

Abstract
SARS-CoV-2 may cause severe respiratory failure due to massive alveolar damage. Currently, no adequate curative therapy for Coronavirus Disease 2019 (COVID-19) disease exists. By considering overall impact of COVID-19 pandemic outbreak, an increased need of extracorporeal membrane oxygenation (ECMO) support becomes evident. We report on our preliminary institutional experience with COVID-19 patients receiving venovenous ECMO support.
Keywords: COVID-19, pandemic, ARDS, extracorporeal membrane oxygenation
A new betacoronavirus, named SARS-CoV-2, which causes a severe acute respiratory syndrome, designated as Coronavirus Disease 2019 (COVID-19), emerged in China in December 2019.1–8 The virus has been designated as a pandemic by the World Health Organization (WHO), on March 11, 2020.1 As of April 5, 2020, COVID-19 has been confirmed in 208 countries and currently involves 1,133,758 cases globally with 62,784 deaths.1 The majority of infections has been reported initially in China followed by Italy, Spain, Iran, and the United States.1
World Health Organization interim guidelines for the management of suspected COVID-19 recommend administering venovenous (VV) extracorporeal membrane oxygenation (ECMO) to eligible patients with COVID-19–related acute respiratory distress syndrome (ARDS) in expert centers .1,2,6–8
We report on our preliminary institutional experience with COVID-19 patients receiving VV ECMO support (Tables 1–3).
Table 1.
Demographics and Origin of Patients with Confirmed SARS-CoV-2 Infection Requiring ECMO Support

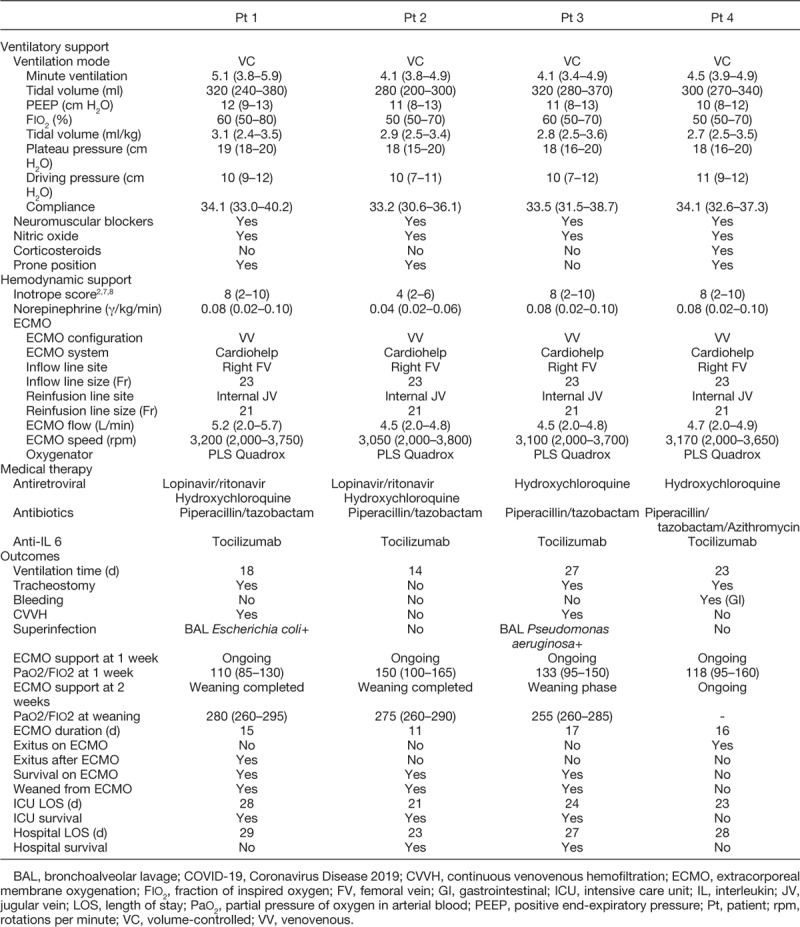
Table 3.
