

The COVID-19 pandemic has affected all of our lives around the world. As surgeons, we proudly work on the frontlines of any local, regional, or global disaster. We care for vulnerable and injured patients in our trauma bays and our critically ill patients in the intensive care unit, regardless of their background, socioeconomic position, or COVID-19 status. During the current pandemic, we remain steadfast and dedicated to excellence in the clinical care of our patients, furthering research and evidence-informed practice while improving the surgical workplace environment by addressing issues of injustice and inequity. The COVID-19 pandemic has now forced us, as surgeons, to shift our ethical focus from individual patient-centered care to a more public health, population-centered care approach. Instead of maximizing individual patient outcomes we must seek to maximize outcomes for the greater population and society where we live and work. Although surgical and critical care societies have been appropriately creating urgently needed clinical guidelines (based on scarce but emerging data), there is little guidance regarding the ethics and equity population issues that surgeons face when working in this new era of COVID-19. As the authors each have a long history of equity work in their various fields, we propose an ethical framework in which to consider these issues affecting us, our patients, and our larger local and global communities.
Since many of us are acute care surgeons, it is important to highlight that we practice trauma-informed care (TIC), which acknowledges the high prevalence of trauma in society.1,2 Trauma has continued during the COVID-19 pandemic, unabated throughout the country. TIC is centered around the consciousness that people come into any encounter with a set of experiences that greatly affect their ability to feel safe and to interact constructively with healthcare. Physicians are trained in medical school to apply universal precautions. This means that we assume that all patients have been exposed to transmissible pathogens, as they may have been exposed to previous trauma. Thus, TIC includes a commitment to both protect physicians from the patient with appropriate personal protective equipment (PPE) while creating a healthcare encounter that protects the patient from us by avoiding retraumatization during the encounter. We pride ourselves in caring not just for the patient, but also for their families, our trainees, and ourselves while recognizing the larger historic and political structures shaping healthcare. We view TIC as the confluence of 3 overarching themes (Fig. 1). These themes are as applicable to COVID-19 disease as they are to firearm violence or other etiologies of trauma.
FIGURE 1.
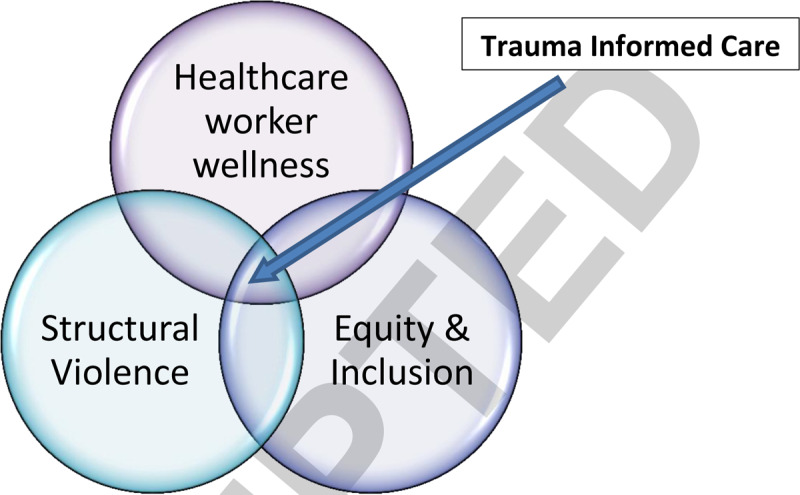
The overlapping domains of trauma-informed care.
-
1.
Healthcare worker (HCW) wellness and mitigating moral distress
-
2.
Societal issues of equity and inclusion
-
3.
Structural violence and deeper issues of structural discrimination
We, as a siblingship of surgeons and physicians, emphatically state the following:
HEALTHCARE WORKER WELLNESS
-
1.
We acknowledge the stress of working during a pandemic that increases risk to our own personal health, increases risk amongst family members and other contacts, and leads to isolation from loved ones. This sentiment has been captured very well by The New Yorker April 06, 2020 cover (Fig. 2).3,4 HCWs are forced to make difficult ethical and moral decisions under extremely challenging circumstances that can lead to moral distress. All frontline HCWs should have easy access to emotional and psychological first aid as in any disaster zone or area.5
-
2.
Nongovernmental healthcare organizations or charities assisting in disaster response should not be propagating messages of discrimination or hate, or coercing volunteer HCWs to contractually agree to such messaging.6
-
3.
