

The Supplemental Security Income (SSI) program, signed into law in 1972, is a federal cash assistance program administered by the Social Security Administration (SSA) that provides supplemental income to individuals below federally set income limits and who have disabilities, are blind, or are at least 65 years old. The SSI program was designed to increase the economic security of vulnerable families; therefore, it also has the potential to promote the health of children with disabilities.1 Childhood poverty is associated with a range of adverse health and developmental outcomes including chronic physical health conditions, mental, behavioral, and developmental disorders (MBDDs) and early mortality.2, 3 Children with disabilities who live in low-income families are one of the most disadvantaged populations, given the dual vulnerabilities associated with disability and poverty.3–5 In 2017, almost 1.2 million children with disabilities received federally administered SSI payments6; however, SSI participation rates for children have been found to vary across states,7 due in part to demographic, economic, and health factors associated with program eligibility as well as state policies.8
In the 1990s, notable policy changes to the SSI program occurred, with implications for children with disabilities. After Sullivan v. Zebley (1990), in addition to considering the specific qualifying impairments listed by SSA, the SSA began to review the functional limitations resulting from a child’s disability to determine SSI eligibility.9 The SSA also added seven MBDDs to the list of eligible child and adult medical impairments: anxiety disorders; somatoform, eating, and tic disorders; personality disorders; psychoactive substance dependence; autistic disorder and other pervasive developmental disorder; attention deficit hyperactivity disorder; and developmental and emotional disorders of newborn and younger infants.10 Further, the Personal Responsibility and Work Opportunity Reconciliation Act of 1996 (PRWORA; P. L. 104–193) refined the Sullivan definition of childhood disability, requiring “marked and severe functional limitations,” and implemented continuing disability reviews for child beneficiaries of SSI every three years if the child’s condition could improve or the likelihood of improvement is unknown. Although the Sullivan decision was associated with expanded SSI access for children, PRWORA may have resulted in fewer children meeting eligibility requirements10 and additional demands on families with children with disabilities applying for SSI benefits.11
Caring for a child with a disability is associated with economic costs to a family in the form of unpaid time spent on family-provided healthcare, lost earnings from reduced or stopped employment, higher average childcare costs, and out-of-pocket healthcare expenses; these additional costs may be compounded for families living in poverty.3, 4, 12–14 Federal income security programs such as SSI have the potential to improve the economic security, parenting, family climate, and overall health of participating families.3, 4, 7, 15, 16 SSI participation for children with disabilities has been shown to decrease poverty rates. 3, 4, 7 SSI eligibility has also been associated with improved parenting behaviors and child motor skills for families facing socioeconomic and health risks, for example, parents with less than a high school degree with low birth weight infants.15 Based on a rigorous review of evidence related, microsimulations, and application of other selection factors, a 2019 National Academies of Sciences, Engineering, and Medicine (NASEM) committee identified modifications to SSI (i.e., increasing the federal SSI benefit maximum by 1/3 or 2/3) as one of ten strategies that could reduce the United States’ (US) child poverty rate, potentially improving child health and wellbeing on a population level.3
Increasing SSI payments could be achieved at the federal level through SSI, or at the state level via State Supplementary Payment (SSP) program, which are authorized by federal SSI legislation. The SSI program legislation established a baseline level of payment to address the minimum financial needs of eligible recipients; however, the legislation allowed flexibility in addressing additional state variability in financial needs through SSP17. SSP programs allow states to provide cash payments to eligible recipients, including some individuals found ineligible for SSI due to exceeding income or asset requirements. Although research on receipt of SSI suggests favorable impacts on children and families,3, 4, 15, 16 research on SSP benefits specifically, is lacking. State variability in the amount of benefits families can receive through SSP could provide an opportunity to explore the NASEM policy option of expanding SSI payments to further reduce child poverty and improve child health.
One avenue for examining state variability is legal epidemiology, or the study of law as a factor in the cause, distribution, and prevention of disease and injury in a population.18 Legal epidemiological studies have previously been used to highlight gaps in statutory and regulatory efforts around public health issues (e.g., vaccination uptake).19 Describing the availability and amount of SSI and SSP benefits, across jurisdictions and over time, to support families of children with disabilities may be a first step toward evaluating the NASEM’s proposed modification to SSI as a potential poverty-alleviation and health improvement tool.
The current study describes data from two longitudinal legal datasets that include statutes and regulations governing SSI and SSP, with respect to children with disabilities. We focused on the period from 1996 to 2018.
Methods
Background Research and Question Development
We used public health law research methods18 to create two longitudinal legal datasets, the first characterizing the laws (statutes and state agency regulations) governing the federal SSI program and the second looking at SSP programs in the 50 states and District of Columbia (i.e., 51 jurisdictions).18, 20 After conducting preliminary legal research and a literature review, two research attorneys independently drafted memoranda describing the statutes and regulations relevant to SSP in five jurisdictions each. Based on this ten-jurisdiction sample, we developed a question set to observe the measurable features of the law. The full research team (including subject matter experts) reviewed the question sets and developed targeted search strings and keyword searches to capture relevant laws. Research attorneys then used WestlawNext, LexisNexis, state legal databases, and the SSA website to compile a comprehensive list of legal citations and amendments from January 1, 1996, to November 1, 2018. In jurisdictions with few or no relevant provisions, research attorneys reviewed online secondary sources to confirm.
