

Abstract
Aims
Heart failure with mid‐range ejection fraction (HFmrEF) has been proposed as a distinct HF phenotype, but whether patients on this category fare worse, similarly, or better than those with HF with reduced EF (HFrEF) or preserved EF (HFpEF) in terms of rehospitalization risks over time remains unclear.
Methods and results
We prospectively included 2961 consecutive patients admitted for acute HF (AHF) in our institution. Of them, 158 patients died during the index admission, leaving the sample size to be 2803 patients. Patients were categorized according to their EF: HFrEF if EF ≤ 40% (n = 908, 32.4%); HFmrEF if EF = 41–49% (n = 449, 16.0%); and HFpEF if EF ≥ 50% (n = 1446, 51.6%). Covariate‐adjusted incidence rate ratios (IRRs) were used to evaluate the association between EF status and recurrent all‐cause and HF‐related admissions. At a median follow‐up of 2.6 years (inter‐quartile range: 1.0–5.3), 1663 (59.3%) patients died, and 6035 all‐cause readmissions were registered in 2026 patients (72.3%), 2163 of them HF related. Rates of all‐cause readmission per 100 patients‐years of follow‐up were 150.1, 176.9, and 163.6 in HFrEF, HFmrEF, and HFpEF, respectively (P = 0.097). After multivariable adjustment, when compared with that of patients with HFrEF and HFpEF, HFmrEF status was not significantly associated with a different risk of all‐cause readmissions (IRR = 0.99; 95% confidence interval [CI], 0.77–1.27; P = 0.926; and IRR = 0.93; 95% CI, 0.74–1.18; P = 0.621, respectively) or HF‐related readmissions (IRR = 1.06; 95% CI, 0.77–1.46; P = 0.725; and IRR = 1.11; 95% CI, 0.82–1.50; P = 0.511, respectively).
Conclusions
Following an admission for AHF, patients with HFmrEF had a similar rehospitalization burden and a similar risk of recurrent all‐cause and HF‐related admissions than had patients with HFrEF or HFpEF. Regarding morbidity risk, HFmrEF seems not to be a distinct HF phenotype.
Keywords: Heart failure, Readmissions, Heart failure with mid‐range ejection fraction, Recurrent events
Introduction
Rehospitalization burden in patients with heart failure (HF) remains very high. 1 , 2 , 3 These readmissions carry important and negative consequences, being related to a poor quality of life and an increased mortality risk, but also accounting for large health care expenditures. 1 , 2 , 3 Overall, readmission burden is similar between patients with HF and reduced ejection fraction (HFrEF) and patients with preserved ejection fraction (HFpEF). 4 , 5 The latest 2016 European Society of Cardiology (ESC) HF Guidelines proposed a distinct category for patients with an EF between 40% and 49%, which was HF with mid‐range EF (HFmrEF), calling for research to fill the knowledge gaps regarding this new entity. 1 Several studies have addressed the epidemiological, clinical, and prognostic differences between HFmrEF and the classical phenotypes of HF ever since, but results have varied considerably across different studies, and very few of them have focused on the morbidity risk. 6 , 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16
Traditionally, the ‘time‐to‐first’ event approach has been the classical method to evaluate the risk of adverse events in HF, including readmission risks. However, in recent years, some experts have argued in favour of replacing classical time‐to‐first analyses with recurrent event methodology. 17 , 18 , 19 . This longitudinal approach would better quantify the hospitalization burden over lifetime in a chronic disease such as HF, and it is being increasingly adopted in recent years, as it is the case of important recent clinical trials in HF, such as the PARAGON‐HF. 20
In this study, we sought to evaluate the readmission burden in patients with HFmrEF and to analyse whether patients in this new category fare worse, similarly, or better in terms of rehospitalization risks than do patients with HFrEF and HFpEF, by means of a recurrent event analysis.
Methods
Study population
We prospectively include a cohort of 2961 consecutive patients admitted for acute HF in the cardiology department of a tertiary teaching hospital (Hospital Clínico Universitario, Valencia‐Spain), from 2004 to 2017. Of them, 158 patients died during the index admission, leaving the final sample size to be 2803 patients. Patients with either new‐onset or worsening HF were included in the registry. A comprehensive set of variables was routinely recorded at baseline using pre‐established registry questionnaires. Left ventricular EF (LVEF) was assessed by two‐dimensional transthoracic echocardiogram in every patient during index hospitalization (96 ± 24 h after admission). LVEF was calculated by the biplane Simpson method. Three commercially available systems were used throughout the study, Agilent Sonos 5500 ie33 and EPIQ 7C (Philips, Massachusetts, USA). HF categories were defined according to the 2016 HF ESC Guidelines: HFrEF (EF < 40%), HFmrEF (EF = 41–49%), and HFpEF (EF ≥ 50%). Treatment with angiotensin‐converting enzyme inhibitors, angiotensin receptor blockers, beta‐blockers, aldosterone antagonist, diuretics, and other therapeutic strategies were individualized by physicians' criteria in clinical daily practice according to established guidelines that were operating by the time patients were included in the registry.
