

Abstract
Background
Hypospadias is a common male birth defect that has shown widespread variation in reported prevalence estimates. Many countries have reported increasing trends over recent decades.
Objective
To analyze the prevalence and trends of hypospadias for 27 international programs over a 31-yr period.
Design, setting, and participants
The study population included live births, stillbirths, and elective terminations of pregnancy diagnosed with hypospadias during 1980–2010 from 27 surveillance programs around the world.
Outcome measurements and statistical analysis
We used joinpoint regression to analyze changes over time in international total prevalence of hypospadias across programs, prevalence for each specific program, and prevalence across different degrees of severity of hypospadias.
Results and limitations
The international total prevalence of hypospadias for all years was 20.9 (95% confidence interval: 19.2–22.6) per 10 000 births. The prevalence for each program ranged from 2.1 to 39.1 per 10 000 births. The international total prevalence increased 1.6 times during the study period, by 0.25 cases per 10 000 births per year (p < 0.05). When analyzed separately, there were increasing trends for first-, second-, and third-degree hypospadias during the early 1990s to mid-2000s. The majority of programs (61.9%) had a significantly increasing trend during many of the years evaluated. Limitations include known differences in data collection methods across programs.
Conclusions
Although there have been changes in clinical practice and registry ascertainment over time in some countries, the consistency in the observed increasing trends across many programs and by degrees of severity suggests that the total prevalence of hypospadias may be increasing in many countries. This observation is contrary to some previous reports that suggested that the total prevalence of hypospadias was no longer increasing in recent decades.
Patient summary
We report on the prevalence and trends of hypospadias among 27 birth defect surveillance systems, which indicate that the prevalence of hypospadias continues to increase internationally.
Keywords: Hypospadias, Prevalence, Trend, Joinpoint regression, International Clearinghouse for Birth Defects Surveillance and Research
1. Introduction
Hypospadias, which is caused by incomplete development of the urethra, is one of the most common congenital anomalies in male infants, with an estimated prevalence of 64.7 cases per 10 000 male live births in the USA [1]. Hypospadias can have different degrees of clinical severity, as defined by the location of the urethral opening [2]. Estimates of the prevalence of hypospadias vary across and within different geographical settings globally. The extent to which artifactual differences (eg, differences in clinical practice, registry ascertainment, or case definitions) contribute to the observed prevalence differences is unknown. Moreover, there have been reports of increases in the prevalence of hypospadias in many countries, especially in the last decades of the 20th century [2–9]. However, a number of countries have also reported that the prevalence has not increased in recent decades [3,7,9–17].
To better understand prevalence trends in recent years across the world, we evaluated hypospadias data in 27 birth defect surveillance programs participating in the International Clearinghouse for Birth Defects Surveillance and Research (ICBDSR).
2. Patients and methods
2.1. Data collection
The ICBDSR is a World Health Organization (WHO)-affiliated network of birth defects surveillance programs. The general methods of the ICBDSR are described elsewhere [18]. Each of the 27 surveillance programs identified hypospadias cases under their established protocol for births during 1980–2010 (case surveillance and selection methods are detailed in the Supplementary material).
2.2. Statistical analysis
We calculated an international total prevalence of hypospadias per 10 000 births, defined as the total number of cases of live births, stillbirths, and elective terminations of pregnancy for fetal anomaly (ETOPFAs) across all 27 programs divided by the total number of births (live births and stillbirths, regardless of sex) during the full study period (1980–2010). (We reported the total prevalence per male and female births for comparability with international prevalence reports of other birth defects.) As some programs did not have data between 1980 and 1999, we also calculated the international total prevalence of hypospadias per 10 000 births for a more recent period (2000–2010). Lastly, we calculated the total prevalence of hypospadias for each individual program during 1980–2010 and 2000–2010. The approximate 95% confidence interval (CI) was also calculated for all prevalence estimates. In addition, we determined the quartile (1, 2, 3, or 4) in which each program’s total prevalence was located (eg, programs in quartile 1 had a total prevalence within the lowest 25% of all the programs).
To visualize the data over time and to assess temporal changes in trends, we conducted analyses using joinpoint regression. Joinpoint regression is helpful for identifying linear trends in total prevalence over time that are restricted to subperiods, rather than testing for linear trends only across the entire time period [19]. This approach agnostically identifies joinpoints that parse the data into periods of varying sizes, based on the presence of similar linear trends within each period [19].
