

Abstract
Since its outbreak in December 2019 in China, the novel coronavirus disease (COVID‐19) has rapidly spread and affected several countries. It has resulted in a difficult situation for cancer patients owing to the risks of the epidemic situation outbreak as well as cancer. Patients with cancer are more likely than the general population to contract COVID‐19 because of the systemic immunosuppressive status caused by malignant diseases or anticancer treatment. Lung cancer has the highest morbidity and mortality in China and the world. Most patients with lung cancer are smokers with poor underlying lung conditions and low immunity, thus it is vital to protect them from epidemic diseases during cancer treatment. It is necessary to provide individualized medical treatment and management of treatment‐related adverse events for patients with lung cancer based on patients' conditions and regional epidemic patterns.
Key points
Significant findings of the study During the outbreak of COVID‐19, taking patients' conditions and regional epidemic patterns into consideration, providing appropriate individualized treatment strategies for lung cancer patients with different stages is an urgent requirement.
What this study adds Based on the characteristics of lung cancer, this article aims to provide recommendations and suggestions of individualized treatment strategies and management of common adverse events for patients with lung cancer during the epidemic period of COVID‐19.
Keywords: COVID‐19, lung neoplasms, therapeutics
Introduction
At the end of 2019, a novel viral pneumonia caused by an unidentified pathogen was reported in Wuhan, China. The causative pathogen was identified as severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2; previously provisionally named 2019 novel coronavirus).1, 2 Owing to its extremely high infectivity and the susceptibility of the population, the 2019 novel coronavirus diseases (COVID‐19) has spread rapidly and widely in China and several other countries in less than two months. Faced with the gravity of the epidemic, China has incorporated COVID‐19 into the statutory Class B infectious diseases and controlled it in accordance with the Class A infectious diseases. Hospitals are not only the gathering places for suspected and diagnosed COVID‐19 patients but also high‐risk areas for infection. Reducing on‐site hospital gathering is a highly effective prevention and control measure to reduce the risk of cross infection, which has obviously affected the routine examination and treatment of lung cancer patients in regions affected by the epidemic.
One study showed that among patients infected with SARS‐CoV‐2, patients with malignant tumors progress to severe disease more rapidly than noncancer patients (13 vs. 43 days, P < 0.0001). The number of severe cases was approximately five times higher in cancer patients than in the general population (39% vs. 8%, P = 0.0003).3 In addition, lung cancer patients are more susceptible to COVID‐19 since they are usually elderly patients and smokers and have low immunity, poor nutritional status and poor lung conditions. Thus, they need to be well protected from COVID‐19. Conversely, some advanced lung cancer patients need to receive regular antitumor treatment due to the high tumor burden and deal with treatment‐related adverse events.
Therefore, to minimize the effect of the epidemic on lung cancer patients, providing recommendations of scientific and reasonable treatment and preventive measures for lung cancer patients in the global epidemic scenario is an urgent requirement. Based on the characteristics of lung cancer, this article focuses on individualized treatment recommendations and measures for adverse events management during the COVID‐19 epidemic.
Prevention of infection is paramount
Due to low immunity combined with poor lung function in lung cancer patients, it is vital to ensure protection and adopt measures for prevention. During the epidemic, lung cancer patients should stay at home and minimize going outside. We suggest that a regularly ventilated, clean, and regularly disinfected environment is necessary for lung cancer patients. In addition, patients should perform proper exercises at home to enhance their immunity. Adequate sleep is essential to maintain a good emotional state, and suitable methods to relieve tension, anxiety, and other emotions should be practiced; a safe and nutritious diet without raw meat and eggs must be consumed. Finally, body temperature and respiratory symptoms should be routinely monitored to identify problems and deal with them promptly.4
Recommendations of individualized medical treatment strategies
Lung cancer patients awaiting treatment
For lung cancer patients who have not yet started medical treatment, the treatment strategy should be comprehensively considered according to the tumor burden and general condition of the patient. For patients awaiting adjuvant chemotherapy after surgery, reasonable decisions should be made based on the postoperative pathology, clinical stage, genetic status, risk factors, and prognostic indicators. One study showed that lung cancer patients with a sluggish recovery can still benefit from delayed adjuvant chemotherapy starting four months after surgery without increasing mortality.5 Therefore, the duration of adjuvant chemotherapy for patients with postoperative lung cancer with earlier clinical stage and better prognosis can be appropriately extended during the epidemic. In addition, for patients with lymph node stage N2 after surgery with epidermal growth factor receptor (EGFR) gene mutations, oral EGFR tyrosine kinase inhibitor (EGFR‐TKI) treatment at home may be considered as the optional adjuvant treatment option,6 which may reduce the risk of cross infection caused by repeated hospital visits.
