

Abstract
Coronavirus disease 2019 (COVID‐19) pandemic poses an increasing challenge for transplant community. Aggressive management measures are conductive to improve compliance and to lower the risk of intra‐hospital infection. In this Personal Viewpoint essay, we shared experiences about management strategies of transplant patients outside hospital amid the epidemic. With the aid of Cloud Clinic service and telemedicine care, transplant patients could be regularly followed up and get medical consultation online. Furthermore, personal health education and mental health assistance are enrolled in our practice.
Keywords: Cloud Clinic, COVID‐19, management, transplantation
1. INTRODUCTION
Coronavirus disease 2019 (COVID‐19) pandemic sweeps across the globe. SRAS‐CoV‐2, the causative agent of COVID‐19, is more infectious than SARS‐CoV and MERS‐CoV. 1 , 2 Hubei Province is the largest area affected by COVID‐19, and meanwhile, Hubei province is widely regarded as the cradle of transplantation in China, in which over 1550 kidney transplant and 400 liver transplant surgery are performed per year. Impairment of immunity could increase incidence of opportunistic infections. 3 , 4 Transplant patients receive regular follow‐up in outpatient clinic, in which they might have epidemiological exposure to infected patients or asymptomatic individuals in incubation period and meet intra‐hospital transmission during the outbreak. 5 In addition, transplant patients are usually accompanied with underlying diseases such as hypertension or diabetes, which are prone to critical outcome of COVID‐19. 6
In this Personal Viewpoint essay, with the aid of Cloud Clinic service and telemedicine care, we conducted aggressive management of transplant patients outside hospital amid COVID‐19 epidemic. We succeeded in improving compliance of patients and lowering the risk of nosocomial infection.
2. CLOUD CLINIC SERVICE
Online telemedicine is highly efficient in remote follow‐up of chronic diseases, cancers, and even badly great natural disaster 7 , 8 , 9 and could offer significant advantages in both price and convenience. 10 During the epidemic outbreak, lockdown and restriction policies implemented by the government of Hubei province made it difficult for outpatient visits. Meanwhile, intra‐hospital spread of COVID‐19 evolved quickly. Online telemedicine has an edge in “no touch, and no cluster.” Therefore, it is rewarding that outpatient visits move from hospital outpatient clinic to online clinic.
To this end, our center launched “Cloud Clinic” service from early February, 2020, the peak period of COVID‐19 outbreak in Hubei province. The flowchart of Cloud Clinic service was shown in Figure 1. Briefly, after registration, patients could access to Cloud Clinic service via chat or via video, then choose an in‐network doctor or an in‐network psychological expert. Covered services from Cloud Clinic include clinical counseling, medication, pharmacy express, mental health assistance, and appointment examination. The main contents of clinical counseling are suggestion on therapeutic drug monitoring (TDM), assessment of laboratory tests, and guidance on SARS‐CoV‐2 infection. For stable patients in late‐phase post‐transplant, we advised them postpone the hospital review. For patients in early‐phase post‐transplant, we sent healthcare workers to patients' home on occasion to take blood samples, and the results will be responded to associated doctors. Every patient has an independent and exclusive medical card which was established by hospital, and doctors can browse all the past test results and assess whether the patient needs to be hospitalized.
FIGURE 1.
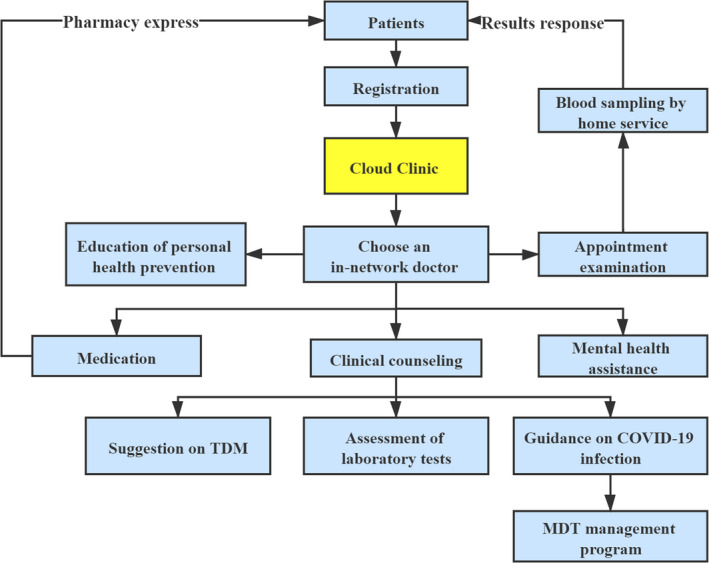
Structure of formation and execution of Cloud Clinic System. Abbreviations: MDT, multidisciplinary team consultation; TDM, therapeutic drug monitoring
In our practice, we have implemented 2460 person times of online telemedicine care for transplant patients amid the epidemic from Feb. 10, 2020 to Apr. 10, 2020. Among them, a total of 53 cases required hospitalization. The demographic characteristics and outcome of these 53 cases were shown in Table 1. Notably, 14 cases were diagnosed with SARS‐CoV‐2 infection and were admitted into the designated hospitals. Twelve were renal recipients and 2 liver recipients. These infected patients were enrolled in a multidisciplinary management program team (MDT). They were required to fill out the online observation form based on the changes in their symptoms every day so that we could monitor the dynamic changes of clinical conditions and provide further medical guidance upon immunosuppression. Rehabilitation experts developed a feasible rehabilitation plan, and psychotherapists encouraged them to have an optimistic attitude. These measures are helpful for successful recovery of most patients infected by SARS‐CoV‐2, and one patient died.