We conducted joinpoint regression for the total analytic group (all 27 programs) during the full study period. These analyses were repeated among a subset of 19 programs with three characteristics (hereafter referred to as the “main subgroup”): (1) population-based ascertainment, (2) ascertainment of cases ≥1 yr of age, and (3) ascertainment of cases from multiple sources. This subanalysis was repeated again, including only eight programs from the main subgroup with at least 30 yr of data available. For comparison, we plotted the total prevalence of these eight programs over time in the same figure.
We also conducted analyses separately for first-, second-, and third-degree hypospadias, including only the 12 programs for which the degree of severity was specified for ≥80% of cases. These analyses were repeated among seven programs that were also in the main subgroup.
To better understand similarities and differences across programs, analyses were also performed during the full study period for each separate program. (Programs with <11 yr of data or with intermediate years of missing data were not included in this analysis, in order to meet the software’s minimal requirements [19].)
All statistical tests were two sided, and we interpreted statistical significance based on p < 0.05. Joinpoint regression analyses were performed using Joinpoint Trend Analysis Software (version 4.4.0.0) from the National Cancer Institute [20].
3. Results
3.1. Program characteristics
The characteristics of each program are summarized in Table 1. The majority of programs used population-based case Identification (21 programs, 77.8%), registered cases up to 12 mo of age or beyond (22 programs, 81.5%), and received notification of cases from multiple sources (19 programs, 70.4%). Only 12 programs (44.4%) specified the degree of severity of hypospadias in ≥80% of cases.
Table 1 –
Summary of program characteristics (International Clearinghouse for Birth Defects Surveillance and Research)
| Program | Delivery years | Total births | Ascertainment to at least 1 yr | Population based | Ascertainment from multiple sources | Degree of severity specified in ≥80% of cases |
|---|---|---|---|---|---|---|
| Argentinaa | 2009–2010 | 42 136 | No | No | No | No |
| Australiab | 1980–2010 | 792 512 | Yes | Yes | Yes | Yes |
| Canada (National)c | 2005–2010 | 1 416 099 | No | Yes | No | No |
| Alberta, Canadad | 1980–2010 | 1 309 669 | Yes | Yes | Yes | No |
| Chile-Maule e | 2002–2010 | 119 900 | No | No | No | Yes |
| Colombia | 2001–2010 | 174 425 | Yes | No | No | Yes |
| Costa Ricaf | 1987–2010 | 1 842 791 | Yesg | Yes | No | No |
| Czech Republic | 1980–2010 | 3 597 530 | Yes | Yes | Yes | Yes |
| Finland | 1993–2010 | 1 068 457 | Yes | Yes | Yes | Yes |
| Franceh | 1980–2010 | 2 819 326 | Yes | Yes | Yes | No |
| Germanyi | 1987–2010 | 336 716 | Yes | Yes | Yes | No |
| Hungary | 1980–2010 | 3 507 915 | Yes | Yes | Yes | No |
| Iranj | 2005–2010 | 130 724 | Yes | No | Yes | –k |
| Lombardia, Italy | 1999–2010 | 179 484 | Yes | Yes | Yes | No |
| Tuscany, Italyl | 1992–2010 | 519 749 | Yes | Yes | Yes | No |
| Maltam | 1993–2010 | 77 261 | Yes | Yes | Yes | Yes |
| Mexicon | 1980–2010 | 1 093 745 | No | No | No | Yes |
| New Zealand | 1980–1993 | 1 638 216 | Yes | Yes | Yes | –k |
| 1996–2010 | ||||||
| Northern Netherlands | 1981–2010 | 496 810 | Yes | Yes | Yes | Yes |
| Slovak Republic | 1995–2010 | 902 372 | Yes | Yes | No | Yes |
| Spaino | 1980–2010 | 2 648 286 | No | No | No | Yes |
| Sweden | 1980–2010 | 3 166 009 | Yes | Yes | Yes | No |
| Arkansas, USAp | 1993–2010 | 684 001 | Yes | Yes | Yes | Yes |
| Atlanta, GA, USAq | 1980–2010 | 1 299 822 | Yes | Yes | Yes | No |
| Texas, USA | 1996–2010 | 5 216 949 | Yes | Yes | Yes | No |
| Utah, USAr | 1999–2010 | 615 886 | Yes | Yes | Yes | Yes |
| Waless | 1998–2010 | 430 710 | Yes | Yes | Yes | No |
National Network of Congenital Anomalies of Argentina (RENAC).