Follow‐up and endpoints
The incidence of recurrent all‐cause and HF‐related rehospitalizations during follow‐up was selected as the primary endpoint. Only unplanned readmissions were included. HF‐related readmissions were those in which worsening or acute HF was the main diagnosis at discharge. Hospitalizations were adjudicated based on the paper‐written and electronic discharges records from every hospital in our health care system. All‐cause mortality was evaluated as a sensitivity analysis. Researchers in charge of endpoints adjudications were all blinded to the HF category.
Ethical concerns
The study was prospectively designed, conformed to the principles outlined in the 1975 Declaration of Helsinki, and approved by the institutional local review ethics committee. All patients gave informed consent.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) or median (inter‐quartile range), whenever appropriate. Discrete variables were summarized as percentages. Baseline continuous variables were compared across HF categories with ANOVA, adopting Kruskal–Wallis test for non‐parametric variables. A descriptive analysis of recurrent events was performed by counting the number of hospitalizations during the entire follow‐up. Crude incidence rates (expressed as number of readmissions per 100 person‐years) were calculated for each readmission endpoint across HF categories. The following aspects were important on how to analyse the data: (i) a concern about informative censoring in HF, meaning that an increase in readmission risks would lead to an associated increase in the risk of subsequent death; and (ii) patient's follow‐up is usually truncated at death as a terminal event, precluding new hospitalizations and potentially introducing bias regarding recurrent event analyses. To overcome these pitfalls, we used bivariate negative binomial regression (NBreg) models that simultaneously model the number of readmissions (as counts) and mortality (as terminal event). Regression estimates for both outcomes are mutually adjusted by means of shared frailty (accounting for the positive correlation between the two outcomes). 21 Completeness of follow‐up was calculated with the Clark or completeness index C (92.5%). The independent association between HFmrEF and recurrent hospitalizations was assessed with either HFrEF or HFpEF as reference categories. Estimates of risk were expressed as incidence rate ratios (IRRs). All variables listed in Table 1 were evaluated as potential covariates in the NBreg models, independently of their P value. A backward stepwise selection, with a P value of 0.157 (Akaike information criterion) for variable inclusion, was used to achieve parsimonious models and prevent model's overfitting. 22 , 23 The covariates included in the multivariable clinical models were as follows: age, sex, no prior HF admission, Charlson co‐morbidity index, heart rate at admission, systolic blood pressure at admission, blood urea nitrogen, haemoglobin, New York Heart Association (NYHA) functional class prior at admission, treatment with beta‐blockers, treatment with mineral receptor antagonists, and the N‐terminal pro‐brain natriuretic peptide (NT‐proBNP). All the covariates included in the model were 100% complete except for Charlson index, prior NYHA class, and NT‐proBNP, that were available in 2785 (98.1%), 2751 (98.1%), and 2612 (93.2%) of the cases. In these cases, we performed a multiple imputation, avoiding dropping such cases.
Table 1.
Baseline characteristics in heart failure patients stratified according to ejection fraction
| HFrEF (n = 908) | HFmrEF (n = 449) | HFpEF (n = 1446) | P value | |
|---|---|---|---|---|
| Demographics | ||||
| Age, years | 70 ± 12 | 75 ± 10 | 76 ± 10 | <0.001 |
| Female, n (%) | 273 (30.1) | 176 (39.2) | 932 (64.4) | <0.001 |
| Medical history | ||||
| Prior NYHA class III–IV, n (%) | 138 (15.2) | 74 (16.5) | 229 (15,8) | 0.556 |
| No prior HF admission, n (%) | 481 (53.0) | 223 (49.7) | 806 (53.9) | 0.063 |
| Hypertension, n (%) | 657 (72.4) | 377 (83.9) | 1168 (80.8) | <0.001 |
| Diabetes mellitus, n (%) | 400 (44.1) | 236 (52.6) | 612 (42.3) | <0.001 |
| Current smoker, n (%) | 175 (19.3) | 63 (14.0) | 105 (7.3) | <0.001 |
| Ischaemic heart disease, n (%) | 407 (44.8) | 203 (45.2) | 383 (26.5) | <0.001 |
| ICD carrier, n (%) | 60 (6.9%) | 11 (2.3%) | 5 (0.4%) | <0.001 |
| CCI > 2, n (%) | 323 (35.6) | 180 (40.1) | 440 (30.4) | <0.001 |
| QRS > 120 ms, n (%) | 384 (42.3) | 176 (39.2) | 323 (22.3) | <0.001 |
| Atrial fibrillation, n (%) | 293 (32.3) | 186 (41.4) | 764 (52.8) | <0.001 |
| Vital signs at admission | ||||
| Heart rate, b.p.m. | 101 ± 26 | 99 ± 27 | 98 ± 30 | 0.042 |
| Systolic blood pressure, mmHg | 140 ± 31 | 150 ± 34 | 150 ± 33 | <0.001 |
