

Abstract
Background
Clinical detection of EGFR‐TKI resistance mechanism through tissue can be really challenging due to risks associated with the procedure. Thus, liquid biopsy, especially circulation tumor DNA (ctDNA) analysis, can be an adequate source for biomarker testing in targeted therapy. Our study was aimed at clinical validation of liquid biopsy next‐generation sequencing (NGS) by comparison with tissue biopsy, and we also investigated clinical utility of ctDNA NGS on the prediction of TKI outcomes.
Methods
Using hybrid capture panel NGS, we compared the concordance, sensitivity, and specificity of ctDNA using 39 paired plasma and tissue biopsy, and investigated the association between ctDNA genomic alterations of 147 first‐generation TKI‐relapsed patients and their response to first‐ and third‐generation TKIs.
Results
The concordance for ctDNA and tissue biopsy was 84.62% among all patients, and even higher among late stage patients (88.24%). Among 147 EGFR‐TKI‐relapsed patients, T790M was the most common reason for resistance (40.13%). Compared with T790M‐positive patients, patients only detected with sensitizing mutations (sensi‐mutations) had lower mutant allele frequency (MAF) of sensi‐mutations (P = 0.031). TP53 mutation showed negative impact on TKI treatments. In survival analysis of third‐generation TKI, we found a positive correlation between ratio of T790M sensi‐mutation and PFS (P = 0.018); also, higher MAFs of both sensi‐mutation and T790M were observed in the PR group than the SD + PD group.
Conclusions
Both ratio of T790M sensi‐mutations and MAFs of EGFR mutations were associated with third‐generation TKI outcomes. Thus, incorporation of high‐throughput NGS into clinical trials may be crucial to identifying the response to osimertinib, as it provides more comprehensive genomic information.
Key points
High concordance of ctDNA and tissue biopsy was observed. NGS of ctDNA from 147 TKI‐relapsed patients showed that both high ratio of T790M sensitizing mutation (sensi‐mutation) and high MAFs of mutations were all associated with better third generation TKI treatment outcomes.
The quantification of both MAFs and T790M sensi‐mutation ratio should be taken into consideration in some clinical situations, and incorporation of high‐throughput NGS into clinical trials may be crucial to identifying the response to osimertinib, as it provides more comprehensive genomic information.
Keywords: High‐throughput NGS, liquid biopsy, MAF, outcomes, ratio
Introduction
Lung cancer represents the leading cause of cancer‐related deaths worldwide.1 A subgroup of non‐small lung cancer (NSCLC) patients have been reported to have activating EGFR mutations,2 and responded well to first‐generation EGFR tyrosine kinase inhibitors (EGFR‐TKIs). However, most patients harboring EGFR‐activating mutations eventually acquire resistance to the first‐generation TKI treatment after a median response of 10–12 months.3 The most common resistance mechanism is the development of T790M mutation in exon 20 of the EGFR gene.3 MET amplification, ERBB2 amplification, PIK3CA mutation and BRAF mutations have also been reported to cause resistance.4, 5
Unfortunately, clinical detection of resistance mechanism through tissue biopsy can be really challenging due to risks associated with the procedure, particularly for TKI‐relapsed patients. Tissue biopsy can also be incomplete because of spatial and temporal tumor heterogeneity. Liquid biopsy obtained by minimal invasive blood draws are therefore became accessible at almost all clinical situations.6 The fraction of circulating tumor DNA (ctDNA) in cell‐free DNA (cfDNA) varies according to tumor stage, tumor burden, vascularization of the tumor, apoptotic rate of tumor and the metastatic potential of the cancer cell.7 As a result, ctDNA often represents a small percentage of the total cfDNA and can be present at really low allele fractions. Therefore, highly sensitive methodologies should be used to detected low abundance mutations from cfDNA in NSCLC patients.8, 9 Currently, digital PCR, BEAMing (beads, emulsion, amplification and magnetics), and next‐generation sequencing (NGS) are widely used in genetic testing of ctDNA.10 Although some of these methods enable a sensitivity detection down to 0.01%, only NGS utilizes parallel sequencing to detect a broader range of genomic alterations by multitarget gene panels.
In this retrospective study, clinical validation of liquid biopsy was performed by concordance, sensitivity, and specificity of ctDNA hybrid capture panel NGS using 39 paired plasma and tissue biopsy from lung cancer patients. We also investigated the resistance mechanisms of 147 plasma samples from first‐generation TKI‐relapsed patients, and analyzed the ability to predict target therapy outcomes by ctDNA NGS.
Methods
Patients
We retrospectively reviewed all the patients who had been diagnosed with NSCLC and undergone ctDNA genetic test using NGS between March 2017 to May 2018 at the Cancer Hospital, Chinese Academy of Medical Sciences (CAMS, Beijing, China). A total of 39 blood samples with paired tissue biopsy samples were enrolled in our study for the comparison between liquid and tissue biopsy. Tissue biopsy samples were all collected at the same time period with blood samples. Another 147 blood samples from first‐generation EGFR‐TKI‐relapsed patients were also enrolled in the study in order to analyze the ability to predict target therapy outcomes by ctDNA NGS.
Study design
The study included 39 blood samples with paired tissue biopsy samples and 147 blood samples collected from first‐generation EGFR‐TKI‐relapsed patients (Fig 1). Clinicopathological parameters were collected through electronic medical records. All tissue samples were formalin‐fixed paraffin‐embedded. For survival analysis, 147 TKI‐relapsed patients were followed up since their first dose of TKI until disease progression. This study was approved by the institutional review board of the Cancer Hospital, CAMS, and was conducted in accordance with the Declaration of Helsinki.