All HCWs in the United States are entitled to immediate and complete protection against COVID-19 infection. There is clear evidence that SARS-CoV2 can stay aerosolized for up to 3 hours, increasing the risk of transmission, beyond droplets.7 Our position is that the current Center for Disease Control and Prevention (CDC) recommendations for SARS-CoV2 protection are inadequate, in terms of optimizing the protection of HCWs, as they are heavily influenced by resource shortages that could have been mitigated by the federal administration early and are incongruous with previous CDC recommendations of 2003 for SARS-CoV1.8,9 It is analogous to the early, false reassurances of the US Environmental Protection Agency after 9/11 about water and air safety at Ground Zero, which ultimately endangered the lives of frontline emergency and HCWs.10 Similarly, we feel that the current CDC recommendations place HCWs at an increased risk of preventable illness and even death. We believe that these guidelines, which could mean the difference between the life and death of HCWs, their patients, or their families, should be biased heavily toward maximal protection versus less effective or unproven compromises.
-
4.
As such, we call for the President of the United States to both invoke the Defense Production Act by executive order and enforce it to direct the nationwide manufacture in the interest of the American people of (1) COVID-19 test kits, (2) ventilators, and (3) PPE. We do not support inciting free-market competition or further partisan politicization between states at this time of our national and global public health crisis.11 We do not support inciting free-market competition between states at this time of public health crisis. The Defense Production Act will also protect citizens, state governors, and county-level officials against any price gouging that is occurring by corporations when negotiating the mass purchases of the above 3 items.
FIGURE 2.
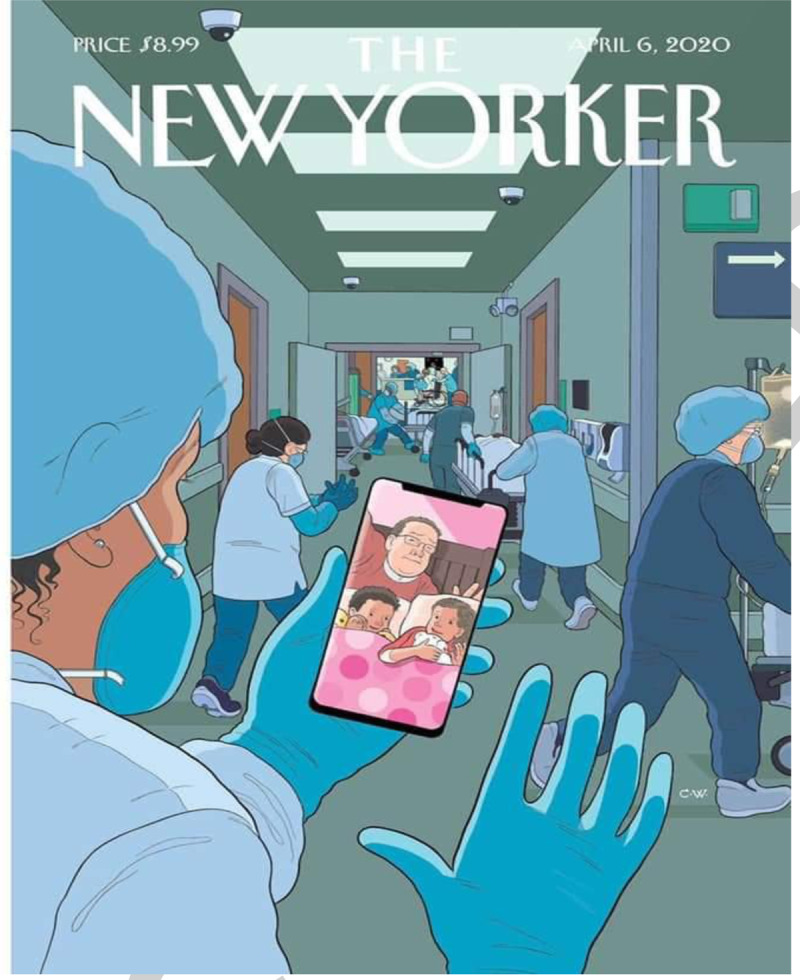
A reflection of our lives as healthcare workers during the COVID-19 pandemic.