However, for patients with advanced lung cancer awaiting chemotherapy, in principle, limited extension of the waiting time with administration of antitumor treatment at the earliest are recommended possible. Professional oncologists must be consulted to identify more convenient alternatives, such as oral targeted drugs or chemotherapeutic agents. For patients that need immediate chemotherapy, choosing the nearest hospital with experience in chemotherapy is recommended.
Lung cancer patients undergoing chemotherapy
Lung cancer patients undergoing chemotherapy may not be able to receive timely chemotherapy during the epidemic. A major concern in these patients is the reduction in antitumor efficacy due to interruption of chemotherapy. Even if there is no effect of the epidemic, during normal chemotherapy, several patients have difficulty in advancing chemotherapy due to intolerable adverse events, local medical conditions, and family factors. Therefore, while we attach importance to the adverse effects of this epidemic on chemotherapy delays in patients with lung cancer, we should also regard the adjustment of chemotherapy regimen rationally. The treatment strategies should be appropriately adjusted under the guidance of an oncologist, according to the tumor burden of the individual, stage and effect of antitumor treatment, tolerance of antitumor treatment, and local epidemic situation.
We suggest that for patients with a low tumor burden and stable disease and those undergoing postoperative adjuvant chemotherapy and maintenance treatment, chemotherapy in hospital can be appropriately postponed or switched to oral chemotherapy with targeted drug administration at home. For patients who need further chemotherapy, it is recommended that the treatment should be carried out under the supervision of an oncologist. A safe chemotherapy regimen with appropriate dosage should be chosen and any adverse events post chemotherapy should be closely monitored.
Lung cancer patients undergoing targeted therapy
Targeted therapy is recommended for patients with advanced lung cancer with sensitive mutations such as EGFR, anaplastic lymphoma kinase fusion (ALK), and ROS1 fusion.7, 8 Studies show that patients receiving targeted therapy in combination with antivascular therapy, chemotherapy, or immunotherapy may experience enhanced antitumor effects.9, 10, 11, 12, 13 However, in the current epidemic situation, being vigilant about a possible increase in adverse events due to combination therapy is necessary.14, 15 Therefore, it is recommended that lung cancer patients with sensitive gene mutations be treated with oral targeted drugs during the outbreak, without combination therapy.16 Although patients can be treated at home with oral drugs, attention should still be paid to the adverse events of some targeted drugs. Patients whose symptoms are obviously relieved after targeted therapy and those with stable disease can be appropriately deferred to the hospital for review during the epidemic. Further, it is necessary to promptly consult a doctor under proper protection under emergency symptoms or obvious disease progression.
Lung cancer patients undergoing immunotherapy
Immune escape mechanism is one of the reasons why tumor cells can continuously replicate and proliferate in the human body.17 Programmed cell death‐1/programmed cell death ligand‐1 (PD‐1/PD‐L1) inhibitors developed by selectively blocking the pathway involved in tumor cell escape have spring boarded this therapy to a new stage, which to a certain extent may maintain longer‐lasting antitumor effects.18, 19, 20 We suggest that for lung cancer patients receiving immunotherapy during the epidemic, it is not urgent to receive immunotherapy on a set date. Considering the adverse events of potential pulmonary toxicity or injury caused by immunotherapeutic drugs, immunotherapy can be suspended or postponed in patients with stable disease.