Mechanical Ventilation, ECMO Support, and Pharmacological Management Plus Outcomes of VV ECMO COVID-19 Patients
Study Population
Coronavirus Disease 2019 infection was confirmed by usage of polymerase chain reaction tests on either nasopharyngeal or lower respiratory tract swab samples ordered at intensive care unit (ICU) admission.
Consideration of ECMO was based on the presence of severe respiratory failure (Murray score >3.0 or pH <7.20 under protective ventilation2,6–8) with sustained clinical deterioration despite optimal conventional treatment and refractory prone positioning. This has been in accordance with Extracorporeal Life Support Organization (ELSO) guidelines document for the adult patient with COVID-19.2,6–8
Diffuse bilateral lung injury by SARS-CoV-2 was confirmed by chest x-ray or computed tomography (CT) scan in all patients3–5,7 (Figure 1).
Figure 1.
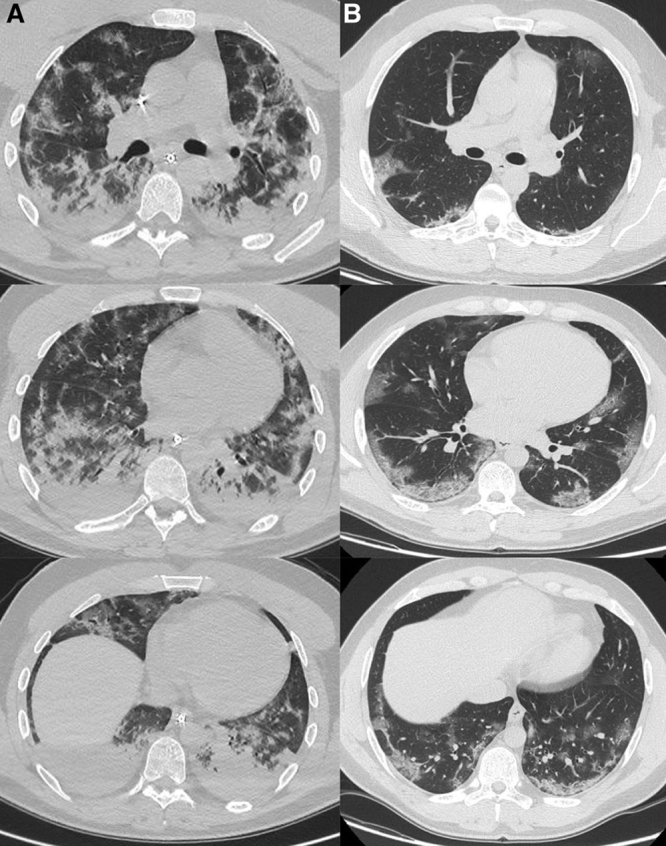
COVID-19 respiratory disease. Computed tomography scan axial view (upper, medium, and lower pulmonary lobes sections). A: Pre-ECMO pulmonary involvement (evidence of multilobular and subpleural ground-glass opacities and consolidation). B: Post-ECMO pulmonary involvement (evidence of resolution). COVID-19, Coronavirus Disease 2019; ECMO, extracorporeal membrane oxygenation.
Aggressive mechanical ventilation (peak or plateau airway pressure >30 cm H2O or fraction of inspired oxygen [Fio2] >0.8) for more than 7 days, uncontrolled active bleeding, severe comorbidity, multiple organ failure, sepsis, disseminated intravascular coagulation, age >65 years, and neurologic damage were used as contraindications for VV ECMO institution.2,7,8
Patients have been considered for ECMO by a multidisciplinary team consisting of experts from Anesthesiology and Intensive Care, Cardiac Surgery, Cardiology, and Infectious Diseases.
The study has been approved by our institutional review board. Informed consent was not required for ECMO treatment, as the use of mechanical support was considered a rescue therapy in all patients.
