

Abstract
Introduction: Lolland-Falster consists of two islands in the southern part of Denmark where income is lower and life expectancy is shorter than in the general Danish population. It is a mixed rural-provincial area with approximately 100,000 inhabitants. The Lolland-Falster Health Study was initiated to gain knowledge on the determinants of health in this disadvantaged area. Methods: The study is a household-based prospective cohort study including people of all ages. The entire household of randomly selected inhabitants is allocated either to an invited group or to an uninvited, non-contacted control group. The data collection encompasses questionnaires, physical examination and biological samples, i.e. blood and urine for same-day analysis and biobank storage, and saliva and faeces also for biobank storage. The civil registration number links collected data for each individual, family and household, with information in Danish registers. The data collection started in February 2016 and is estimated to end by 2019 after the enrolment of 20,000 people. Analysis: A number of in-depth sub-studies are planned. Emphasis will be given to analysis of intra- and inter-family variations in health determinants, genetics, lifestyle and health status. Ethics: Region Zealand’s Ethical Committee on Health Research (SJ-421) and the Danish Data Protection Agency (REG-24-2015) approved the study. Trial registration: Clinicaltrials.gov (NCT02482896). Strength and limitations of this study: The strength of this study is that Lolland-Falster Health Study is a useful scientific resource for investigating cross-sectional difference and time trends within and between individuals, families and households. LOFUS adds diversity to the previously collected Danish population studies in urbanized areas. The limitation is that data collection is expensive. Conclusions: LOFUS will contribute to the knowledge on health in disadvantaged, rural-provincial areas.
Keywords: Epidemiology, households, public health, cohort analysis, family health, genetics
Introduction
Denmark is a small country with 5,800,000 inhabitants [1] and a universal free healthcare system. Despite this, disparities in socioeconomic status and health-related factors according to geographical location are evident [2]. Lolland and Falster are two southern islands with a mixed rural-provincial population of 103,000 inhabitants [3]. Lolland Municipality consists of the Western part of Lolland, whereas Guldborgsund Municipality consists of the Eastern part of Lolland and Falster (Figure 1). The Lolland-Falster population is less educated [4], has a lower income [5], has more people outside the workforce [6] and, especially on Lolland, more people move out of the area than into it [7]. Average life expectancy in Denmark overall is presently 80.8 years, but only 78.5 years in Guldborgsund Municipality and 77.3 years in Lolland Municipality [8].
Figure 1.
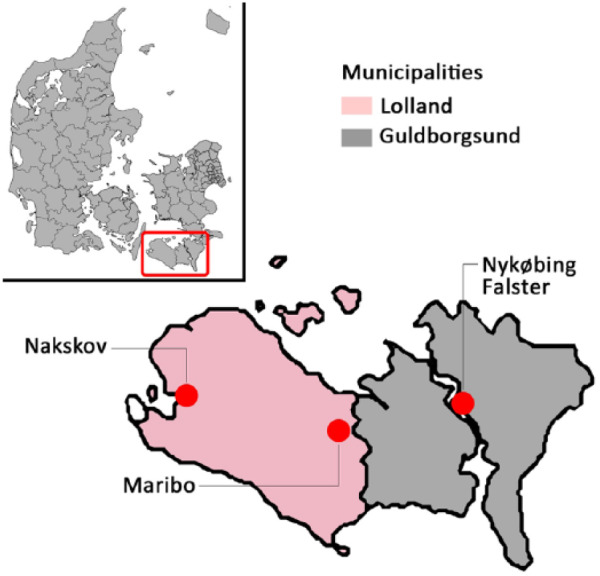
Map of Denmark with Lolland-Falster marked. Lolland Municipality in red and Guldborgsund Municipality in grey. Nakskov, Maribo and Nykøbing Falster are shown. Lolland is the island to the left and Falster is the island to the right. Lolland Municipality consists of the Western part of Lolland, whereas Guldborgsund Municipality consists of the Eastern part of Lolland and Falster.
Low socioeconomic status is associated with underlying adverse health outcomes in children as well as adults [9–14]. Correspondingly, the inhabitants of Lolland-Falster have reported a high burden of physical and mental health problems, a high prevalence of unhealthy lifestyle factors, and lack of contact with friends and family in the recently published questionnaire-based Health Profile 2017 [15]. The health and well-being of children and adults on Lolland-Falster are thus of public health concern.