Figure 1.
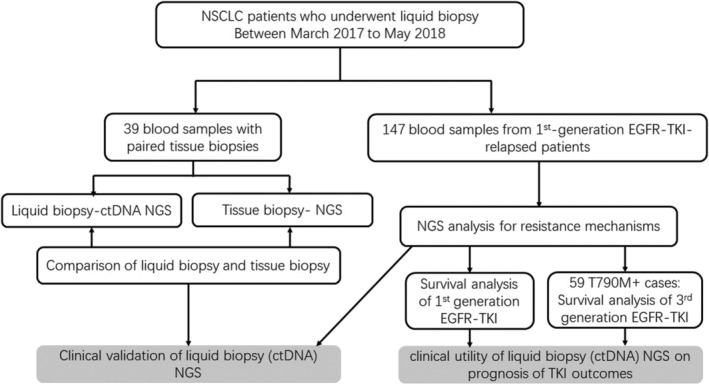
Study flow chart. Abbreviations: ctDNA, circulation tumor DNA; NGS, next generation sequencing; NSCLC, non‐small cell lung cancer.
FFPE tissue specimen processing and DNA extraction
Tissue biopsy samples were collected and processed by standard procedures. DNAs from FFPE samples were extracted using QIAamp DNA FFPE Tissue Kits (Qiagen, Duesseldorf, Germany), following the manufacturer's instructions. DNA quantity was determined by Qubit 2.0 Fluorometer (Thermo Fisher Scientific, Carlsbad, CA, USA).
Plasma processing and DNA extraction
We collected 10 mL of whole blood into EDTA‐containing tubes, and plasma was separated within one hour of collection. Briefly, whole blood at 4°C was centrifuged at 2000 × g for 10 minutes, and the supernatant was transferred to a new 15 mL tube and centrifuged at 16000 × g for another 10 minutes at 4°C. About 4 mL plasma was then collected for DNA extraction. CtDNA was extracted from 4 mL plasma using the Plasma Circulating Nucleic Acid Preparation Kit (Qiagen, Duesseldorf, Germany), following the manufacturer's instructions. DNA quantity was determined by Qubit 2.0 Fluorometer (Thermo Fisher Scientific, Carlsbad, CA, USA).
NGS analyses
Targeted NGS were performed using a capture‐based panel that covers 168 cancer‐related genes as previously reported.11 Available indexed samples were sequenced on NextSeq (Illumina, San Diego, CA) with paired‐end reads. The minimal median sequencing depth was 12 000× for ctDNA and 1000× for tissue DNA.
Clinical response evaluation
The response evaluation was assessed according to Response Evaluation Criteria in Solid Tumors (RECIST), version 1.112 by an independent medical oncologist. Progression‐free survival (PFS) was calculated from the date of initiation of TKI to the date of disease progression. The objective response rate (ORR) was calculated as the total percentage of patients with optimal efficacy of complete response (CR) or partial response (PR). The disease control rate (DCR) was calculated as the total percentage of patients with CR, PR or stable disease (SD).
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, Chicago, IL, USA) version 22.0. Differences between groups were compared using the Pearson's χ2 test for categorical data, and t‐tests for continuous data. PFS were estimated using the Kaplan‐Meier method, and differences in PFS were assessed by log‐rank test. A two‐sided P‐value <0.05 was considered statistically significant.
Results
Comparison of liquid and tissue biopsy
A total of 39 paired blood and tissue biopsy were enrolled in our study. Nine paired tissue‐liquid samples were obtained from the TKI‐resistant patients, while the other 30 paired samples were obtained from TKI‐naïve patients. NGS tests using ctDNA revealed 15 cases were negative for all driver‐gene alterations, 12 cases harboring EGFR mutations, three cases harboring KRAS mutations, seven cases harboring ALK rearrangement, one case with ROS1 rearrangement, and one case with RET rearrangement. High concordance of 84.62% were observed between ctDNA and tissue biopsies (Table 1). NGS sensitivity for ctDNA was 82.14% and specificity was 90.91%. It should be noted that the case with RET rearrangement in ctDNA NGS showed negative results in its paired tissue biopsy NGS. The probable reason for this was tumor heterogeneity.
Table 1.
Comparison of ctDNA NGS and tissue biopsies NGS (N = 39)
| Tissue biopsy NGS | ||||
|---|---|---|---|---|
| Tissue biopsy Liquid biopsy | Negative | Positive | Concordance | |
| ctDNA NGS | Negative | 10† | 5‡ | 84.62%†† |
| Positive | 1§ | 23¶ | ||
Including two stage I–II cases and 8 stage III–IV cases.
Including two stage I–II cases and 3 stage III–IV cases.
Stage III–IV patients.
Including one stage I–II cases and 22 stage III–IV cases.
The concordance was 88.24% for late stage (stage III–IV) patients.
Among nine TKI‐resistant paired samples, two cases were proved to be ctDNA NGS false negative with positive tissue NGS results (one gefitinib‐resistant case and one crizotinib‐resistant case). Among 30 TKI‐naïve paired samples, four cases were proved to be ctDNA NGS false negative. For the type of biopsy procedure,, 21 patients underwent lung biopsies (13 transbronchial lung biopsies, and nine transthoracic needle lung biopsies), six cases obtained tumor cells from malignant pleural effusion, and eight cases underwent cervical lymph node biopsies. Liver, hip, and brain biopsies were used for the other three cases, respectively.