Inclusion and Exclusion Criteria
The federal SSI dataset includes laws that govern the federal definition of a “child,”, the disability criteria for eligible children, the federal application, parental income requirements, and the monthly benefit rates. The state SSP dataset includes laws that regulate the availability of optional state supplementary payments, eligibility of children with disabilities, administration of the SSP program, state application forms, income eligibility, living arrangements, SSP payment amounts, interim cash assistance, and application for other benefits as a condition of continued SSP enrollment. To be included in the dataset, the SSI or SSP law had to be in effect at any date during the study period.
Laws governing the mandatory state supplement1 were excluded because of their inapplicability to children within our study period. Researchers also excluded laws covering children who were only considered eligible by the state because of blindness, laws pertaining to resource exemptions and exclusions from countable income, state medical assistance programs, and laws that did not apply to children. Laws related to the income of “essential persons,” or live-in caretakers, were excluded, but laws deeming parental income to children (i.e., laws determining how much parental income and resources counted toward child SSI eligibility) were included. Agency policies were not included.
Collection and Coding of Laws
For relevant laws, two researchers independently reviewed statutory and administrative history information to identify and record amendments over time, noting whether each change was substantive or not. A “substantive” change is one that affected the response to one or more coding questions (e.g., increase or decrease in payment amount). After identifying relevant provisions, researchers used publicly available sources to obtain the text of each iteration of the law. To create the federal SSI dataset, researchers collected the relevant law from the SSA website. Each state’s legal dataset was redundantly built and coded by two attorney researchers. Coding divergences2 were resolved after discussion with the legal research team, with a supervising attorney arbitrating any outstanding discrepancies.
Data Abstraction
For this analysis, we focused on a subset of the variables included in the full legal datasets. From the federal SSI legislation, we examined the maximum monthly benefit amount potentially available to eligible individuals, coded as the dollar amount listed in the legislation. From the state SSP dataset, we examined four key variables: whether the jurisdiction offered any state supplemental payments (e.g., for adults or for children), whether children were eligible for the state supplemental payments, whether the law specified what type(s) of disability deemed a child eligible or ineligible for benefits, and information about the SSP benefit level. Specific data abstracted about the benefit level indicated if the jurisdiction defined the maximum benefit