

Short abstract
LINKED CONTENT
This article is linked to Al‐Ani et al and Garg et al papers. To view these articles, visit https://doi.org/10.1111/apt.15779 and https://doi.org/10.1111/apt.15796.
The excellent review by Al‐Ani et al reflects a consensus approach to management of inflammatory bowel disease during the SARS‐CoV‐2 pandemic that has been established remarkably rapidly by very effective international collaboration. 1 Much of the focus has appropriately been on the potential impact of immuno‐modulating therapies. We would also like to highlight the potential importance of nutrition and particularly vitamin D as raised by Panarese and Shahini. 2
There are marked variations in mortality from COVID‐19 between different countries. It is becoming clear that countries in the Southern Hemisphere are seeing a relatively low mortality (Figure 1 and Table 1). 2 , 3 It could be argued that the virus spread later to the Southern Hemisphere and that countries there are simply behind those in the Northern Hemisphere but as time goes by this argument looks increasingly weak. In Australia, 100 cases were reported by 10th March, 1000 by 21st March; in the UK, the first 100 had been reported by 5th March and the first 1000 by 14th March, just 1 week earlier. If one compares the mortality (68 per million) in the UK by 3rd April with the mortality (2 per million) in Australia by 10th April, there is still a huge discrepancy.
FIGURE 1.
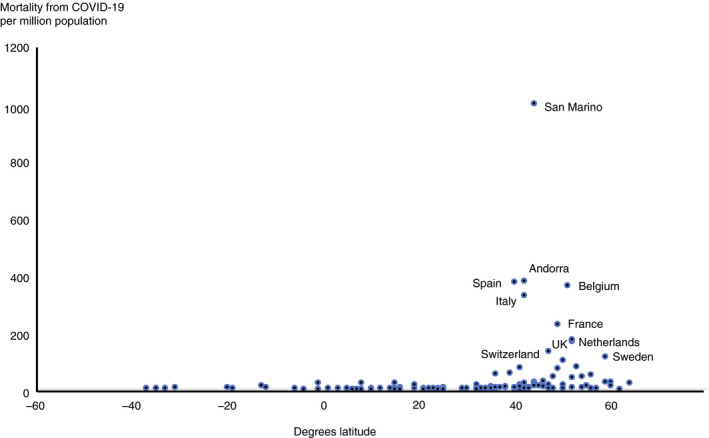
Correlation between mortality from COVID‐19 per million by country and latitude. All countries with >150 cases included. Data are from https://www.worldometers.info/coronavirus/ 3 accessed 15th April 2020. Latitude is for capital city. It can be seen that mortality is relatively low at latitudes less than 35 degrees North, the point below which adequate sunlight is likely to have been received to maintain vitamin D levels during the winter. Correlation between mortality and latitude r = 0.53, P < 0.0001 by Spearman's rank correlation
TABLE 1.
Comparison between latitude (of capital city in each country) and mortality from COVID‐19 per million population—as per Panarese et al, 2 with further analysis and updated 15th April 2020 from https://www.worldometers.info/coronavirus/ 3
| Countries | Latitude degrees | Total cases (N) | Total deaths (N) | Deaths/Million population |
|---|---|---|---|---|
| Iceland | 64 | 1720 | 8 | 23 |
| Faeroe | 62 | 184 | 0 | 0 |
| Norway | 60 | 6740 | 145 | 27 |
| Finland | 60 | 3237 | 64 | 12 |
| Sweden | 59 | 11 927 | 1203 | 119 |
| Estonia | 59 | 1400 | 35 | 26 |
| Latvia | 57 | 666 | 5 | 3 |
| Russia | 56 | 24 490 | 198 | 1 |
| Denmark | 56 | 6681 | 309 | 53 |
| Lithuania | 55 | 1091 | 29 | 11 |
| Belarus | 54 | 3728 | 36 | 4 |
| Isle of Man | 54 | 256 | 4 | 47 |
| Ireland | 53 | 11 479 | 406 | 82 |
| Germany | 52 | 132 321 | 3502 | 42 |
| UK | 52 | 93 873 | 12 107 | 178 |
| Netherlands | 52 | 28 153 | 3134 | 183 |
| Poland | 52 | 7408 | 268 | 7 |
| Belgium | 51 | 33 573 | 4440 | 383 |
| Czechia | 50 | 6151 | 163 | 15 |
| Luxembourg | 50 | 3307 | 67 | 107 |
| Ukraine | 50 | 3764 | 108 | 2 |
| France | 49 | 143 303 | 15 729 | 241 |
| Channel Islands | 49 | 445 | 13 | 75 |
| Austria | 48 | 14 321 | 393 | 44 |
| Slovakia | 48 | 863 | 6 | 1 |
| Switzerland | 47 | 26 336 | 1221 | 141 |
| Moldova | 47 | 1934 | 43 | 11 |
| Hungary | 47 | 1579 | 134 | 14 |
| Kazakhstan | 47 | 1290 | 16 | 0.9 |