This has formed the background for the Lolland-Falster Health Study (LOFUS). The study is organized as a large-scale household-based prospective cohort study with self-reported questionnaires, physical examinations, biological samples and links to Danish registries. It is the expectation that this study can form the basis for research into the causes of the disease burden of the Lolland-Falster population and inform the planning of preventive and health-promoting interventions.
Denmark has a number of ongoing population-based studies, e.g. the Danish Diet, Cancer and Health Study [16], the Copenhagen City Heart Study [17], the Danish General Suburban Population Study [18], the Copenhagen General Population Study [18], and the Danish National Birth Cohort [20]. However, it is a unique feature of LOFUS to focus in the mixed rural-provincial part of the Danish population and to include entire household members as study participants. From a public health perspective, it is important to investigate diverse populations to avoid selection bias and to enhance generalizability.
Objectives
The primary aim of LOFUS is to create a scientific resource with a research database and a biobank with the opportunity to investigate cross-sectional differences and longitudinal changes in risk factors and disease burden within and between individuals, families and households. The specific aims are to:
1) identify socioeconomic, hereditary, lifestyle, familial and environmental risk factors;
2) examine family and household patterns in poor health and salutogenic factors;
3) examine interaction between characteristics of the local community and the individual health status;
4) describe time trends in risk factors and disease burden;
5) investigate if time trends in risk factors have an effect on disease burden;
6) identify new risk factors for disease;
7) investigate interactions between risk factors; and
8) with special reference to the biobank part of LOFUS, understand the association between naturally occurring bacteria and pathogens, oxidative stress, metabolic changes and genetic and epigenetic factors in disease occurrence.
Hypothesis
The burden of diseases in the Lolland-Falster population is hypothesized to result from a combination of socioeconomic, genetic, lifestyle-related, familial and environmental factors, and the combination and weight of these factors are expected to differ from the pattern seen in previous studies of populations in the capital and larger cities of Denmark [17–19].
Methods and analysis
Study design
LOFUS is a household-based prospective cohort study including two populations: an invited group and an uninvited, non-contacted control group. The data collection for the invited group encompasses questionnaires, physical examinations and collection of biological specimens.
Population
The target population is the 42,084 inhabitants in Lolland Municipality (2017 figures) [21] and 60 979 (2017 figures) inhabitants in Guldborgsund Municipality [22]. Inhabitants of all ages and nationalities are included. Excluded are incapacitated people with guardians, individuals without a permanent residence, inhabitants with address protection and inhabitants unable to understand Danish or English. Enrolment started in February 2016 and will be ongoing until the end of 2019, then planned to reach 20,000 participants.
Invitation and booking procedures
Almost daily, and adjusted to the current staffing capacity, people aged 18 or above are randomly selected from the Danish Civil Registration System. Their entire households are then randomly allocated to either the invitation or the control group in a 2:1 ratio (Figure 2). Only people and addresses not previously invited are eligible for selection. Invitations are sent individually to each member of the invited households. It is mandatory for Danes ⩾15 years to have an electronic personal mailbox (e-box) for messages from public authorities including from the healthcare sector [14]. Therefore, LOFUS invitations are issued via the e-boxes. Inhabitants exempted from e-box and <15 years receive invitation by ordinary mail. Invited people not responding within two weeks by either email, phone, or text message are re-invited. After a minimum of another two weeks, attempts are made to reach non-responders by phone.
Figure 2.

Population, households and study sample for the Lolland-Falster Health Study. Randomly selected households are randomly allocated to either the invitation group (in grey) or the control group (in white) in a 2:1 ratio.
Invited individuals who agree to participate are booked for an appointment and receive a confirmation letter including the link and password to their web-based questionnaire. Members of a household are booked together, if they prefer. LOFUS has three stationary sites: in Nakskov, Maribo, and Nykøbing Falster (Figure 1). All sites have an undisturbed room for the dialogue concerning the written informed consent. In Nakskov and Maribo, there is another room for the health examination, whereas the facility in Nykøbing Falster has three such rooms. At booking, participants are free to decide which site to attend. If participants are unable to visit the stationary site, the staff can visit them at home using a fully equipped camper or provide a taxi.
Staff
Certified nurses and biomedical laboratory technicians obtain the written informed consent and perform the health examinations. At employment, the staff undergo a mandatory introduction programme covering standard operation procedures and ethical and communicative aspects of the work. Adherence to procedures is monitored through self-assessment and follow-up by colleagues and management.