level as an amount or as a formula (or if the maximum benefit level was not codified into law). For laws that specified amounts, the exact dollar value was coded. For laws that specified formulas, six categories were developed to capture all variations observed in the laws over time, based on combinations of the SSI/Federal Benefit Rate, a state-determined standard of need, assistance, or benefit, and countable income. The full research protocols, codebooks and datasets are available at http://bit.ly/FederalSSI and at http://bit.ly/SSPprograms.
Results
The number of jurisdictions offering State Supplementary Payment (SSP) programs was relatively stable between 1996 and 2018, with a few inflection points, Figure 1. The number of jurisdictions offering SSP benefits to eligible individuals increased from 39 jurisdictions in 1996 to 45 by the end of 2018, with new jurisdictions adding SSP benefits in 1999 (Texas), 2004 (New Mexico, Utah), 2005 (Nevada, Oregon), and 2006 (Kansas). Although South Carolina offered SSP benefits in 1996, the jurisdiction stopped offering SSP benefits between July 1997 and March 2001 and then resumed the benefits through 2018. The number of jurisdictions that expanded their SSP to children also remained relatively steady during the study period. Twenty jurisdictions offered SSP to eligible children in 1996. From 1996 to 2018, three additional states deemed children eligible (Kentucky in 2002, Utah in 2004, and Oregon in 2011). Therefore, as of November 1, 2018, SSP was available to children with disabilities in 23 of the 45 jurisdictions offering SSP benefits. At no point during the years covered was a child’s SSP eligibility dependent upon the type of disability.
FIGURE 1.
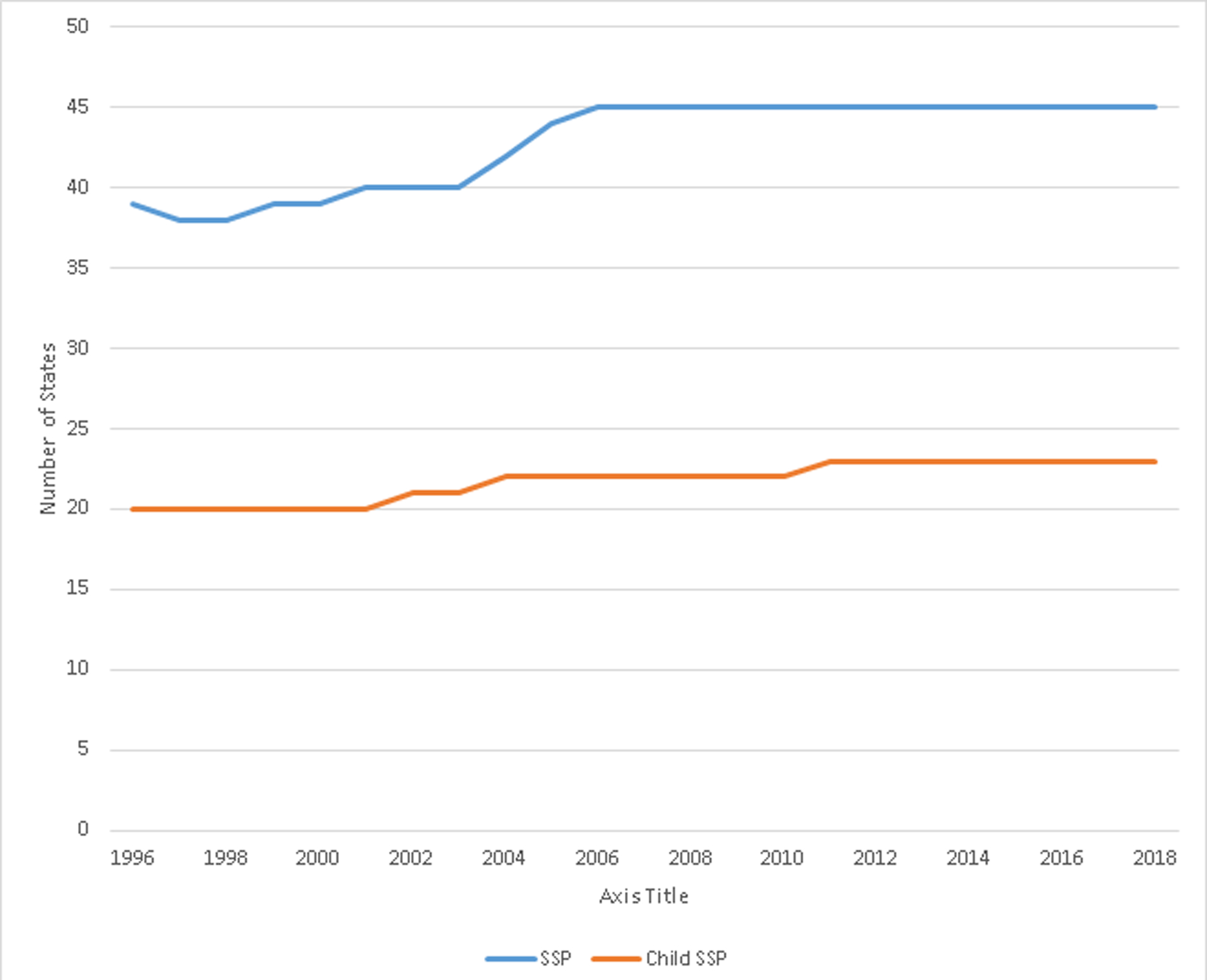
Number of United States (U.S.) Jurisdictions (50 U.S. States and District of Columbia) Providing State Supplementary Payment (SSP) Programs Overall and With Provisions for Children, 1996–2018
Between 1996 and 2018, SSI benefit amounts under federal law increased from a maximum monthly benefit amount for a single individual of $470 in 1996 to $750 in 2018. Of the 20 jurisdictions that offered SSP for children in 1996, four jurisdictions (Illinois, Maine, Montana, Rhode Island) listed monthly SSP amounts in their codified laws, and six jurisdictions listed formulas for calculation of SSP amounts (California, Hawaii, Idaho, New York, Vermont, Wisconsin). Of the 23 jurisdictions that offered SSP for children in 2018, 16 listed either a specific payment amount (7 states; Illinois, Maine, Montana, Pennsylvania, Rhode Island, Utah, Washington) or a formula for payment calculation (9 states; California, Colorado, Hawaii, Iowa, Kentucky, New York, Oklahoma, Vermont, Wisconsin). In addition, Idaho listed both a payment amount and formula, and Massachusetts referred to their state website for payment standards rather than listing a specific amount in the law. The most common formula for payment calculation in 2018 (for six of the nine states specifying a formula) was