

The COVID‐19 pandemic is caused by a novel coronavirus, SARS‐CoV‐2, isolated in patients with severe pneumonia in China on December 30, 2019, having spread throughout the world since then with 2,056,054 cases diagnosed and 134,177 deaths (as of 15th April 2020).
The clinical presentation widely referenced is fever, cough, headache, myalgia, asthenia, anosmia, and diarrhea 1 , 2 ; but few dermatological findings associated with the virus have been described to date. 3 , 4 , 5
Over recent days, a series of cases in Spain have begun to emerge noted by many dermatologists. Amongst them is a group to which the authors belong called Teledermasolidaria. This group of dermatologists has been treating urgent cases from home via an application made available by the Spanish Academy of Dermatology and Venereology (AEDV).
Initially, a series of cases consulted us through our personal mobile phones and sent their photographs to us. Later, the queries increased in number. Most of the patients were children (median 13 years) and young adults (median 31, average 36, range 18–91 years old). The lesions are initially reddish and papular resembling chilblains. Subsequently, in the span of approximately 1 week they become more purpuric and flattened. Finally, they seem to resolve by themselves without requiring any treatment. Patients did not show Raynaud or signs of ischemia. Although there is some referred discomfort or pain when palpated, the skin lesions were not very symptomatic. The majority of patients did not present with coronavirus symptoms and when presented they were mild fever or congestion. Except for the oldest patient (91 years old), none of them presented with significant respiratory condition, and they were generally in good health.
Herein we share with the dermatology communities around the world a sample of our private patients with chilblain‐like lesions which may be a cutaneous manifestation of COVID‐19 so that dermatologists can be aware of these findings.
Cases
Our cohort of six patients presented with multiple skin lesions, especially on the toes, soles, fingers, extremities and/or heel similar to chilblains as shown in Figs. 1, 2, 3, 4, 5 and Table 1. Our patients were asymptomatic without coronavirus symptoms. Very few referred cough, fever, or congestion 3‐4 weeks before and some had risky contacts. Two of the patients had a positive test weeks before.
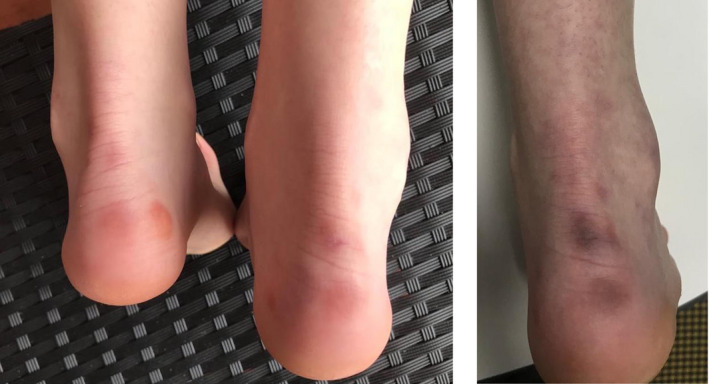
Figure 1.

(a) chilblain lesions on toes (b) detail of the toe lesions (c) similar lesions on heel
Figure 2.
(a) Initial erythematous and papular lesions on heels b) the same lesions one week later
Figure 3.

An acral lesion with a little crust
Figure 4.

Erythematous lesions slightly painful to rubbing
Figure 5.