Among these 39 patients, five were early stage patients (I–II stage) and 34 were late stage patients (III–IV stage) (Table 1). If we only took late stage patients into consideration, the concordance, sensitivity, and specificity for ctDNA among late stage patients were 88.24%, 88.00% and 88.89%, respectively.
Patient characteristics
The clinicopathologic characteristics of 147 EGFR‐TKI‐relapsed patients are summarized in Table 2. The median age at diagnosis was 62 years (range 34–83) and 57.14% (84/147) patients were female. A total of 59.18% (87/147) of patients were never smokers, and 21.77% (32/147) were former smokers (with 28 cases missing data). A total of 57.14% (84/147) were stage IIIB/IV patients without surgery, while 41.50% (61/147) were postoperative recurrent patients. The most common EGFR mutation type was L858R (44.9%, 66/147), followed by exon19 deletions (19del) (40.8%, 60/147). Other clinical characteristics such as metastasis status are listed in Table 2.
Table 2.
Clinicopathological characteristics of EGFR‐TKI‐relapsed patients
| Characteristics | No. of patients (N = 147) |
|---|---|
| Median age, years (range) | 62 (34–83) |
| Sex | |
| Male | 63 (42.86%) |
| Female | 84 (57.14%) |
| Tobacco | |
| Ever | 32 (21.77%) |
| Never | 87 (59.18%) |
| Missing data | 28 (19.05%) |
| Stage before TKI treatment | |
| IIIB/IV without surgery | 84 (57.14%) |
| Postoperative recurrent | 61 (41.50%) |
| Missing data | 2 (1.36%) |
| Sensitizing mutation before TKI treatment | |
| 18 exon (G719X) | 5 (3.40%) |
| 18 + 20 exon (G719X + L861X) | 4 (2.72%) |
| 20 exon alterations (20ins or S768X) | 3 (2.04%) |
| 19 exon deletions (19del) | 60 (40.82%) |
| L858R | 66 (44.89%) |
| Missing data | 9 (6.12%) |
| Metastases (when liquid biopsy was performed) | |
| M0/M1a | 52 (35.37%) |
| M1b | 91 (61.90%) |
| Missing data | 4 (2.72%) |
| Bone metastases | |
| No | 88 (59.86%) |
| Yes | 55 (37.41%) |
| Missing data | 4 (2.72%) |
| Brain metastases | |
| No | 68 (46.26%) |
| Yes | 56 (38.10%) |
| Missing data | 23 (15.65%) |
NGS results for EGFR‐TKI‐relapsed patients
Cancer‐related gene mutations were detected in most patients (81.63%, 120/147) including EGFR, MET, ERBB2, TP53, PIK3CA, PTEN, RB1, SMAD4, CTNNB1, CDKN2A, and MTOR, whereas 27 patients (18.36%) were negative in the NGS test (Fig 2a). T790M was observed as resistance mechanism in 40.13% (59/147) patients; EGFR sensitizing mutations without T790M were only detected in 27.89% (41/147) of patients; and 29.93% (44/147) of patients were negative for EGFR mutations (Fig 2a). For the 44 patients, the median age at diagnosis was 62.5 years (range 40–81) and 56.82% (25/44) patients were female. A total of 47.73% (21/44) received EGFR‐TKI treatment as first‐line, while 50.00% (22/44) received EGFR‐TKI after chemotherapy (one missing data). A total of 36.36% (16/44) of those patients had brain metastases when liquid biopsy was performed. No difference in brain metastases ratio were observed between the 44 patients and others with EGFR mutations. However, bone metastases were more common in patients detected with EGFR mutations than those without any EGFR mutations (44.00% vs. 25.58%, P = 0.042). No other significant difference of clinical characteristics were observed between patients who were negative for EGFR mutations and others. We also found 2.04% (3/147) of patients developed alternative pathway activations (including MET amplification and ERBB2 amplification) as resistance mechanisms. A total of 133 cases have been tested for TP53 status, and 45.86% (61/133) of them detected with TP53 mutations. TP53 mutations were more common observed with a concurrent 19del mutation than L858R (P = 0.014, Fig S4a). We also found that TP53 mutations much more frequently coexisted with other cancer‐related gene alterations (P = 0.025, Fig S4b).
Figure 2.

NGS results for ctDNA from 147 first‐generation EGFR‐TKI‐relapsed patients. (a) Sensitizing mutation types before TKI treatment of 147 cases, and mutation profiling of ctDNA NGS results. (b) Comparison of T790M frequency between different sensitizing mutation types (19del vs. L858R). (c) Difference in ctDNA quantity between T790M‐positive patients and patients only been detected with sensitizing mutations. (d) Difference in sensitizing mutation MAFs between T790M‐positive patients and patients only been detected with sensitizing mutations. (a)  19DEL,
19DEL,  L858R,
L858R,  18exon,
18exon,  18+20exons,
18+20exons,  20exon,
20exon,  unknown sensitizing mutations,
unknown sensitizing mutations,  sensitizing mutations+T790M,
sensitizing mutations+T790M,  sensitizing mutations+alternative pathway activations,
sensitizing mutations+alternative pathway activations,  only sensitizing mutations,
only sensitizing mutations,  with EGFR amplification,
with EGFR amplification,  mutations,
mutations,  , Not Available, (b)
, Not Available, (b)  T790M1+,
T790M1+,  T790M1−.
T790M1−.