| Croatia | 46 | 1741 | 34 | 8 |
| Slovenia | 46 | 1248 | 61 | 29 |
| Serbia | 45 | 4873 | 99 | 11 |
| Canada | 44 | 27 063 | 903 | 24 |
| Romania | 44 | 7216 | 362 | 19 |
| Bosnia and Herzegovina | 44 | 1110 | 41 | 12 |
| San Marino | 44 | 372 | 36 | 1061 |
| Bulgaria | 43 | 735 | 36 | 5 |
| Kyrgyzstan | 43 | 449 | 5 | 0.8 |
| Italy | 42 | 162 488 | 21 067 | 348 |
| North Macedonia | 42 | 974 | 45 | 22 |
| Andorra | 42 | 659 | 31 | 401 |
| Montenegro | 42 | 288 | 4 | 6 |
| Georgia | 42 | 306 | 3 | 0.8 |
| USA | 41 | 614 246 | 26 064 | 79 |
| Turkey | 41 | 65 111 | 1403 | 17 |
| Uzbekistan | 41 | 1275 | 4 | 0.1 |
| Albania | 41 | 494 | 25 | 9 |
| Spain | 40 | 177 633 | 18 579 | 397 |
| China | 40 | 82 295 | 3342 | 2 |
| Azerbaijan | 40 | 1253 | 13 | 1 |
| Armenia | 40 | 1111 | 17 | 6 |
| Portugal | 39 | 18 091 | 599 | 59 |
| S. Korea | 38 | 10 591 | 225 | 4 |
| Greece | 38 | 2170 | 101 | 10 |
| Algeria | 37 | 2070 | 326 | 7 |
| Iran | 36 | 76 389 | 4777 | 57 |
| Japan | 36 | 8100 | 146 | 1 |
| Malta | 36 | 399 | 3 | 7 |
| Cyprus | 35 | 695 | 12 | 10 |
| Afghanistan | 35 | 784 | 25 | 0.6 |
| Pakistan | 34 | 5988 | 107 | 0.5 |
| Tunisia | 34 | 747 | 34 | 3 |
| Lebanon | 34 | 658 | 21 | 3 |
| Iraq | 33 | 1400 | 78 | 2 |
| Israel | 32 | 12 200 | 126 | 15 |
| Morocco | 32 | 1988 | 127 | 3 |
| Jordan | 32 | 397 | 7 | 0.7 |
| Palestine | 32 | 308 | 2 | 0.4 |
| Egypt | 30 | 2350 | 178 | 2 |
| India | 29 | 11 555 | 396 | 0.3 |
| Kuwait | 29 | 1405 | 3 | 0.7 |
| Saudi Arabia | 25 | 5862 | 79 | 2 |
| Qatar | 25 | 3711 | 7 | 2 |
| Bahrain | 25 | 1671 | 7 | 4 |
| Taiwan | 25 | 395 | 6 | 0.3 |
| UAE | 24 | 4933 | 28 | 3 |
| Bangladesh | 24 | 1231 | 50 | 0.3 |
| Cuba | 23 | 766 | 21 | 2 |
| Hong Kong | 22 | 1017 | 4 | 0.5 |
| Oman | 21 | 910 | 4 | 0.8 |
| Reunion | 21 | 391 | 0 | 0 |
| Vietnam | 21 | 297 | 0 | 0 |
| Mexico | 19 | 5399 | 406 | 3 |
| Dominican Republic | 19 | 3286 | 183 | 17 |
| Brazil | 16 | 25 758 | 1557 | 7 |
| Guatemala | 16 | 180 | 5 | 0.3 |
| Philippines | 15 | 5453 | 349 | 3 |
| Senegal | 15 | 314 | 2 | 0.1 |
| Martinique | 15 | 158 | 8 | 21 |
| Thailand | 14 | 2643 | 43 | 0.6 |
| Niger | 14 | 570 | 14 | 0.6 |
| Honduras | 14 | 419 | 31 | 3 |
| Burkina Faso | 12 | 528 | 30 | 1 |
| Djibouti | 12 | 363 | 2 | 2 |
| Costa Rica | 10 | 618 | 3 | 0.6 |
| Guinea | 10 | 404 | 1 | 0.1 |
| Venezuela | 10 | 197 | 9 | 0.3 |
| Panama | 8 | 3574 | 95 | 22 |
| Ivory Coast | 8 | 638 | 6 | 0.2 |
| Nigeria | 7 | 373 | 11 | 0.05 |
| Sri Lanka | 7 | 235 | 7 | 0.3 |
| Ghana | 6 | 636 | 8 | 0.3 |
| Colombia | 5 | 2979 | 127 | 2 |
| Cameroon | 5 | 848 | 17 | 0.6 |
| Malaysia | 3 | 5072 | 83 | 3 |
| Singapore | 1 | 3252 | 10 | 2 |
| Ecuador | −1 | 7603 | 369 | 21 |
| Kenya | −1 | 225 | 10 | 0.2 |
| DRC | −4 | 241 | 20 | 0.2 |
| Indonesia | −6 | 5136 | 469 | 2 |
| Peru | −12 | 10 303 | 230 | 7 |
| Mayotte | −13 | 217 | 3 | 11 |
| Bolivia | −19 | 397 | 28 | 2 |
| Mauritius | −20 | 324 | 9 | 7 |
| Chile | −31 | 7917 | 92 | 5 |
| South Africa | −33 | 2415 | 27 | 0.5 |
| Australia | −35 | 6447 | 63 | 2 |
| Argentina | −35 | 2443 | 108 | 2 |
| Uruguay | −35 | 492 | 8 | 2 |
| New Zealand | −37 | 1386 | 9 | 2 |
This article is being made freely available through PubMed Central as part of the COVID-19 public health emergency response. It can be used for unrestricted research re-use and analysis in any form or by any means with acknowledgement of the original source, for the duration of the public health emergency.