SOCIETAL ISSUES OF EQUITY AND INCLUSION
We recognize that the threat highlighted by the Federal Bureau of Investigation of hate crimes against Asian and Asian-Americans is increasing across the United States.12 We call for all citizens to protect each other against such occurrences by calling out and reporting hate crimes when and wherever they may occur. We are concerned that biases already inherent in our healthcare system may worsen during the COVID-19 pandemic and that freedom of speech is of paramount importance when identifying potential and real risks to public health.
-
1.
We condemn the use of racism-inciting, nonscientific terms or colloquialisms when referring to this and other pandemics, to eliminate stigmatization or blame of groups. Please refer to the representative #EAST4ALL infographic on the topic of racism, xenophobia, and stigma in the time of COVID-19 (Fig. 3), the statement of the Society for Asian Academic Surgeons,13 the statement from the American College of Surgeons,14 and information from the CDC on reducing stigma.15
-
2.
As testing for COVID-19 is limited with considerable variability in guidelines, who gets tested may ultimately be a result of implicit bias. There may exist an overrepresentation of on-demand testing of the “rich and famous” and higher social classes compared to undertesting, as with other medical investigations, of Black and Brown communities and other underserved groups.16 We call on the CDC to collect and report publicly on the racial, ethnic, or class demographic information of patients receiving testing to identify and address such biases in real time.
-
3.
Freedom of speech should be preserved and protected for all members of society when advocating for the public health of their communities:
-
i.
To echo the recent statement of the American College of Surgeons, HCWs should be able to speak freely, without fear of reprisals, about shortages of PPE and potential immediate solutions.17
-
ii.
Military healthcare providers and leaders at all levels of the command structure should feel free to speak up about concerns of any threat to the public health of their colleagues or the service members under their charge, also without fear of reprisals or adverse career actions.18
-
i.
FIGURE 3.
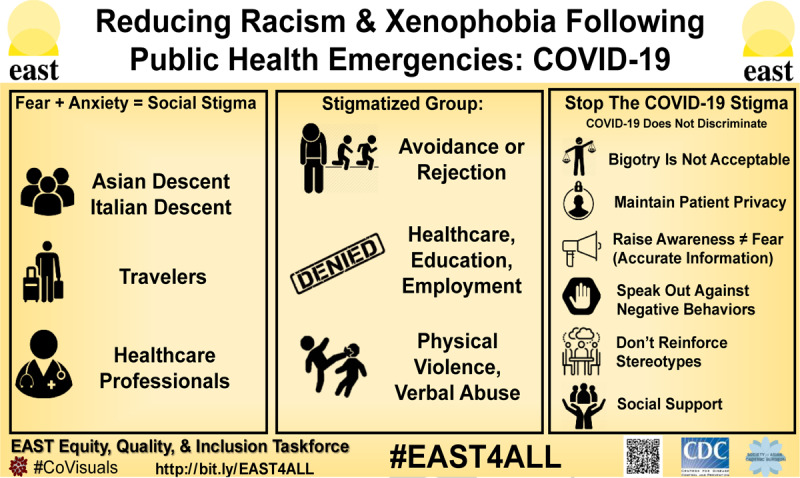
#EAST4ALL Co-Visual Infographic.
STRUCTURAL VIOLENCE19
Given the various, necessary shelter-in-place orders across the nation and the halting of the US economy, we recognize the disproportionate economic burden that this will have on both individuals and families. We recognize that even the ability to shelter in place and socially distance are dependent on one's privilege or socioeconomic status. In particular, this will have a devastating impact on communities which have been economically marginalized through systemic racism and biases, notably African-American communities, with long historic roots in the United States.20 As a result, they are already experiencing a very high and disproportionate mortality rate from COVID-19, reflecting such structural violence.21 This is, by definition, a genocidal crime against humanity.22,23 Brown and Latinx communities are also at risk, as are individuals dependent on precarious employment such as the gig economy. White, rural families living in poverty may face food insecurity and hospital closures for economic reasons, closing off scant intensive care unit beds. Native American communities are at risk of further economic hardship, affecting an already tenuous supply of water and electricity into some reservations across the country, on a backdrop of colonialism and cultural genocide. Undocumented individuals, homeless, and incarcerated individuals in correctional facilities are at a particularly increased risk of large-scale disease transmission and illness. We anticipate that many vulnerable populations have already been severely affected by the far-reaching effects of this pandemic due to numerous mental, physical, and financial factors. We recommend immediate economic relief for families and individuals proportionate to their needs and economic vulnerability, and the establishment of a basic universal income. We also call for the elimination of all structures and mechanisms of systemic racism and discrimination (eg, redlining) and immediate economic redress and compensation for those most affected.