TABLE 1.
Demographic characteristics and outcome of recipients require hospitalization
| Diagnosis | Number | Outcome | |
|---|---|---|---|
| Improved | Death | ||
| Renal | |||
| Infection | 39 | 37 | 2 |
| Community‐acquired pneumonia | 2 | 2 | 0 |
| PJP | 2 | 2 | 0 |
| CMV pneumonia | 5 | 4 | 1 |
| COVID‐19 pneumonia | 12 | 11 | 1 |
| Tuberculosis | 3 | 3 | 0 |
| Urinary infection | 6 | 6 | 0 |
| Shingles | 3 | 3 | 0 |
| Sepsis | 1 | 1 | 0 |
| Gastroenteritis | 3 | 3 | 0 |
| Parvovirus B19 | 2 | 2 | 0 |
| Acute rejection | 7 | 7* | 0 |
| Renal artery stenosis | 1 | 1 | 0 |
| Cerebral infarction | 1 | 1 | 0 |
| Infection | |||
| Liver | 5 | 4 | 1 |
| Community‐acquired pneumonia | 1 | 1 | 0 |
| COVID‐19 pneumonia | 2 | 2 | 0 |
| Biliary infection | 2 | 1 | 1 |
| Total | 53 | 50 | 3 |
Abbreviations: CMV, Cytomegalovirus; COVID‐19, Coronavirus 2019; PJP, Pneumocystis Jiroveci Pneumonia.
Of these seven improved patients, one got graft dysfunction.
3. PERSONAL HEALTH EDUCATION AND MENTAL HEALTH ASSISTANCE ONLINE
The biological features and kinetic changes of SARS‐CoV‐2 are not fully recognized, and asymptomatic carriers with normal chest computed tomography (CT) findings are also infectious. 11 It was reported that of the six family members who traveled to Wuhan, five were identified as COVID‐19, 12 which showed high risk of family cluster. Hence, personal health protection should be concerned. Our Cloud Clinic released videos of public health education, in which hand hygiene and personal protection equipment had been notified as core strategies in the prevention of infection, and patients could access to them for free. We advised patients to stay at home during epidemic outbreak in order to decline the incidence of exposure. Furthermore, diary temperature monitoring, disinfection, and food nutrition are recommended.
Coronavirus disease 2019 epidemic has aroused increasing attention nationwide. Both patients and healthcare workers are amid insurmountable psychological pressure. 13 Previous studies revealed that depression increased mortality rate post‐transplant. 14 Therefore, screening and intervention on mental health problems are essential for transplant patients. We performed a cross‐sectional study to evaluate the physical and mental status of post‐transplant patients. A total of 492 recipients who resided in Wuhan attended telephonic interview during the period of epidemic outbreak. The results showed that 81.1% (n = 399) of them had varying degrees of negative emotions such as fear (69.7%), difficulty falling asleep (19.3%), and depression (11.0%). It implied that mental health crisis was ubiquitous in transplant population. They not only worried about being infected by SARS‐CoV‐2, but also worried about the side‐effects of delaying hospital visits. Unreasonable immunosuppressive therapy could increase the incidence of infection or rejection. 15 , 16 Of 399 patients who had negative emotions, 67.2% (n = 268) worried about these. In addition, 20.8% (n = 83) thought that they would be susceptible population for SARS‐CoV‐2 infection due to long‐term immunosuppression. One‐to‐one mental health crisis assistance is provided in Cloud Clinic service. Patients are encouraged to actively adjust their emotions, to present positive attitude, and to do exercise properly.