Regular examination of lung cancer patients
Regular examination of patients with early‐stage postoperative lung cancer can be delayed. For advanced lung cancer patients receiving targeted therapy with sensitive gene mutations, the scheduled examination can be appropriately postponed or delayed on the basis of the cancer conditions. The interval between examinations can be extended to more than 2–3 months for patients with symptomatic remission or stable disease. During the postponed examination period, patients are advised to continuously take the original targeted drugs and closely monitor symptoms. Patients should be examined immediately and be kept well‐protected from infection, if symptoms progressively worsen. Examinations during chemotherapy should be performed in a timely manner as far as possible under permissible epidemic situations. The examination procedures and methods should be simplified to shorten hospital stays. After examination, patients may consult oncologists online or offline to comprehensively select the appropriate follow‐up treatment plans.
Management of common adverse events
Some lung cancer patients are required to undergo antitumor treatment such as systemic chemotherapy during the epidemic and deal with treatment‐related adverse events outside the hospital. The common adverse events include myelosuppression, nausea, and vomiting. We provide some recommendations for management of common adverse events outside the hospital for reference.
Routine blood examination should be emphasized in the management of patients during chemotherapy intermission to monitor the extent of myelosuppression through the important concerns including leukocyte counts, neutrophils, platelets, and red blood cells and hemoglobin levels. Mild‐to‐moderate myelosuppression can be treated with corresponding oral drugs. However, the following conditions need to be treated under medical guidance: leukocyte count <2.0 × 109/L, neutrophil count <1.0 × 109/L, or infection symptoms such as fever, frequent urination, and abnormal vaginal secretions in women; platelet count <50 × 109/L, or the occurrence of gum/nose bleeds and skin congestion; hemoglobin level < 100 g/L, or pale appearance, fatigue, anorexia, etc.
In order to reduce the incidence of nausea and vomiting, we recommend that patients rest and maintain a reasonable diet before chemotherapy. In addition to medication to prevent nausea and vomiting caused by chemotherapy such as ondansetron, studies have shown that psychological adjustments such as periorbital massage, listening to music, enjoying pictures, and yoga can also reduce the incidence of nausea and vomiting.21, 22, 23 If vomiting persists, a lateral position is essential when vomiting to prevent choking. After vomiting, we recommend that patients rinse their mouths with warm water in order to keep their mouths clean as well as clearing up vomit to avoid revomiting caused by the pungent smell. Moreover, if the manifestations continue, such as abnormal vomit color, excessive vomiting and dizziness, then patients should be taken to hospital for symptomatic treatment.
In addition, it is necessary to monitor the liver, kidney function and electrolytes in a timely manner, and intervene if necessary during the intervals between courses of chemotherapy. Moreover, lung cancer patients at home need to be aware of dyspnea caused by mass compression, bleeding or massive hemoptysis caused by tumor invasion of surrounding organs, electrolytes imbalance, and other emergencies such as severe arrhythmia. In case of emergencies, patients should seek medical treatments immediately under the condition of epidemic protection.