Questionnaires
The LOFUS questionnaires are constructed from a combination of previously used items and scales and new scales developed for the purpose. Five, partially different, questionnaires are used for the age groups 0–1, 2–3, 4–10, 11–17, and ⩾18 years. Key items include self-assessed health and well-being, mental and physical health, relationships and lifestyle factors, Table I for the ⩾18 years’ questionnaire. Furthermore, some sub-studies have additional questionnaires for designated subsets of the participants. Participants are recommended to complete the questionnaire electronically at home before attending the health examination. Parents should complete the questionnaire for children ⩽10 years. If needed, the staff can help with completing the questionnaires at the health examination. Paper-based questionnaires are used only when participants cannot master the electronic version.
Table I.
Questionnaire in the Lolland-Falster Health Study for participants ⩾18 years.
| Scale/items |
| Health and well-being |
| Mental health |
| Self-care |
| Diseases |
| Pain |
| Prescription and over the counter medication |
| Diet |
| Screen/digital time |
| Physical activity |
| Transport |
| Sleep |
| Height and weight |
| Smoking |
| Pets |
| Alcohol and drugs |
| Periods, pregnancies and births |
| Family and friends |
| Life events |
| Marital status |
| Education and work status |
| Personality* |
| Contact to healthcare system* |
| Work load* |
| Ear, nose and throat problems* |
| Incontinence in women* |
| Frailty and functions* |
| Health literacy* |
Additional items triggered by response to selected items above.
Health examination
The health examination includes measurement of anthropometrics, electrocardiography, blood pressure, pulse, oxygen saturation, spirometry, hand grip strength and accelerometer-assessed physical activity. The content of the health examination varies to some extent by age group (Table II). Other examinations may be added by appointment with research collaborators.
Table II.
Health examination in the Lolland-Falster Health Study.
| Examination | Age (years) | Equipment |
|---|---|---|
| Arm blood pressure | ⩾4 | Welch Allyn Connex Pro BPO 3400 Electronic blood pressure devise |
| Ankle blood pressure* | ⩾50 | Welch Allyn Connex Pro BPO 3400 Electronic blood pressure devise and EDAN SD3 Vitrosonic Pocket Doppler 8 MHz probe |
| Electrocardiogram | All | GE Healthcare ECG device MAC 5500 HD |
| Height | All | SECA 216 Wall-mounted height measure |
| Weight | All | Tanita Body Composition Analyzer BC-420MA III or Electronic scale Tanita WB 150 SMA |
| Waist and hip circumference | All | Tape measure |
| Head circumference | <4 | SECA 212 Measuring tape |
| Lung function (spirometry) | ⩾7 | MicroLabTM and MicroLoopTM Handheld Spirometer with PC Software |
| Peripheral oxygen saturation | All | NellcorTM Portable SpO2 Patient Monitoring System, PM10N |
| Pulse | All | NellcorTM Portable SpO2 Patient Monitoring System, PM10N |
| Bioimpedance | ⩾18 | Tanita Body Composition Analyzer BC-420MA III |
| Hand-grip strength | ⩾50 | Seahan digital hand dynamometer |
| Electronic accelerometer measurement** | Families with child/children <18 | Axivity AX3 2 × accelerometer |
Collected 2016 and 2017.
Collected 2017 and 2018.
Staff collaborate with parents to create a supportive environment for children to comply with the health examination, e.g. confidence is built through play where young children pretend to assist the staff with measuring older siblings or parents.
Biological sample collection, analyses and storage conditions
The biological specimens include blood, urine, saliva and faeces (Table III). Capillary blood is collected from all participants and whole blood from participants ⩾15 years. Urine, saliva and faeces are collected from a subset of participants (Table III). Whole blood samples (38 ml) are drawn in the non-fasting state between 8:40 a.m. and 6:30 p.m. in vacutainer blood collection tubes (Becton, Dickinson and Company; Franklin Lakes, NJ, USA). The 12 ml blood and 4 ml urine samples for same-day biochemical analyses are kept at 21ºC (±4ºC) until delivery at 8:00 p.m. for immediate analysis at the Department of Clinical Biochemistry (Nykøbing Falster Hospital) (Table III). The Departments of Clinical Biochemistry at Nykøbing Falster and Næstved Hospitals (40 km north of Nykøbing Falster) are accredited by the standard ISO 15189, and the Region Zealand Biobank is hosted in Næstved. Assays are followed up daily for precision and several times yearly for accuracy with a Scandinavian quality-control programme.