based on subtracting income from a jurisdiction-determined standard of assistance. Between 1996 and 2018, SSP amounts remained constant or decreased over time for the majority of jurisdictions. Only in Washington did benefit amounts increase over time and then stabilize. The benefit amounts for individual monthly payments ranged from $8–64.35 in 1996 to $3.13–60.43 in 2018, Figure 2. In 2018, three states (Idaho, Indiana, New York) required recipients to apply for other benefits as a condition of continued SSP enrollment.
FIGURE 2.
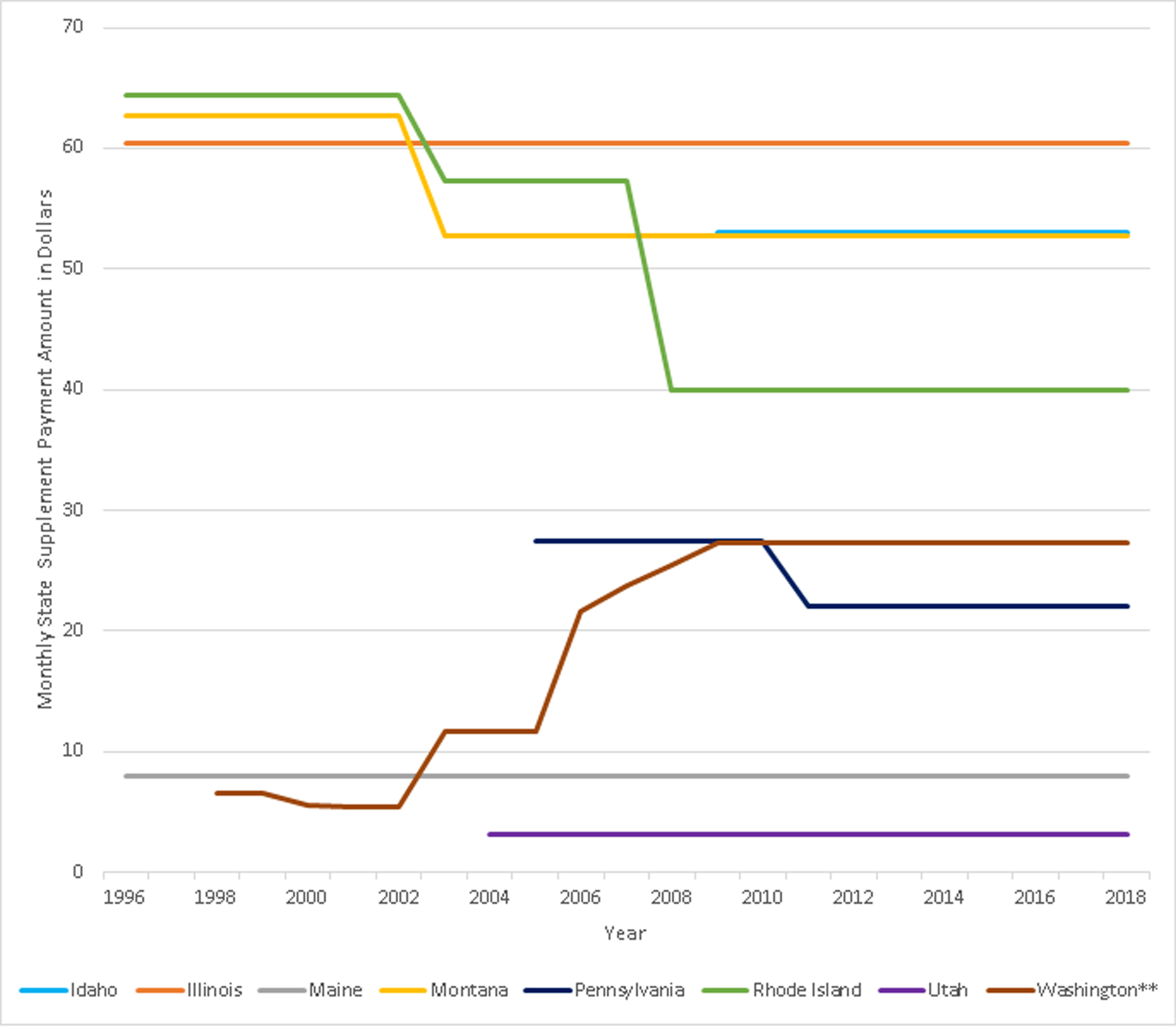
State Supplementary Payment (SSP) Program Amounts* Over Time in the 8 United States Jurisdictions that List Payment Amounts in their Laws, 1996–2018
*Only jurisdictions with SSP payment amounts listed in the codified law were included.
** Any change in the calendar year lasting more than 6 months was considered the payment level for that year; two changes are not captured by this graphic for Washington (7/1/2000–10/31/2000: $6.55 and 11/1/2000–4/30/2001: $2.45).
As a proxy to assess the degree of alignment between NASEM’s suggested expansion of SSI benefit levels and codified law, we calculated the total maximum benefits that an eligible child might receive in 2018 by summing the federal SSI monthly maximum individual benefit ($750) and the SSP amounts among the eight states listing payment amounts in their laws. This calculation allowed us to examine whether any jurisdiction, based on combined SSI and SSP amounts, would equal NASEM’s proposed SSI payment increase of 1/3 ($997.50 in 2018) or 2/3 ($1245 in 2018). Illinois had the highest combined monthly maximum payment amount of $810.43 among jurisdictions that listed SSP amounts in their laws in 2018, Figure 3. Formulas for SSP calculation could not be included in this analysis.
FIGURE 3.
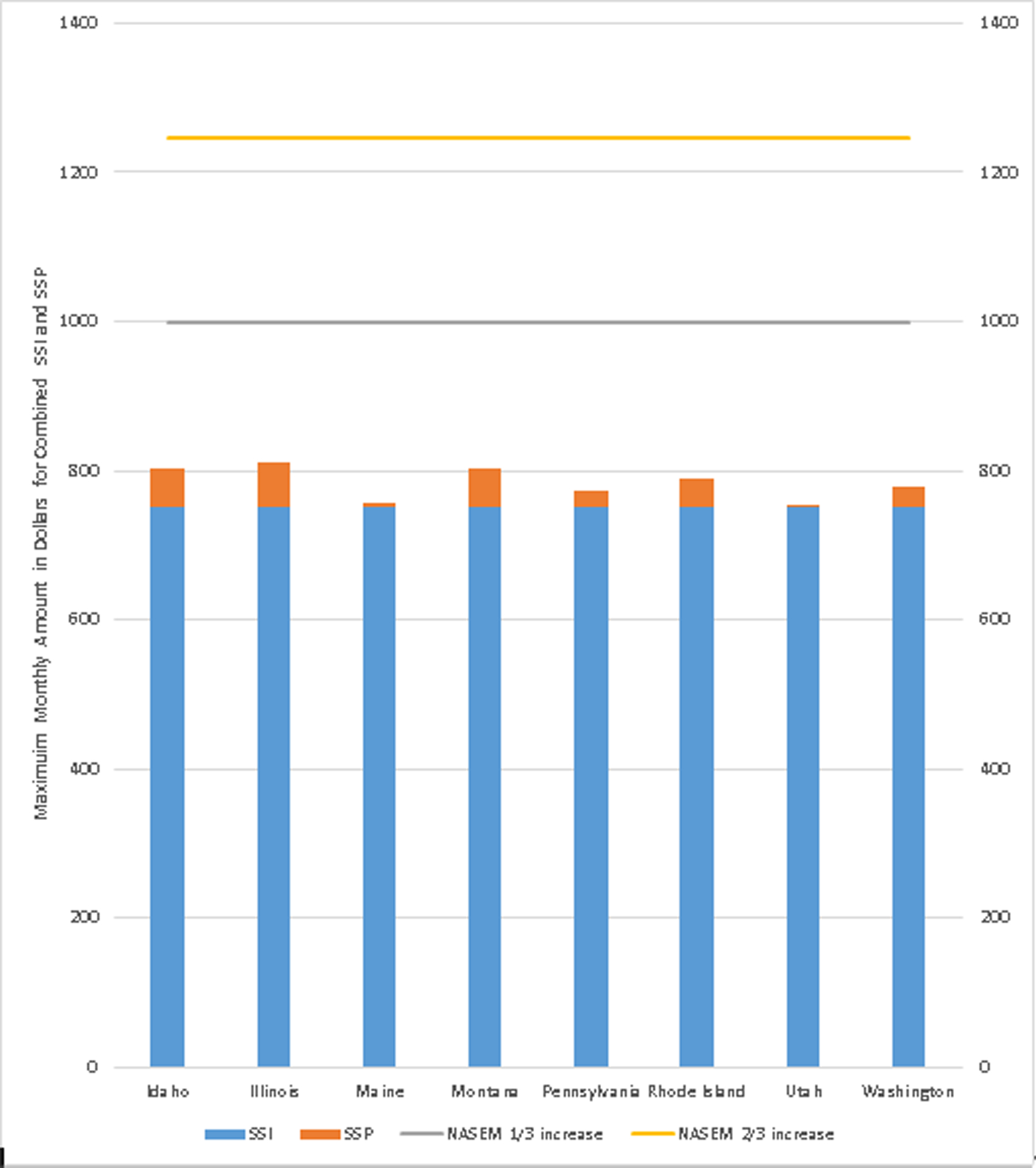
Combined 2018 Maximum Supplemental Security Income (SSI) and State Supplementary Payments (SSP) in the 8 United States Jurisdictions that List Payment Amounts in their Laws * Relative to the National Academies of Sciences Engineering and Medicine (NASEM) Proposed SSI Modifications
*Only jurisdictions with SSP payment amounts listed in the codified law were included. A NASEM SSI payment increase of 1/3 was equal to $997.50 in 2018 and 2/3 $1245 in 2018.
Regional variations in 2018 SSP laws that apply to both children and adults were noted, Figure 4. Jurisdictions with state mandates that included child eligibility of SSP were more concentrated in the Northeastern and Western jurisdictions. Nine jurisdictions in the West, seven jurisdictions in the Northeast, five jurisdictions in the Midwest, and one each in the Southwest and Southeast had state mandates for SSP that were inclusive of children.
FIGURE 4.
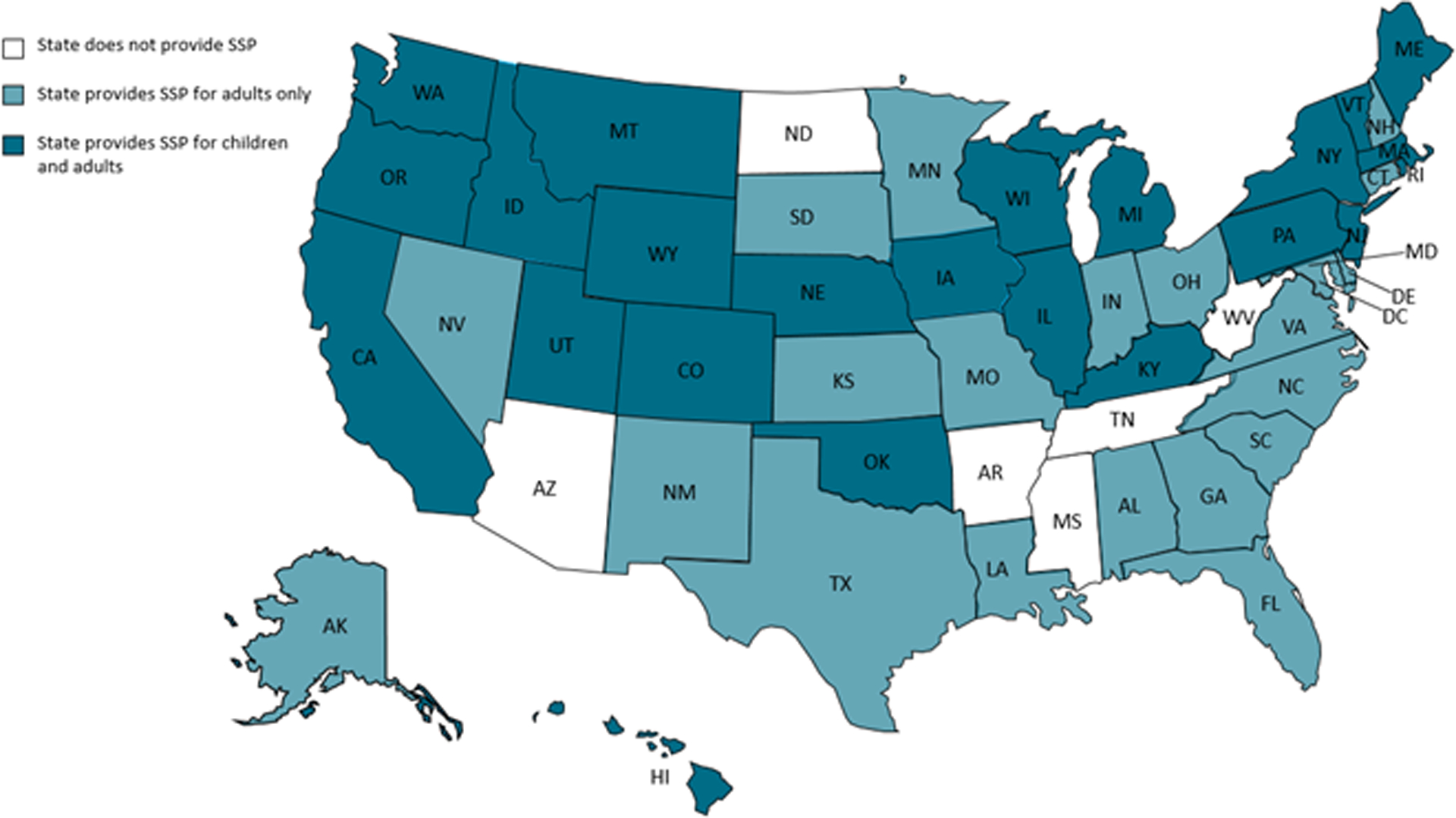
United States Map of State Supplementary Payment (SSP) Programs for Adults Only and for Adults and Children, 2018
Discussion