Extracorporeal Membrane Oxygenation Support Setting
The ultracompact Cardiohelp (Getinge, Maquet-Cardiopulmonary AG, Rastatt, Germany) has been adopted as ECMO system. For inflow, the right femoral vein was cannulated percutaneously using the Seldinger technique with a 38 cm long, 21–23 Fr heparin-coated cannula (Bio-Medicus NextGen, Medtronic Inc., Minneapolis, MN). For reinfusion (outflow), a 15 cm long, 15–17 Fr heparin-coated cannula (Bio-Medicus NextGen, Medtronic Inc.) was used, implanted into the right internal jugular vein.
All the components of the ECMO system and tubings were heparin coated (Bioline coating; Getinge, Maquet-Cardiopulmonary AG), and systemic anticoagulation was maintained using unfractionated heparin to a partial thromboplastin time of 1.5 normal.2,6,7
Pressures on the ECMO circuit, blood gas analysis, general laboratories, and complete blood coagulation study were also monitored daily. Echocardiography was not performed routinely.
Patient Management and Weaning from Extracorporeal Membrane Oxygenation
After cannulation, patient management was optimized to minimize further ventilator-induced lung injury (VILI).2,6–8 Regarding oxygenation, ECMO blood flow was maximized to reduce the Fio2 less than 0.6 and maintain hemoglobin saturation more than 85%. Positive end-expiratory pressure (PEEP) was maintained above 8 cm H2O. If severe hypoxemia (Pao2, <60 mm Hg) still subsisted, the threshold for red blood cell transfusion was elevated from 7.0 to 9.0 g/dl. The threshold for prophylactic platelet transfusion was 35.000/μl, whereas the targeted post-transfusion goal was 100,000/μl in the presence of active bleeding. Regarding CO2 removal, sweep gas flow was maximized to allow a normal pH, small tidal volumes (<6 ml/kg/predicted body weight), and plateau pressures less than 25 cm H2O. Paralysis and sedation were maintained.
After improvement of native lung function (Fio2 <0.5, PEEP <10 cm H2O, peak inspiratory pressure in pressure-controlled ventilation [PIP] <25 cm H2O), ECMO flow was gradually reduced to 2.0 L/min.2,6–8 Sweep gas flow was then tapered and finally shut off for 40 minutes. If blood gases remained stable for more than 6 hours, the ECMO system was removed, and decannulation was carried out.
Statistical Analysis