Western Australian Register of Developmental Anomalies.
Canadian Congenital Anomalies Surveillance System.
Alberta Congenital Anomalies Surveillance System.
Registro de malformaciones congénitas del Servicio de Salud Maule (RRMC-SSM).
Centro de Registro de Enfermedades Congénitas.
For births during 2009 and later only.
Registre des Malformations en Rhône-Alpes (REMERA).
Saxony-Anhalt.
Tabriz Registry of Congenital Anomalies.
No information on degree of severity.
Tuscan Registry of congenital defects (RTDC).
Malta Congenital Anomalies Register.
Registration and Epidemiologic Surveillance of External Congenital Malformations (RYVEMCE).
Spanish Collaborative Study of Congenital Malformations (ECEMC).
Arkansas Reproductive Health Monitoring System.
Metropolitan Atlanta Congenital Defects Program.
Utah Birth Defect Network.
Congenital Anomaly Register & Information Service for Wales.
3.2. International prevalence of hypospadias
For all programs combined, there were 36127 500 births and 74 814 cases with hypospadias. The international total prevalence of hypospadias was 20.9 (95% CI: 19.2–22.6) per 10 000 births among 27 programs of the ICBDSR during 1980–2010. For 2000–2010 specifically, the international total prevalence was 23.8 (95% CI: 22.1–25.5) per 10 000 births. Program-specific prevalences for 19802010 and 2000–2010 were tabulated (Table 2) and also presented in a histogram (Fig. 1). Arkansas, USA, had the highest total prevalence (39.1 cases per 10 000 births, 95% CI: 36.7–41.4), while Argentina had the lowest total prevalence (2.1 cases per 10 000 births, 95% CI: 1.1–4.8). Programs in Latin American countries (ie, Argentina, Chile, Colombia, Mexico, and Costa Rica) had relatively lower total prevalence estimates than programs in other regions (Fig. 1). The total prevalence in Europe was highly variable, ranging from 10.6 (France) to 37.4 (Lombardia, Italy) cases per 10 000 births. Only four (Atlanta, GA, USA; Mexico; Spain; and Slovak Republic) out of 27 programs had a lower total prevalence in the recent period (2000–2010) than the whole period (1980–2010; Fig. 1).
Table 2 –
Total prevalence of hypospadias by program and time period (International Clearinghouse for Birth Defects Surveillance and Research)
| Program | Delivery years | 1980–2010 |
2000–2010 |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Total prevalence per 10 000 | 95% Confidence interval |
Quartilea | Total prevalence per 10 000 | 95% Confidence interval |
Quartilea | ||||
| Lower | Upper | Lower | Upper | ||||||
| Argentina | 2009–2010 | 2.14 | 1.11 | 4.83 | Q1 | 2.14 | 1.11 | 4.83 | Q1 |
| Australia | 1980–2010 | 33.68 | 31.58 | 35.34 | Q4 | 36.21 | 34.26 | 38.32 | Q4 |
| Canada (National) | 2005–2010 | 24.45 | 23.57 | 25.31 | Q3 | 24.45 | 23.57 | 25.31 | Q3 |
| Alberta, Canada | 1980–2010 | 21.13 | 19.77 | 22.31 | Q3 | 21.51 | 19.84 | 22.94 | Q2 |
| Chile-Maule | 2002–2010 | 8.26 | 6.62 | 9.85 | Q1 | 8.26 | 6.62 | 9.85 | Q1 |
| Colombia | 2001–2010 | 4.70 | 4.24 | 9.17 | Q1 | 4.70 | 4.24 | 9.17 | Q1 |