Table III.
Sample preservative, volume and measurements.
| Type of sample | Age, years | Volume collected (ml) | Measurements | Type of analyzer |
|---|---|---|---|---|
| Natrium-citrate | ⩾15 | 4.5 | INR | STA-R (Stago) |
| Lithium-Heparin (PST) | ⩾15 | 3.5 | Chemistry* | Siemens Dimension Vista 1500 |
| Clot activator (SST) | ⩾15 | 6.0 | Biobank-serum | − |
| EDTA | ⩾15 | 2*10 | Biobank plasma and buffy coat | − |
| EDTA | ⩾15 | 2.0 | Haematology** | Sysmex XE-5000 |
| EDTA | ⩾15 | 2.0 | HbA1C | TOSOH-G8 |
| Finger stick | Any age | − | Plasma Glucose | Bayer Contour XT |
| Urine | ⩾15 | 4 | Albumin/creatinine ratio | Siemens Dimension Vista 1500 |
| Urine*** | ⩾7 | 2*4 | Biobank | − |
| Saliva*** | ⩾11 | 3*1.8 | Biobank | − |
| Faeces*** | Any age | 3*2-10 | Biobank | − |
PST: plasma separation tube; SST: serum separation tube; EDTA: ethylene diamine tetra-acetate; HbAlC: glycated haemoglobin A1c.
Chemistry: iron, transferrin, ferritin, free triiodothyronine (fT3), free thyroxine (fT4), thyroid stimulating hormone (TSH), sodium, potassium, alkaline phosphate, alanine amino transferase, bilirubin, creatinine, total cholesterol, low-density lipoprotein cholesterol (calculated), high-density lipoprotein cholesterol, triglyceride, albumin, high-sensitivity C-reactive-protein (hsCRP), eGFR (calculated).
Haematology: WBC, white blood cell; BASO, basophil; IG, immature granulocyte; NRBC, nucleated red blood cell; RET, reticulocyte; Ret-He, reticulocyte haemoglobin content; IRF/LRF/MRF/HRF immature, low, medium and high reticulocyte fraction; PLT, platelet (volume fraction); IPF, immature platelet fraction; PCT, platelet volume fraction; PDW, platelet volume difference (max-min); RBC, red blood cell; HGB, haemoglobin; HCT, haematocrit; MCV, mean corpuscular volume; MCHC, mean corpuscular haemoglobin concentration; RDW, red blood cell distribution; MPV, mean platelet volume; NEUT, neutrophil; LYMPH, lymphocyte; MONO, monocyte; EO, eosinophil.
Samples collected 2016 and 2017.
The 2 × 10 ml whole blood ethylene diamine tetra-acetate (EDTA) and 6 ml serum for biobank storage are spun and stored at 4ºC (±2ºC) overnight; transported refrigerated (4ºC ± 2ºC) to the biobank on the next morning; centrifuged; and aliquoted into 5 × 270 µl serum, 2 × 865 µl buffy coat, and 10 × 270 µl plasma using an automated system; and finally stored at −80ºC. Participants eligible for saliva collection should not have been eating, drinking, smoking, or using an inhalator or chewing gum for at least 60 minutes prior to collection. Saliva is collected after a maximum of 5 minutes of gum base stimulation. Urine (2 × 4 ml) and saliva (3 × 1.8 ml) for biobank storage are aliquoted into cryotubes and kept on dry ice immediately after collection and during transport until storage at −80ºC the same evening. Participants agreeing to contribute three tubes of faeces are instructed in the home procedure using a specialised toilet-insert to collect the faeces without contamination, and to keep the sealed samples in their own freezer until LOFUS staff pick it up later; the faecal samples are transported on dry ice and stored at −80ºC.
A full health examination including collection of and instruction for biological samples lasts on average 30 minutes per child <15 years old, 50 minutes per person 15–50 years and 75 minutes per adult ⩾50 years.
Biobanks
Blood samples are stored in the Region Zealand Biobank. Specimens of urine, saliva and faeces are stored at the biobank of the Novo Nordisk Foundation Center for Basic Metabolic Research, University of Copenhagen, and additional urine samples are stored at the Department of Pharmacology, Rigshospitalet.
