

Abstract
With the COVID-19 pandemic progressing, guidance on strategies to mitigate its devastating effects in nursing facilities (NFs) is critical to preventing additional tragic outcomes. Asymptomatic spread of COVID-19 from nursing facility staff and residents is a major accelerator of infection. Facility-wide point-prevalence testing is an emerging strategy in disease mitigation. Because time is not available to await the results of randomized controlled trials before implementing strategies in this high-risk setting, an expert Delphi panel composed of experienced long-term care medicine professionals has now met to provide testing guidance for SARS-Coronavirus-2 to NFs. After many email and telephone discussions, the panel responded to a questionnaire that included six different scenarios, based on varying availability of Polymerase Chain Reaction (RT-PCR) testing and personal protective equipment (PPE). The panel endorsed facility-wide testing of staff and residents without dissent when diagnostic RT-PCR was available. While the panel recognized the limitations of RT-PCR testing, it strongly recommended this testing for both staff and residents in NFs that were either COVID-19 naive or had limited outbreaks. There was also consensus on testing residents with atypical symptoms in a scenario of limited testing capability. The panel favored testing every 1 to 2 weeks if testing was readily available, reducing the frequency to every month as community prevalence declined or as the collection of additional data further informed clinical critical thinking and decision-making. The panel recognized that frequent testing would have consequences in terms of potential staff shortages due to quarantine after positive tests and increased PPE use. However, the panel felt that not testing would allow new clusters of infection to form. The resulting high mortality rate would outweigh the potential negative consequences of testing. The panel also recognized the pandemic as a rapidly evolving crisis, and that new science and increasing experience might require an updating of its recommendations. The panel hopes that its recommendations will be of value to the long-term care industry and to policy makers as we work together to manage through this challenging and stressful time.
Key words: Coronavirus, COVID-19, testing, nursing facilities
The Impact of the COVID-19 Pandemic on Nursing Facilities
The article “Nursing Homes are Ground Zero for COVID-19 Pandemic” is the first to describe a major outbreak of SARS-CoV-2 infection in a U.S. nursing facility (NF) in Kirkland, Washington (1). Almost simultaneously, the world began learning about the large number of deaths in NFs throughout Italy and Spain (2). Close living quarters, the high incidence of cognitive impairment, the need for frequent daily caregiver interactions, and the advanced age and high comorbidity burden of NF residents, are some of the factors that have led to unmitigated disease spread. The high risk of this infection in older adults, especially those in congregate living settings, is well recognized (3, 4). Although reporting of COVID-19 positive rates is now required in U.S. NFs, testing and reporting of positive rates has thus far been sporadic. Some reports now suggest that deaths of NF residents and workers may account for 35% or more of all COVID-19 deaths in the U.S. (5). New clusters of infection among NF residents could contribute to further spread outside the facility by staff, as well as potentially by visitors if visitor restrictions are relaxed.
Evidence for Testing in Nursing Facilities
Aggressive testing has been a hallmark and best practice for countries to “flatten the curve” of this pandemic (6). Taking the same approach in NFs, as well as in other congregate settings such as assisted living facilities, seems essential because of the susceptibility of the population. A number of reports document the prevalence of NF outbreaks (7). Examining the characteristics of these outbreaks may provide approaches to containment and mitigation of this epidemic (8). “Unrecognized asymptomatic and pre-symptomatic infections might contribute to transmission in these settings,” concluded an MMWR published on March 27 2020 (9). The article went on to state that “as testing availability improves, consideration might be given to test-based strategies for identifying (nursing facility) residents with SARS-CoV-2 infection…” (9). Recommendations have also recognized the “importance of proactive steps to identify and exclude potentially infected staff and visitors, early recognition of potentially infected patients, and implementation of appropriate infection prevention and control measures” (10).