Erythematous‐violaceous lesions in acral areas of the toe. The patient had similar lesions on the other foot
Table 1.
Location and symptoms of chilblain‐like lesions in children and adults during the pandemic
| Age/sex | Chilblain location/symptoms | COVID‐19 positive | Symptoms of COVID‐19, | Close contact to COVID‐19 | Time in weeks during/prior/after COVID‐19 | |
|---|---|---|---|---|---|---|
| 1 | 15/M | Toes, heel/ mild itchy |
PCR negative Chest X‐ray: bilateral pneumonia |
Asymptomatic | No | Unknown: skin lesions led to the diagnosis of pneumonia, otherwise asymptomatic. |
| 2 | 15/F | Finger, heel/ mildly painful when pressing | Test not done | Nasal congestion, diarrhea | Father with COVID‐19, close contact | One week prior mild symptoms and 3 weeks after visiting her father |
| 3 | 23/F | Toes/mild itchy | Test not done | Fever, headaches, itchy | Lives in high risk area | 3 weeks prior |
| 4 | 44/M | Toe/mildly painful when pressing | Test not done | Sore throat | Unknown | Sore throat 10 days earlier |
| 5 | 91/M | Toe | Yes (requiring hospitalization) | Recovered | After 3 weeks of COVID‐19 confirmed | |
| 6 | 24/F | Toes/painful when pressing | Yes | After infection |
This article is being made freely available through PubMed Central as part of the COVID-19 public health emergency response. It can be used for unrestricted research re-use and analysis in any form or by any means with acknowledgement of the original source, for the duration of the public health emergency.
Patient 1
An asthmatic 15‐year‐old male patient consulted in the Emergency Department for multiple skin lesions (five in toes and heels; Fig. 1a–c). The patient was otherwise asymptomatic. Because of an awareness of this type of lesion, a chest x‐ray was performed showing mild bilateral pneumonia. The patient was treated with hydroxychloroquine, azithromycin, and prophylactic heparin with resolution of the lung opacities. Surprisingly, polymerase chain reaction (PCR) and rapid antibody test were negative.
Patient 2
A 15‐year‐old female presented with lesions in fingers and heels 3 weeks after visiting her father who had COVID‐19. She was living with him until he became ill and consequently was admitted to the hospital after testing positive for COVID‐19. She had nasal congestion and mild diarrhea 1 week before the skin lesions appeared. Similar to the other patients, the lesions initially were reddish and palpable (Fig. 2a) and 1 week later became purpuric (Fig. 2b).
Patient 3
A 23‐year‐old female consulted through mobile phone because of lesions on her toes that were a little itchy. She recalls having fever and headache 3 weeks before the onset of skin lesions. We did not have the possibility to do any test for COVID‐19. However, she lives in a high‐risk COVID‐19 area.
Patient 4
A 44‐year‐old male consulted through mobile phone because of a slightly painful lesion on his toe, especially when touched, that was preceded by sore throat. We were not able to test this patient either.
Patient 5
A 91‐year‐old male from the Primary Care Centre consulted for a cutaneous asymptomatic lesion on his toe. He had been hospitalized because of COVID‐19 confirmed by PCR 3 weeks before. We do not know exactly when the skin lesions appeared but he was recovering at home at the time the lesions were noticed by his doctor.
Patient 6
A 24‐year‐old female with lesions on her toes after COVID‐19 infection confirmed by PCR. Unfortunately, we have no photographs of her lesions.
Discussion
The lack of confirmatory testing does not allow us to corroborate the association of these type of lesions with COVID‐19. However, the high number of consultations made for these rare lesions in the current epidemiological context makes us think that there may be a relationship. Spain is currently in a state of alarm so the population has been isolated in their homes since March 14, which makes another etiology like cold or trauma unlikely.
Similar lesions and news about the same type of injuries in teenagers and young people have appeared simultaneously in other countries (Italy and France), which are at a similar moment in the curve of the epidemic. 6 , 7
Our hypothesis is that these lesions could be a late manifestation of COVID‐19. This theory is based on the fact that the lesions appeared weeks after reaching the peak of infections in Spain but not at the beginning so far as we are aware. This is supported by the fact that some of the patients reported compatible symptoms or higher risk contacts (sick persons or health workers) weeks prior to the appearance of skin lesions. We hypothesized that it could be antigen‐antibody immunological processes at a time when the viral load and infectivity are low.
The fact that the PCR had been negative in some of the patients in which it was performed, could be justified for three reasons: there was no coronavirus infection, false negatives, or that it was really a late manifestation in which PCR had already reversed to negative.