Database
The LOFUS database uses MS SQL Server as the back-end data-storage, whereas the front-end user-interface is developed in MS Access. For proper protection of the participant-related data, the Access file contains no data. The database is used for both data storage and administrative management of the project, and it is stored on statutory logged drives. Only authorized personnel have access and all activity is logged. Completeness and correctness of datasets are controlled regularly.
Danish registries
In Denmark, all individuals are designated a unique civil registration number at birth by the Danish Civil Registration System (CRS) [23]. The number is used throughout life for healthcare, education, tax and employment purposes. The CRS also includes the name, gender, date of birth, place of birth, vital status (dead/alive), citizenship, identity of parents, spouses and place of residence. The CRS was initiated in 1968 and is continuously updated [23]. The CRS is also linked to other registries, such as The Danish National Patient Register with information since 1977 [24], The Danish Cancer Registry with information since 1943 [25], and the Danish National Prescription Registry with information since 1994 [26]. In LOFUS, individuals in both the invited and the control group are identified by their unique civil registration number, which allows linkage to and follow-up in Danish registers.
Return of results
Abnormal findings at the health examination, e.g. severely low or high glucose level or severely abnormal electrocardiogram (ECG), are conferred immediately with the attending physician at the local hospital, who determines if hospitalization is needed or if the LOFUS participants should be recommended to contact their general practitioner (GP).
No later than 2 weeks after the health examination, the participants receive a letter with selected results of the health examination, e.g. blood pressure, lung function, haemoglobin and glycated haemoglobin A1c. Biochemical and physical measurements distinctly deviating from the reference range and elevated scores on the Major Depression Inventory [27] or the Anxiety Symptom Scale (Danish: Angst-Symptom-Spørgeskemaet) [28] trigger a recommendation for participants to consult their GP. For children, the content of the letter relies on the actual examinations they underwent, but height, weight and blood sugar are always included. All participants can check the full outcome of the biochemical analyses on their electronic health records on Sundhed.dk [29].
‘Grey-zone’ ECGs are assessed by a cardiologist within a few days. If follow up is recommended, the participant is contacted and receives a copy of the ECG print, which is also sent to their GP. In addition, excess values on other biochemical measurements and/or burden of psychotic experiences are assessed individually.
Data analysis plan
The overall purpose of LOFUS is to identify associations between socioeconomic, genetic, lifestyle-related, familial and environmental factors and health. Currently, more than 15 sub-studies have been identified with specific analysis plans within genetics, microbiome, toxicology, internal medicine, gynaecology, geriatrics, physical activity, psychiatry, sociology and psychology. In addition, several other articles are planned. First, with use of Danish registries we will make a cross-sectional comparison of participating people with invited non-participants to investigate participation bias. Second, we will investigate the proportion of participants referred to the hospital or their GP in need of treatment for newly detected diseases or with treatment failure of prevalent diseases. Third, associations between reported lifestyle factors, or biochemical markers and health status will be searched for in the baseline data for participants. Fourth, participants, invited non-participants and the control group will be followed up in the national registers to identify associations between baseline characteristics and disease occurrence. A special emphasis will be given to identification of family clustered health problems and statistical tools for these analyses will be developed.
Governance
A steering committee of researchers and administrators is responsible for the strategic, economic and operational decisions concerning the project. Members of the Danish scientific community assess protocols for sub-studies before approval by the steering committee. Sub-studies must adhere to the rules and regulations on research ethics and data protection. The LOFUS staff is employed at the Nykøbing Falster Hospital.
Ethics and dissemination
Region Zealand’s Ethical Committee on Health Research approved the study (SJ-421). The Danish Data Protection Agency approved the study (REG-24-2015). The study is registered in Clinical Trials (NCT02482896).
LOFUS uses two written consent forms: one for participants aged 0–14 years to be signed by the holders of custody and one for participants aged ⩾15 years. Both forms include a range of items that should be considered separately, e.g. storage of biological samples, genetic mapping and linkage to health registers and medical records. It is thus possible to opt in or out of selected parts.
Datasets for sub-studies are extracted without the civil registration numbers. If pseudo identification numbers are used, the link between these and the civil registration numbers is kept in a separate file. The LOFUS data will be deposited in the Danish Data Achieve after the data collection. Access to data will follow the rules of the archive [30].
Results will be published in peer-reviewed, international and preferably open-access journals, listing authors according to authorship guidelines. Positive, negative and inconclusive results will be published.