| Costa Rica | 1987–2010 | 4.77 | 4.24 | 5.42 | Q1 | 6.17 | 5.62 | 6.74 | Q1 |
| Czech Republic | 1980–2010 | 25.64 | 24.31 | 27.72 | Q3 | 31.86 | 30.29 | 32.70 | Q4 |
| Finland | 1993–2010 | 15.54 | 14.64 | 16.37 | Q2 | 15.97 | 14.74 | 17.11 | Q2 |
| France | 1980–2010 | 10.60 | 9.56 | 11.54 | Q1 | 12.55 | 11.67 | 13.49 | Q1 |
| Germany | 1987–2010 | 18.21 | 16.47 | 20.61 | Q2 | 19.32 | 17.09 | 21.65 | Q2 |
| Hungary | 1980–2010 | 22.30 | 21.17 | 23.92 | Q3 | 25.78 | 23.28 | 28.35 | Q3 |
| Iran | 2005–2010 | 13.69 | 8.70 | 18.41 | Q2 | 13.69 | 8.70 | 18.41 | Q2 |
| Lombardia, Italy | 1999–2010 | 37.38 | 33.42 | 40.92 | Q4 | 38.11 | 34.17 | 41.70 | Q4 |
| Tuscany, Italy | 1992–2010 | 19.22 | 17.15 | 21.16 | Q2 | 20.17 | 18.07 | 22.34 | Q2 |
| Malta | 1993–2010 | 29.64 | 22.46 | 38.88 | Q4 | 36.45 | 26.22 | 47.28 | Q4 |
| Mexico | 1980–2010 | 3.17 | 2.67 | 3.40 | Q1 | 2.75 | 2.04 | 3.53 | Q1 |
| New Zealand | 1980–1993 | 19.61 | 16.56 | 22.21 | Q2 | 27.02 | 24.65 | 29.70 | Q3 |
| 1996–2010 | |||||||||
| Northern Netherlands | 1981–2010 | 15.06 | 12.80 | 17.05 | Q2 | 20.04 | 17.39 | 22.98 | Q2 |
| Slovak Republic | 1995–2010 | 21.98 | 20.30 | 23.81 | Q3 | 21.35 | 19.09 | 23.93 | Q2 |
| Spain | 1980–2010 | 14.75 | 14.12 | 16.34 | Q2 | 12.11 | 11.47 | 12.73 | Q1 |
| Sweden | 1980–2010 | 20.01 | 18.52 | 21.48 | Q3 | 24.97 | 23.39 | 26.26 | Q3 |
| Arkansas, USA | 1993–2010 | 39.11 | 36.67 | 41.43 | Q4 | 40.13 | 36.67 | 43.50 | Q4 |
| Atlanta, GA, USA | 1980–2010 | 31.28 | 29.66 | 32.70 | Q4 | 30.21 | 27.99 | 32.61 | Q3 |
| Texas, USA | 1996–2010 | 28.14 | 26.36 | 29.01 | Q3 | 28.57 | 27.32 | 29.75 | Q3 |
| Utah, USA | 1999–2010 | 30.59 | 28.03 | 32.84 | Q4 | 31.05 | 28.52 | 33.34 | Q3 |
| Wales | 1998–2010 | 31.65 | 30.57 | 32.80 | Q4 | 32.15 | 31.25 | 33.13 | Q4 |
| Total | – | 20.91 | 19.19 | 22.63 | – | 23.78 | 22.06 | 25.50 | – |
Q1 corresponds to the lowest quartile of total prevalence and Q4 corresponds to the highest quartile.
Fig. 1 -.

Total prevalence of hypospadias (per 10 000) for International Clearinghouse for Birth Defects Surveillance and Research (ICBDSR) programs, grouped by world region, 1980–2010 and 2000–2010.
Changes in the international total prevalence of hypospadias were visualized using joinpoint regression (Supplementary Fig. 1), with joinpoints identified at 1996 and 1999. Since 1999, the total prevalence increased significantly by 0.25 cases per year (p = 0.001). This analysis was repeated among the main subgroup (Fig. 2A). For these programs, there was an increasing trend during the entire period 1980–2010, and this increase was statistically significant (p < 0.001) during 1980–1996 (0.19 cases per year) and 1999–2010 (0.34 cases per year). The analysis was repeated using data from the eight programs with at least 30 yr of data (Fig. 2B). Among these programs, there was a 1.6-time increase in the total prevalence of hypospadias during the entire study period (from 1980 to 2010) by an average of 0.34 cases per year (p < 0.001). Among these programs (Fig. 2C), France had a relatively lower total prevalence during the entire period.
