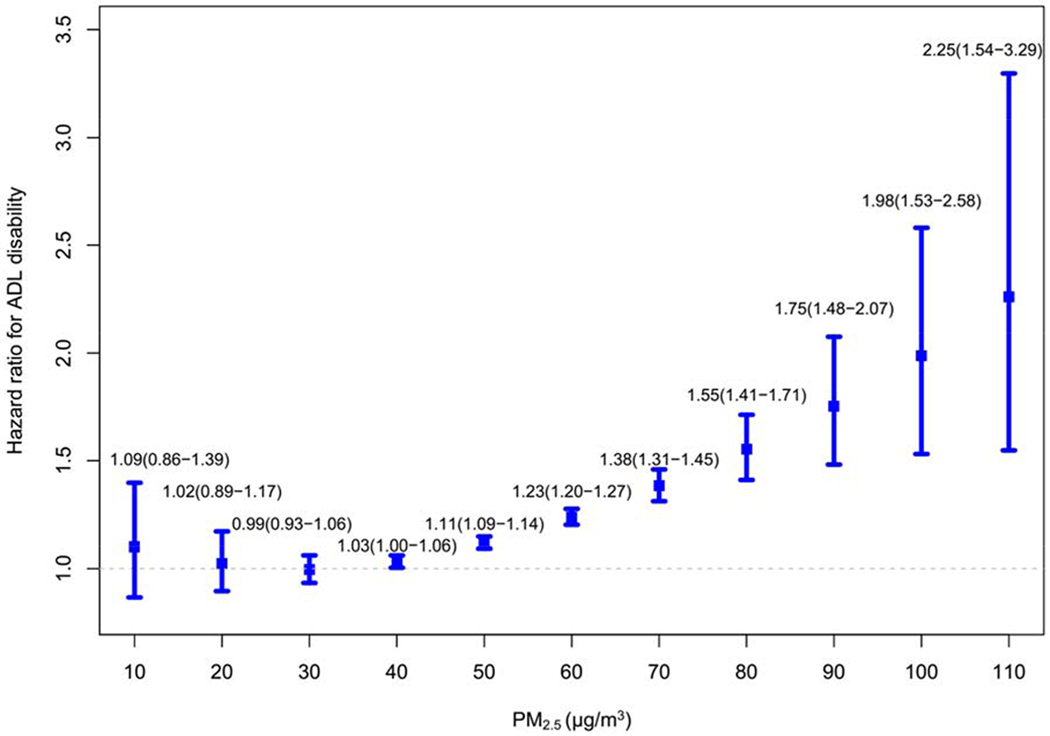
Association of PM2.5 and disability in ADL in Cox models with penalized splines among Chinese oldest old (33 μg/m3 as reference).a
a Adjusting for age, sex, residence, current marital status, living pattern, educational level, occupation, source of income, parity, playing cards, smoking status, alcohol consumption, physical activity, hypertension, heart disease, cerebrovascular disease, diabetes mellitus, respiratory disease and cognitive impairment at baseline.
3.3. Sub-group and sensitivity analyses
Significant interactions of sex (P=0.012), smoking status (P=0.008), and cognitive function (P<0.001) with PM2.5 for disability in ADL were observed; there were no significant interactions of residence location with PM2.5. Men, smokers, and participants with cognitive impairment might be more vulnerable to the effects of long-term PM2.5 exposure (Figure 3). The associations of PM2.5 and disability in ADL were unchanged or slightly strengthened in the various sensitivity analyses that included the following: lagging 1-, 2-, 3-, 4-years exposure period exposure (Supplementary Table S1).; averaging exposures from baseline to the event, excluding participants with address changes, only adjusting for sex and age, excluding participants lost to follow-up, and excluding participants with comorbidities (Supplementary Table S2).
Figure 3.