4. CONCLUSIONS
The COVID‐19 epidemic is undoubtedly a serious disaster. We launched “Cloud Clinic” service to take online telemedicine care instead of traditional outpatient visits for transplant patients. This measure could availably improve the patients’ compliance and lower the risk of intra‐hospital transmission of COVID‐19. We could remotely monitor the clinical course of COVID‐19 and make therapeutic strategies for infected patients through online MDT management program. Meanwhile, we implemented online public health education and mental health assistance for patients, which may be conductive to recovering from psychological crisis during the epidemic.
CONFLICTS OF INTEREST
The authors of this manuscript have no conflicts of interest to disclose as described.
AUTHOR CONTRIBUTIONS
Bin Liu and Dunfeng Du contributed to the study design and critical revision of the report. Yuanyuan Zhao contributed to writing of the report. Yuanyuan Zhao and Lai Wei contributed to data collection.
ACKNOWLEDGEMENT
No financial or material support to disclose.
Zhao Y, Wei L, Liu B, Du D. Management of transplant patients outside hospital during COVID-19 epidemic: A Chinese experience. Transpl Infect Dis. 2020;22:e13327. 10.1111/tid.13327
Contributor Information
Bin Liu, Email: binliu@tjh.tjmu.edu.cn.
Dunfeng Du, Email: dfdu@tjh.tjmu.edu.cn.
REFERENCES
- 1. Drosten C, Günther S, Preiser W, et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348(20):1967‐1976. [DOI] [PubMed] [Google Scholar]
- 2. Bermingham A, Chand MA, Brown CS, et al. Severe respiratory illness caused by a novel coronavirus, in a patient transferred to the United Kingdom from the Middle East, September 2012. Euro Surveill. 2012;17(40):20290. [PubMed] [Google Scholar]
- 3. Zhu L, Xu X, Ma K, et al. Successful recovery of COVID‐19 pneumonia in a renal transplant recipient with long‐term immunosuppression. Am J Transplant. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Attias P, Melica G, Boutboul D, et al. Epidemiology, risk factors and outcomes of opportunistic infections after kidney allograft transplantation in the era of modern immunosuppression: a monocentric cohort study. J Clin Med. 2019;8(5):594. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Day M. Covid‐19: identifying and isolating asymptomatic people helped eliminate virus in Italian village. BMJ. 2020;368:m1165. [DOI] [PubMed] [Google Scholar]
- 6. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708‐1720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Qaderi SM, Vromen H, Dekker HM, Stommel M, Bremers A, de Wilt J. Development and implementation of a remote follow‐up plan for colorectal cancer patients. Eur J Surg Oncol. 2020;46(3):429‐432. [DOI] [PubMed] [Google Scholar]
- 8. Grove BE, Oho AUID, Ivarsen P, et al. Remote follow‐up using patient‐reported outcome measures in patients with chronic kidney disease: the PROKID study ‐ study protocol for a non‐inferiority pragmatic randomised controlled trial. BMC Health Serv Res. 2019;19(1):631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Aiken A, Digol I, Trussell J, Gomperts R. Self reported outcomes and adverse events after medical abortion through online telemedicine: population based study in the Republic of Ireland and Northern Ireland. BMJ. 2017;357:j2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Vo AH, Brooks GB, Bourdeau M, Farr R, Raimer BG. University of Texas Medical Branch telemedicine disaster response and recovery: lessons learned from hurricane Ike. Telemed J E Health. 2010;16(5):627‐633. [DOI] [PubMed] [Google Scholar]
- 11. Bai Y, Yao L, Wei T, et al. Presumed asymptomatic carrier transmission of COVID‐19. JAMA. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person‐to‐person transmission: a study of a family cluster. Lancet. 2020;395(10223):514‐523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Li W, Yang Y, Liu ZH, et al. Progression of mental health services during the COVID‐19 Outbreak in China. Int J Biol Sci. 2020;16(10):1732‐1738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Dew MA, Rosenberger EM, Myaskovsky L, et al. Depression and anxiety as risk factors for morbidity and mortality after organ transplantation: a systematic review and meta‐analysis. Transplantation. 2015;100(5):988‐1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Kumar D, Michaels MG, Morris MI, et al. Outcomes from pandemic influenza A H1N1 infection in recipients of solid‐organ transplants: a multicentre cohort study. Lancet Infect Dis. 2010;10(8):521‐526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Huang G, Zhang L, Liang X, et al. Risk factors for BK virus infection and BK virus‐associated nephropathy under the impact of intensive monitoring and pre‐emptive immunosuppression reduction. Transplant Proc. 2014;46(10):3448‐3454. [DOI] [PubMed] [Google Scholar]