It has also been discussed in dermatology forums whether these lesions are histologically translating vasculitis or the presence of microthrombi. Acro‐ischemia has been described in critical COVID‐19 patients in the context of possible hypercoagulation status. 8 Similarly, digital ischemia has been described as a complication of influenza, probably in relation to immunological mechanisms and the activation of a prothrombotic state. 9 These published cases differ from our presented patients as they are in the context of an acute infection with criteria of severity and findings of cutaneous ischemia in adult patients. Purpuric skin lesions have also been described in children in the context of other viral infections. Although parvovirus is perhaps the virus most involved in purpuric lesions, we would like to highlight a published case of acute hemorrhagic edema of infancy due to a different coronavirus (NL63). 10
Unfortunately, at the present time we have not had the opportunity to biopsy to verify whether these lesions are vasculitis or vasculopathy, microthrombi occlusion, cutaneous polyarteritis nodosa (PAN), or chilblain‐like lupus.
It is interesting that cutaneous lesions have also been described in animals (particularly in cats) in coronavirus infections and that they have been more frequent in young animals and in late stages of the disease. In these cases, the lesions are different presenting as nodular pyodermatitis but in the biopsies vasculitis and necrosis have been described. 11
Our impressions are only hypothetical so confirmation is needed. Our proposal is that, until it can be confirmed, when faced with these type of lesions we need to explore possible contacts with COVID‐19, and in every case inquire about the existence of fever or cold in the weeks prior to the appearance of the skin lesions. Likewise, these lesions could help the diagnosis in patients who are otherwise asymptomatic. In fact, it is considered that between 20–78% of cases could be asymptomatic, 12 which would be consistent with our series if the hypothesis is confirmed. Furthermore, it would be of great interest to perform the reverse transcription polymerase chain reaction (RT‐PCR) test and IgM ‐IgG serological test in these patients.
Until further confirmation that these lesions are related to COVID‐19, we must be cautious and recommend general measures of social distance, hygiene, self‐isolation, and surveillance.
Acknowledgments
We wish to express our appreciation to Dr. Cristina Galván for leading the immeasurable study on skin lesions and COVID‐19 in Spain, as well as Dr. Rosa Taberner for her reputable blog (blog dermapixel) where one may find further information regarding this problem, and all my colleagues on the “dermachat” forum. Finally, Dr. Pablo Fonda is to be commended for his excellent and inspiring initiative, Teledermasolidaria. We also want to show our condolences for the deceased and their families.
Conflict of interest: None.
Funding source: None.
The related Letter from the Editor of this paper is available (https://doi.org/10.1111/ijd.14956)
References
- 1. Phelan AL, Katz R, Gostin LO. The novel coronavirus originating in Wuhan, China. JAMA 2020; 323(8): 709 10.1001/jama.2020.1097 [DOI] [PubMed] [Google Scholar]
- 2. Huang C, Wang Y, Li X, et al Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020; 395: 497–506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Recalcati S. Cutaneous manifestations in COVID‐19: a first perspective. J Eur Acad Dermatol Venereol 2020. [Epub ahead of print]. 10.1111/jdv.16387 [DOI] [PubMed] [Google Scholar]
- 4. Fernandez‐Nieto D, Ortega‐Quijano D, Segurado‐Miravalles G, Pinedo‐Ortega C, Prieto‐Barrios M, Jimenez‐Cauhe J. Comment on: cutaneous manifestations in COVID‐19: a first perspective. Safety concerns of clinical images and skin biopsies. J Eur Acad Dermatol Venereol 2020. [Epub ahead of print]. 10.1111/jdv.16470 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Mahé A, Birckel E, Krieger S, Merklen C, Bottlaender L. A distinctive skin rash associated with Coronavirus Disease 2019? J Eur Acad Dermatol Venereol 2020. [Epub ahead of print]. 10.1111/jdv.16471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Mazzotta F, Troccoli T. Monday's case: acute acro‐ischemia in the child at the time of COVID‐19. Eur J Pediatr Dermatol 2020. [Google Scholar]
- 7. Mollaret G. Covid‐19: les dermatologues appellant à la vigilance sur les acrosyndromes et érythèmes faciaux. Le quotidien du medecin 2020. Apr. Available from: https://www.lequotidiendumedecin.fr/specialites/dermatologie/covid-19-les-dermatologues-appellent-la-vigilance-sur-les-acrosyndromes-et-erythemes-faciaux.
- 8. Zhang Y, Cao W, Xiao M, et al Clinical and coagulation characteristics of 7 patients with critical COVID‐2019 pneumonia and acro‐ischemia. Zhonghua Xue Ye Xue Za Zhi 2020; 41: E006. [DOI] [PubMed] [Google Scholar]
- 9. Korytny A, Kibari A, Rosner I, Zisman D. Digital ischemia in a patient with recent influenza A infection. IMAJ 2018; 20: 446–447. [PubMed] [Google Scholar]
- 10. Chesser H, Chambliss JM, Zwemer E. Acute hemorrhagic edema of infancy after coronavirus infection with recurrent rash. Case Rep Pediatr 2017; 2017: 1–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Redford T, Al‐Dissi AN. Feline infectious peritonitis in a cat presented because of popular skin lesions. Can Vet J 2019; 60: 183–185. [PMC free article] [PubMed] [Google Scholar]
- 12. Black JRM, Bailey C, Swanton CH. COVID‐19: the case for health‐care worker screening to prevent hospital transmission. Lancet 2020. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]