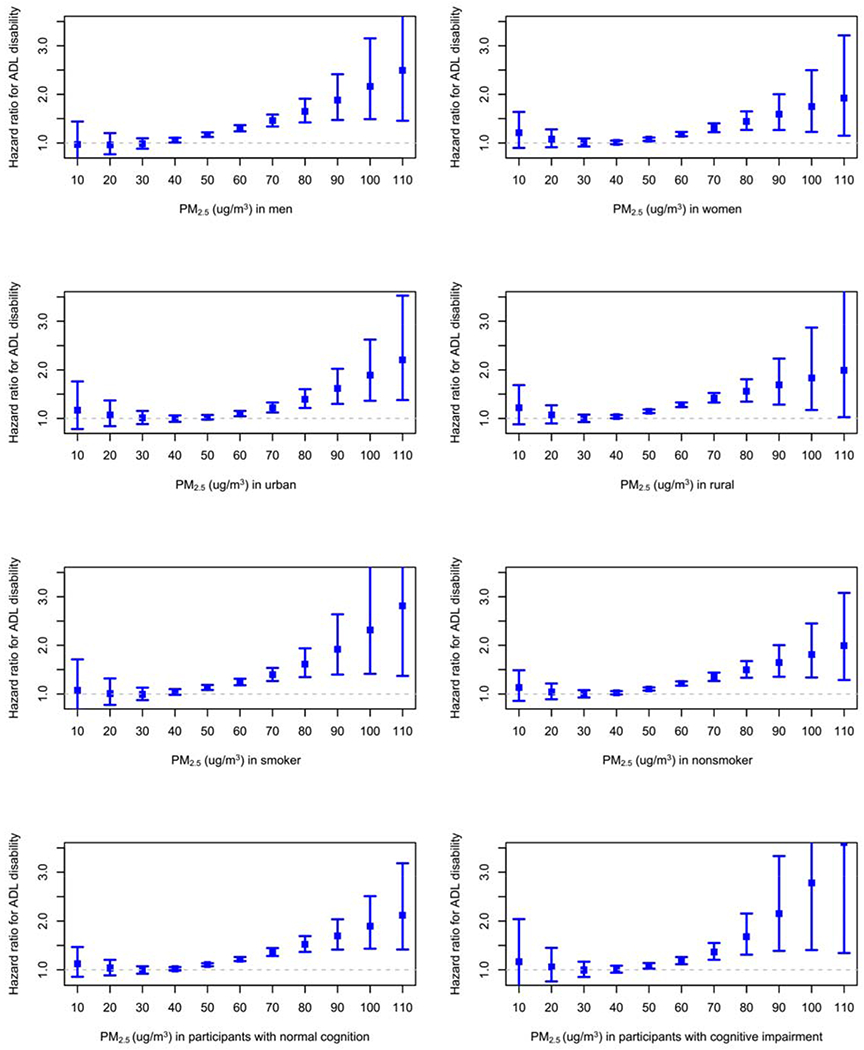
Subgroup analyses: association of PM2.5 and disability in ADL in Cox models with penalized splines among Chinese oldest old (33 μg/m3 as reference).
a Adjusting for age, sex, residence, current marital status, living pattern, educational level, occupation, source of income, parity, playing cards, smoking status, alcohol consumption, physical activity, hypertension, heart disease, cerebrovascular disease, diabetes mellitus, respiratory disease and cognitive impairment at baseline
4. Discussion
In this prospective cohort study of community-based oldest old, higher risk of disability in ADL incidence occurred among those with individual, higher long-term exposure to PM2.5. In addition, men, smokers, and participants with cognitive impairment might be more vulnerable to this effect. Our study adds to the current limited evidence of an adverse effect of PM2.5 on physical functioning in oldest old; to our knowledge, this is the first cohort study to demonstrate the association for this specific age group. The major contribution of our study is the identification of the threshold value (33 μg/m3) of PM2.5 for disability in ADL incidence in a large subsample of oldest-old living in 866 highly diverse counties and cities in a nationwide representative study. The strengths of this study also included standard measurements of disability, exposure estimation at an individual level, extensive information regarding important confounding factors, accounting for possible bias from selective attrition and use of Cox models with penalized splines to estimate the shape of the dose-response relationship.
4.1. Previous studies
Our findings are generally consistent with the limited prior epidemiological evidence focusing on older adults. In the cross-sectional study of the 2002 wave of the CLHLS, a higher API at the county or city level was associated with a 25% higher risk of disability in ADL among Chinese older adults aged 65+7. The study of the CLHLS 2002-2005 wave also revealed a decrease in 3-yr self-reported health expectancies with increasing API at the county or city level8. In a cohort of 1762 Dutch older adults aged 55 to 85, long-term exposure to air pollution, such as NO2, PM10, and PMcoarse, adversely affected performance-based and self-reported physical functioning9. A recent study from Chicago using NOx as an indicator of traffic-related air pollution identified a significant association between long-term air pollution exposure and progression in physical disability among older adults10. An early study reported an association of short-term exposure to PM2.5 with increased disability days11. A cross-sectional study among more than 45 000 adults (mean age: 56 years) from China, Ghana, India, Mexico, Russia, and South Africa showed that exposure to ambient PM2.5 might be one risk factor for disability with women and older adults as the vulnerable population12.
