

The 2019 novel coronavirus (initially termed as 2019‐nCoV, and thereafter formally renamed as severe acute respiratory syndrome‐coronavirus 2 [SARS‐CoV‐2]) originating from Wuhan City, China, is an etiological agent of ongoing outbreaks of coronavirus disease (COVID‐19). 1 , 2 , 3 Phylogenetic analysis suggested that SARS‐CoV‐2 is possible progenitor of SARS‐CoV with bat origin. 4 , 5 As of 8 April 2020, the pandemic of COVID‐19 has swept almost 184 countries (and/or regions), comprising 1 485 981 cases of confirmed SARS‐CoV‐2 infection (https://www.gisaid.org/epiflu-applications/global-cases-covid-19). Not surprisingly, China has become one of severely affected epidemic area of COVID‐19, which is fulfilled with 82 870 infection cases (3339 deaths). Of note, Zhejiang province is one of best controlled place within China, in that only one death of 1267 confirmed COVID‐19 cases is recorded. Italy is a seriously affected country outside China, whose number of confirmed patients (139 442 cases) is next to those of Spain (148 220 cases) and United States (432 438 cases). As for those individuals traveling between Zhejiang Province and Italy, the potential carriers of COVID‐19 are not clinically addressed. Here, we close the missing gap on this issue. We are the first to report a cluster of imported COVID‐19 cases from Italy.
In total, we have observed eight confirmed SARS‐CoV‐2 cases. Except that the patient 8 give no syndrome, all the other seven individuals display the mild symptom of an influenza‐like illness (ILI), like cough (Figure 1). More importantly, they are featuring with person‐to‐person transmission of COVID‐19, in that they are occupied in the same restaurant of Bergamo City, Italy. The eight Chinese citizens are natives of Qingtian County of Lishui City, in Zhejiang Province of China and worked for many years in a restaurant of Bergamo City, Italy. Because of the rapid increase of confirmed SARS‐CoV‐2 cases, they returned from Milan Malpensa Airport, Italy, to Shanghai Pudong International Airport, China, on 27 February 2020. In addition to the international flight between Italy and China, it also included two distinct domestic transportation, namely (a) a shuttle service from their living place, Bergamo City to the departure Milan Malpensa Airport, Italy; and (b) a booked shuttle service from Shanghai to Qingtian County, Zhejiang Province. During these journeys, they did not wear masks. The patient 5 (P5: male, 32‐year‐old), and his wife (P6: female, 31‐year‐old) stayed at home for the isolation, and all the other individuals were subjected to the designated local isolation.
Figure 1.
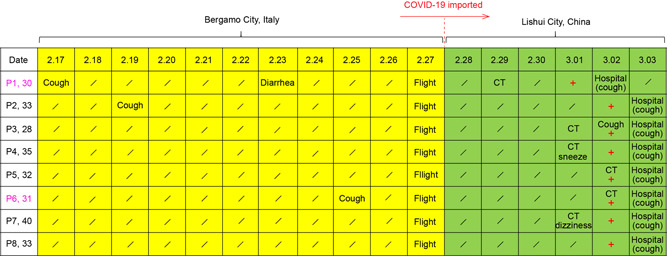
Epidemiological history of this cluster of imported patients with COVID‐19. Of note, all the eight patients (P1 to P8), whose hometowns refer to Qingtian County, worked in the same restaurant in Bergamo City, Italy. P2 is the husband of P1, and P3 was the younger brother of P1. P6 was the wife of P5. On 27 February, all the patients purchased charter service from Bergamo City, to Milan Malpensa Airport, Italy, and then boarded on an international flight to Shanghai Pudong International Airport. Among the eight patients (P1 to P8), two females are colored pink. P1 was a first confirmed SARS‐CoV‐2 case, who was admitted to the designated hospital in Lishui City, on 2 March, 2020. One day later, all the remaining seven individuals with close contact with Patient 1 in Italy, the epidemic area of COVID‐19, was recognized as positive for SARS‐CoV‐2, and admitted to the same hospital. Slight cough (but not fever), a symptom of influenza‐like illness (ILI), is the representative characteristics of this cluster of imported cases with COVID‐19. Designations: the plus “+,” positive for COVID‐19; “/”, “not applied.” COVID‐19, coronavirus disease; CT, computed tomography; SARS‐CoV2, severe acute respiratory syndrome‐coronavirus 2
Retrospectively, the patient 1 (P1: female, 30‐year‐old) reported her clinical onset of cough (and little bit headache) 2 weeks ago before returning from Italy and diarrhea on 23 Febuary 2020 (Figure 1). Thus, she was immediately transferred by ambulance and admitted to the fever clinics of Qingtian County People's Hospital on 29 February 2020. Meanwhile, computed tomography (CT) imaging of P1 showed multiple‐patchy ground‐glass opacities in left lung (from middle lobe to bottom lobe, Figure S1A), implying the possibility of viral pneumonia. During the local hospitalization, she received the routine antiviral treatment with Arbidol tablets. As expected, the throat swabs from patient 1 tested positive for COVID‐19 with the detection of real‐time quantitative polymerase chain reaction. Therefore, patient 1 was immediately transferred to Lishui City's centralized isolation site for further supportive therapy. The husband of patient 1 (P2: male, 33‐year‐old) began to have dry cough with less yellowish sputum on 19 February, and it lasted for 2 weeks (Figure 1). Along with the presence of a single ground‐glass opacity in the right bottom lobe (Figure S1B), the positive diagnosis of P2 for SARS‐CoV‐2 by Qingtian County Center for Disease Control and Prevention on 2 March 2020, prompted the arrival of being transferred to the hospital of centralized isolation in Lishui City, on 3 March (Figure 1). Not surprisingly, her younger brother of P1 (P3: male, 28‐year‐old) presented the clinical onset of cough, and slight inflammation of left lung (Figure S1C), which is fully consistent with the detection of SARS‐CoV‐2 in his oropharyngeal swabs (Figure 1). Unlike her husband (P5: male, 32‐year‐old), the patient 6 (P6: female, 31‐year‐old) displayed the onset of cough 1 week earlier (Figure 1). Both them were verified by CT and nucleic acid detection to be positive for COVID‐19 (Figures 1 and S1E,F). Evidently, the above five cases defined two familial clusters of person‐to‐person transmission of COVID‐19. Different from that the confirmed SARS‐CoV‐2 case of P4 (male, 35‐year‐old) is clinically characterized with sneezing (Figure S1D), P7 (male, 40‐year‐old) displayed dizziness on his clinical onset (Figure S1G). It was unusual for patient 8 (P8: male, 33‐year‐old) that he had no detective onset (Figure S1H), despite the positive recognition of SARS‐CoV‐2. This might hint the cryptic and/or earlier stage of COVID‐19 development. In contrast, all the other seven cases of COVID‐19 consistently produced symptoms of ILI. It is unusual, but not without any precedent. Though that they are far different from those of heavy patients with COVID‐19 reported by other research groups, 6 , 7 a similar scenario was also recorded in a local case admitted to Lishui People's Hospital. 8
To the best of our knowledge, it represents a first description of clustered imported cases of Italian COVID‐19. Unlike severe pneumonia, most of them (7 out of 8) exhibited mild flu‐like symptoms. Presumably, this was due to the human‐to‐human transmission of COVID‐19 within an Italian restaurant. Taken together, this constituted an additional input into a full spectrum of viral diseases of SARS‐CoV‐2 infection in China and beyond.
CONFLICT OF INTERESTS
The authors declare that there are no conflict of interests.
AUTHOR CONTRIBUTIONS
YF and WW designed and supervised this project. WW and DZ collected the clinical and epidemiological data. YF, WW, DZ, and XJ analyzed the data and prepared the tables and figures. YF drafted this manuscript.
ETHICS STATEMENT
This was a retrospective study of COVID‐19 conducted in Lishui People's Hospital, Zhejiang Province of China. According to the guideline of the National Health Commission, China, all the confirmed COVID‐19 cases received the isolation and supportive therapy in the designated provisional hospital. All the clinical data collection (esp. chest computed tomography) and epidemiological surveys were conducted under the approval by Ethics Committee of Lishui People's Hospital (LLW‐FO‐401). Given the importance of clinical data sharing in public and academic societies, the routine written informed consent of patients was waived during this special period of ongoing COVID‐19 epidemic in China and beyond.
Supporting information
Supporting information
Supporting information
Funding Information National Natural Science Foundation of China, Grant/Award Number: 31830001
REFERENCES
- 1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382:727‐733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Guan W, Ni Z, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708–1720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID‐19) outbreak in China: summary of a report of 72 314 cases from the Chinese center for disease control and prevention. JAMA. 2020;323:1239. [DOI] [PubMed] [Google Scholar]
- 4. Xu Y, Wang L, Jia X, Feng Y. 2019‐nCoV: a possible progenitor for SARS‐CoV with bat origin? PrePrint. 2020. 10.20944/preprints202003.0159.v1 [DOI] [Google Scholar]
- 5. Hu D, Zhu C, Ai L, et al. Genomic characterization and infectivity of a novel SARS‐like coronavirus in Chinese bats. Emerg Microbes Infect. 2018;7(1):154‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507‐513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Shi H, Han X, Jiang N, et al. Radiological findings from 81 patients with COVID‐19 pneumonia in Wuhan, China: a descriptive study. Lancet Infect Dis. 2020;20:425‐434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Zhang H, Wang W, Wu N, et al. Influenza‐like illness caused by the 2019 novel coronavirus (2019‐nCoV) via the person‐to‐person transmission. PrePrint. 2020. 10.20944/preprints202003.200160.v202001 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting information
Supporting information