T790M was more likely to coexist with 19del than L858R, although with a borderline P‐value (Fig 2b, P = 0.171). Compared with cases only detected with sensitizing mutations, the T790M‐positive group seemed to have higher ctDNA quantity for NGS library construction (mean ± SD: 72.37 ± 28.17ng vs. 60.82 ± 23.38 ng, P = 0.033, Fig 2c) and higher sensitizing mutant allele frequency (MAF) (mean MAF ± SD: 7.13% ± 10.88% vs. 3.13% ± 7.02%, P = 0.031, Fig 2d). In the T790M‐positive group, the ratio of T790M/sensitizing mutation in 80% patients was below 100%, which suggested intratumor heterogeneity of T790M.
Among 59 T790M‐positive cases, the association of clinical characteristics and MAFs of T790M were also analyzed (one missing data). A total of 35.59% (21/59) of patients underwent surgeries before TKI treatment. When ctDNA NGS was performed, 50.85% (30/59) had bone metastases, 37.29% (22/59) had brain metastases. The majority of patients (74.58%, 44/59) had extrapulmonary metastases (M1b), 18.64% (11/59) were M1a, while only three cases (5.08%) did not have metastasis. We found that the MAF of T790M were significantly higher in M1b cases than others (M0 and M1a) (mean ± SD: 4.66% ± 7.27% vs. 0.39% ± 0.39%, P < 0.001). No other significant association was observed between other clinical characteristics and T790M MAFs. No significant association was observed between clinical characteristics and sensi‐mutation MAFs.
Survival analysis of first‐generation TKI
All 147 patients received first‐generation EGFR‐TKI treatment between March 2007 to Feb 2018, and were diagnosed with disease progression. ORR for first‐generation TKI was 54.47% and DCR was 96.27%. No significant difference of ORR or DCR was observed between 19del and L858R. However, the TP53 mutation group had a much lower ORR than the TP53 wild‐type group (P = 0.046, Table 3).
Table 3.
Response to treatment for patients with EGFR‐TKI
| Sensitizing mutations | T790M status after first TKI relapsed | TP53 status | |||||||
|---|---|---|---|---|---|---|---|---|---|
| 19del | L858R | P | Positive | Negative | P | Positive | Negative | P | |
| Response to first‐generation TKI | |||||||||
| Type of response ‐ No. (%) | |||||||||
| Complete response | 1 (1.67) | 2 (3.03) | 1 (1.69) | 2 (2.27) | 2 (3.28) | 0 (0) | |||
| Partial response | 27 (45.00) | 34 (51.52) | 24 (40.68) | 46 (52.27) | 23 (37.70) | 42 (58.33) | |||
| Stable disease | 25 (41.67) | 24 (36.36) | 31 (52.54) | 25 (28.41) | 28 (45.90) | 23 (31.94) | |||
| Progressive disease | 3 (5.00) | 1 (1.52) | 0 (0) | 5 (5.68) | 3 (4.92) | 2 (2.78) | |||
| Could not be evaluated | 4 (6.67) | 5 (7.58) | 3 (5.08) | 10 (11.36) | 5 (8.20) | 5 (6.94) | |||
| Objective response rate ‐ % (95% CI) | 50.00 (36.49–63.51) | 59.02 (46.32–71.72) | 0.332 | 44.64 (31.21–58.08) | 61.54 (50.49–72.58) | 0.053 | 44.64 (31.21–58.08) | 63.69 (50.80–74.57) | 0.046 |
| Disease control rate % (95% CI) | 94.64 (88.56–100) | 98.36 (95.08–100) | 0.284 | 100 | 93.59 (88.03–99.15) | 0.054 | 95.64 (88.56–100) | 97.01 (92.83–100) | 0.511 |
| Time to response ‐ months | |||||||||
| Mean | 3.74 | 6.29 | 0.102 | 2.66 | 8.07 | 0.000 | 3.59 | 6.59 | 0.033 |
| 95% CI | 2.08–5.40 | 3.78–8.81 | 1.92–3.40 | 5.51–10.64 | 1.97–5.21 | 4.32–8.86 | |||
| Duration of response – months | |||||||||
| Mean | 13.30 | 15.95 | 0.490 | 16.57 | 11.49 | 0.136 | 14.35 | 12.78 | 0.651 |
| 95% CI | 8.33–18.27 | 10.09–21.81 | 11.57–21.57 | 7.07–15.90 | 8.65–20.06 | 8.58–16.98 | |||
| Response to third‐generation TKI | |||||||||
| Type of response ‐ No. (%) | |||||||||
| Complete response | 0 (0) | 0 (0) | 0 (0) | ‐ | ‐ | 0 (0) | 0 (0) | ||
| Partial response | 17 (56.67) | 7 (28.00) | 26 (44.07) | ‐ | ‐ | 17 (51.52) | 7 (35.00) | ||
| Stable disease | 7 (23.33) | 13 (52.00) | 20 (33.90) | ‐ | ‐ | 9 (27.27) | 8 (40.00) | ||
| Progressive disease | 0 (0) | 0 (0) | 1 (1.69) | ‐ | ‐ | 1 (3.03) | 0 (0) | ||
| Could not be evaluated | 6 (20.00) | 5 (20.00) | 12 (20.34) | ‐ | ‐ | 6 (18.18) | 5 (25.00) | ||
| Objective response rate ‐ % (95% CI) | 70.83 (51.23–90.44) | 35.00 (12.10–57.90) | 0.017 | 55.32 (40.56–70.07) | ‐ | ‐ | 62.96 (43.50–82.43) | 46.67 (18.07–75.26) | 0.318 |
| Disease control rate ‐ % (95% CI) | 100 | 100 | ‐ | 97.87 (93.59–100) | ‐ | ‐ | 96.30 (88.68–100) | 100 | 0.463 |
| Time to response ‐ months | |||||||||
| Mean | 1.96 | 1.79 | 0.697 | 1.92 | ‐ | ‐ | 1.77 | 1.95 | 0.708 |
| 95% CI | 1.41–2.51 | 1.03–2.54 | 1.48–2.34 | ‐ | 1.16–2.38 | 1.19–2.70 | |||
| Duration of response ‐ months | |||||||||
| Mean | 4.98 | 6.07 | 0.447 | 5.66 | ‐ | ‐ | 4.54 | 7.16 | 0.092 |
| 95% CI | 2.65–7.31 | 3.85–8.28 | 4.25–7.06 | ‐ | 2.40–6.68 | 4.39–9.94 | |||
The median PFS of first‐generation TKI was 13.73 months (95% CI: 12.16–15.31 months, Fig S1a). Sensitizing mutation types showed no significant influence on PFS, neither did TP53 status (Fig S1b,S1c). The T790M‐positive group had a much shorter time to response than the T790M‐negative group (P = 0.000, Table 3). Also, the TP53 positive group had a shorter time to response than the TP53 wild‐type group (P = 0.037, Table 3).