Polymerase Chain Reaction (RT-PCR) testing for the presence of the virus is an important tactic in containing and mitigating the impact of COVID-19 (11). Early studies demonstrate that testing often uncovers asymptomatic infection (12). There have also been concerns regarding the relatively high percentage of false negatives, noted to be as high as 30% (13, 14). As of February 27, 2020, testing was not readily available in the U.S. (15). As testing became more readily available, NFs and assisted living facilities were not identified as priority locations for testing. Serologic testing for antibodies to the virus may be helpful in identifying individuals who have been infected, and could help with population statistics, determining who might have immunity, and developing a pool of potential donors of convalescent serum (16). However, NF residents may not have a robust antibody response, as is the case for other viral infections. Among staff, the presence of antibodies occurs after a significant interval and is not useful in identifying staff members who may be infectious. Even among staff who have antibodies, whether they are immune, and the duration of such immunity, is not known (16). Thus using serologic testing to assist with staffing decisions is fraught with challenges.
On April 24, 2020, a New England Journal of Medicine editorial, based on another study, stated, “A new approach that expands Covid-19 testing to include asymptomatic persons residing or working in skilled nursing facilities needs to be implemented now” (17, 18). Viral load may also have an impact on the outcomes of COVID-19 infection (19). However, severity of illness might only correlate with viral load at the time that severity is measured. Nevertheless, robust testing for the virus among NF staff and residents could influence a facility to respond quickly with isolation and full use of PPE. Rapid implementation of these measures before a full symptomatic outbreak could potentially reduce the viral load during a facility outbreak.
Even before publication of this editorial, the California Association of Long Term Care Medicine, which has been working on an approach to COVID-19 proactively since early March, posted its “Long Term Care Quadruple Aim for COVID-19 Response” on April 17, 2020 (20). The four pillars of this quadruple aim include: (1) stellar infection prevention interventions; (2) abundant personal protective equipment (PPE); (3) readily available testing; and (4) operating in emergency preparedness mode.
Reported Challenges to Widespread Testing in Nursing Facilities
Despite evidence supporting the value of testing, there have been barriers to universal testing in NFs and assisted living facilities. On April 22, 2020, the Director of the Los Angeles County Department of Public Health acknowledged this issue, stating that not testing all staff and residents had been “wrong” (21). Even the Centers for Disease Control and Prevention (CDC) testing guidelines have not explicitly recommended widespread testing of residents and staff regardless of symptoms. Guidance from April 30, 2020 stated: “if testing capacity is not sufficient for unit-wide Point Prevalence Survey (PPS), testing should be prioritized for symptomatic residents and other high-risk residents” (22). Moreover, in regard to NF staff, the guidance was: “If testing capacity allows, Point Prevalence Survey (PPS) of all HCP (Health Care Providers) should be considered in facilities with suspected or confirmed cases of COVID-19” (22). Neither of these scenarios took into account asymptomatic and pre-symptomatic cases of COVID-19 in both staff and residents. The concept of point prevalence surveys has not clearly delineated the extent to which testing should take place. An example of widespread testing of residents and staff of one facility in Los Angeles found 90% of staff and 75% of residents to be positive, and nearly all staff and most residents were asymptomatic (23).
Despite these findings, some NFs, as well as assisted living facilities, have resisted testing. While the CDC guidelines attempted to recognize the lack of readily available testing, they did not address other factors that have led to resistance to or avoidance of testing both staff and residents. Some NFs believe that identifying positive cases of COVID-19 can lead to negative press (24, 25). Some are also concerned that they might have to send positive staff home, exacerbating existing staffing shortages (26). Staff may refuse to come to work, leading to further staffing shortages (27). AMDA (The Society For Post Acute And Long Term Care Medicine) has published a policy statement regarding testing strategies that further delineates many of these challenges (28). While these concerns have a factual basis, the clinical reality of the devastating impact of COVID-19 infections when allowed to spread unfettered in NFs should outweigh these concerns.
The need for preventive and mitigation strategies is urgent, and the fact that these conflicting factors continue to distract policy makers from recommending widespread testing in the NF setting led us to convene a panel of long-term care medicine professionals to make recommendations on testing given the varying scenarios that currently exist in U.S. NFs.
