

Abstract
Hypertension and obesity are known to be linked, with recent studies in mice proposing that leptin may be mediating this effect. This regulation, however, may not extend to humans, where a yet-to-be-identified factor is likely the underlying cause of hypertension.
It has been shown in population studies that a number of cardiovascular risk factors correlate with obesity and form the metabolic syndrome. The mechanism by which these cardiovascular risk factors relate to obesity are unclear. Simonds et. al. (1) have proposed that leptin mediates the increase in blood pressure associated with obesity. The basis for this largely comes from mouse studies in which leptin appears to activate sympathetic activity through neuronal circuits in the dorsal-medial hypothalamus. Simonds et. al. (1) present evidence that leptin mediates an increase in both systolic and diastolic blood pressure as well as an increase in heart rate in a diet-induced obesity mouse model.
In an attempt to extend the relevance of these mouse experiments to humans they cite several observations. The major observation is that patients with congenital leptin deficiency or leptin receptor deficiency have low systolic blood pressure (but normal diastolic blood pressure) compared to weight matched controls. Although patients with congenital leptin deficiency respond to leptin therapy by increased satiety and weight loss, there is no change in blood pressure when leptin is given to these individuals. Further, Simonds et. al. (1) point out that Heymsfield et. al. (2) did not observe an increase in blood pressure in obese patients who had minimal weight loss in response to leptin therapy.
Current human data suggest that metabolic parameters such as appetite, body weight, triglycerides, and diabetes control respond to leptin administration in endogenous low-leptin states (3, 4) but not in endogenous high-leptin states (2). The proposal that leptin mediates the increase in blood pressure in obesity, an endogenous high-leptin state, would represent an exception to the general idea of leptin resistance in endogenous high-leptin states.
Because leptin administration does not increase blood pressure in congenital leptin deficiency, we examined another low leptin state, lipodystrophy, to see if leptin affects blood pressure. Lipodystrophies are a heterogeneous group of disorders characterized by generalized or depot-specific absence of subcutaneous adipose tissue and, hence, low levels of the adipocyte-derived hormone, leptin. Complications of lipodystrophy are typical of an extreme variant of the obesity-associated metabolic syndrome, including insulin resistance, diabetes, hypertriglyceridemia, and fatty liver disease; these complications are significantly improved by leptin replacement. We examined blood pressure in 107 patients with lipodystrophy of various types. Patients were enrolled in a prospective, single-arm, open-label study evaluating effects of recombinant human leptin (metreleptin) on metabolic complications of lipodystrophy. The study was approved by the institutional review board of the National Institute of Diabetes and Digestive and Kidney Diseases (NCT00025883), and all patients or their guardians provided written informed consent.
Unlike patients with congenital leptin deficiency, more than one third of patients with lipodystrophy (mean age 24 ± 15 years) had hypertension in the leptin-deficient state. Further, we found no increase in either systolic or diastolic blood pressure in these patients after 6 months of leptin treatment, and small but significant decreases in systolic and diastolic blood pressure after 12 months of leptin treatment at a mean dose of 0.085 ± 0.035 mg/kg/day (Figure 1). Under these conditions, serum leptin levels are increased significantly by exogenous leptin administration (4).
Figure 1.