Management of lung infiltrative lesions during the epidemic outbreak
Lung cancer patients may be prone to lung infections due to low immunity or lung damage caused by chemotherapy, and targeted and immunotherapy drugs, which may lead to different degrees of lung infiltrative lesions on chest CT.14, 24, 25 These lesions need to be distinguished from the chest manifestations of COVID‐19 with multiple small patchy shadows and interstitial changes in early stage, multiple lung ground‐glass shadows, and infiltration shadows later, and even lung consolidation in severe cases.26, 27 We suggest that if this kind of problem occurs, patients should pay more attention to monitoring their respiratory symptoms and temperature with the suspension of antitumor treatment, and visit a hospital under the premise of self‐isolation and protection. Even patients without typical clinical symptoms, and peripheral blood routine performance cannot rule out the possibility of asymptomatic SARS‐CoV‐2 infection. We recommend that patients complete epidemiological history screening, SARS‐CoV‐2 nucleic acid and IgM/IgG antibody tests at designated hospitals to rule out COVID‐19 infection from other bacteriological infectious pneumonia or drug‐induced lung injury.28 The procedures recommended for SARS‐CoV‐2 infection screening and distinguished diagnosis are shown in Fig 1. The next appropriate treatment may be determined according to the causes and comprehensive situation of the individual patient.
Figure 1.
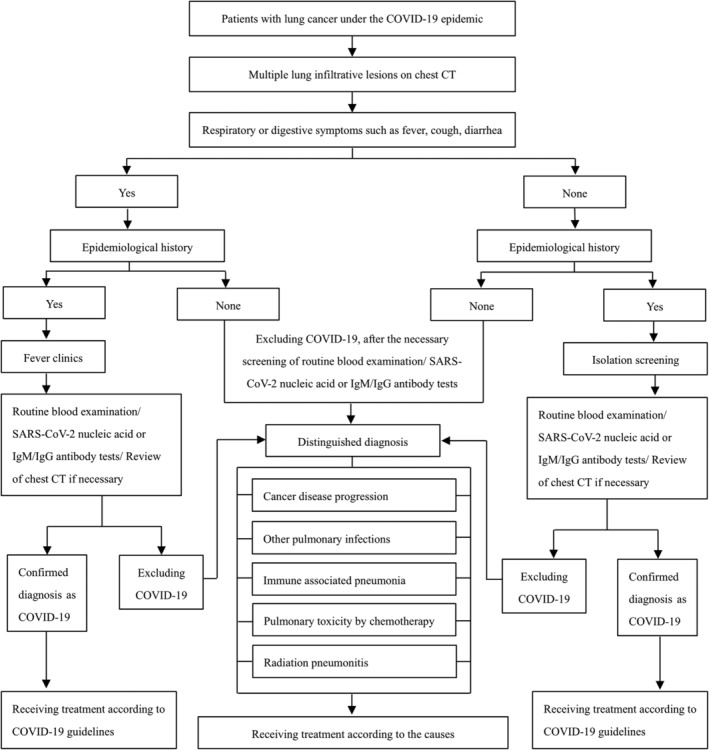
Procedures for SARS‐CoV‐2 infection screening and distinguished diagnosis with lung infiltrative lesions.
Psychological management during COVID‐19
The COVID‐19 global health emergency has resulted in increased anxiety, fear, depression and other negative emotions among civilians.29 Studies have shown that approximately half of the survivors of malignant tumors have moderate fear of cancer recurrence.30 Coupled with epidemic, lung cancer patients may worry about COVID‐19 and the impact of delayed antitumor treatment on their own treatment efficacy, which makes them more predisposed to anxiety, depression, and insomnia. We recommend that lung cancer patients may utilize association, relaxation exercises, appropriate venting to eliminate negative emotions,31 and use online psychological consultations and interventions if necessary.32
In conclusion, the COVID‐19 epidemic is undoubtedly a profound global health emergency, but people worldwide are courageous and need to be brave to fight this battle. Here, we provide available recommendations for the alternative transitional treatment and management of common treatment‐related adverse events for lung cancer patients at different stages during the epidemic. The war against the COVID‐19 epidemic will eventually be won, and we are willing to work with cancer patients to overcome the challenges!
Disclosure
The authors declare they have no competing interests.
Acknowledgments
This work was supported by the National key research and development project 2019YFC1315700; the National Natural Sciences Foundation Key Program (81630071); CAMS Innovation Fund for Medical Sciences (CIFMS 2016‐I2M‐3‐008); Aiyou foundation (KY201701), Ministry of Education Innovation Team development project (IRT‐17R10), and CAMS Key Laboratory of translational research on lung cancer (2018PT31035).