-
1.
We recognize the devastating and all too common parallel burdens of concomitant loss of employment and thus loss of healthcare insurance and access. We recommend comprehensive, free testing and medical care for all COVID-19 positive individuals without fear of subsequent economic hardship or bankruptcy. In addition to testing, contact tracing must be prioritized and conducted by public health officials to mitigate further spread among vulnerable communities. We call for a robust, nationally coordinated universal healthcare system to protect all Americans from financial ruin or disaster in times of illness, with emphasis on preventive care. We also call for a robust system of public health to protect citizens from current and future public health crises such as the COVID-19 pandemic and its possible resurgence.
-
2.
As surgeons, we recognize the urgent need for the abovementioned economic support for our most vulnerable communities, as such stressors may lead to further intentional, interpersonal violence compounded by an increased risk of COVID-19 infection. These at-risk communities include but are not limited to:
-
i.
poverty-stricken communities (urban or rural) that have increased access to legal and/or illegal firearms increasing the risk of homicide and/or suicide
-
ii.
food insecure families and children dependent on nutrition in schools
-
iii.
intimate partner and domestic violence of all genders, especially during periods of mandated “shelter-in-place”
-
a.
shelter availability may be scarce with situations of overcrowding increasing the risk of transmission of COVID-19
-
a.
-
iv.
unintentional injury or death of children from easy access to unprotected firearms in the homes
-
v.
elderly in assisted living facilities at risk of exposure and neglect, with a higher case fatality rate than younger people
-
vi.
HCWs hired by third party contracts for hospitals who are being furloughed or laid-off and therefore losing healthcare benefits
-
vii.
undocumented individuals fearful of testing, detained in unsafe Immigration and Customs Enforcement conditions, separated from families or who risk deportation back to a violent environment
-
viii.
homeless individuals with no access to clean water or hand sanitizer and experience overcrowding in shelters
-
ix.
incarcerated individuals in correctional facilities where physical distancing and hand hygiene are difficult
-
x.
individuals struggling with mental illness or substance abuse
-
xi.
sex trade workers vulnerable to exploitation and homelessness
Urgent and well-coordinated action at the local, state, and federal levels must be taken to protect these vulnerable populations, united by social class, to prevent the rapid spread of COVID-19 and any risk of intentional, interpersonal violence or death.
-
i.
-
3.
There will be an anticipated greater than 30% unemployment rate in the United States as a result of the COVID-19 pandemic, which will surpass the unemployment rate of the Great Depression of 1929. We support a nationally sponsored economic response plan, similar to president Franklin D. Roosevelt's New Deal almost 100 years ago, which will prioritize public work projects, financial reforms, and regulations with an emphasis on economic recovery for vulnerable populations.
The COVID-19 pandemic has pushed our national and global communities to a critical and unprecedented moment for humanity. We find ourselves asking what kind of society we want for ourselves, our families, and our children in the future. On a global level, we call for the administration of the United States to re-engage in our previous Good Neighbor Policy20 by (i) respecting all nations and their people, (ii) adopting a policy of noninterference and nonintervention, and (iii) in ceasing hostilities affecting the public health of populations equally affected by COVID-19 such as through wars or economic sanctions. As surgeons in the United States and around the world, we can be leaders in the free, reciprocal, and collegial distribution of medical knowledge, ideas, and resources and set the stage for the kind of global society we wish to shape together.
Our response to the virus is indeed a reflection of who we are as individuals and how we, as a society, see our responsibilities to our local, national, and global neighbors.
Let this be seen by future generations as our greatest hour.
Footnotes
The authors declare no conflicts of interest.
REFERENCES
- 1.Reeves E. A synthesis of the literature on trauma-informed care. Issues Ment Health Nurs 2015; 36:698–709. [DOI] [PubMed] [Google Scholar]
- 2.Bruce MM, Kassam-Adams N, Rogers M, et al. Trauma providers’ knowledge, views, and practice of trauma-informed care. J Trauma Nurs 2018; 25:131–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.The New Yorker April 6, 2020 | The New Yorker [Internet]. [cited 2020 Apr 9]. Available from: https://www.newyorker.com/magazine/2020/04/06
- 4.Maunder RG, Leszcz M, Savage D, et al. Applying the lessons of SARS to pandemic influenza: an evidence-based approach to mitigating the stress experienced by healthcare workers. Can J Public Health 2008; 99:486–488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Group behind NYC's COVID-19 field hospital run by antigay evangelist [Internet]. NBC News [Accessed April 4, 2020]. Available at: https://www.nbcnews.com/feature/nbc-out/group-behind-central-park-s-covid-19-field-hospital-run-n1173396.