| Diastolic blood pressure, mmHg | 82 ± 19 | 84 ± 21 | 80 ± 19 | <0.001 |
| Echocardiography | ||||
| LVEF, % | 31.3 ± 6.3 | 44.9 ± 2.5 | 61.6 ± 7.4 | <0.001 |
| LV diastolic diameter, mm | 63.0 ± 7.9 | 57.7 ± 8.1 | 49.9 ± 7.0 | <0.001 |
| Left atrium diameter, mm | 44.0 ± 7.9 | 43.9 ± 8.4 | 43.9 ± 8.0 | 0.453 |
| Deceleration time, ms | 185 ± 55.6 | 209.4 ± 66.8 | 223.1 ± 58.5 | <0.001 |
| E/e′ ratio | 18.7 ± 8.5 | 17.4 ± 7.2 | 18.5 ± 11.2 | 0.263 |
| TAPSE, mm | 17.6 ± 8.4 | 18.1 ± 3.0 | 19.5 ± 6.0 | <0.001 |
| PASP, mmHg | 42.8 ± 10.2 | 45.0 ± 31.3 | 47.0 ± 16.0 | <0.001 |
| Laboratory | ||||
| BUN, mg/dL | 58.9 ± 31.6 | 61.3 ± 30.6 | 60.1 ± 30.5 | 0.377 |
| Haemoglobin, g/dL | 12.9 ± 1.9 | 12.7 ± 1.9 | 12.1 ± 1.9 | <0.001 |
| Sodium, mEq/L | 138.5 ± 4.2 | 138.9 ± 4.3 | 138.4 ± 4.7 | 0.121 |
| NT‐proBNP, pg/mL a | 5923 (8109) | 5612 (7913) | 3530 (5230) | <0.001 |
| Serum creatinine at admission, mg/dL | 1.31 ± 0.6 | 1.36 ± 0.7 | 1.23 ± 0.6 | <0.001 |
| Treatment at discharge | ||||
| Furosemide dose, mg | 71.7 ± 43.5 | 69.5 ± 45.5 | 63.1 ± 43.1 | <0.001 |
| Beta‐blockers, n (%) | 691 (76.1) | 316 (70.4) | 937 (64.8) | <0.001 |
| ACEI or ARB, n (%) | 668 (71.9) | 298 (64.9) | 917 (61.8) | <0.001 |
| MRA, n (%) | 519 (54.2) | 132 (27.9) | 220 (14.3) | <0.001 |
ACEI, angiotensin‐converting enzyme inhibitor; ARB, angiotensin‐II receptor blockers; b.p.m., beats per minute; BUN, blood urea nitrogen; CCI, Charlson co‐morbidity index; E/e′, ratio of mitral peak velocity of early filling (E) to early diastolic mitral annular velocity (e′); HF, heart failure; HFrEF, heart failure with reduced ejection fraction; HFmrEF, heart failure with mid‐range ejection fraction; HFpEF, heart failure with preserved ejection fraction; ICD, implantable cardiac defibrillator; LV, left ventricular; LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonist; NT‐proBNP, N‐terminal pro‐brain natriuretic peptide; NYHA, New York Heart Association functional class; PASP, pulmonary artery systolic pressure; TAPSE, tricuspid annular plane systolic excursion.
Values are mean ± standard deviation or n (%).
Values are median (inter‐quartile range).
A two‐sided P value of <0.05 was considered to be statistically significant for all analyses. All survival analyses were performed using STATA 15.1 (StataCorp. 2015. Stata Statistical Software: Release 14.1. College Station, TX: StataCorp LP). The ‘Bivcnto’ Stata module was used in the multivariable regression models for bivariate count outcomes.
Results
Baseline characteristics
Mean age of the cohort was 73.6 ± 11.1 years, 1381 (49%) were women and 1293 (46%) had been previously admitted for acute HF. The distribution of the cohort across HF categories was as follows: HFrEF, n = 908 (32.4%); HFmrEF, n = 449 (16.0%); and HFpEF, n = 1446 (51.6%). Table 1 summarizes baseline characteristics stratified by the HF category according to EF status. Overall, patients with HFmrEF had mostly an intermediate clinical profile when compared to patients with HFrEF or HFpEF. For instance, age, prevalence of female sex, atrial fibrillation, echocardiographic signs of right ventricular systolic dysfunction or pulmonary hypertension, NT‐proBNP levels, or the use of HF medications were in‐between in HFmrEF when compared with the classical phenotypes. In some other clinical features, such as ischaemic heart disease or renal dysfunction, HFmrEF patients resembled more HFrEF. HFmrEF patients showed the highest prevalence of cardiovascular risk factors such as hypertension or diabetes, and a high profile of co‐morbidities, as expressed with the Charlson co‐morbidity index.
All‐cause readmissions
At a median follow‐up of 2.6 years (1.0–5.3), a cumulative total of 6035 all‐cause readmissions were registered in 2026 patients (72.3%). Of note, 865 (42.7%) and 379 (18.7%) patients were readmitted ≥3 or ≥5 times along the follow‐up, respectively. No significant differences in the crude incidence rates of all‐cause readmissions were found across HF categories (P = 0.097). Rates per 100 person‐years of follow‐up for recurrent all‐cause hospitalizations across HF categories are shown in Figure 1 . However, after multivariate adjustment, and when compared with that in patients with either HFrEF or HFpEF, HFmrEF status was not significantly associated with a different risk of all‐cause readmissions (IRR = 0.99: 95% confidence interval [CI], 0.77–1.27; P = 0.926; and IRR = 0.93: 95% CI, 0.74–1.19; P = 0.578, respectively) (Figure 2 ). All the IRRs for the different comparisons among the three HF categories are shown in Table 2 . Interestingly, no differences were observed in the risk of all‐cause readmissions between the two classical HF phenotypes (HFrEF vs. HFpEF, Table 2 ).