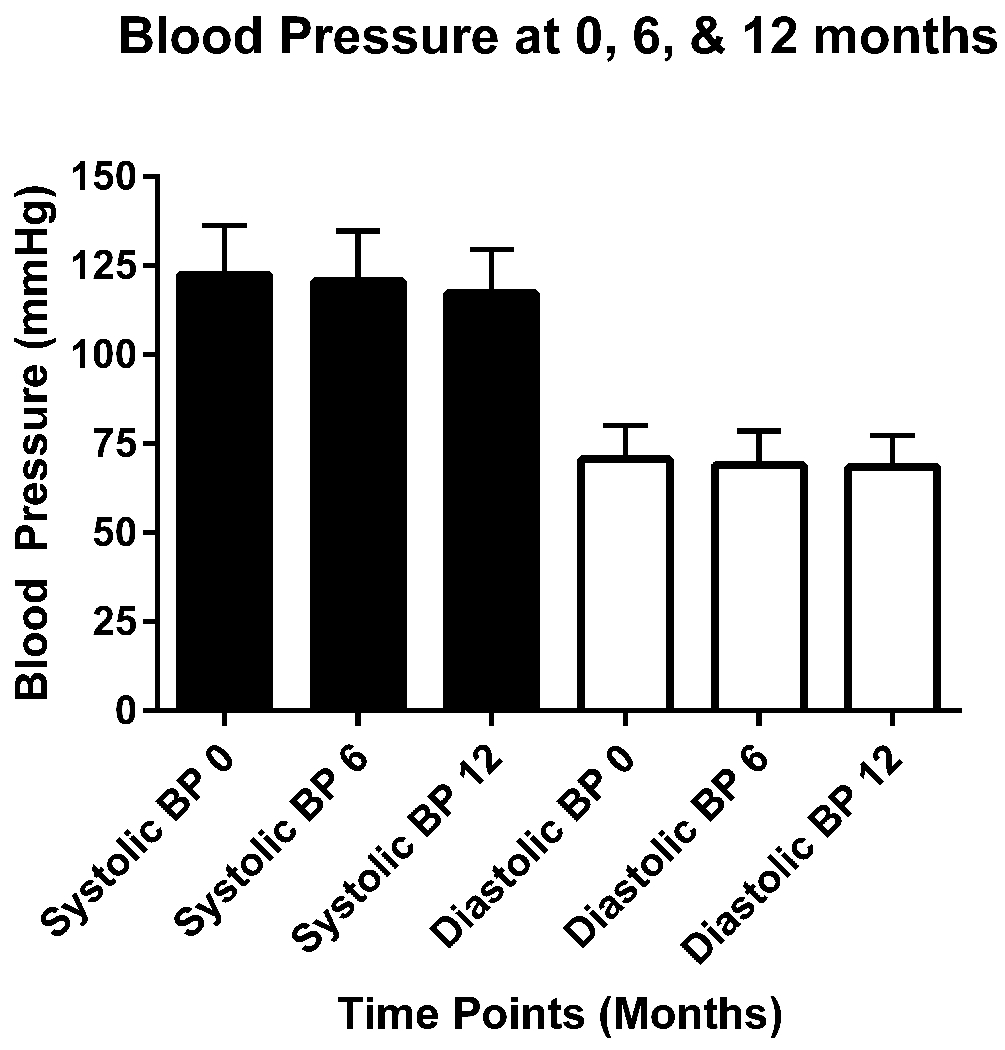
Blood Pressure in 107 Patients with Lipodystrophy at Baseline and after 6 and 12 Months of Leptin Replacement
Blood pressure decreased significantly after 12 months (p = 0.003 for systolic and 0.02 for diastolic).
These data demonstrate that mouse models may not predict human adverse events. Thus, hypertension was not considered an adverse event in the FDA approval of leptin as a therapy for lipodystrophy, which is consistent with the data presented in Figure 1. We conclude that, because leptin administration does not increase blood pressure in the leptin responsive states of congenital leptin deficiency or lipodystrophy, it is premature to suggest that leptin is the mediator of the hypertension associated with human obesity.
References
- 1.Simonds SE, Pryor JT, Ravussin E, Greenway FL, Dileone R, Allen AM, et al. Leptin mediates the increase in blood pressure associated with obesity. Cell. 2014;159(6):1404–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Heymsfield SB, Greenberg AS, Fujioka K, Dixon RM, Kushner R, Hunt T, et al. Recombinant leptin for weight loss in obese and lean adults: a randomized, controlled, dose-escalation trial. JAMA. 1999;282(16):1568–75. [DOI] [PubMed] [Google Scholar]
- 3.Farooqi IS, Matarese G, Lord GM, Keogh JM, Lawrence E, Agwu C, et al. Beneficial effects of leptin on obesity, T cell hyporesponsiveness, and neuroendocrine/metabolic dysfunction of human congenital leptin deficiency. J Clin Invest. 2002;110(8):1093–103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Oral EA, Simha V, Ruiz E, Andewelt A, Premkumar A, Snell P, et al. Leptin-replacement therapy for lipodystrophy. N Engl J Med. 2002;346(8):570–8. [DOI] [PubMed] [Google Scholar]