Modified Delphi Process
With the COVID-19 pandemic progressing, guidance on strategies to mitigate its devastating effects in NFs is critical to prevent additional tragic outcomes. The existing literature, policies evolving or being implemented in some NF chains, and feedback from experts appear to have a consistent message, but guidance and actions regarding testing in NFs have been inconsistent. The field of Geriatric Medicine has historically used a modified Delphi process in order to develop approaches to care (29, 30). The rapidly evolving nature of this pandemic necessitated that this modified Delphi process occur over a relatively short period of time. On April 19, 2020, an email thread was initiated by the first author that posed the following question: “Asymptomatic staff can be contagious. Why wouldn’t we want to identify staff who will become the vector for transmission? What is the downside to widespread testing of staff in nursing homes?” Over the course of two weeks, many clinicians and experts in long-term care medicine who were actively dealing with COVID-19 in NFs around the country weighed in via email and phone calls. These communications began the first stage of the modified Delphi process. A panel composed of 16 experienced long-term care professionals was formed, including 14 physicians, one infection preventionist and a geriatric pharmacist. The entire panel is recognized either as authors or acknowledged for their participation in the Delphi process. An anonymous survey was conducted, with questions on COVID-19 testing in six different NF scenarios, based on the preceding discussions (see Table 1).
Table 1.
Scenarios for Testing Created for the Delphi Panel Survey
| 1. No PPE, Readily Available Testing (A NF that is truly lacking in PPE, but is capable of testing all staff and residents regularly. This should be uncommon, but possible. Represents an interesting theoretical situation). |
| 2. Abundant PPE, No Available Testing (A NF that has abundant PPE, but is completely lacking in the ability to test all staff and residents regularly. This should also be uncommon, but possible. Represents an interesting theoretical situation). |
| 3. Abundant PPE, Readily Available Testing (A NF that has abundant PPE, but is capable of testing all staff and residents regularly. This should be the gold standard, and is starting to occur in many communities). |
| 4. Abundant PPE, Limited Testing Available (A NF that has abundant PPE, is not capable of testing all staff and residents regularly, but has enough testing to test a modicum of staff and residents. This may be common in many communities at this time). |
| 5. Limited PPE, Limited Testing Available (A NF that has limited PPE, due to supply chain issues, and is not capable of testing all staff and residents regularly, but has enough testing to test a modicum of staff and residents. This may be somewhat common in many communities at this time) |
| 6. Limited PPE, Readily Available Testing (A NF that has limited PPE, due to supply chain issues, but is capable of testing all staff and residents regularly. This would be a rare situation in most communities. Represents an interesting theoretical situation). |
The panelists were given the following preface to the survey: “The six scenarios assume a community where COVID-19 infections are already occurring (no specific point prevalence, but the infection is known to be in the community). The starting point for considering the following scenarios is that the nursing facility is COVID-19 naive. However, any of these scenarios could also occur in a NF where there could have been some known cases of COVID-19 infection in either staff or residents, but have already been managed, i.e., staff sent home, residents discharged to hospital or isolated when that option is available. It also assumes that finding replacement staff is a viable option.” Table 2 and Figures 1–3 illustrate the results of this survey.
Figure 2.
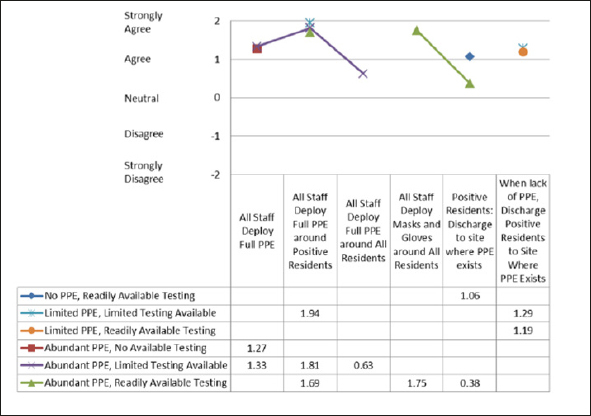
Scenario Responses: PPE
Table 2.