Discussion
The last 25 years of segregation in Denmark has resulted in employed people moving away from Lolland-Falster, and at the same time, unemployed people or people outside the labour market moving in [7]. This segregation forms a challenge for the health status in Lolland-Falster in two ways. First, some of the newcomers are out of work for health reasons. Second, the decline in taxable income limits the possibilities for investments in preventive and health-promoting activities, such as better schools and daycare. In addition, Lolland-Falster faces challenges in recruiting medical doctors and other health professionals for both the primary and the secondary sector.
LOFUS was initiated to provide insight into the association between socioeconomic, genetic, lifestyle-related, familial and environmental factors and health in this disadvantaged area. The unique civil registration number [23] links collected data for each participating individual, family and household, with information in Danish registers on vital status, socioeconomic status, diagnoses and use of healthcare. The broad range of collected data allows for linkage of, for instance, socioeconomic status, lifestyle and health status with microbiome data [31,32]. A number of sub-studies already planned at the initiation of LOFUS are expected to provide new insights, e.g. Early ageing – social causes behind frailty and loss of function; Psychiatric problems among children and young people; Personality, subjective well-being and health; Prevalence of metabolic syndrome in Lolland-Falster; Family function, cognitive function and health competences as determinants for mental and physical health. The project is open for other collaborators upon request. We expect the range of sub-studies to increase over the years.
Strengths and limitations
LOFUS is the only prospective cohort study of the rural population in Denmark. LOFUS is a useful scientific resource for investigating cross-sectional differences and time trends within and between individuals, families and households in all age groups. LOFUS adds diversity to the previously collected Danish general population studies, which have been collected in Copenhagen or other urbanized areas.
The extensive, and partly health-related, population movements [7] in and out of Lolland-Falster complicates identification of causal relationships between health determinants and health. Both baseline and follow-up data will be influenced by the selection bias. Therefore, it is a strength that place of residence and employment history of the LOFUS participants can be retrieved from the Danish registers even before they were recruited to LOFUS.
The invitation procedure for LOFUS using a random selection of households via an index person ⩾18 years causes an overrepresentation of households with more than one person. However, sampling of households on a continuous basis was considered impossible. By linking to population registers, it will be possible to compare the constitution of participants with the non-participants, the uninvited control group and the entire Lolland-Falster population. As in other population studies, it is expected that non-participants will have lower socioeconomic status, more illnesses and lower mean survival than participants [33,34].
To limit expenses and the duration of the health examination, the original protocol was modified such that measurement of ankle blood pressure and collection of faeces, saliva and urine samples for biobank storage were only performed from February 2016 to the end of 2017. Accelerometer-assessed physical activity was restricted to 2017 and 2018.
Perspectives
Previous population-based health studies in Denmark have primarily focused on urbanized populations. This is the case for the Diet, Cancer and Health study recruiting participants from Copenhagen and Aarhus [16], the Copenhagen City Heart Study [17] and the Copenhagen General Population Study [19]. To make research findings generalizable for the general public and use the results in public-health planning and precision medicine, these studies do not only need to be large, but also represent the underlying diversity in the population. LOFUS is an important addition as it focuses on a rural-provincial area with socioeconomic and health challenges. LOFUS forms the first possibility to learn about determinants of health in the disadvantaged areas of Denmark and will contribute to the international knowledge on health in rural-provincial areas. Comparison across Danish health studies can inform local and national politics.
The Copenhagen General Population Study [19], the Danish General Suburban Population Study [18] and LOFUS include similar datasets. Therefore, it will be possible to correlate the profiles of their measures and compare the morbidity and mortality of these respective populations. A previous comparison between the Copenhagen General Population Study and the Danish General Suburban Population Study showed that whereas 16% of the participants in the Copenhagen study were obese, this applies to 21% in the suburban population [18]. With its higher mortality, the LOFUS population will add an extra dimension to these comparisons. Suggestions for predicting overall mortality based on data similar to those collected to these three Danish population studies have previously been reported based on United States data, e.g. the enhanced Intermountain Mortality Risk Score [35] and the Health Status Metric [36]. We plan to apply these United States suggestions to the Danish data.
Acknowledgments
The authors would like to thank the inhabitants of Lolland-Falster and the LOFUS staff for their commitment to the study. Thank you to Sara Lethan Abild for the layout of the figures and to Elsebeth Lynge for inspiration, critical reading and comments.
Footnotes
Author contributions: Knud Rasmussen and Christina Ellervik initiated the Lolland-Falster Health Study. Randi Jepsen is the project manager of the study. All other authors have contributed to the design and facilitation of the study. Randi Jepsen drafted the paper. All authors revised the present paper and have agreed on the final version.