Children with disabilities in low-income households are one of the most disadvantaged populations when compared to their higher income peers without disabilities.3–5 SSI payments have been shown to raise half of child beneficiary households above the poverty line.4 SSP programs give jurisdictions the authority to provide additional benefits for children with disabilities and their families. Less than half of U.S. jurisdictions offered SSP benefits to children in 2018, with an increase of three states from 1996 (20 states) to 2018 (23 states). Among those jurisdictions providing SSP benefits to children, SSP amounts were small (ranging from $8–64.35 in 1996 and $3.13–60.43, in 2018). Payments have remained stable or decreased over the past twenty years, for seven out of the eight jurisdictions with codified SSP amounts, despite cost of living increases over time. When we combined SSP with SSI maximum benefit amounts in the eight states listing payment amounts in their codified law, benefit amounts were $187.07- $244.37 below NASEM’s proposed one-third SSI modification or $434.57-$491.37 below the proposed two-third increase to SSI benefits. NASEM’s simulation models suggest that more families would be lifted out of poverty, and outcomes for children with disabilities would likely improve if SSI-related benefits were raised to the levels proposed by NASEM (through SSI, SSP, or both).3
Our study identified that more US jurisdictions in the Northern and Western regions, in 2018, provided SSP for eligible children in their codified laws in comparison to jurisdictions in the Southern and Midwestern regions. In our study, the number of jurisdictions providing SSP in general or SSP for children increased by six and three jurisdictions, respectively, over our 22-year study period. Although our study period included notable federal policy changes that could have influenced jurisdictions’ decisions to enact SSP laws for children, the relationship between changes in federal policies not specific to SSI and jurisdiction-level decisions to enact SSP for children remains unclear. Future research could evaluate the potential impact of federal policies on SSP and other income security programs that coincided with the inflection points noted in our analysis of SSP for children (e.g., 2002, 2004, and 2011). Examination of jurisdiction-level SSP-related policies and implementation procedures, along with factors external to the programs (e.g., state expansion of Medicaid), could identify levers for using SSI and SSP to improve the health of children with disabilities.
Given variability in availability of SSP benefits for children, children with disabilities in low-income households may need additional options for support and connections to other income security, healthcare, and educational programs (e.g., Medicaid, Supplemental Nutrition Assistance Program, special education services) to achieve their full health and development potential.4 Three of the 23 jurisdictions providing SSP for children included a legal requirement that SSP applicants also apply for other state benefits as a