Scenarios for Testing Created for the Delphi Panel Survey
| Scenario | Strongly Agree | Agree | Neutral | Disagree | Strongly Disagree | |
|---|---|---|---|---|---|---|
| 1. | No PPE, Readily Available Testing | Test All Staff | 14 | 1 | 1 | |
| Test All Residents | 12 | 3 | 1 | |||
| Positive Staff: Send home, initiate contact tracing | 12 | 1 | 2 | 1 | ||
| Positive Residents: Discharge to site where PPE exists | 8 | 3 | 3 | 2 | ||
| 2. | Abundant PPE, No Available Testing | All Staff Deploy Full PPE | 9 | 3 | 1 | 2 |
| Isolate Residents with Atypical Symptoms | 11 | 3 | 1 | |||
| Isolate Residents with Typical Symptoms | 13 | 1 | 1 | |||
| Isolate Asymptomatic Residents | 5 | 3 | 2 | 4 | 1 | |
| 3. | Abundant PPE, Readily Available Testing | Test All Staff | 13 | 3 | ||
| Test All Residents | 11 | 4 | 1 | |||
| Positive Staff: Send home, initiate contact tracing | 10 | 5 | 1 | |||
| Positive Residents: Discharge to site where PPE exists | 4 | 5 | 3 | 1 | 3 | |
| Isolate and Test Residents with Atypical Symptoms | 11 | 5 | ||||
| Isolate and Test Residents with Typical Symptoms | 13 | 3 | ||||
| Positive Residents: Isolate w/ Droplet Precautions | 13 | 3 | ||||
| All Staff Deploy Full PPE around Positive Residents | 13 | 2 | 1 | |||
| All Staff Deploy Masks and Gloves around All Residents | 12 | 4 | ||||
| 4. | Abundant PPE, Limited Testing Available | All Staff Deploy Full PPE | 10 | 2 | 1 | 2 |
| Test Symptomatic Staff | 11 | 3 | 1 | 1 | ||
| Test Residents with Atypical Symptoms | 10 | 6 | ||||
| Test Residents with Typical Symptoms | 11 | 4 | 1 | |||
| Positive Staff: If Symptomatic, Send home, initiate contact tracing | 12 | 2 | 2 | |||
| Isolate Residents with Atypical Symptoms | 13 | 2 | 1 | |||
| Isolate Residents with Typical Symptoms | 14 | 2 | ||||
| Positive Residents: Isolate w/ Droplet Precautions | 14 | 2 | ||||
| All Residents: Isolate w/ Droplet Precautions | 4 | 1 | 6 | 4 | 1 | |
| All Staff Deploy Full PPE around Positive Residents | 14 | 1 | 1 | |||
| All Staff Deploy Full PPE around All Residents | 5 | 5 | 3 | 1 | 2 | |
| 5. | Limited PPE, Limited Testing Available | Send Symptomatic Staff Home, Initiate Contact Tracing | 13 | 2 | 1 | |
| Test Symptomatic Staff | 11 | 2 | 2 | 1 | ||
| Isolate Residents with Atypical Symptoms | 14 | 1 | 1 | |||
| Isolate Residents with Typical Symptoms | 14 | 1 | 1 | |||
| Test Residents with Atypical Symptoms | 8 | 6 | 2 | |||
| Test Residents with Typical Symptoms | 10 | 4 | 2 | |||
| Positive Residents: Isolate w/ Droplet Precautions | 13 | 3 | ||||
| All Staff Deploy Full PPE around Positive Residents | 15 | 1 | ||||
| When lack of PPE, Discharge Positive Residents to Site Where PPE Exists | 5 | 8 | 1 | |||
| 6. | Limited PPE, Readily Available Testing | Test All Staff | 13 | 3 | ||
| Test All Residents | 12 | 3 | 1 | |||
| Positive Staff: Send home, initiate contact tracing | 14 | 2 | ||||
| Positive Residents: Isolate w/ Droplet Precautions | 13 | 3 | ||||
| When lack of PPE, Discharge Positive Residents to Site Where PPE Exists | 8 | 5 | 1 | 2 | ||
Figure 1.
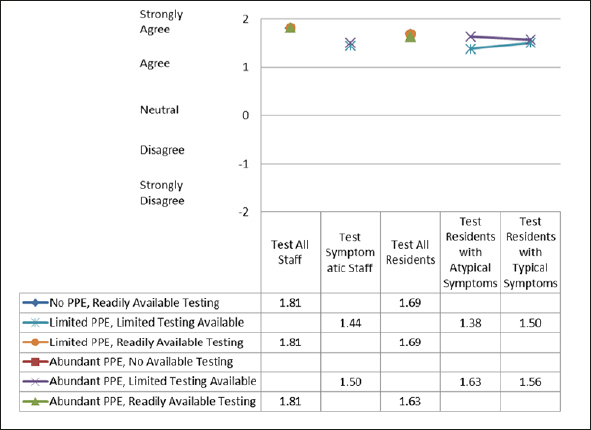
Scenario Responses: Testing
Figure 3.