Survival analysis of third‐generation TKI
Among 59 patients detected with T790M, 46 patients had received osimertinib treatment during September 2015 to June 2018. The last follow‐up date was 31 August 2018, when 43.48% (20/46) of patients progressed from third‐generation TKI treatment. A total of 41.30% (19/46) of these patients were treated with second‐line therapy, and 43.48% (20/46) of patients received osimertinib as third‐line treatment (chemotherapy as first‐line therapy, and first‐generation TKI as second‐line therapy). Six patients received more than two lines of treatment before osimertinib, with one missing data. ORR and DCR for third‐generation TKI were 55.32% and 97.87%, respectively. Patients harboring 19del had higher ORR than those harboring L858R (P = 0.017, Table 3). Moreover, compared with optimal efficacy of the SD + PD group, the PR group seemed to have higher MAF of sensitizing mutation (mean ± SD: 12.37% ± 13.37% vs. 2.67% ± 4.17%, P = 0.002) and higher T790M MAF (mean ± SD: 5.68% ± 7.47% vs. 1.49% ± 3.18%, P = 0.014) (Fig 3a).
Figure 3.
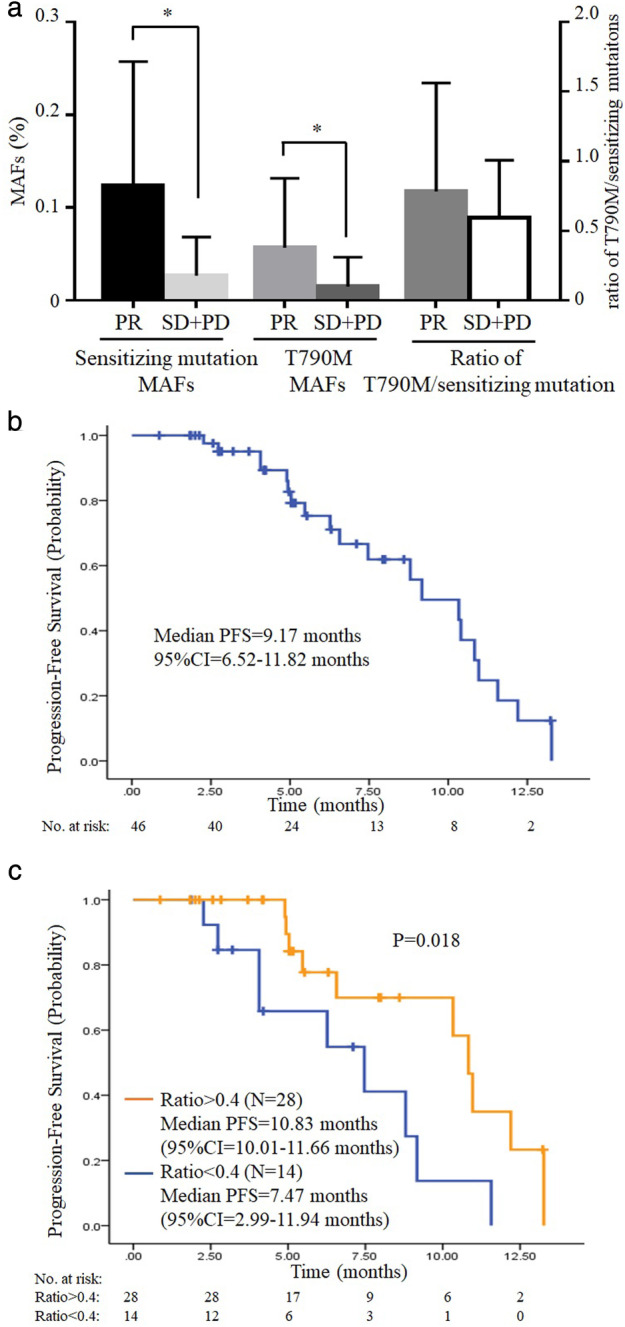
Survival analysis of third‐generation TKI. (a) Comparison of sensitizing mutation MAFs, T790M MAFs and ratio of T790M sensitizing mutation (sensi‐mutation) according to optimal efficacy of third‐generation TKI. (b) Kaplan‐Meier estimates of third‐generation TKI progression‐free survival (PFS). (c) Survival curves according to ratio of T790M sensi‐mutation.