Contributor Information
Zhe Zhao, Email: 939662016@qq.com.
Jie Wang, Email: zlhuxi@163.com.
References
- 1. Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) and coronavirus disease‐2019 (COVID‐19): The epidemic and the challenges. Int J Antimicrob Agents 2020; 55: 105924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Jin YH, Cai L, Cheng ZS et al A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019‐nCoV) infected pneumonia (standard version). Mil Med Res 2020; 7: 4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Liang W, Guan W, Chen R et al Cancer patients in SARS‐CoV‐2 infection: A nationwide analysis in China. Lancet Oncol 2020; 21: 335–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Yuan JH, Li QS. Therape uticprocess and doctor‐patient protection measures of patients undergoing radiotherapy for tumors in the epidemic of novel coronavirus pneumonia. J Mod Oncol 2020; 28: 1–3. [Google Scholar]
- 5. Salazar MC, Rosen JE, Wang Z et al Association of delayed adjuvant chemotherapy with survival after lung cancer surgery. JAMA Oncol 2017; 3: 610–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Zhong WZ, Wang Q, Mao WM et al Gefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II‐IIIA (N1‐N2) EGFR‐mutant NSCLC (ADJUVANT/CTONG1104): A randomised, open‐label, phase 3 study. Lancet Oncol 2018; 19: 139–48. [DOI] [PubMed] [Google Scholar]
- 7. da Cunha SG, Shepherd FA, Tsao MS. EGFR mutations and lung cancer. Annu Rev Pathol 2011; 6: 49–69. [DOI] [PubMed] [Google Scholar]
- 8. Sgambato A, Casaluce F, Maione P, Gridelli C. Targeted therapies in non‐small cell lung cancer: A focus on ALK/ROS1 tyrosine kinase inhibitors. Expert Rev Anticancer Ther 2018; 18: 71–80. [DOI] [PubMed] [Google Scholar]
- 9. Li JX, Huang JM, Jiang ZB et al Current clinical Progress of PD‐1/PD‐L1 immunotherapy and potential combination treatment in non‐small cell lung cancer. Integr Cancer Ther 2019; 18:1534735419890020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Wargo JA, Reuben A, Cooper ZA, Oh KS, Sullivan RJ. Immune effects of chemotherapy, radiation, and targeted therapy and opportunities for combination with immunotherapy. Semin Oncol 2015; 42: 601–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Liu M, Wang X, Li H et al The effect of apatinib combined with chemotherapy or targeted therapy on non‐small cell lung cancer in vitro and vivo. Thorac Cancer 2019; 10: 1868–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Wang Y, Xie S, He B. Effect of EGFR gene polymorphism on efficacy of chemotherapy combined with targeted therapy for non‐small cell lung cancer in Chinese patients. Am J Cancer Res 2019; 9: 619–27. [PMC free article] [PubMed] [Google Scholar]
- 13. Qiang H, Chang Q, Xu J et al New advances in antiangiogenic combination therapeutic strategies for advanced non‐small cell lung cancer. J Cancer Res Clin Oncol 2020; 146: 631–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Sun X, Roudi R, Dai T et al Immune‐related adverse events associated with programmed cell death protein‐1 and programmed cell death ligand 1 inhibitors for non‐small cell lung cancer: A PRISMA systematic review and meta‐analysis. BMC Cancer 2019; 19: 558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Hoffner B, Leighl NB, Davies M. Toxicity management with combination chemotherapy and programmed death 1/programmed death ligand 1 inhibitor therapy in advanced lung cancer. Cancer Treat Rev 2020; 85: 101979. [DOI] [PubMed] [Google Scholar]