Declaration of conflicting interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Region Zealand, Nykøbing Falster Hospital, Guldborgsund Municipality and Lolland Municipality.
ORCID iD: Randi Jepsen  https://orcid.org/0000-0003-0934-9850
https://orcid.org/0000-0003-0934-9850
References
- [1]. Statistics Denmark. The whole country [in Danish], https://www.statistikbanken.dk/statbank5a/default.asp?w=1366 → Befolkning og valg → Folketal → FOLK1A → 2017K4, Hele landet: 2018 (accessed 11 January 2018). [Google Scholar]
- [2]. Brønnum-Hansen H, Baadsgaard M. Widening social inequality in life expectancy in Denmark. A register-based study on social composition and mortality trends for the Danish population. BMC Public Health 2012;12:994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3]. Statistics Denmark. Lolland and Guldborgsund municipalities [in Danish], https://www.statistikbanken.dk/statbank5a/default.asp?w=1366 → Befolkning og valg → Folketal → FOLK1A → 2017K4, Lolland og Guldborgsund: 2018 (accessed 11 January 2018). [Google Scholar]
- [4]. Sabiers SE, Larsen HB. Residence of the social classes in 2012 [in Danish]. Copenhagen: Arbejderbevægelsens Erhvervsråd, 2014. [Google Scholar]
- [5]. Statistics Denmark. Income in the whole country, Lolland, and Guldborgsund [in Danish], https://www.statistikbanken.dk/statbank5a/default.asp?w=1366 → Arbejde, indkomst og formue → Person- og familieindkomster → INDKP101 → 2016, Hele landet, Lolland og Guldborgsund Kommune: 2018. (accessed 11 January 2018). [Google Scholar]
- [6]. Bjørsted E, Mølgaard A. More than one third are on social benefits in some municipalities [in Danish]. Copenhagen: : Arbejderbevægelsens Erhvervsråd, 2013. [Google Scholar]
- [7]. Juul JS, Blicher SP. Exit of successful inhabitants from and entry of vulnerable newcomers to Lolland [in Danish]. Copenhagen: Arbejderbevægelsens Erhvervsråd, 2016. [Google Scholar]
- [8]. Statistics Denmark. Life expectancy in Denmark [in Danish], https://www.statistikbanken.dk/statbank5a/default.asp?w=1366 → Befolkning og valg → Dødsfald og Middellevetid → HISB77 → 2015:2016, Hele landet: 2018. (accessed 11 January 2018). [Google Scholar]
- [9]. Bjelland I, Krokstad S, Mykletun A, et al. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc Sci Med 2008;66:1334–45. [DOI] [PubMed] [Google Scholar]
- [10]. Reiss F. Socioeconomic inequalities and mental health problems in children and adolescents: a systematic review. Soc Sci Med 2013;90:24–31. [DOI] [PubMed] [Google Scholar]
- [11]. Molarius A, Berglund K, Eriksson C, et al. Mental health symptoms in relation to socio-economic conditions and lifestyle factors: A population-based study in Sweden. BMC Public Health 2009;9:302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12]. Gershon AS, Dolmage TE, Stephenson A, et al. Chronic obstructive pulmonary disease and socioeconomic status: A systematic review. COPD 2012;9:216–26. [DOI] [PubMed] [Google Scholar]
- [13]. Stringhini S, Carmeli C, Jokela M, et al. Socioeconomic status and the 25 x 25 risk factors as determinants of premature mortality: A multicohort study and meta-analysis of 1.7 million men and women. Lancet 2017;389:1229–37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14]. Iguacel I, Fernandez-Alvira JM, Bammann K, et al. Social vulnerability as a predictor of physical activity and screen time in European children. Int J Public Health 2018;63:283–95. [DOI] [PubMed] [Google Scholar]
- [15]. Blaakilde AL, Hansen BH, Olesen LS, et al. Health Profile 2017 for Region Zealand and municipalities - “How are you?”[in Danish]. Sorø, Danmark: Region Zealand, 2018. [Google Scholar]
- [16]. Tjønneland A, Olsen A, Boll K, et al. Study design, exposure variables, and socioeconomic determinants of participation in Diet, Cancer and Health: a population-based prospective cohort study of 57,053 men and women in Denmark. Scand J Public Health 2007;35:432–41. [DOI] [PubMed] [Google Scholar]