Fig. 2 -.

Trends in the International total prevalence of hypospadias among ICBDSR programs with select characteristics using joinpoint regression, 1980–2010. a (A) Among 19 programs with (1) population-based ascertainment, (2) age of ascertainment ≥1 yr, and (3) ascertainment from multiple sources. (B) Among eight programs with (1) population-based ascertainment, (2) age of ascertainment ≥1 yr, (3) ascertainment from multiple sources, and (4) at least 30 yr of data. (C) Results by program, among eight programs with (1) population-based ascertainment, (2) age of ascertainment ≥1 yr, (3) ascertainment from multiple sources, and (4) at least 30 yr of data. ICBDSR= International Clearinghouse for Birth Defects Surveillance and Research. a Stars indicate joinpoints with statistically significant (p < 0.05) trends.
3.3. Prevalence of hypospadias by degree of severity
Fig. 3A–C shows the results from joinpoint regression analyses for first-, second-, and third-degree hypospadias, respectively. These analyses were restricted to programs with the degree of severity of hypospadias specified in >80% of cases (12 programs). Across all three degrees of severity, increasing trends were observed from the mid-1990s to the mid-2000s (Fig. 3A–C). Similar trends were observed after repeating these analyses among seven programs that were also in the main subgroup (Supplementary Fig. 2A–C). Among these, 62.2% of cases had first-degree hypospadias, 20.1% had second-degree hypospadias, 4.5% had third-degree hypospadias, and 13.2% had an unspecified degree of severity (data not shown).
Fig. 3 -.

Trends in the International total prevalence of hypospadias for 12 ICBDSR programs by clinica! degree of severity, 1980–2010 a,b: (A) First-degree hypospadias, (B) second-degree hypospadias, and (C) third-degree hypospadias. ICBDSR = International Clearinghouse for Birth Defects Surveillance and Research. a Stars indicate joinpoints with statistically significant (p < 0.05) trends. b Programs for which the degree of severity was unspecified in ≥80% of cases were excluded.
3.4. Program-specific prevalence of hypospadias
Supplementary Fig. 3 illustrates the results from the joinpoint regression for each program with at least 11 yr of data (the software’s minimal requirements). Five of the 27 programs were excluded from these analyses because they had <11 yr of data (Argentina, Colombia, Chile, Canada [National], and Iran). As the software required complete data for each year analyzed, New Zealand was also excluded due to missing data for some years. Table 3 summarizes the trends from these analyses. Different trend patterns were observed across programs, including patterns of increases in total prevalence during much or all of the study period for a number of programs. In fact, significant increases in the total prevalence of hypospadias were observed for 45.0% of the years of observation, whereas significant decreases in the total prevalence were observed for only 10.4% of the years of observation.
Table 3 –
Annual trends in the total prevalence of hypospadias by program, 1980–2010
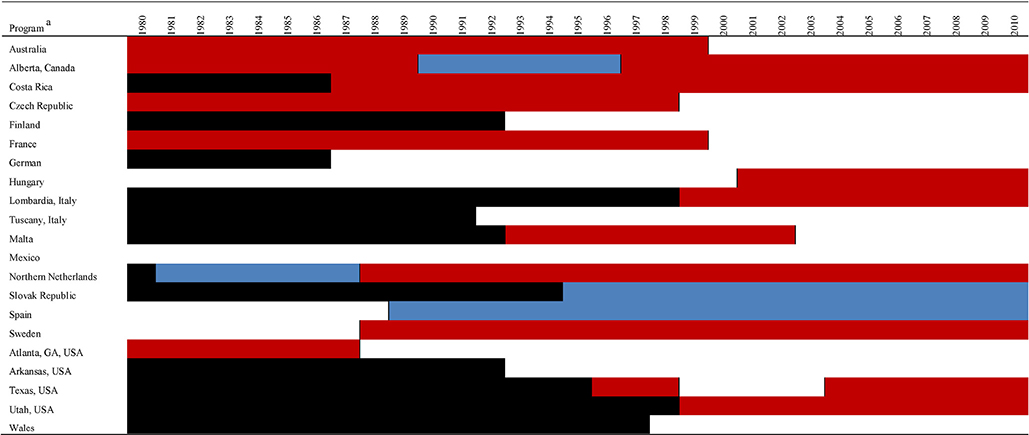 |
Key: red boxes represent years with a significantly increasing trend in total prevalence of hypospadias (p < 0.05); blue boxes, years with a significantly decreasing trend (p < 0.05); white boxes, years with no significant trend (p ≥ 0.0.5); and black boxes, years with no observations.