Variables are reported as median and interquartile ranges. For statistical analysis, we used SPSS 24.0 (SPSS, Inc., Chicago, IL).
Results
As of March 1, 2020, during COVID-19 pandemic outbreak, 59 consecutive adult patients with confirmed infection were admitted at our Cardio-Thorac-Vascular Department (out of >300 confirmed cases throughout S. Orsola University Hospital, Bologna; Tables 1, 2).
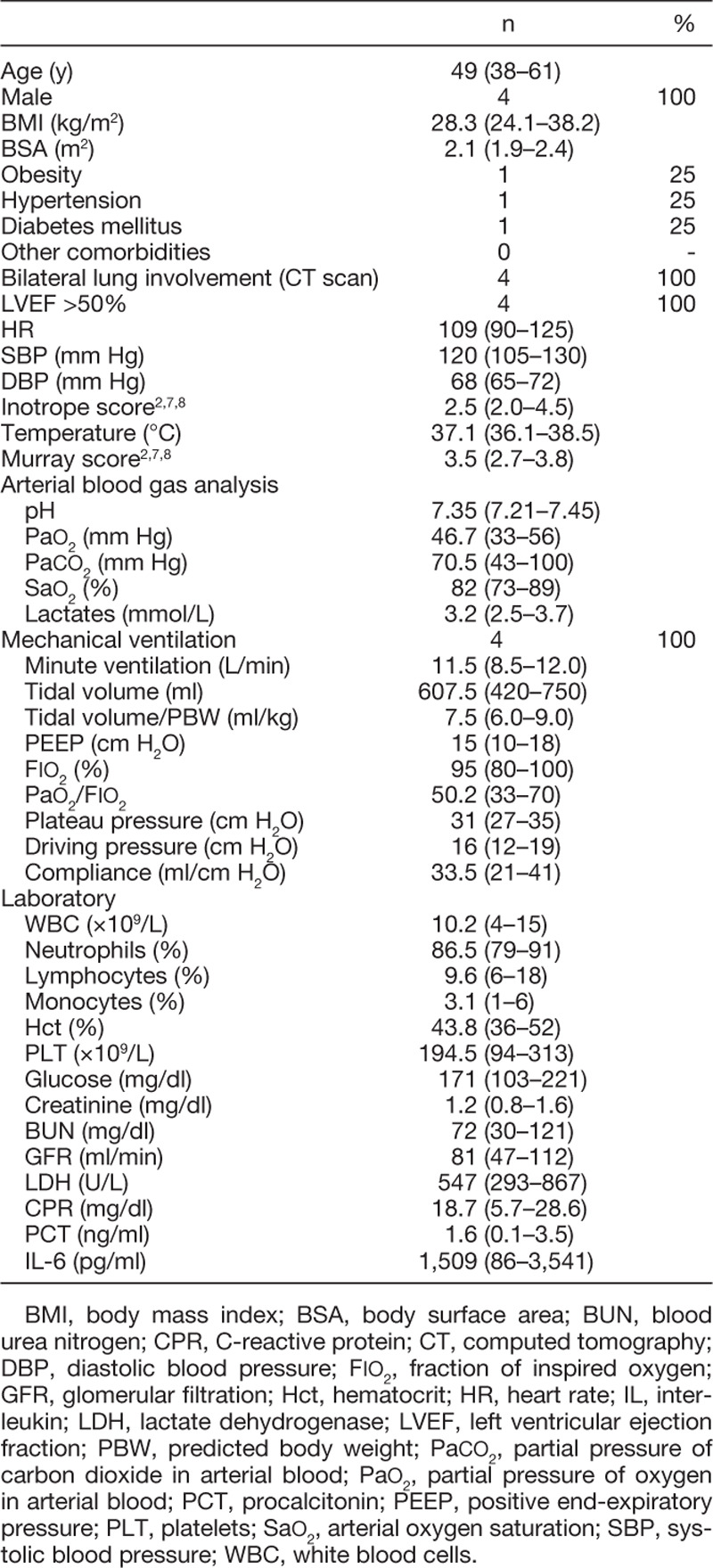
Table 2.
Clinical Features at Admission of SARS-CoV-2 Patients
All patients suffered severe respiratory failure and were admitted to our ICU. Four of them were referred for ECMO establishment (Table 1). Our ECMO population had no severe comorbidities.
The clinical course consisted of rapid in-hospital deterioration with early ICU admission for ventilatory support. The Murray score2,6–8 was used to evaluate respiratory failure severity before VV ECMO implantation. In all patients, alternative rescue therapies such as prone position and inhaled nitric oxide (NO) were used before ECMO referral.
Intensive care unit survival has been 75% (Table 3). Three patients were weaned from VV ECMO (75%). Computed tomography scan and chest x-ray typical ground-glass features and consolidations decreased (Figure 1). However, the first weaned patient suffered acute recurrence of pneumonia and eventually died on day 9 after VV ECMO removal. The second weaned patient has been successfully extubated and fully mobilized thus joining a rehabilitation care. The third weaned patient is still intubated and on inhaled NO with a slight resolution of the pulmonary disease.
The remaining patient suffered severe gastrointestinal bleeding, while on ECMO, with high transfusion requirements, namely, of red blood cells (RBC/day 0.57 [0.30–0.10]) and platelets (PLT/day 0.45 [0.10–0.70]), which resulted to be fatal (Table 3).
Neither oxygenator failure nor ECMO circuit failure occurred. No neurologic complications occurred.
In all patients, lung-protective ventilation was sustained during ECMO support and maintained in the three weaned patients on the first day after ECMO cessation. The level of PEEP was gradually decreased during weaning from ECMO and afterward during weaning from mechanical ventilation. Percutaneous tracheostomy was performed in three patients.