Unlike the majority of the prior cross-sectional studies, as a prospective cohort study, the present study makes it possible to identify a more confident relationship between PM2.5 exposure and disability in ADL. Our ability to estimate exposures at an individual level provides unique and valuable data to complement those prior studies at a community-based level. Notably, the hazard ratio for oldest old in our study was significantly higher than in other studies conducted in adults or younger elderly in the general population7–12. The oldest old generally have worse health conditions, which may diminish their ability to adapt to air pollution exposure. In consideration of the unique characteristics for those aged 80+, the extent to which our results might generalize to other age groups are unclear.
4.2. Explanations
There are known or postulated biological mechanisms that support the plausibility of an association between ambient PM2.5 exposure and disability. Inhaled fine particles may enter by direct translocation through the olfactory bulb, then could elicit inflammatory responses and oxidative stress26, which have also been one pathological pathway of the occurrence of disability10. Higher air quality promotes outdoor physical activities, which may protect against risk for subsequent disability in ADL and enhance recovery after the onset of disability in ADL23. It is also possible that chronic exposure to PM2.5 could result in damage in methylation of DNA repair genes27, which may be linked to disability. Because disability and health status were likely to be results of PM2.5 exposure rather than causes of it, and because of our use of a prospective cohort study design, reverse causality is not likely to be a big concern in the present study. Additionally, selection bias was partly examined by a number of sensitivity and subgroup analyses.
The association between PM2.5 and disability in ADL has appeared to be stronger in men, has also been reported previously28. Specifically, we hypothesize that this may be attributable more time spent outdoors, higher level of physical activity in daily life required more air inhalation for men, leaded to higher accumulation of toxic chemicals from the air than women. Notably, participants with cognitive impairment were not as adept at handling these added stressors and, therefore, have a higher risk of disability in ADL as a result of the exposure21. Not surprisingly, it was found that the adverse effects of PM2.5 exposure were greater in smokers, considering the combined effects of air pollution and smoking on health29.
In a large epidemiologic study, personal air monitoring devices is impractical, especially for measuring long-term exposures. By contrast, GIS-based spatiotemporal models offered the ability to estimate individual annual average exposures at baseline and averaged exposures from baseline to the event for the 15 453 participants, which has been validated and applied in previous studies22. The exposure measurements were based on participants’ residential locations, and thus limited by the assumption that participants spent most of their time at home; an assumption we believe to be reasonable for the oldest old in this study.
Policy implications
The study found that the oldest old may be more vulnerable to the negative effects of long-term air pollution exposure. It suggested detailed measurements targeting on different populations including the general adults, younger elderly and the oldest old may be needed to identify the high-risk population and give their priority to health protection in the rural and urban regions. Additionally, in the published integrated exposure-response model for long-term exposure of PM2.5 from global burden of diseases, the concentration range of 50-100 μg/m3 were estimated by second-hand smoke due to the gap of epidemiological evidence on high ambient PM2.5 exposure and health outcome from developing countries30. The developing countries, was similar to the PM2.5 exposure and at a similar different stage of the epidemiologic transition to China. Future studies are needed to investigate whether the conclusions drawn from in China can be transferred to other developing countries with similar characteristics. The results will provide important policy implications to policy-makers and service providers in the disciplines of health and environmental protection, especially in the developing countries such as China and India31.
Increasing awareness of the harmful effects of air pollution has led to the development of guidelines to prevent excess exposure to these toxicants. For better air quality management to protect public health, the Chinese NAAQS were revised by adopting the interim target values in air quality guidelines in 2012, in which concentration limits for annual averages of PM2.5 were 35 μg/m3,18,19. However, the formulation of air quality standards requires integrated assessments of risks of air pollution attributable to disease burden and feasibility of environmental management32. Our results support that reduction to current WHO air quality interim target-1 and Chinese national ambient air quality standards (35 μg/m3) may be associated with lower risk of disability in ADL. It highlight more air pollution health researcher were needed to explore the benefits of continued reductions for cleaner air (i.e., 10ug/m3 for PM2.5 annual average) in setting up health risk management-based air quality standards in China..