Joinpoint regression was not performed for programs with <11 yr of data (Argentina, Colombia, Chile, Canada [National], and Iran) or any years of missing data during the period analyzed (New Zealand) due to the software’s minimum data requirements.
4. Discussion
Among 27 programs participating in the ICBDSR, the total prevalence of hypospadias was 20.9 per 10 000 births during 1980–2010, although it varied greatly by geographical region.
The international total prevalence of hypospadias increased during the entire study period, with significant increases from 2000 to 2010. When we restricted to programs among the main subgroup, the rates of increase were similar, although the time trend was significant over more years. The increasing trends were also consistent for most of the study period across all degrees of clinical severity of hypospadias.
Our international total prevalence estimates of hypospadias were similar to those from previous studies, with many previous reported estimates from individual ICBDSR programs, including the USA [5], Australia [2], Germany [21], Northern Netherlands [21], Hungary [21], Malta [21], Spain [21], and Tuscany [21]. For Latin American countries, our results were consistent with previous estimates from Argentina [22] and Mexico [23]. In fact, all Latin American programs had a relatively low prevalence that fell within the lowest quartile of all participating programs. As the magnitude of the difference was quite large and consistent across programs in Latin American countries, it is possible that the difference between Latin American countries and other countries may reflect true prevalence differences, perhaps related to differences in both genetic and nongenetic hypospadias risk factors.
As previously reported, programs in the USA and northern Europe had higher prevalence estimates [23]. There have been reports of increases in the prevalence of hypospadias in many countries, particularly during the late 1960s until around the early 1990s in the USA and Europe (reviewed in the work of Agopian [24]). Our results for the period from 1980 to early 1990s seem consistent with these reported increases.
However, this increase was reported to stabilize or even decrease in more recent years in many, though not all, studies [3,7,21], whereas we detected an increase throughout this time. For example, separate reports from Washington State, USA (1987–2002 births) [17], New York State, USA (1983–1995 births) [13], Scotland (1988–1997 births) [11], Italy (2001–2004 births) [14], Finland (1970–1994 births) [12], and Europe (1980–1999 births from the EUROCAT network) [7] did not indicate increases in the prevalence in more recent years. Furthermore, individual reports from Spain (1996–2002 births) [16], Northern England (19932000 births) [10], and Japan (1985–1997 births) [15] suggested that the prevalence may have been decreasing in recent years. As expected, among the countries represented in our study (ie, Finland, Italy, Spain, and other European regions), much of the corresponding data within these same time windows appeared to be similar in our data (ie, not increasing). However, our results among all programs indicated an increase in the total prevalence during recent years. This difference was probably related to the inclusion of a very large number of programs throughout a long (and in many instances, more recent) analysis period (1980–2010), as well as our use of joinpoint regression. However, it is noteworthy that these increases were not observed during the entire period for each program, and it is important to remember that our findings were most influenced by the programs with larger sample sizes.
Although our study likely reflects a better estimate of global trends than smaller studies, it is likely that some of the observed prevalence increases in our study were artifactual, and reflect changes over time in how cases with hypospadias were identified and documented at the medical facility and/or were ascertained by the surveillance system (eg, underascertainment in earlier years). While quality metrics for systematic assessment of birth defect surveillance have recently been proposed [25], many programs have not yet reported on these metrics [26,27]. Some ICBDSR systems implemented systematic surveillance changes during the study period (Supplementary Table 1), including a stronger focus on ascertaining less severe hypospadias cases in more recent years [21] and improvements in data collection over time.
Nevertheless, we still observed increasing prevalence time trends in the main subgroup, which represented 47.0% of total births across all ICBDSR programs. The data from these programs may have been less subject to bias compared with those from other sites, and these trends within this subgroup were similar to the trends observed in the full analytic group. This consistency suggests that much of the increasing trends in the prevalence of hypospadias may represent a true (nonartifactual) increase. However, consistent trends were not seen across every program.