- 6.Van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med 2020; 382:1564–1567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.COVID-19_PPE_illustrations-p.pdf [Internet]. [Accessed April 4, 2020]. Available at: https://www.cdc.gov/coronavirus/2019-ncov/downloads/COVID-19_PPE_illustrations-p.pdf.
- 8.2003 - Interim Domestic Guidance on the Use of Respirator.pdf [Internet]. [Accessed April 3, 2020]. Available at: https://www.cdc.gov/sars/clinical/respirators.pdf.
- 9.Former EPA head admits she was wrong to tell New Yorkers post-9/11 air was safe | US news | The Guardian [Internet]. [cited April 3, 2020]. Available at: https://www.theguardian.com/us-news/2016/sep/10/epa-head-wrong-911-air-safe-new-york-christine-todd-whitman.
- 10.Farley R. Trump, Biden and the Defense Production Act [Internet]. FactCheck.org. 2020 [cited April 3, 2020]. Available at: https://www.factcheck.org/2020/04/trump-biden-and-the-defense-production-act/.
- 11.News ABC. FBI Warns of Potential Surge in Hate Crimes Against Asian Americans Amid Coronavirus [Internet]. ABC News. [cited April 3, 2020]. Available at: https://abcnews.go.com/US/fbi-warns-potential-surge-hate-crimes-asian-americans/story?id=69831920.
- 12.ipsupport. The Society of Asian Academic Surgeons (SAAS) [Internet]. [cited April 4, 2020]. Available at: https://www.asiansurgeon.org/
- 13.April 3, 2020. ACS Statement on Discrimination [Internet]. American College of Surgeons. [cited April 4, 2020]. Available at: https://www.facs.org/covid-19/discrimination.
- 14.CDC. Coronavirus Disease 2019 (COVID-19) [Internet]. Centers for Disease Control and Prevention. 2020 [cited April 4, 2020]. Available at: https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/reducing-stigma.html.
- 15.Doctors Are Concerned That Black Communities Might Not Be Getting Access To Coronavirus Tests [Internet]. BuzzFeed News. [cited April 3, 2020]. Available at: https://www.buzzfeednews.com/article/nidhiprakash/coronavirus-tests-covid-19-black.
- 16.April 1, 2020. American College of Surgeons Statement on PPE Shortages during the COVID-19 Pandemic [Internet]. American College of Surgeons. [cited April 3, 2020]. Available at: https://www.facs.org/covid-19/ppe/acs-statement.
- 17.Navy relieves captain who raised alarm about COVID-19 on ship [Internet]. NBC News. [Accessed April 3, 2020]. Available at: https://www.nbcnews.com/news/military/navy-expected-relieve-captain-who-raised-alarm-about-covid-19-n1175351.
- 18.Galtung J. Violence, peace, and peace research. J Peace Res 1969; 6:167–191. [Google Scholar]
- 19.Bleich SN, Findling MG, Casey LS, et al. Discrimination in the United States: experiences of black Americans. Health Serv Res 2019; 54: suppl 2: 1399–1408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Good Neighbor policy. In: Wikipedia [Internet]. 2020 [Accessed April 4, 2020]. Available at: https://en.wikipedia.org/w/index.php?title=Good_Neighbor_policy&oldid=947890874.
- 21.Calma J. America set up black communities to be harder hit by COVID-19 [Internet]. The Verge. 2020 [cited 2020 Apr 9]. Available from: https://www.theverge.com/2020/4/8/21213974/african-americans-covid-19-coronavirus-race-disparities.
- 22.United Nations Office on Genocide Prevention and the Responsibility to Protect [cited 2020 Apr 28] https://www.un.org/en/genocideprevention/genocide.shtml.
- 23.United Nations Office on Genocide Prevention and the Responsibility to Protect [cited 2020 Apr 28] https://www.un.org/en/genocideprevention/crimes-against-humanity.shtml.