condition of SSP eligibility, suggesting connections between programs may also vary across jurisdictions. Future research could investigate if mandatory requirements to apply for other benefits create barriers for families, leading to decreased SSP program participation, or if such requirements remove barriers to eligible families receiving benefits from other programs. On the federal level, SSI regulations require applicants to apply for all other benefits for which one may be eligible.21 The Promoting the Readiness of Minors in Supplemental Security Income (PROMISE) demonstration projects are an example of a collaborative effort that aims at further addressing and evaluating these connections between federal programs to better support the educational and vocational needs of youth with disabilities (and their families) as they transition into adulthood.22 PROMISE programs provide case management for the youth participants in SSI and their families, benefits counseling and financial literacy training, vocational support and paid or unpaid work experiences, parent support programming, and secondary school supports.22 Implementation data from PROMISE highlight the importance of: interagency collaborations and service coordination for youth receiving SSI, professional development for staff serving families and youth, person-centered supports and services for youth and families to increase engagement and program participation, and investments in time and commitment to consistency for engaging families .23, 24
Although we initially sought to identify whether jurisdictions determined child SSP eligibility based on physical conditions, MBDDs, or both, none of the states that offered SSP differentiated on disability type. Stigma against MBDDs persists, and even with parity laws, gaps remain in service access among children with MBDDs.25 Determinations that children with MBDDs qualify for SSI have decreased over time, 2004–2013.10 In addition, considerable variability could exist in both the state rates of SSI-related eligibility determinations for childhood MBDDs and the state rates of children from low-income households who received SSI benefits for MBDDs.26 Thus, even if codified laws do not differentiate SSP eligibility based on type of disability (as in all of the 23 jurisdictions in this analysis that offered child SSP in 2018), state-specific determination practices could lead to differences in eligibility based on disability type. Hoagwood and colleagues suggest that many children with MBDDs do not receive the SSI benefits they may be eligible to receive in some jurisdictions due to state-level differences in the determination and implementation processes (e.g., the disability evaluation and application process, and policies on eligibility for multiple income security programs).26 Future research could explore factors that affect variability in SSI or SSP implementation for children with MBDDs and associations between SSI or SSP participation by children with disabilities and health outcomes.