It has been proposed that the observed prevalence increase might reflect increases in exposure to hypospadias risk factors overtime [9]. However, given the broad range of potentially relevant environmental and occupational exposures that could be responsible for the observed increase, as well as issues related to exposure dosage, timing, and other factors, it has been challenging to identify the main culprits. It is also possible that changes over time in the distribution of other parental factors associated with hypospadias risk (eg, parity, body mass index, maternal age, and fertility treatments) may have influenced the prevalence over time, but data were not available to assess this possibility in our analyses [24]. Further study of potential hypospadias risk factors, including genetic factors, endocrine disruptors, and other maternal and paternal exposures and characteristics may shed light on this possibility.
This study had some known limitations. First, it lacked uniformity in data collection across programs, which may have led to heterogeneity among cases across programs. Initiatives related to standardizing these methodologies across programs would be helpful to future work. Second, as individual-level data were not available, we could not adjust for differences in the distributions of hypospadias risk factors across countries, and this unmeasured confounding may also have partially accounted for the differences in hypospadias prevalence across programs. Third, the joinpoint regression modeled the data based on an assumption of linear trends across subperiods, although it did not account for completely nonlinear (eg, exponential) trends. Nevertheless, this statistical approach had more flexibility than a traditional assessment of a continuous prevalence estimate under the assumption of a linear change over an entire study period, which would not have been able to agnostically identify changes limited to study subperiods. We also did not have data related to co-occurring congenital malformations (~88.5% of hypospadias is expected to be isolated in European countries [21]) or on hypospadias treatment; while we had data on hypospadias severity for some programs, these data were not available for the majority of programs.
Despite these limitations, this study has several important strengths. We analyzed data from surveillance programs across the world, representing one of the largest case samples among published studies. Further, our data allowed us to look at trends over a 31-yr period. We also investigated the trends by differing degrees of severity and considered differences in characteristics of surveillance programs.
5. Conclusions
Our results suggest that the international total prevalence of hypospadias increased during 1980–2010 and that these trends were probably not entirely artifactual. Considering these trends, it seems clear that further surveillance around hypospadias is critical.
Supplementary Material
Acknowledgments
The authors thank Anna Barakova, MD, from the National Health Information Centre Team in Bratislava, for her cooperation. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Financial disclosures: A.J. Agopian certifies that all conflicts of interest, including specific financial interests and relationships and affiliations relevant to the subject matter or materials discussed in the manuscript (eg, employment/affiliation, grants or funding, consultancies, honoraria, stock ownership or options, expert testimony, royalties, or patents filed, received, or pending), are the following: None.
Funding/Support and role of the sponsor: None.
Footnotes
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in the online version, at https://doi.org/10.1016/j.eururo.2019.06.027.
References
- [1].Mai CT, Isenburg J, Langlois PH, et al. Population-based birth defects data in the United States, 2008 to 2012: presentation of state-specific data and descriptive brief on variability of prevalence. Birth Defects Res A Clin Mol Teratol 2015;103:972–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Nassar N, Bower C, Barker A. Increasing prevalence of hypospadias in Western Australia, 1980–2000. Arch Dis Child 2007;92:580–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Loane M, Dolk H, Kelly A, Teljeur C, Greenlees R, Densem J. Paper 4: EUROCAT statistical monitoring: identification and investigation of ten year trends of congenital anomalies in Europe. Birth Defects Res A Clin Mol Teratol 2011;91(Suppl. 1):S31–43. [DOI] [PubMed] [Google Scholar]
- [4].Czeizel A, Toth J, Czvenits E. Increased birth prevalence of isolated hypospadias in Hungary. Acta Paediatr Hung 1986;27:329–37. [PubMed] [Google Scholar]