Figure 1.
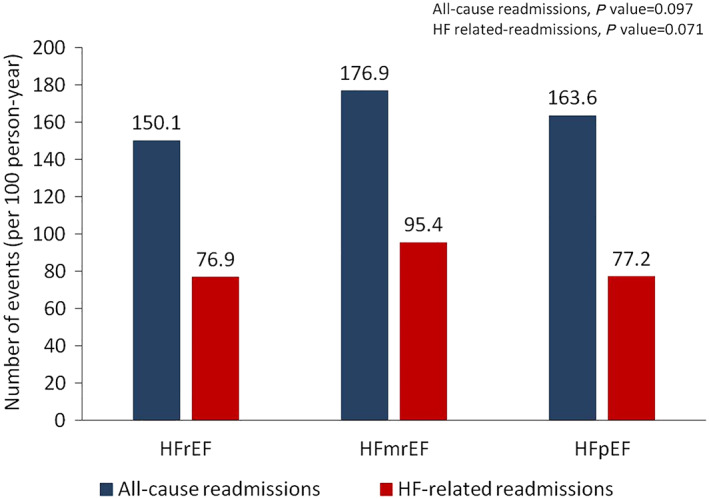
Crude incidence of all‐cause and HF‐related readmission rates in patients with HFrEF, HFmrEF, and HFpEF. HFmrEF, heart failure with mid‐range ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction. Completeness of follow‐up, using Clark C index, was 92.5%.
Figure 2.
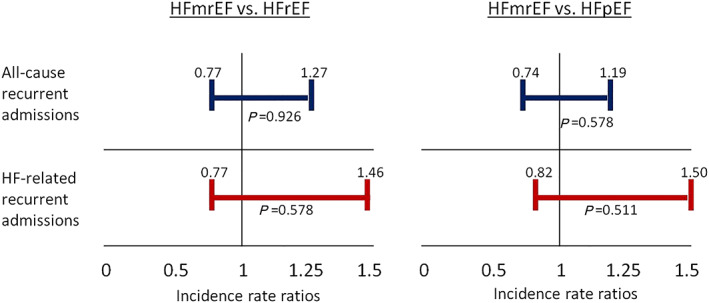
Risk of recurrent all‐cause and HF‐related hospitalizations in HFmrEF when compared with HFrEF or HFpEF in the multivariable regression models for bivariate count outcomes. HFmrEF, heart failure with mid‐range ejection fraction; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction.
Table 2.
Risk of all‐cause and heart failure‐related recurrent admissions in patients with heart failure with mid‐range ejection fraction when compared with those with heart failure with reduced ejection fraction and heart failure with preserved ejection fraction in the multivariate models
| NBreg models | IRR (95% CI) | P value | IRR (95% CI) | P value |
|---|---|---|---|---|
| All‐cause recurrent admissions | ||||
| HFrEF as reference | HFpEF as reference | |||
| HFmrEF | 0.99 (0.77–1.27) | 0.926 | 0.93 (0.74–1.19) | 0.578 |
| HFpEF/HFrEF a | 1.06 (0.85–1.32) | 0.621 | 0.95 (0–76‐1.18) | 0.621 |
| Heart failure‐related recurrent admissions | ||||
| HFrEF as reference | HFpEF as reference | |||
| HFmrEF | 1.06 (0.77–1.46) | 0.578 | 1.11 (0.82–1.50) | 0.511 |
| HFpEF/HFrEF a | 0.96 (0.72–1.27) | 0.761 | 1.04 (0.79–1.38) | 0.761 |
CI, confidence interval; HFrEF, heart failure with reduced ejection fraction; HFmrEF, heart failure with mid‐range ejection fraction; HFpEF, heart failure with preserved ejection fraction; IRR, incidence rate ratio; NBreg, negative binomial regression.
HFpEF vs. HFrEF and HFrEF vs. HFpEF, as indicated.
Heart failure‐related readmissions
A cumulative total of 2245 readmissions were registered in 1144 patients (40.8%). Crude incidence rates of HF‐related readmissions per 100 person‐years of follow‐up are shown in Figure 1 . These rates were numerically slightly higher in HFmrEF when compared with those in the other categories, but these differences were not significant (P = 0.071). After multivariable adjustment, estimates of risk remained unaltered. Thus, no significant differences were found in the risk of recurrent HF‐related hospitalizations in HFmrEF when compared with either HFrEF or HFpEF (IRR = 1.06; 95% CI, 0.77–1.46; P = 0.578; and IRR = 1.11; 95% CI, 0.82–1.50; P = 0.511, respectively) (Figure 2 ). All the IRRs for the different comparisons among the three HF categories are shown in Table 2 . In addition, there were again no differences in the risk of HF readmissions between HFrEF and HFpEF patients (Table 2 ).
All the covariates and their estimates in the multivariate NBreg models for both hospitalizations endpoints are presented in Table 3 .
Table 3.