The median PFS of third‐generation TKI was 9.17 months (95% CI = 6.52–11.82 months, Fig 3b). No significant difference of PFS was observed between the 19del and L858R groups, nor TP53 status (Fig S2a,S2b). A receiver operating characteristic curve (ROC curve) was drawn to determine the most appropriate cutoff value of T790M sensitizing mutation (sensi‐mutation) ratio for predicting third‐generation TKI progression (Fig S3). According to ROC curve, we chose ratio = 0.4 (point a in Fig S3) as the cutoff value, and categorized all these patients into two groups: ratio > 0.4 group (28 cases) and ratio < 0.4 group (14 cases). Using Kaplan‐Meier analysis, ratio > 0.4 group had a much better PFS of third‐generation TKI than ratio < 0.4 group (P = 0.018, Fig 3(c)).
Discussion
Molecular testing using high throughput NGS can provide more comprehensive genomic information for detection of resistance mechanisms and treatment outcome monitoring.13 Although the gold standard to assess genomic mutation is through the detection of tissue biopsy, tumor tissue is not always available due to the limitation of invasive procedures, insufficient sample for testing, and intratumor heterogeneity. Liquid biopsy of ctDNA has proven to be an adequate source for biomarker testing in targeted therapy. However, there are few studies reporting the clinical utility of liquid biopsy in the real world. Our study was aimed at clinical validation of liquid biopsy NGS by comparison with tissue biopsy, and also investigated clinical utility of ctDNA NGS on prediction of third‐generation TKI outcomes in a large Chinese cohort.
In our study, concordance for ctDNA and tissue biopsy was 84.62% among all stage patients, and even higher among late stage patients (88.24%), consistent with previous studies.14, 15 We also investigated the resistance mechanisms of 147 plasma from first‐generation TKI‐relapsed patients, and T790M was the most common reason for the resistance of first‐generation TKI (40.13%) (Fig 2a). Taniguchi et al. also reported that T790M occurred in 43.5% of TKI‐relapsed patients using ctDNA BEAMing.16 Our results indicated that NGS‐based platform is competent for detection of ctDNA mutations to guide the target therapy, especially when resistance to TKI occurs and no tumor tissue is available.
We found that T790M was more likely to coexist with 19del than with L858R (50% vs. 37.88%, Fig 2b). Ke et al. reported that prevalence of T790M was significantly higher in 19del than in the L858R subgroup (50.4% vs. 36.4%, P = 0.043).17 A previous in vitro and in vivo study proved that 19del/T790M cells had increased oncogenic activity compared with L858R/T790M cells.18 Therefore, we speculate that 19del cell clones may have the ability to make T790M become the dominant cell clones after TKI treatment. In the study by Babu Koyyala et al. the incidence of T790M were similar between the 19del and L858R group (55.56% vs. 53.85%)19; while Del Re et al. proved that the incidence of T790M in 19del was slightly lower than in L858R after gefitinib/erlotinib treatment (73.08% vs. 84.62%), but T790M was more likely to coexist with 19del than L858R after afatinib treatment (38.24% vs. 14.29%).20 We believe that the different technology used and different population enrolled in the studies could both influence the results. In addition, although different opinions have been reported, few of these studies had a statistically significance conclusion. Therefore further studies with a larger population are still needed to confirm the results.
In our study, the ratio of T790M sensi‐mutation in most patients was below 100%, which indicated that T790M was present in a subpopulation of EGFR sensitizing mutation cells. Interestingly, we also found that compared with those detected with both sensitizing mutations and T790M, patients only detected with sensitizing mutations had a lower MAF of sensitizing mutations (Fig 2d). We also found that T790M MAFs were significantly associated with metastasis status, and M1b patients had higher T790M MAFs than others. It should be noted that for those patients without extrapulmonary metastases, it is likely that T790M in ctDNA was too low to be detected. These findings highlight the possibility that some patients might have T790M MAF lower than the limitation of detection (LOD) and only sensitizing mutations were detected. It is a reminder that for patients harboring only sensitizing mutation with low MAF in ctDNA test, there is possibility that they can still benefit from third‐generation TKI treatment.
In survival analysis of first‐generation TKI, the median PFS was 13.73 months, consistent with the published data.21 ORR and DCR for first‐generation TKI were 54.47% and 96.27%, respectively. Although no significant influence was observed on PFS for sensitizing mutation types and TP53 status, we did find that TP53 mutation patients had a much lower ORR than TP53 wild‐type patients. A previous study also reported that TP53 missense mutations was significantly associated with DCR for first‐generation TKI,22 which also indicated the negative impact of TP53 mutation on target therapy.