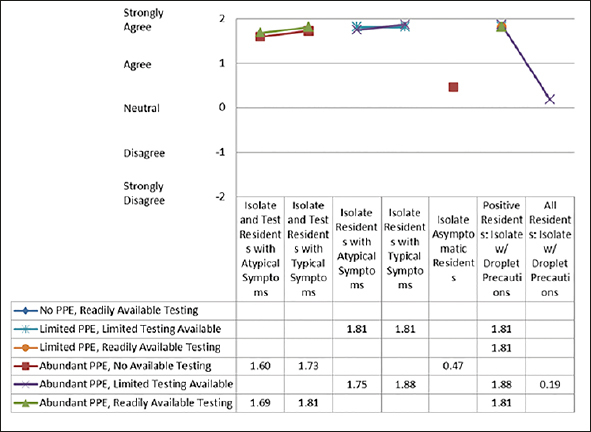
Scenario Responses: Residents
After completing the survey, the results were collated and disseminated to the members of the Delphi panel. A first draft of this paper was crafted, and the members of the panel participated in two subsequent phone calls whereupon the consensus statements laid out in this paper were discussed and reviewed. Ten members of the panel chose to actively participate as authors and the remainder chose to be acknowledged for their efforts as participants.
Conclusions and Implications
The single most important finding from this Delphi panel is that its members consistently support point prevalence facility-wide testing, with no dissent, of all staff and residents when testing is readily available. The panel feels strongly that long-term care providers, as well as federal, state, and local officials should listen to experienced health professionals on the front lines, fighting this pandemic, when making policy decisions.
Recognizing that there are limitations inherent to RT-PCR testing, there is full agreement in the value of testing both staff and residents in NFs that are either COVID-19 naive or have had limited outbreaks. The testing of all staff provides the opportunity for NFs to respond to outbreaks before staff and residents become symptomatic. While assisted living facilities were not included in the given scenarios, the panel feels that similar conclusions would be appropriate in these high-risk settings. In the scenario of limited testing capability, the panel also recommends testing of residents with atypical symptoms, because such symptoms are common in NF residents and could represent the early manifestations of COVID-19. The panel favors testing every 1 to 2 weeks, if testing is readily available, based on the fact that the incubation period for developing symptoms varies from 3–5 days up to 2 weeks. Ultimately, the frequency can be reduced to every month as community prevalence declines. The panel also acknowledges that the results from testing will further inform clinical critical thinking and decision-making with regards to the frequency of ongoing testing.
The other important conclusion from the panel relates to the availability of PPE. The ideal situation for protecting both residents and staff is aggressive use of testing, intensive infection control procedures, and PPE. There is unanimous agreement that residents who test positive and/or have both typical and atypical symptoms should be isolated. Staff in these circumstances should fully take advantage of PPE and be trained in its proper use.
There are differing opinions in the scenario with limited PPE and/or limited testing. There is still a very strong consensus around isolating residents with typical or atypical symptoms. The only scenario without a clear consensus is the option of isolating all residents when there is abundant PPE and limited testing available. Even in the setting of limited testing, the panel agrees with testing residents with both typical and atypical symptoms.
The panel recognizes that frequent testing will have consequences in terms of potential staff shortages due to quarantine after positive tests, as well as the potential to further increase the need for and burn rate of PPE. However, the panel feels that the risks of not testing, resulting in new clusters of infection that could have high mortality rates, outweigh the risks of these potential consequences. While the panel did not specifically address testing visitors or vendors, it goes without saying that anyone entering a facility should adhere to the same testing criteria as facility staff.
The panel also recognizes that the pandemic is a rapidly evolving crisis, and that new science and increasing experience may require an updating of its recommendations. In the meantime, we hope that our deliberations and recommendations will be of value to the long-term care industry and to policy makers as we work together to manage through this challenging and stressful time.
Acknowledgements
A panel of experienced long-term care clinicians who volunteered their time to participate in the Delphi process developed the recommendations included in this document. The work was unfunded, and the recommendations represent the opinions of the panel members, and not the organizations they work in.