- [5].Paulozzi LJ, Erickson JD, Jackson RJ. Hypospadias trends in two US surveillance systems. Pediatrics 1997;100:831–4. [DOI] [PubMed] [Google Scholar]
- [6].Fernández N, Pérez J, Monterrey P, et al. ECLAMC study: prevalence patterns of hypospadias in South America: multi-national analysis over a 24-year period. Int Braz J Urol 2017;43:325–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Dolk H, Vrijheid M, Scott JE, et al. Toward the effective surveillance of hypospadias. Environ Health Perspect 2004;112:398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Springer A, Van Den Heijkant M, Baumann S. Worldwide prevalence of hypospadias. J Pediatr Urol 2016;12:152.e1–e. [DOI] [PubMed] [Google Scholar]
- [9].Paulozzi LJ. International trends in rates of hypospadias and cryptorchidism. Environ Health Perspect 1999;107:297–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Abdullah N, Pearce M, Parker L, Wilkinson J, Jaffray B, McNally RJ. Birth prevalence of cryptorchidism and hypospadias in northern England, 1993–2000. Arch Dis Child 2007;92:576–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Ahmed S, Dobbie R, Finlayson A, et al. Prevalence of hypospadias and other genital anomalies among singleton births, 1988–1997, in Scotland. Arch Dis Child Fetal Neonatal Ed 2004;89:F149–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Aho M, Koivisto A-M, Tammela T, Auvinen A. Is the incidence of hypospadias increasing? Analysis of Finnish hospital discharge data 1970–1994. Environ Health Perspect 2000;108:463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Choi J, Cooper KL, Hensle TW, Fisch H. Incidence and surgical repair rates of hypospadias in New York State. Urology 2001;57:151–3. [DOI] [PubMed] [Google Scholar]
- [14].Ghirri P, Scaramuzzo RT, Bertelloni S, et al. Prevalence of hypospadias in Italy according to severity, gestational age and birthweight: an epidemiological study. Ital J Pediatr 2009;35:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Kurahashi N, Murakumo M, Kakizaki H, et al. The estimated prevalence of hypospadias in Hokkaido, Japan.J Epidemiol 2004;14:73–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Martínez-Frías ML, Prieto D, Prieto L, Bermejo E, Rodríguez-Pinilla E, Cuevas L. Secular decreasing trend of the frequency of hypospadias among newborn male infants in Spain. Birth Defects Res A Clin Mol Teratol 2004;70:75–81. [DOI] [PubMed] [Google Scholar]
- [17].Porter MP, Faizan MK, Grady RW, Mueller BA. Hypospadias in Washington State: maternal risk factors and prevalence trends. Pediatrics 2005;115:e495–9. [DOI] [PubMed] [Google Scholar]
- [18].Nassar N, Leoncini E, Amar E, et al. Prevalence of esophageal atresia among 18 international birth defects surveillance programs. Birth Defects Res A Clin Mol Teratol 2012;94:893–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Kim H-J, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med 2000;19:335–51. [DOI] [PubMed] [Google Scholar]
- [20].Applications Branch, Surveillance Research Program, National Cancer Institute. Methodology S. Joinpoint regression program, version 2013; 4(4). [Google Scholar]
- [21].Bergman JE, Loane M, Vrijheid M, et al. Epidemiology of hypospadias in Europe: a registry-based study. World J Urol 2015;33:2159–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Campaña H, Pawluk MS, López Camelo JS. Prevalencia al nacimiento de 27 anomalías congénitas seleccionadas, en 7 regiones geográ-ficas de la Argentina. Arch Argentin Pediatr 2010;108:409–17. [DOI] [PubMed] [Google Scholar]
- [23].Kallen B, Bertollini R, Castilla E, et al. A joint international study on the epidemiology of hypospadias. Acta Paediatr Scand Suppl 1986;324:1–52. [DOI] [PubMed] [Google Scholar]
- [24].Agopian AJ. Descriptive epidemiology of hypospadias In: Preston DH, editor. Hypospadias: risk factors, epidemiology and surgical outcomes. Nova Science Publishers Inc.; 2015. p. 1–24. [Google Scholar]
- [25].Groisman B, Mastroiacovo P, Barbero P, Bidondo MP, Liascovich R, Botto LD. A proposal for the systematic assessment of data quality indicators in birth defects surveillance. Birth Defects Res 2019;111:324–32. [DOI] [PubMed] [Google Scholar]
- [26].Groisman B, Barbero P, Mastroiacovo P, Botto LD, Bidondo MP, Liascovich R. Application of quality indicators to data from the National Network of Congenital Anomalies of Argentina. Birth Defects Res 2019;111:333–40. [DOI] [PubMed] [Google Scholar]
- [27].EUROCAT: European Surveillance of Congenital Anomalies. Data quality indicators. http://www.eurocat-network.eu/aboutus/datacollection/dataquality/dataqualityindicators.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.