In survival analysis of third‐generation TKI, the median PFS was 9.17 months. ORR and DCR for third‐generation TKI were 55.32% and 97.87%, respectively, which was consistent with the previous report.6 It should be noted that in our study, higher MAFs of both sensitizing mutation and T790M were associated with better optimal efficacy (Fig 3a). Recently, Li et al. reported that the abundance of EGFR sensitizing mutations was significantly associated with ORR to first‐generation TKIs,23 and also a Japanese study reported L858R MAF may be a potential predictive factor of TKI treatment efficacy.24 We inferred that low MAFs of both sensitizing mutations and T790M caused by the intratumor heterogeneity may contribute to resistance of TKI treatment and played a negative role in targeted treatment efficacy. Using Kaplan‐Meier analysis, we found that the high ratio of T790M/sensitizing mutation (ratio > 0.4) group benefited longer PFS of third‐generation TKI (Fig 3c). Similar results were reported by Ariyasu et al. among 33 tumor tissues from first‐generation TKI‐relapsed patients.25 Marzia Del Re et al. reported a different cutoff ratio for T790M sensi‐mutation. In their study, cfDNA was analyzed by droplet digital PCR (ddPCR), and patients with T790M sensi‐mutation >0.22 had better PFS than others.26 We believe that the different technology used in their research might be the reason for the difference between cutoff ratios. We used capture‐based NGS for cfDNA analysis, which might have a lower efficiency in capture deletions than ddPCR.27 Since there were 47.83% (22/46) patients who received osimertinib harboring 19del in our study, it is reasonable that T790M sensi‐mutation ratio was higher than the ratio in the study by Del Re et al. Thus, the cutoff ratio in our study was slightly higher than the study by Del Re et al. As we revealed that the ratio of T790M/sensitizing mutation varied in different patients because of intratumor heterogeneity, the most possible reason for the negative impact of low T790M ratio on third‐generation TKI PFS is that clones lacking T790M are likely to have other resistance mechanisms and respond poorly to third‐generation TKI treatment.
Our study was limited by a few factors. First, our work was a retrospective study and only included first‐generation TKI‐relapsed blood samples. Baseline blood samples collected before first‐generation TKI treatment may be more effective to predict first‐generation TKI outcomes. Second, the number of T790M‐positive patients received osimertinib was relatively small, and not all progressed from third‐generation TKI treatment. Future studies are still needed to confirm the results with a larger population.
In summary, our study indicated that high‐throughput NGS based platforms are competent for the detection of ctDNA mutations to guide the target therapy, especially when tissue biopsy was not available. However, it should always be noted that for those patients harboring low MAF sensitizing mutation without T790M in ctDNA NGS, it is possible that their T790M mutation is under LOD, and can still benefit from third‐generation TKI treatment. In survival analysis, TP53 mutation showed negative impact on target therapy outcomes. We also found that in third‐generation TKI treatment, both high ratio of T790M sensi‐mutations and high MAFs of EGFR mutations were associated with better outcomes of third‐generation TKI treatment. Therefore, the quantification of both MAFs and T790M sensi‐mutation ratio should be taken into consideration in some clinical situations, and incorporation of high‐throughput NGS into clinical trials may be crucial in identifying the response to osimertinib, as it provides more comprehensive genomic information, such as mutation types and the MAF.
Disclosure
No authors report any conflict of interest.
Supporting information
Figure S1 Kaplan‐Meier estimates of first‐generation TKI progression‐free survival of 147 cases. (a) Survival curves of all 147 cases; (b) survival curves according to sensitizing mutation types; and (c) survival curves according to TP53 status.
Figure S2 Kaplan‐Meier estimates of third‐generation TKI progression‐free survival of 46 patients. (a) Survival curves according to sensitizing mutation types; and (b) survival curves according to TP53 status.
Figure S3 Receiver operating characteristic (ROC) curve, point a: ratio (T790M sensitizing mutation) = 0.4.
Figure S4 The association between TP53 status and other genetic alterations. (a) TP53 status and EGFR sensitizing mutations. (b) TP53 status and other cancer‐related gene mutations detected by next‐generation sequencing (NGS).
Acknowledgments
This work was supported by grants of National Natural Science Foundation of China (NSFC No. 81802294), the CAMS Innovation Fund for Medical Sciences (2017‐I2M‐2‐003), and Beijing Hope Run Special Fund of Cancer Foundation of China (LC2017B08).
Contributor Information
Ying Jianming, Email: jmying@cicams.ac.cn.
Jie He, Email: hejie@cicams.ac.cn.
References
- 1. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin 2018; 68 (1): 7–30. [DOI] [PubMed] [Google Scholar]
- 2. Lynch TJ, Bell DW, Sordella R et al Activating mutations in the epidermal growth factor receptor underlying responsiveness of non‐small‐cell lung cancer to gefitinib. N Engl J Med 2004; 350 (21): 2129–39. [DOI] [PubMed] [Google Scholar]
- 3. O'Kane GM, Barnes TA, Leighl NB. Resistance to epidermal growth factor receptor tyrosine kinase inhibitors, T790M, and clinical trials. Curr Oncol 2018; 25 (Suppl. 1): S28–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Lin Y, Wang X, Jin H. EGFR‐TKI resistance in NSCLC patients: Mechanisms and strategies. Am J Cancer Res 2014; 4 (5): 411–35. [PMC free article] [PubMed] [Google Scholar]
- 5. Lim SM, Syn NL, Cho BC, Soo RA. Acquired resistance to EGFR targeted therapy in non‐small cell lung cancer: Mechanisms and therapeutic strategies. Cancer Treat Rev 2018; 65: 1–10. [DOI] [PubMed] [Google Scholar]