4.3. Limitations
Several limitations merit attention. First, our study provides only indirect evidence for an effect of PM2.5 exposure since air pollution is a complex mixture in which PM2.5 is one component among many. Second, only outdoor exposures to PM2.5 were estimated based on residential location, insufficient adjustment of indoor air pollution (such as household solid fuel use), second-hand smoking and other air pollutants, which may lead to potential confounding32, may comprise a limitation in this study. Third, in this study, more accurate estimation of PM2.5, such as the PM2.5 exposure at actually date of survey, were not available, even though lagging 1-, 2-, 3-, 4-years exposure period exposure were matched. Fourth, it is possible that there is information bias in the design of the present study, as a result that disability in ADL could be occurred at any time during a 2- to 3-year interval of follow-up, the exact date of the event was not collected. Fifth, potential reversibility of the incident disability in ADL when performing Cox models may weaken the robustness of the present finding, although the probability of reversible physical disability was relatively low for this population of oldest old with an average age of 92.3±7.3 years.
5. Conclusions
We observed a clear J-shaped dose-response relationship of long-term exposure to PM2.5 with corresponding disability in ADL incidence among Chinese oldest old; the risk magnitude increased with increments of PM2.5 concentrations. This association was detected at a threshold of 33 μg/m3, which was basically consistent with current Chinese NAAQS, demonstrating that current annual averages for PM2.5 in NAAQS can be sufficient for mitigating excess risk of disability in ADL from long-term PM2.5 exposures for those aged 80+. Therefore, air pollution reduction may be a means for reducing the public health burden of disability and increasing the quality of life of the older adults-particularly aged 80+, men, smokers and people with cognitive impairment. However, the generality of our findings should be further confirmed in other studies.
Supplementary Material
Highlights.
The dose-response relationship between long-term PM2.5 exposure and ADL was J-shaped
The identification of a threshold of 33 μg/m3 for PM2.5 and ADL disability incidence
The first cohort study to demonstrate effect of PM2.5 on ADL for the oldest old
Air pollution reduction may reduce the public health burden of disability in the elderly.
Acknowledgments
We are grateful to all participating people and their families. We acknowledge all staffs and postgraduates for their great contributions to the program.
Funding
This work was supported by National Natural Sciences Foundation of China (81273160, 81573247, and 71490732), the U.S. National Institute on Aging (2P01AG031719, 5P30AG028716) and United Nations Fund for Population Activities.
Role of the funding source
The financial supporters had no involvement in study design, data collection, analysis and interpretation of data, writing of the report, and decision to submit the article.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of Interest
None.
References:
- 1.GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017; 390: 1211–1259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.China aging problem national commission, China ministry of civil affairs, China ministry of finance. The fourth survey on the living conditions of urban and rural elderly in China. 2016. [Google Scholar]
- 3.Qian J, Chen Y, Rao K, et al. Trends analysis and prediction on disability of China mainland aging population and policy suggestion. Chin J Health Stat 2012; 29: 6–9. [Google Scholar]
- 4.Artaud F, Dugravot A, Sabia S, et al. Unhealthy behaviours and disability in older adults: three-City Dijon cohort study. BMJ 2013; 347: f4240. [DOI] [PubMed] [Google Scholar]
- 5.Kaufman JD, Adar SD, Barr RG; et al. Association between air pollution and coronary artery calcification within six metropolitan areas in the USA (the Multi-Ethnic Study of Atherosclerosis and Air Pollution): a longitudinal cohort study. Lancet 2016; 388: 696–704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Guan WJ, Zheng XY, Chung KF, et al. Impact of air pollution on the burden of chronic respiratory diseases in China: time for urgent action. Lancet 2016; 388: 1939–1951. [DOI] [PubMed] [Google Scholar]
- 7.Zeng Y, Gu D, Purser J, et al. Associations of environmental factors with elderly health and mortality in China. Am J Public Health 2010; 100:298–305. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wen M, Gu D. Air Pollution Shortens Life Expectancy and Health Expectancy for Older Adults: The Case of China. J Gerontol A Biol Sci Med Sci 2012; 67:1219–1229. [DOI] [PubMed] [Google Scholar]
- 9.de Zwart F, Brunekreef B, Timmermans E, et al. Air Pollution and Performance-Based Physical Functioning in Dutch Older Adults. Environ Health Perspect 2018; 126:017009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jennifer W, Kaufman JD, Szpiro AA, et al. Exposure to traffic-related air pollution in relation to progression in physical disability among older adults. Environ Health Perspect; 2016, 124:1000–1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Stieb D M, Smith-Doiron M, Brook J R, et al. Air pollution and disability days in Toronto: results from the national population health survey. Environ Res 2002; 89:210–219. [DOI] [PubMed] [Google Scholar]