All patients received tocilizumab and hydroxychloroquine (Table 3).3,4 Lopinavir/ritonavir antiviral therapy was used in two patients. Piperacillin/tazobactam antibiotic prophylaxis was used in all patients while azithromycin was adopted, additionally, in one.3,4,7 Corticosteroids were used in a single case while on ECMO.
Low dosage of vasoactive drugs (norepinephrine) infusion and consecutive positive fluid balance was frequently needed during VV ECMO support (Table 3).2,7,8 Low dosage of corticosteroids have been used as anti-inflammatory agents after ECMO removal.
Conclusions
SARS-CoV-2 may cause severe respiratory failure due to massive alveolar damage.2–7 The rate of ARDS ranges from 15% to 30% among patients who require hospitalization.1,2,7
Currently, no adequate curative therapy for COVID-19 disease exists.3–7 By considering overall impact of COVID-19 pandemic outbreak, an increased need of ECMO support becomes evident.2,6–8 So far, the ELSO registry accounts 143 COVID-19 respiratory ECMO running systems worldwide, mostly being in Europe and the United States.2,8 As of April 4, 2020, Euro COVID-19 survey/study showed 253 ongoing VV ECMO patients while 52 have been successfully weaned from ECMO support.2,8
In COVID-19 patients, the initial pulmonary pattern is not similar to ARDS, as hypoxia is prevalent and pulmonary compliance is generally high.3–7 The main finding is hypoxic vasoconstriction. The lungs are inflated and increasing PEEP or prone positioning does not help. Lung CT scans in those patients confirm that there are no significant areas to recruit. Moreover, high PEEP levels may compromise right cardiac filling and an increase of the need for fluid intake and/or norepinephrine.5–7
Ventilator-induced lung injury, volutrauma, barotrauma, oxygen toxicity should be avoided and “lung-protective ventilation” is the recommended strategy for COVID-19 patients.2,5–7
In addition to viral pneumonia, consequently, those patients likely have had self-inflicted VILI, due to diffusely initial type ICUs management and misunderstanding with subsequent decrease in compliance and edema in the lower lobes.4–7 Those patients present a pattern similar to ARDS and they benefit from PEEP and prone positioning.
If the conservative treatment is not effective, VV ECMO support might be considered.2,6–8 Unfortunately, ECMO infrastructures and resources are limited, globally.7,8
Our small sample of COVID-19 ECMO patients presented young age and showed no severe comorbidities but severe ARDS occurred in all of them. Thus, warm caution and thoughtful approaches for timely detection and treatment should be taken for people who are currently living in high-density COVID-19–infected areas1 to preserve life.
Footnotes
Disclosure: The authors have no conflicts of interest to report.
References
- 1.WHO: Rolling Updates on Coronavirus Disease (COVID-19). https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen. Accessed April 5, 2020.
- 2.ELSO: COVID-19 Cases on ECMO in the ELSO Registry. https://www.elso.org/COVID19.aspx. Accessed April 5, 2020.
- 3.Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N Engl J Med 2020382: 1199–1207 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Guan WJ, Zhong NS. Clinical characteristics of COVID-19 in China. Reply. N Engl J Med 2020382: 1861–1862 [DOI] [PubMed] [Google Scholar]
- 5.Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020 doi: 10.1001/jamainternmed.2020.0994. [Epub ahead of print] doi: 10.1001/jamainternmed.2020.0994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir Med 20208: 475–481 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Akar AR, Ertugay S, Kervan U, et al. Turkish Society of Cardiovascular Surgery (TSCVS) Proposal for use of ECMO in respiratory and circulatory failure in COVID-19 pandemic era. 2020. 28: Epub ahead of print doi: 10.5606/tgkdc.dergisi.2020.09293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ramanathan K, Antognini D, Combes A, et al. Planning and provision of ECMO services for severe ARDS during the COVID-19 pandemic and other outbreaks of emerging infectious diseases. Lancet Respir Med 20208: 518–526 [DOI] [PMC free article] [PubMed] [Google Scholar]