- 6. Oxnard GR, Thress KS, Alden RS et al Association between plasma genotyping and outcomes of treatment with osimertinib (AZD9291) in advanced non‐small‐cell lung cancer. J Clin Oncol 2016; 34 (28): 3375–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Diehl F, Schmidt K, Choti MA et al Circulating mutant DNA to assess tumor dynamics. Nat Med 2008; 14 (9): 985–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Volik S, Alcaide M, Morin RD, Collins C. Cell‐free DNA (cfDNA): Clinical significance and utility in cancer shaped by emerging technologies. Mol Cancer Res 2016; 14 (10): 898–908. [DOI] [PubMed] [Google Scholar]
- 9. Luo J, Shen L, Zheng D. Diagnostic value of circulating free DNA for the detection of EGFR mutation status in NSCLC: A systematic review and meta‐analysis. Sci Rep 2014; 4: 6269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Diaz LA Jr, Bardelli A. Liquid biopsies: Genotyping circulating tumor DNA. J Clin Oncol 2014; 32 (6): 579–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Li Y, Zhang T, Zhang J et al Response to crizotinib in advanced ALK‐rearranged non‐small cell lung cancers with different ALK‐fusion variants. Lung Cancer 2018; 118: 128–33. [DOI] [PubMed] [Google Scholar]
- 12. Eisenhauer EA, Therasse P, Bogaerts J et al New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 2009; 45 (2): 228–47. [DOI] [PubMed] [Google Scholar]
- 13. Gagan J, Van Allen EM. Next‐generation sequencing to guide cancer therapy. Genome Med 2015; 7 (1): 80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Odegaard JI, Vincent JJ, Mortimer S et al Validation of a plasma‐based comprehensive cancer genotyping assay utilizing orthogonal tissue‐ and plasma‐based methodologies. Clin Cancer Res 2018; 24 (15): 3539–49. [DOI] [PubMed] [Google Scholar]
- 15. Thompson JC, Yee SS, Troxel AB et al Detection of therapeutically targetable driver and resistance mutations in lung cancer patients by next‐generation sequencing of cell‐free circulating tumor DNA. Clin Cancer Res 2016; 22 (23): 5772–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Taniguchi K, Uchida J, Nishino K et al Quantitative detection of EGFR mutations in circulating tumor DNA derived from lung adenocarcinomas. Clin Cancer Res 2011; 17 (24): 7808–15. [DOI] [PubMed] [Google Scholar]
- 17. Ke EE, Zhou Q, Zhang QY et al A higher proportion of the EGFR T790M mutation may contribute to the better survival of patients with exon 19 deletions compared with those with L858R. J Thorac Oncol 2017; 12 (9): 1368–75. [DOI] [PubMed] [Google Scholar]
- 18. Godin‐Heymann N, Bryant I, Rivera MN et al Oncogenic activity of epidermal growth factor receptor kinase mutant alleles is enhanced by the T790M drug resistance mutation. Cancer Res 2007; 67 (15): 7319–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Babu Koyyala VP, Batra U, Jain P et al Frequency of T790M mutations after progression on epidermal growth factor receptor tyrosine kinase inhibitor in metastatic non‐small cell lung cancer in Indian patients: Real‐time data from tertiary cancer hospital. Lung India 2018; 35 (5): 390–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Del Re M, Petrini I, Mazzoni F et al Incidence of T790M in patients with NSCLC progressed to Gefitinib, Erlotinib, and Afatinib: A study on circulating cell‐free DNA. Clin Lung Cancer 2019. 10.1016/j.cllc.2019.10.003. [DOI] [PubMed] [Google Scholar]
- 21. Li W, Qiu T, Guo L. Primary and acquired EGFR T790M‐mutant NSCLC patients identified by routine mutation testing show different characteristics but may both respond to osimertinib treatment. Cancer Lett 2018; 423: 9–15. [DOI] [PubMed] [Google Scholar]
- 22. Canale M, Petracci E, Delmonte A et al Impact of TP53 mutations on outcome in EGFR‐mutated patients treated with first‐line tyrosine kinase inhibitors. Clin Cancer Res 2017; 23 (9): 2195–202. [DOI] [PubMed] [Google Scholar]
- 23. Li X, Cai W, Yang G et al Comprehensive analysis of EGFR‐mutant abundance and its effect on efficacy of EGFR TKIs in advanced NSCLC with EGFR mutations. J Thorac Oncol 2017; 12 (9): 1388–97. [DOI] [PubMed] [Google Scholar]
- 24. Ono A, Kenmotsu H, Watanabe M et al Mutant allele frequency predicts the efficacy of EGFR‐TKIs in lung adenocarcinoma harboring the L858R mutation. Ann Oncol 2014; 25 (10): 1948–53. [DOI] [PubMed] [Google Scholar]
- 25. Ariyasu R, Nishikawa S, Uchibori K et al High ratio of T790M to EGFR activating mutations correlate with the osimertinib response in non‐small‐cell lung cancer. Lung Cancer 2018; 117: 1–6. [DOI] [PubMed] [Google Scholar]
- 26. Del Re M, Bordi P, Rofi E et al The amount of activating EGFR mutations in circulating cell‐free DNA is a marker to monitor osimertinib response. Br J Cancer 2018; 119 (10): 1252–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Liu D, Zhou H, Shi D et al Quality control of next‐generation sequencing‐based in vitro diagnostic test for onco‐relevant mutations using multiplex reference materials in plasma. J Cancer 2018; 9 (9): 1680–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1 Kaplan‐Meier estimates of first‐generation TKI progression‐free survival of 147 cases. (a) Survival curves of all 147 cases; (b) survival curves according to sensitizing mutation types; and (c) survival curves according to TP53 status.
Figure S2 Kaplan‐Meier estimates of third‐generation TKI progression‐free survival of 46 patients. (a) Survival curves according to sensitizing mutation types; and (b) survival curves according to TP53 status.
Figure S3 Receiver operating characteristic (ROC) curve, point a: ratio (T790M sensitizing mutation) = 0.4.
Figure S4 The association between TP53 status and other genetic alterations. (a) TP53 status and EGFR sensitizing mutations. (b) TP53 status and other cancer‐related gene mutations detected by next‐generation sequencing (NGS).