These data represent the first longitudinal legal epidemiological review of SSI and SSP laws for children with disabilities within 51 jurisdictions across 22 years. We used a double-coding methodology with consensus agreement and multiple state legal databases to ensure the validity of results. However, several limitations are also important to consider. First, this legal epidemiological study captured only codified laws, which do not describe external factors that influence state implementation of SSP programs. Certain regulatory texts were inaccessible in several states, from legal research databases and state legislative or administrative websites (Colorado, Hawaii, Idaho, Iowa, Kentucky, Oklahoma), particularly in the 1990s or early 2000s. Where the legal text was inaccessible, we did not code the jurisdiction as providing SSP. Each jurisdiction varied in their recordkeeping of regulatory amendments, some relying on inaccessible internal manuals to house their SSP eligibility and implementation rules. Therefore, jurisdictions might have required an application, set an income threshold variable from the SSI limit, or established other eligibility criteria, but did not legislate these requirements within the law and therefore this information could not be included in our data. Where we were able to obtain legal text indicating the availability of SSP benefits, we used secondary sources (e.g., SSA State Supplementation reports and state administrative agency websites and databases) to confirm findings. Second, laws often did not state explicitly whether children were included in SSP. Where the jurisdiction’s legal text did not distinguish whether children were eligible for SSP benefits, we coded the jurisdiction as offering SSP benefits to children as SSI legislation allows for the “disabled” category to include children. As such, our tally of jurisdictions may be an underestimation (due to inaccessibility of the legal text), or overestimation (due to including states in which the law does not distinguish between adults and children) of the number of jurisdictions with SSP available for children. Future work could further validate these findings by conducting mixed methods research within the jurisdictions where SSP availability or eligibility is not regulated through state statutes and regulations. Third, although 23 jurisdictions provided SSP for children, only 18 jurisdictions provided information on SSP amounts or formulas in their laws. SSP amounts may be higher or lower than we were able to ascertain with our review of laws and regulations. Therefore, additional research examining SSP amounts and economic analyses examining relationships between SSP and cost of living over time could move us closer to evaluating NASEM’s policy option for expanded SSI. Finally, potential explanatory variables were beyond the scope of this project (e.g., whether children receiving SSP were automatically enrolled in other income security programs such as Medicaid or whether other benefits such as Temporary Assistance for Needy Families (TANF) varied relative to SSP amounts).
Despite SSI’s availability in all jurisdictions as a federal law governing the entire US, SSP availability for children has not increased markedly over the last 20 years. Fewer than half of US jurisdictions mandate SSP availability to children with disabilities. Our initial exploration of SSI-related policies as a tool for improving the economic stability of children with disabilities and their families suggests that current SSPs, in combination with SSI, are not yet aligned with the recent evidence base used by NASEM3 that suggested increased SSI amounts (by 1/3 and 2/3) could offset some of the additional financial costs of caring for a child with disabilities living in poverty. SSI and SSP are one type of program that supports children at economic and health risk; understanding more about how this program reaches children and works in combination with other federal and state income security programs may help identify policies and strategies that further support children with disabilities in low-income households.
Implications for Policy & Practice.
In 2018, 23 of 51 jurisdictions legally mandated that State Supplementary Payment (SSP) programs were available for children; additional research could examine jurisdiction-level factors that facilitate or impede the implementation of SSP for children.
If SSI and SSP benefits are not at sufficient levels to support optimal health of children with disabilities in low-income households, such families may need additional options for support and connections to other income security, healthcare, and educational programs; additional research could identify policy opportunities and barriers to connecting these programs on federal and state levels.
Future research could involve mixed methods research within individual jurisdictions to determine jurisdiction-level decisions to implement SSP and set payment amounts as a means to further NASEM’s SSI expansion for poverty-reduction and health-improvement for children by expanding their amounts and reach for children with disabilities.
Next steps to improve our understanding of the impacts of SSI and SSP for children may include examining how codified laws translate to both implementation of SSP on an administrative agency level (according to internal procedures) in the form of the receipt of payments to families and the effects of these laws on child and family outcomes. Additional research could examine the relationship between SSI and SSP and the eligibility requirements as codified in legal texts across the United States.
Funding
This manuscript was supported by Cooperative Agreement Numbers NU38OT000307 and NU38OT000141 awarded to ChangeLab Solutions and funded by the Centers for Disease Control and Prevention. This research was supported in part by an appointment to the Research Participation Program at the Centers for Disease Control and Prevention administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the U.S. Department of Energy and CDC.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. This document was coauthored by a Cherokee Nation Assurance contractor in the Public Health Law Program (PHLP) in the Center for State, Tribal, Local, and Territorial Support at the US Centers for Disease Control and Prevention (CDC).
Footnotes
Author disclosure statement
The authors declare no conflict of interest.
A 1973 federal amendment to the SSI law required that states must pay mandatory supplemental payments to individuals who are aged, blind, or disabled who were transferred in 1974 from the state to the federal SSI program. Mandatory payments only applied to those who were receiving SSI payments in 1973; therefore, any child in our study years would not be eligible for those mandatory payments.