All the covariates and their estimates in the multivariate negative binomial regression models for all‐cause and heart failure‐related recurrent admissions
| IRR (CI 95%) | P value | IRR (CI 95%) | P value | |
|---|---|---|---|---|
| All‐cause recurrent admissions | HF‐related recurrent admissions | |||
| Age | 1.03 (1.02–1.04) | <0.001 | 1.04 (1.03–1.05) | <0.001 |
| Male sex | 1.25 (1.05–1.50) | 0.013 | 1.03 (0.82–1.30) | 0.770 |
| No prior HF admission | 0.55 (0.47–0.66) | <0.001 | 0.13 (0.10–0.16) | <0.001 |
| Charlson index | 1.16 (1.10–1.22) | <0.001 | 1.12 (1.10–1.25) | <0.001 |
| SBP | 0.99 (0.99–0.99) | <0.001 | 0.99 (0.99–0.99) | 0.001 |
| Heart rate | 0.99 (0.99–1.00) | 0.126 | 0.99 (0.99–1.00) | 0.148 |
| Haemoglobin (g/dL) | 0.92 (0.88–0.96) | <0.001 | 0.92 (0.87–0.98) | 0.006 |
| BUN (g/dL) | 1.00 (0.99–1.00) | 0.119 | 1.00 (0.99–1.00) | 0.156 |
| Serum sodium | 0.99 (0.96–0.99) | 0.007 | 0.96 (0.94–0.98) | 0.001 |
| NT‐proBNP (pg/mL) | 1.00 (1.00–1.01) | 0.002 | 1.00 (1.00–1.01) | 0.002 |
| Prior NYHA class | 1.23 (1.08–1.39) | 0.001 | 1.13 (0.96–1.33) | 0.138 |
| Beta‐blockers | 0.81 (0.68–0.97) | 0.020 | 0.82 (0.66–1.03) | 0.089 |
| MRA | 0.83 (0.69–1.01) | 0.072 | 0.86 (0.67–1.11) | 0.252 |
BUN, blood urea nitrogen; CI, confidence interval; HF, heart failure; IRR, incidence rate ratio; MRA, mineralocorticoid receptor antagonist; NT‐proBNP, N‐terminal pro‐brain natriuretic peptide; NYHA, New York Heart Association; SBP, systolic blood pressure.
All‐cause mortality
A total of 1663 patients died (59.3%) in the follow‐up. By Kaplan–Meier analysis, patients with HFrEF showed the highest risk of long‐term all‐cause mortality (Figure S1 ). However, following multivariate adjustment, no significant differences in the risk of death across HF categories were found (HFmrEF vs. HFrEF: IRR = 0.96; 95% CI, 0.72–1.23; P = 0.779; and HFpEF vs. HFrEF: IRR = 0.96; 95% CI, 0.75–1.23; P = 0.758).
Discussion
In this large single‐centre registry, we found that all‐cause readmission rates of HFmrEF patients were similar to those seen in patients with HFrEF and HFpEF. Accordingly, HFmrEF status, when compared with HFrEF or HFpEF, was not associated with a different risk of recurrent all‐cause hospitalizations. With regard to HF‐related readmissions, incidence rates and the risk of HF‐related recurrent events were also comparable in the three HF categories.
A need for evaluating the risk of rehospitalizations in heart failure with mid‐range ejection fraction
HFmrEF was officially launched as a distinct entity in the 2016 ESC HF Guidelines. 1 One of the main objectives of this new phenotype was to encourage research to better elucidate clinical characteristics, prognosis, and treatment for patients with an EF between 41% and 49%. As recommended in the Guidelines, many studies had addressed all these open issues ever since, 6 , 7 , 9 , 11 , 12 , 13 , 14 , 15 , 16 , 24 , 25 but the adoption of this new category has been controversial. 26 , 27 In addition, despite that many studies have focused on the clinical profile or the mortality risk of HFmrEF, none of them have primarily focused on readmission risks. 6 , 7 , 9 , 11 , 12 , 13 , 14 , 15 , 16 , 24 , 25 Overall, prior studies on readmission risks in HFmrEF have shown conflicting results. For instance, two meta‐analyses assessing the prognosis in HFmrEF were published in 2018. 7 , 11 In the meta‐analysis by Altaie and Khalife, the risk of an HF‐related readmission was similar in HFmrEF when compared with that in HFpEF or HFrEF. 11 On the contrary, Lauritsen et al. reported that the risk of an HF rehospitalization was lower in HFmrEF than in HFrEF but was significantly higher than in HFpEF. 7 Nowadays, hospitalizations in HF are a matter of great interest. Hospital admissions are increasing worldwide, affecting patients' quality of life and increasing the risk of further adverse events. 1 , 2 , 3 In this context, further research into rehospitalization burden in HFmrEF seemed to be appropriate.
Risk of readmission in heart failure with mid‐range ejection fraction: a distinct phenotype?
As previously stated, prior studies have reported somewhat conflicting results in HFmrEF. In data from the ‘Get with the Guidelines’ registry, Shah et al. reported that patients with HFmrEF had slightly higher readmission rates than patients with HFpEF, whereas HF readmissions rates were intermediate between the two classical phenotypes. 14 On the contrary, survival free of all‐cause and HF readmissions was similar regardless of EF in the Trial of Intensified versus standard Medical Therapy in Elderly patients with Congestive Heart Failure (TIME‐CHF), 13 and along the same line, no differences were found in the incidence of HF readmissions across the three HF categories in a multicentre national cohort of 1241 patients discharged from acute HF in Spain, 24 in concordance with our results.