- [17]. Aguib Y, Al Suwaidi J. The Copenhagen City Heart Study (Østerbroundersøgelsen). Glob Cardiol Sci Pract 2015;2015:33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18]. Bergholdt HK, Bathum L, Kvetny J, et al. Study design, participation and characteristics of the Danish General Suburban Population Study. Dan Med J 2013;60:A4693. [PubMed] [Google Scholar]
- [19]. Naslund-Koch C, Nordestgaard BG, Bojesen SE. Common breast cancer risk alleles and risk assessment: A study on 35,441 individuals from the Danish general population. Ann Oncol 2017;28:175–81. [DOI] [PubMed] [Google Scholar]
- [20]. Olsen J, Melbye M, Olsen SF, et al. The Danish National Birth Cohort: Its background, structure and aim. Scand J Public Health 2001;29:300–7. [DOI] [PubMed] [Google Scholar]
- [21]. Statistics Denmark. Lolland Municipality [in Danish], https://www.statistikbanken.dk/statbank5a/default.asp?w=1366 → Befolkning og valg → Folketal → FOLK1A → 2017K4, Lolland Kommune: 2018. (accessed 11 January 2018). [Google Scholar]
- [22]. Statistics Denmark. Guldborgsund Municipality [in Danish], https://www.statistikbanken.dk/statbank5a/default.asp?w=1366 → Befolkning og valg → Folketal → FOLK1A → 2017K4, Guldborgsund Kommune: 2018. (accessed 11 January 2018). [Google Scholar]
- [23]. Pedersen CB. The Danish Civil Registration System. Scand J Public Health 2011;39:22–5. [DOI] [PubMed] [Google Scholar]
- [24]. Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health 2011;39:30–3. [DOI] [PubMed] [Google Scholar]
- [25]. Gjerstorff ML. The Danish Cancer Registry. Scand J Public Health 2011;39:42–5. [DOI] [PubMed] [Google Scholar]
- [26]. Kildemoes HW, Sørensen HT, Hallas J. The Danish National Prescription Registry. Scand J Public Health 2011;39:38–41. [DOI] [PubMed] [Google Scholar]
- [27]. Nielsen MG, ørnbøl E, Bech P, et al. The criterion validity of the web-based Major Depression Inventory when used on clinical suspicion of depression in primary care. Clin Epidemiol 2017;9:355–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28]. Gerlach J. (ed). The anxiety book. The symptoms, causes and treatment of anxiety [in Danish]. Copenhagen: PsykiatriFondens Forlag, 2008, p.304. [Google Scholar]
- [29]. Sundhed.dk. eHealth in Denmark, https://www.sundhed.dk/borger/service/om-sundheddk/ehealth-in-denmark/ (accessed 12 February 2018).
- [30]. Statistics Denmark. Statistical legislation, https://www.dst.dk/en/OmDS/lovgivning (accessed 22 January 2018).
- [31]. Pedersen HK, Gudmundsdottir V, Nielsen HB, et al. Human gut microbes impact host serum metabolome and insulin sensitivity. Nature 2016;535:376–81. [DOI] [PubMed] [Google Scholar]
- [32]. Allin KH, Nielsen T, Pedersen O. Mechanisms in endocrinology: Gut microbiota in patients with type 2 diabetes mellitus. Eur J Endocrinol 2015;172:R167–77. [DOI] [PubMed] [Google Scholar]
- [33]. Langhammer A, Krokstad S, Romundstad P, et al. The HUNT study: participation is associated with survival and depends on socioeconomic status, diseases and symptoms. BMC Med Res Methodol 2012;12:143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34]. Knudsen AK, Hotopf M, Skogen JC, et al. The health status of nonparticipants in a population-based health study: the Hordaland Health Study. Am J Epidemiol 2010;172:1306–14. [DOI] [PubMed] [Google Scholar]
- [35]. May HT, Anderson JL, Muhlestein JB, et al. Improvement in the predictive ability of the Intermountain Mortality Risk Score by adding routinely collected laboratory tests such as albumin, bilirubin, and white cell differential count. Clin Chem Lab Med 2016;54:1619–28. [DOI] [PubMed] [Google Scholar]
- [36]. Bello GA, Dumancas GG, Gennings C. Development and validation of a clinical risk-assessment tool predictive of all-cause mortality. Bioinform Biol Insights 2015;9:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]