Conflicts of Interest: The authors have no conflicts of interest. This research did not receive any funding from agencies in the public, commercial, or not-for-profit sectors.
Footnotes
In addition to the authors, the panel included: Jesse Cohen, MD — Newton Rehabilitation and Health Care Center; Dolly Greene, RN, BSN, CIC — Infection Prevention & Control Resources; James McKinnell, MD — Los Angeles Biomedical Research Institute; Swati Gaur, MD, MBA, CMD — New Horizons Long Term Care Facilities; Joshua Uy, MD — Penn Medicine; Thomas Yoshikawa, MD — Department of Veterans Affairs (VA) Greater Los Angeles Healthcare System
References
- 1.Barnett ML, Grabowski DC. Nursing Facilities Are Ground Zero for COVID-19 Pandemic. JAMA Health Forum. Published March 24, 2020. Accessed May 14, 2020. https://jamanetwork.com/channels/health-forum/fullarticle/2763478 [DOI] [PubMed]
- 2.Many covid deaths in care facilities are unrecorded. The Economist, May 9, 2020.
- 3.Wang L, He W, Yu X, et al. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J Infect. 2020;S0163-4453(20):30146–8. doi: 10.1016/j.jinf.2020.03.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gardner W, States D, Bagley N. The Coronavirus and the Risks to the Elderly in Long-Term Care. Journal of Aging & Social Policy. Published April 3, 2020. Accessed May 14, 2020. DOI: 10.1080/08959420.2020.1750543 [DOI] [PubMed]
- 5.Yourish K, et al. One-Third of All U.S. Coronavirus Deaths Are Nursing Home Residents or Workers. May 11, 2020. https://www.nytimes.com/interactive/2020/05/09/us/coronavirus-cases-nursing-homes-us.html
- 6.Lorenzoni, G, Lanera C, Azzolina D. et al. Is a more aggressive COVID-19 case detection approach mitigating the burden on ICUs? Some reflections from Italy. Crit Care. 2000. 24, 175. 10.1186/s13054-020-02881-y [DOI] [PMC free article] [PubMed]
- 7.Comas-Herrera A, Zalakain J. Mortality associated with COVID-19 outbreaks in care facilities: early international evidence. International Long Term Care Policy Network. April 12, 2020. Accessed May 14, 2020.
- 8.McMichael TM, Clark S, Pogosjans S, et al. COVID-19 in a Long-Term Care Facility — King County, Washington, February 27–March 9, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:339–342. doi: 10.15585/mmwr.mm6912e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kimball A, Hatfield KM, Arons M, et al. Asymptomatic and Presymptomatic SARS-CoV-2 Infections in Residents of a Long-Term Care Skilled Nursing Facility — King County, Washington, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69:377–381. doi: 10.15585/mmwr.mm6913e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.McMichael Temet M., Currie Dustin W., Clark Shauna, Pogosjans Sargis, Kay Meagan, Schwartz Noah G., Lewis James, Baer Atar, Kawakami Vance, Lukoff Margaret D., Ferro Jessica, Brostrom-Smith Claire, Rea Thomas D., Sayre Michael R., Riedo Francis X., Russell Denny, Hiatt Brian, Montgomery Patricia, Rao Agam K., Chow Eric J., Tobolowsky Farrell, Hughes Michael J., Bardossy Ana C., Oakley Lisa P., Jacobs Jesica R., Stone Nimalie D., Reddy Sujan C., Jernigan John A., Honein Margaret A., Clark Thomas A., Duchin Jeffrey S. Epidemiology of Covid-19 in a Long-Term Care Facility in King County, Washington. New England Journal of Medicine. 2020;382(21):2005–2011. doi: 10.1056/NEJMoa2005412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.To KK, Tsang OT, Chik-Yan Yip C, Chan KH, Wu TC, Chan JMC, et al. Consistent detection of 2019 novel coronavirus in saliva. Clin Infect Dis 2020;ciaa149. doi: 10.1093/cid/ciaa149 [DOI] [PMC free article] [PubMed]