- 16. Lung Cancer Study Group . Chinese thoracic society, Chinese Medical Association. [expert recommendations on the management of patients with advanced non‐small cell lung cancer during epidemic of COVID‐19 (trial version)]. Zhonghua Jie He He Hu Xi Za Zhi 2020; 43: E031 10.3760/cma.j.cn112147-20200221-00138. [DOI] [PubMed] [Google Scholar]
- 17. Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: Integrating immunity's roles in cancer suppression and promotion. Science 2011; 331: 1565–70. [DOI] [PubMed] [Google Scholar]
- 18. Alsaab HO, Sau S, Alzhrani R et al PD‐1 and PD‐L1 checkpoint signaling inhibition for cancer immunotherapy: Mechanism, combinations, and clinical outcome. Front Pharmacol 2017; 8: 561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Santini FC, Hellmann MD. PD‐1/PD‐L1 Axis in lung cancer. Cancer J 2018; 24: 15–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Villanueva N, Bazhenova L. New strategies in immunotherapy for lung cancer: Beyond PD‐1/PD‐L1. Ther Adv Respir Dis 2018; 12: 1753466618794133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Dadkhah B, Anisi E, Mozaffari N, Amani F, Pourghasemian M. Effect of music therapy with Periorbital massage on chemotherapy‐induced nausea and vomiting in gastrointestinal cancer: A randomized Controlled Trail. J Caring Sci 2019; 8: 165–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Karagozoglu S, Tekyasar F, Yilmaz FA. Effects of music therapy and guided visual imagery on chemotherapy‐induced anxiety and nausea‐vomiting. J Clin Nurs 2013; 22: 39–50. [DOI] [PubMed] [Google Scholar]
- 23. Raghavendra RM, Nagarathna R, Nagendra HR et al Effects of an integrated yoga programme on chemotherapy‐induced nausea and emesis in breast cancer patients. Eur J Cancer Care 2007; 16: 462–74. [DOI] [PubMed] [Google Scholar]
- 24. Carlisle PS, Gucalp R, Wiernik PH. Nosocomial infections in neutropenic cancer patients. Infect Control Hosp Epidemiol 1993; 14: 320–4. [DOI] [PubMed] [Google Scholar]
- 25. Binder D, Hubner RH, Temmesfeld‐Wollbruck B, Schlattmann P. Pulmonary toxicity among cancer patients treated with a combination of docetaxel and gemcitabine: A meta‐analysis of clinical trials. Cancer Chemother Pharmacol 2011; 68: 1575–83. [DOI] [PubMed] [Google Scholar]
- 26. Li Y, Xia L. Coronavirus disease 2019 (COVID‐19): Role of chest CT in diagnosis and management. Am J Roentgenol 2020; 4: 1–7. [DOI] [PubMed] [Google Scholar]
- 27. Dai WC, Zhang HW, Yu J et al CT imaging and differential diagnosis of COVID‐19. Can Assoc Radiol J 2020; 4: 846537120913033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Rubin EJ, Baden LR, Morrissey S. Audio interview: What clinicians need to know in diagnosing and treating Covid‐19. N Engl J Med 2020; 382: e19. [DOI] [PubMed] [Google Scholar]
- 29. Wang C, Pan R, Wan X et al Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID‐19) epidemic among the general population in China. Int J Environ Res Public Health 2020; 17: E1729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Simard S, Thewes B, Humphris G et al Fear of cancer recurrence in adult cancer survivors: A systematic review of quantitative studies. J Cancer Surviv 2013; 7: 300–22. [DOI] [PubMed] [Google Scholar]
- 31. Duan L, Zhu G. Psychological interventions for people affected by the COVID‐19 epidemic. Lancet Psychiatry 2020; 7: 300–2. 10.1016/S2215-0366(20)30073-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Liu S, Yang L, Zhang C et al Online mental health services in China during the COVID‐19 outbreak. Lancet Psychiatry 2020; 7: e17–8. 10.1016/S2215-0366(20)30077-8. [DOI] [PMC free article] [PubMed] [Google Scholar]