When mortality per million is plotted against latitude, it can be seen that all countries that lie below 35 degrees North have relatively low mortality. Thirty‐five degrees North also happens to be the latitude above which people do not receive sufficient sunlight to retain adequate vitamin D levels during winter. This suggests a possible role for vitamin D in determining outcomes from COVID‐19. There are outliers of course—mortality is relatively low in Nordic countries—but there vitamin D deficiency is relatively uncommon, probably due to widespread use of supplements. 4 Italy and Spain, perhaps surprisingly, have relatively high prevalences of vitamin D deficiency. Vitamin D deficiency has also been shown to correlate with hypertension, 5 diabetes, 6 obesity 7 and ethnicity 8 —all features associated with increased risk of severe COVID‐19.
There are considerable experimental data showing that vitamin D is important in regulating and suppressing the inflammatory cytokine response of respiratory epithelial cells and macrophages to various pathogens including respiratory viruses. 9 Evidence that vitamin D might protect against infection is modest but it is important to note that the hypothesis is not that vitamin D would protect against SARS‐CoV‐2 infection but that it could be very important in preventing the cytokine storm and subsequent acute respiratory distress syndrome that is commonly the cause of mortality. 10
Research is urgently needed to assess whether there may be a correlation between vitamin D status and severity of COVID‐19 disease. Meanwhile, the evidence supporting a protective effect of vitamin D against severe COVID‐19 disease is very suggestive, a substantial proportion of the population in the Northern Hemisphere will currently be vitamin D deficient, and supplements, for example, 1000 international units (25 micrograms) per day are very safe. It is time for governments to strengthen recommendations for vitamin D intake and supplementation, particularly when under lock‐down.
AUTHORSHIP
Guarantor of the article: None.
Author contributions: All authors contributed to writing and revision and approved the final version.
ACKNOWLEDGEMENTS
Declaration of personal interests: JMR is Co‐Editor of Alimentary Pharmacology and Therapeutics and with the University of Liverpool and Provexis UK, holds a patent for use of a soluble fibre preparation as maintenance therapy for Crohn's disease plus a patent for its use in antibiotic‐associated diarrhoea. Patent also held with the University of Liverpool and others in relation to use of modified heparins in cancer therapy. SS has received speaker fees from MSD, Actavis, Abbvie, Dr Falk pharmaceuticals, Shire and received educational grants from MSD, Abbvie, Actavis and is an advisory board member for Abbvie, Dr Falk pharmaceutics and Vifor pharmaceuticals. EL and RAK have no conflicts to declare.
REFERENCES
- 1. Al‐Ani A, Rentsch C, Prentice R, et al. Review article: prevention, diagnosis and management of COVID‐19 in the inflammatory bowel disease patient. Aliment Pharmacol Ther. 2020; 10.1111/apt.15779 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Panarese A, Shahini E. COVID‐19 and vitamin D. (letter). Aliment Pharmacol Therap. 2020;51:993‐995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. https://www.worldometers.info/coronavirus/ Accessed April 15, 2020.
- 4. Lips P, Cashman KD, Lamberg‐Allardt C, et al. Current vitamin D status in European and Middle East countries and strategies to prevent vitamin D deficiency: a position statement of the European Calcified Tissue Society. Eur J Endocrinol. 2019;180:P23‐P54. [DOI] [PubMed] [Google Scholar]
- 5. Kunutsor SK, Apekey TA, Steur M. Vitamin D and risk of future hypertension: meta‐analysis of 283,537 participants. Eur J Epidemiol. 2013;28:205‐221. [DOI] [PubMed] [Google Scholar]
- 6. Mauss D, Jarczok MN, Hoffmann K, Thomas GN, Fischer JE. Association of vitamin D levels with type 2 diabetes in older working adults. Int J Med Sci. 2015;12:362‐368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Yao Y, Zhu L, He L, et al. A meta‐analysis of the relationship between vitamin D deficiency and obesity. Int J Clin Exp Med. 2015;8:14977‐14984. [PMC free article] [PubMed] [Google Scholar]
- 8. Herrick KA, Storandt RJ, Afful J, et al. Vitamin D status in the United States, 2011–2014. Am J Clin Nutr. 2019;110:150‐157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Greiller CL, Martineau AR. Modulation of the immune response to respiratory viruses by vitamin D. Nutrients. 2015;7:4240‐4270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Laird E, Kenny RA.Vitamin D deficiency in Ireland: Implications for COVID‐19. Results from the Irish longitudinal study on ageing. 2020. 10.38018/TildaRe.2020-05 [DOI]