- 12.Nishiura H, Kobayashi T, Suzuki A, et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19) International Journal of Infectious Diseases. 2020;94:154–55. doi: 10.1016/j.ijid.2020.03.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Long C, Xu H, Shen Q, et al. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur J Radiol. 2020;126:108961. doi: 10.1016/j.ejrad.2020.108961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.West CP, Montori VM, Sampathkumar P. COVID-19 Testing: The Threat of False-Negative Results. Mayo Clin Proc. 2020;S0025-6196(20):30365–7. doi: 10.1016/j.mayocp.2020.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.del Rio C, Malani PN. COVID-19—New Insights on a Rapidly Changing Epidemic. JAMA. 2020;323(14):1339–1340. doi: 10.1001/jama.2020.3072. [DOI] [PubMed] [Google Scholar]
- 16.Sethuraman N, Jeremiah SS, Ryo A. Interpreting Diagnostic Tests for SARS-CoV-2 [published online ahead of print, 2020 May 6]. JAMA. 2020;10.1001/jama.2020.8259. doi: 10.1001/jama.2020.8259 [DOI] [PubMed]
- 17.Gandhi Monica, Yokoe Deborah S., Havlir Diane V. Asymptomatic Transmission, the Achilles’ Heel of Current Strategies to Control Covid-19. New England Journal of Medicine. 2020;382(22):2158–2160. doi: 10.1056/NEJMe2009758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Arons Melissa M., Hatfield Kelly M., Reddy Sujan C., Kimball Anne, James Allison, Jacobs Jesica R., Taylor Joanne, Spicer Kevin, Bardossy Ana C., Oakley Lisa P., Tanwar Sukarma, Dyal Jonathan W., Harney Josh, Chisty Zeshan, Bell Jeneita M., Methner Mark, Paul Prabasaj, Carlson Christina M., McLaughlin Heather P., Thornburg Natalie, Tong Suxiang, Tamin Azaibi, Tao Ying, Uehara Anna, Harcourt Jennifer, Clark Shauna, Brostrom-Smith Claire, Page Libby C., Kay Meagan, Lewis James, Montgomery Patty, Stone Nimalie D., Clark Thomas A., Honein Margaret A., Duchin Jeffrey S., Jernigan John A. Presymptomatic SARS-CoV-2 Infections and Transmission in a Skilled Nursing Facility. New England Journal of Medicine. 2020;382(22):2081–2090. doi: 10.1056/NEJMoa2008457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Liu Y, Yan L, Wan L. Viral dynamics in mild and severe cases of COVID-19. The Lancet Infectious Diseases. 2020;S1473-3099(20):30232–2. doi: 10.1016/S1473-3099(20)30232-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.https://www.caltcm.org/assets/CALTCM%20COVID19%20QUADRUPLE%20AIM%20FINAL.pdf
- 21.https://ktla.com/news/local-news/1-a-county-officials-to-provide-latest-updates-on-coronavirus-crisis/
- 22.https://www.cdc.gov/coronavirus/2019-ncov/hcp/nursing-facilities-testing.html
- 23.https://www.latimes.com/california/story/2020-04-23/coronavirus-nursing-home-expanded-testing
- 24.https://www.reviewjournal.com/local/local-las-vegas/secrecy-fear-rampant-in-local-nursing-facilities-where-covid-19-is-too-2019702/
- 25.https://publicintegrity.org/health/coronavirus-and-inequality/when-nursing-home-workers-feel-like-lambs-led-to-slaughter/
- 26.Gardner W, States D, Bagley N. The Coronavirus and the Risks to the Elderly in Long-Term Care. Journal of Aging & Social Policy. Published April 3, 2020. Accessed May 14, 2020. DOI: 10.1080/08959420.2020.1750543 [DOI] [PubMed]
- 27.https://abc7.com/riverside-county-magnolia-rehabilitation-and-nursing-center-coronavirus/6086748/
- 28.http://paltc.org/sites/default/files/AMDA%20Policy%20Statement%20on%20Testing%202020%2005%2018%20FINAL.pdf
- 29.Jones J, Duncan H. Consensus methods for medical and health services research. BMJ. 1995;311:376–380. doi: 10.1136/bmj.311.7001.376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Staykova MP. Rediscovering the Delphi Technique: A Review of the Literature. Advances in Social Sciences Research Journal. 2019;6(1):218–229. [Google Scholar]