It is important to highlight that in all of these previous studies, readmission risks have been evaluated as a time‐to‐first event. Although this methodology is well recognized, it probably does not accurately reflect the hospitalization burden in HF. Nowadays, in order to capture the morbidity burden following an admission for acute HF in a more comprehensive way, some experts recommend to evaluate every readmission that occur during follow‐up, because recurrent events are the typical feature of HF disease progression. 17 , 18 , 19 The only study in which morbidity risk of HFmrEF patients has been reported according to this methodology has been conducted by Lund et al. on patients included in the Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) programme. 25 Patients with LVEF = 40–49%, when compared with HFpEF patients, showed a non‐significant trend to a higher risk of recurrent HF admissions. Such an analysis was not conducted for all‐cause rehospitalizations, in which, by a time‐to‐first analysis, it was somewhat surprising that HFmrEF status was associated with the lowest risk of readmission. CHARM included stable HF patients, whereas our patients were included following an admission for acute HF in ‘real‐world’ clinical daily practice. In our cohort, HFmrEF patients were considerably older and showed a higher prevalence of co‐morbidities than those from CHARM. Along this line, in the ESC‐HF Long‐Term (ESC‐HF‐LT) registry, the incidence of all‐cause and HF readmissions was also much lower in HFmrEF than in HFrEF. 9 These data had a deep impact on the results from the meta‐analysis of Lauritsen et al., resulting in a lower risk of HF readmissions in HFmrEF than in HFrEF. 7 As in CHARM, patients included in the ESC‐HF‐LT were stable, were relatively young, and showed a lower prevalence of co‐morbidities than did patients included in our registry (e.g. diabetes: 32.3% vs. 52.5%; atrial fibrillation: 18.3% vs. 41.7%, respectively). Conversely, patients in both the TIME‐CHF trial and the study by Gómez‐Otero were more similar to our cohort, 13 , 24 resulting in similar readmission risks in the three HF categories. We believe that such differences in the clinical profile of the patients may help to explain the different outcomes across studies and the conflicting results of previous meta‐analyses.
HFmrEF is a heterogeneous and controversial category. It has been stated that many patients in this category are indeed in transition from one classical HF phenotype to the other, mostly from HFrEF to the so‐called HF with improved or recovered EF. 28 , 29 , 30 We hypothesize that the clinical profile of patients with HFmrEF may be different depending on the clinical scenario. This ‘transitional’ HFmrEF phenotype may be more dominant in stable HF cohorts than in patients admitted for acute HF. For instance, 34.8% patients with an LVEF = 40–49% from the ESC‐HF‐LT registry were implantable cardiac defibrillator carriers. 9 The labelling of those patients with improved EF as HFmrEF may introduce significant bias, as patients with improved EF are a low‐risk cohort, 28 , 29 and this could help to explain the lowest risk attributed to HFmrEF in some of the previous studies.
In summary, our findings confirm the prohibitive burden of hospitalizations following an episode of acute HF regardless LVEF status. HFmrEF seems not to be a distinct phenotype with regard to readmission risks. In our opinion, we should move forward, leaving back the LVEF‐centric way of evaluating the HF‐associated morbidity. There is an unmet need for reducing the readmission burden in every HF patient, beyond their LVEF status.
Limitations
There are some limitations of our study that need to be acknowledged. First, this is a single‐centre observational study in which hidden bias might be operating. Second, data on LVEF prior to the index episode are scarce and preclude us to state definite conclusions on the percentage of patients with HF and improved EF in our cohort. In addition, longitudinal assessment of LVEF was out of the scope of the present study, so transitional changes in HF categories during the follow‐up were not evaluated. Fourth, we did not focus on any specific rehospitalization clustering in the follow‐up. Finally, the adoption of recurrent event methodology in the HF field is relatively new, so there might be areas still subjected to controversy. However, it seems to portray a more accurate evaluation of the morbidity burden than the traditional time‐to‐first event endpoints.
Conclusions
Following an admission for acute HF, patients with HFmrEF had a similar risk of recurrent all‐cause and HF‐related hospitalizations than had patients with either HFrEF or HFpEF. Further works aiming to unravel whether patients with HFmrEF exhibit crucial pathophysiological, clinical, or therapeutic singularities in HF are warranted.
Conflict of interest
None declared.
Supporting information
Figure S1. Kaplan–Meier all‐cause mortality curves according to left ventricular ejection fraction. HFmrEF: heart failure with mid‐range ejection fraction; HFpEF: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction.
Santas, E. , de la Espriella, R. , Palau, P. , Miñana, G. , Amiguet, M. , Sanchis, J. , Lupón, J. , Bayes‐Genís, A. , Chorro, F. J. , and Núñez Villota, J. (2020) Rehospitalization burden and morbidity risk in patients with heart failure with mid‐range ejection fraction. ESC Heart Failure, 7: 1007–1014. 10.1002/ehf2.12683.