- 12.Lin H, Guo Y, Yang Z, et al. Exposure to ambient PM2.5, associated with overall and domain-specific disability among adults in six low- and middle-income countries. Environ Int 2017; 104:69–75. [DOI] [PubMed] [Google Scholar]
- 13.Zeng Y, Feng Q, Hesketh T, et al. Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. Lancet 2017; 389:1619–1629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yin P, He Q Fan M, et al. Particulate air pollution and mortality in 38 of China’ s largest cities: time series analysis. BMJ 2017; 356: j667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.World Health Organization. WHO | WHO Global Urban Ambient Air Pollution Database (update 2016). 2016. WHO; http://www.who.int/phe/health_topics/outdoorair/databases/cities/en/ [Google Scholar]
- 16.Tak E, Kuiper R, Chorus A, et al. Prevention of onset and progression of basic ADL disability by physical activity in community dwelling older adults: a meta-analys is. Ageing Res Rev 2013; 12: 329–338. [DOI] [PubMed] [Google Scholar]
- 17.Katz S, Ford AB, Moscowitz RW, et al. The index of ADL: A standardized meas ure of biological and psychosocial function. JAMA 1963; 185:914–919. [DOI] [PubMed] [Google Scholar]
- 18.MEP (Ministry of Environmental Protection of China). Ambient Air Quality Stand ards. (Document GB 3095-2012). Beijing: Ministry of Environmental Protection of the People’s Republic of China; 2012. [Google Scholar]
- 19.World Health Organization. WHO Air quality guidelines for particulate matter, ozone, nitrogen dioxide and sulfur dioxide: global update 2005: summary of risk assessment. Geneva: World Health Organization, 2006. [Google Scholar]
- 20.Zhang J, Mauzerall DL, Zhu T, et al. Environmental health in China: progress to wards clean air and safe water. Lancet 2010; 375: 1110–1119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lv YB, Gao X, Yin ZX, et al. Revisiting the association of blood pressure with mortality in the oldest old: a community-based longitudinal prospective study in China. BMJ 2018; 361: k2158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.van Donkelaar A, Martin RV, Brauer M, et al. Global Estimates of Fine Particulate Matter using a Combined Geophysical-Statistical Method with Information from Satellites, Models, and Monitors. Environ Sci Technol 2016; 50: 3762–3772. [DOI] [PubMed] [Google Scholar]
- 23.Yang M, Ding X, Dong B. The measurement of disability in the elderly: a systematic review of self-reported questionnaires. J Am Med Dir Assoc 2014; 15: 150.e1–9. [DOI] [PubMed] [Google Scholar]
- 24.Eisen EA, Agalliu I, Thurston SW, et al. Smoothing in occupational cohort studies: an illustration based on penalised splines. Occup Environ Med 2004; 61:854–860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gill TM, Guralnik JM, Pahor M, et al. Effect of structured physical activity on overall burden and transitions between states of major mobility disability in older persons. Ann Intern Med 2016; 165:833–840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Tzivian L, Winkler A, Dlugaj M, et al. Effect of long-term outdoor air pollution and noise on cognitive and psychological functions in adults. Int J Hyg Environ Health 2015; 218:1–11. [DOI] [PubMed] [Google Scholar]
- 27.Neven KY, Saenen ND, Tarantini L, et al. Placental promoter methylation of DNA repair genes and prenatal exposure to particulate air pollution: an ENVIRONAGE cohort study. Lancet Planet Health 2018; 2: e174–e183. [DOI] [PubMed] [Google Scholar]
- 28.Liu T, Zhang Y H, Xu Y J, et al. The effects of dust-haze on mortality are modified by seasons and individual characteristics in Guangzhou, China. Environ Pollut 2014; 187:116–123. [DOI] [PubMed] [Google Scholar]
- 29.Lin H, Guo Y, Kowal P, et al. Exposure to air pollution and tobacco smoking an d their combined effects on depression in six low- and middle-income countries. Br J Psychiatry 2017; 211:157–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lelieveld J, Klingmüller K, Pozzer A, et al. Cardiovascular disease burden from ambient air pollution in Europe reassessed using novel hazard ratio functions. Eur Heart J, 2019, 40: 1590–1596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cohen AJ, Brauer M, Burnett R, et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet, 2017, 389: 1907–1918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kan HD. A review of standard value of fine particulate matter (PM(2.5)) ruled by National Ambient Air Quality Standards (GB3095-2012) in China. Chin J Prev Med 2012; 46:396–398. [PubMed] [Google Scholar]
- 33.GBD 2013 Risk Factors Collaborators, Forouzanfar MH, Alexander L, et al. Global, regional, and national comparative risk assessment of 79 behavioral, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015; 386:2287–2323. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.