The rate of divergences ranged from 14.9– 18.9%.
References
- 1.Kelleher KJ, Boat TF, Houtrow AJ, Hoagwood K. Poverty and Supplemental Security Income: can DBPs take a more active role. J Dev Behav Pediatr. 2016;37:267–268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pascoe JM, Wood DL, Duffee JH, Kuo A, Committee on Psychosocial Aspects of Child and Family Health. Mediators and adverse effects of child poverty in the United States. Pediatrics. 2016;137:e20160340. [DOI] [PubMed] [Google Scholar]
- 3.National Academies of Sciences Engineering and Medicine. A Roadmap to Reducing Child Poverty. Washington, DC: The National Academies Press; 2019. [PubMed] [Google Scholar]
- 4.Romig K SSI: A Lifeline for Children with Disabilities. Washington, DC: Center on Budget and Policy Priorities; 2017. [Google Scholar]
- 5.Parish SL, Cloud JM. Financial well-being of young children with disabilities and their families. Soc Work. 2006;51:223–232. [DOI] [PubMed] [Google Scholar]
- 6.Social Security Administration. SSI Annual Statistical Report, 2017. Baltimore, MD: Social Security Administration; 2018. [Google Scholar]
- 7.National Academies of Sciences Engineering and Medicine. Fostering Healthy Mental, Emotional, and Behavioral Development in Children and Youth: A National Agenda. Washington, DC: National Academies Press; 2019. [PubMed] [Google Scholar]
- 8.Sevak P, Bruns S. What Have We Learned About SSI Receipt Among Children? Washington, DC: Mathematica Policy Research; 2018. [Google Scholar]
- 9.Garrett AB, Glied S. The effect of US Supreme Court ruiling Sullivan v. Zebley on child SSI and AFDC enrollment National Bureau of Economic Research. 1997;Working paper 6125. [Google Scholar]
- 10.National Academies of Sciences Engineering and Medicine. Mental Disorders and Disabilities Among Low-Income Children. Washington, DC: The National Academies Press; 2015. [PubMed] [Google Scholar]
- 11.Wilcox BL, Colman RA, Wyatt JM. The Personal Responsibility and Work Opportunity Reconciliation Act of 1996 In: Bottoms BL, Kovera MB, McAuliff BD, eds. Children, Social Science, and the Law. New York, NY: Cambridge University Press; 2002. [Google Scholar]
- 12.Anderson D, Dumont S, Jacobs P, Azzaria L. The personal costs of caring for a child with a disability: a review of the literature. Public Health Rep. 2007;122:3–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Romley JA, Shah AK, Chung PJ, Elliott MN, Vestal KD, Schuster MA. Family-provided health care for children with special health care needs. Pediatrics. 2017;139:e20161287. [DOI] [PubMed] [Google Scholar]
- 14.Stabile M, Allin S. The economic costs of childhood disability. Future Child. 2012;22:65–96. [DOI] [PubMed] [Google Scholar]
- 15.Guldi M, Hawkins A, Hemmeter J, Schmidt L. Supplemental Security Income and Child Outcomes: Evidence from Birth Weight Eligibility Cutoffs. Cambridge, MA: National Bureau of Economic Research; 2018. [Google Scholar]
- 16.Duggan MG, Kearney MS. The impact of child SSI enrollment on household outcomes. J Policy Anal Manage. 2007;26:861–886. [Google Scholar]
- 17.Rigby DE. State Supplementation Under Federal SSI Program. J Soc. Sec. Bull 1974;37:21. [Google Scholar]
- 18.Burris S, Ashe M, Levin D, Penn M, Larkin M. A transdisciplinary approach to public health law: the emerging practice of legal epidemiology. Annu Rev Public Health. 2016;37:135–148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hoss A, Meyerson BE, Zimet GD. State statutes and regulations related to Human Papillomavirus vaccination. Hum Vaccin Immunother. 2019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Presley D, Reinstein T, Burris S. Resources for Policy Surveillance: A Report Prepared for the Centers for Disease Control and Prevention Public Health Law Program: Temple University Legal Studies Research Paper No. 2015–09.
- 21.Social Security Administration. Annual report of the Supplemental Security Income Program. Baltimore, MD: Social Security Administration; 2018. [Google Scholar]
- 22.Honeycutt T, Livermore G. Promoting Readiness of Minors in Suppmental Security Income (PROMISE): The Role of PROMISE in the Landscape of Federal Programs Targeting Youth with Disabilities. Washington, DC: Mathematica Policy Research; 2018. [Google Scholar]
- 23.Mamun A, Patnaik A, Levere M, et al. Promoting Readiness of Minors in SSI (PROMISE) evaluation: Interim services and impact report. Washington, DC: Mathematica; 2019. [Google Scholar]
- 24.Nye-Lengerman K, Gunty A, Johnson D, Hawes M. What matters: Lessons learned from the implementation of PROMISE model demonstration projects Journal of Vocational Rehabilitation. 2019;51:275–284. [Google Scholar]
- 25.Cummings JR, Lucas SM, Druss BG. Addressing public stigma and disparities among persons with mental illness: the role of federal policy. Am J Public Health. 2013;103:781–785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hoagwood KE, Zima BT, Buka SL, Houtrow A, Kelleher K. State-to-state variation in SSI enrollment for children with mental disabilities: an administrative and ethical challenge. Psychiatr Serv. 2016;68:195–198. [DOI] [PMC free article] [PubMed] [Google Scholar]