References
- 1. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González‐Juanatey JV, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulus P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association of the ESC. Eur Heart J 2016; 37: 2129–2200. [DOI] [PubMed] [Google Scholar]
- 2. Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for heart failure. Problems and perspectives. J Am Coll Cardiol 2013; 61: 391–403. [DOI] [PubMed] [Google Scholar]
- 3. Ponikowski P, Anker SD, AlHabib KF, Cowie M, Force TL, Hu S, Jaarsma T, Krum H, Rastogi V, Rohde LE, Samal UC, Shimokawa H, Siswanto BB, Sliwa K, Filippatos G. Heart Failure: preventing disease and death worldwide. ESC Heart Failure 2014; 1: 4–25. [DOI] [PubMed] [Google Scholar]
- 4. Santas E, Valero E, Mollar A, García‐Blas S, Palau P, Miñana G, Núñez E, Sanchis J, Chorro FJ, Núñez J. Burden of recurrent hospitalizations following an admission for acute heart failure: preserved versus reduced ejection fraction. Rev Esp Cardiol (Engl Ed) 2017; 70: 239–246. [DOI] [PubMed] [Google Scholar]
- 5. Chun S, Tu JV, Wijeysundera HC, Austin PC, Wang X, Levy D, Lee DS. Lifetime analysis of hospitalizations and survival of patients newly admitted with heart failure. Circ Heart Fail 2012; 5: 414–421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Bambhani V, Kizer JR, Lima JAC, van der Harst P, Bahrami H, Nayor M, de Filippi CR, Enserro D, Blaha MJ, Cushman M, Wang TJ, Gansevoort RT, Fox CS, Gaggin HK, Kop WJ, Liu K, Vasan RS, Psaty BM, Lee DS, Brouwers FP, Hillege HL, Bartz TM, Benjamin EJ, Chan C, Allison M, Gardin JM, Januzzi JL, Levy D, Herrington DM, van Gilst WH, Bertoni AG, Larson MG, de Boer RA, Gottdiener JS, Shah SJ. Predictors and outcomes of heart failure with mid‐range ejection fraction. Eur J Heart Fail 2018; 20: 651–659. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lauritsen J, Gustafsson F, Abdulla J. Characteristics and long‐term prognosis of patients with heart failure and mid‐range ejection fraction compared with reduced and preserved ejection fraction: a systematic review and meta‐analysis. ESC Heart Fail 2018; 5: 685–694. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Hsu JJ, Ziaeian B, Fonarow GC. Heart failure with mid‐range (borderline) ejection fraction. Clinical implications and future directions. J Am Coll Cardiol HF 2017; 11: 763–771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Chioncel O, Lainscak M, Seferovic PM, Anker SD, Crespo‐Leiro MG, Harjola VP, Parissis J, Laroche C, Piepoli MF, Fonseca C, Mebazaa A, Lund L, Ambrosio GA, Coats AJ, Ferrari R, Ruschitzka F, Maggioni AP, Filippatos G. Epidemiology and one‐year outcomes in patients with chronic heart failure and preserved, mid‐range and reduced ejection fraction: an analysis of the ESC Heart Failure Long‐Term Registry. Eur J Heart Fail 2017; 19: 1574–1585. [DOI] [PubMed] [Google Scholar]
- 10. Nauta JF, Hummel YM, van Melle JP, van der Meer P, Lam CSP, Ponikowski P, Voors AA. What have we learned about heart failure with mid‐range ejection fraction one year after its introduction? Eur J Heart Fail 2017; 19: 1569–1573. [DOI] [PubMed] [Google Scholar]
- 11. Altaie S, Khalife W. The prognosis of mid‐range ejection fraction heart failure: a systematic review and meta‐analysis. ESC Heart Fail 2018; 5: 1008–1016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Rastogi A, Novak E, Platts AE, Mann DL. Epidemiology, pathophysiology and clinical outcomes for heart failure patients with a mid‐range ejection fraction. Eur J Heart Fail 2017; 19: 1597–1605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Rickenbacker P, Kaufmann BA, Maeder MT, Bernheim A, Goetschalckx K, Pfister O, Pfisterer M, Brunner‐La Rocca HP, for the TIME‐CHF investigators . Heart failure with mid‐range ejection fraction: a distinct clinical entity? Insights from the Trial of Intensified versus standard Medical therapy in Elderly patients with Congestive Heart Failure (TIME‐CHF). Eur J Heart Fail 2017; 19: 1586–1596. [DOI] [PubMed] [Google Scholar]
- 14. Shah KS, Xu H, Matsouaka RA, Bhatt DL, Heidenreich PA, Hernandez AF, Devore AD, Yancy CW, Fonarow GC. Heart failure with preserved, borderline and reduced ejection fraction. 5‐year outcomes. J Am Coll Cardiol 2017; 70: 2476–2486. [DOI] [PubMed] [Google Scholar]
- 15. Koh AS, Tay WT, Teng THK, Vedin O, Benson L, Dahlstrom U, Savarese G, Lam CSP, Lund LH. A comprehensive population‐based characterization of heart failure with mid‐range ejection fraction. Eur J Heart Fail 2017; 19: 1624–1634. [DOI] [PubMed] [Google Scholar]
- 16. Ibrahim NE, Song Y, Cannon CP, Doros G, Russo P, Poniraki A, Alexanian C, Januzzi JL Jr. Heart failure with mid‐range ejection fraction: characterization of patients from the PINNACLE Registry®.ESC. Heart Fail 2019; 6: 784–792. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Anker SD, McMurray J. Time to move on from “time‐to‐first”: should all events be included in the analysis of clinical trials? Eur Heart J 2012; 33: 2764–2765. [DOI] [PubMed] [Google Scholar]
- 18. Rogers JK, Pocock SJ, McMurray JJ, Granger CB, Michelson EL, Ostergren J, Pfeffer M, Solomon SD, Swedberg K, Yusuf S. Analysing recurrent hospitalizations in heart failure: a review of statistical methodology, with application to CHARM‐preserved. Eur J Heart Fail 2014; 16: 33–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Rogers JK, Jhund PS, Perez AC, Bohm M, Cleland JG, Gullestad L, Kjekshus J, van Veldhuisen DJ, Wikstrand J, Wedel H, McMurray JJV, Pocock SJ. Effect of rosuvastatin on repeat heart failure hospitalizations: the CORONA Trial (Controlled Rosuvastatin Multinational Trial in Heart Failure). J Am Coll Cardiol HF 2014; 2: 289–297. [DOI] [PubMed] [Google Scholar]
- 20. Solomon SD, Rizkala AR, Gong J, Wang W, Anand IS, Ge J, Lam CSP, Maggioni AP, Martinez F, Packer M, Pfeffer MA, Pieske B, Redfield MM, Rouleau JL, van Valdhuisen DJ, Zannad FJ, Zile MR, Desai AS, Shi VC, Lefkowitz MP, McMurray JJV. Angiotensin receptor neprilysin inhibition in heart failure with preserved ejection fraction. Rationale and design of the PARAGON‐HF trial. J Am Coll Cardiol HF 2017; 5: 471–482. [DOI] [PubMed] [Google Scholar]
- 21. Xu X, Hardin JW. Regression models for bivariate count outcomes. Stata J 2016; 16: 301–315. [Google Scholar]
- 22. Sauerbrei W, Royston P, Binder H. Selection of important variables and determination of functional form for continuous predictors in multivariable model building. Stat Med 2007; 26: 5512–5528. [DOI] [PubMed] [Google Scholar]
- 23. Núñez E, Steyerberg EW, Núñez J. Regression modeling strategies. Rev Esp Cardiol (Engl Ed) 2011; 64: 501–507. [DOI] [PubMed] [Google Scholar]
- 24. Gómez‐Otero I, Ferrero‐Gregori A, Varela A, Seijas J, Pascual‐Figal DA, Delgado J, Álvarez‐Garcia J, Fernández‐Avilés F, Worner F, Alonso‐Pulpón L, Cinca J, González‐Juanatey JR, on behalf of Red Española de Insuficiencia Cardiaca researchers (REDINSCOR II). Mid‐range ejection fraction does not permit risk stratification among patients hospitalized for acute heart failure. Rev Esp Cardiol (Engl Ed) 2017; 70: 338–346. [DOI] [PubMed] [Google Scholar]
- 25. Lund LH, Claggett B, Liu J, Lam CSP, Jhund PS, Rosano GM, Swedberg K, Yusuf S, Granger CB, Pfeffer MA, McMurray JJV, Solomon SD. Heart failure with mid‐range fraction in CHARM: characteristics, outcomes and the effect candesartan across the entire ejection fraction spectrum. Eur J Heart Fail 2018; 20: 1230–1239. [DOI] [PubMed] [Google Scholar]
- 26. Packer M. Heart failure with a mid‐range ejection fraction. A disorder that a phychiatrist would love. JACC Heart Fail 2017; 11: 805–807. [DOI] [PubMed] [Google Scholar]
- 27. Bayés‐Genís A, Núñez J, Lupón J. Heart failure with mid‐range ejection fraction: a transition phenotype? Eur J Heart Fail 2017; 19: 1635–1637. [DOI] [PubMed] [Google Scholar]
- 28. Gulati G, Udelson JE. Heart failure with improved ejection fraction. Is it possible to escape one's past? J Am Coll Cardiol HF 2018; 9: 725–733. [DOI] [PubMed] [Google Scholar]
- 29. Lupón J, Díez‐López C, De Antonio M, Domingo M, Zamora E, Moliner P, González P, Santesmases J, Troya MI, Bayés‐Genís A. Recovered heart failure with reduced ejection fraction and outcomes: a prospective study. Eur J Heart Fail 2017; 19: 1615–1623. [DOI] [PubMed] [Google Scholar]
- 30. Lupón J, Gavidia‐Bovadilla G, Ferrer E, de Antonio M, Perera‐Lluna A, Lópe‐Ayerbe J, Domingo M, Núñez J, Zamora E, Moliner P, Santiago‐Vacas E, Santesmases J, Bayés‐Genís A. Heart failure with preserved ejection fraction infrequently evolves toward a reduced phenotype in long‐term survivors: a long‐term prospective longitudinal study. Circ Heart Fail 2019; 12: e005652. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Kaplan–Meier all‐cause mortality curves according to left ventricular ejection fraction. HFmrEF: heart failure with mid‐range ejection fraction; HFpEF: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction.