

Abstract
Introduction:
Cheiloscopy and dactyloscopy have long been the most commonly used methods for forensic investigations. Orthodontists perform numerous diagnostic procedures, which include radiographs, photographs and impressions of the teeth and palate for the evaluation of malocclusion. The data recorded by them provide immense information about a patient. Fingerprints, lip prints and palatal rugae have been considered the most stable, reliable, imitable, convenient, cost-effective and time-friendly modes of investigating crime and other purposes.
Aim:
The main aim of this study is to correlate cheiloscopy, fingerprint pattern and palatoscopy to skeletal Class I sagittal jaw relationship and to include cheiloscopy, fingerprint pattern assessment and palatoscopy in routine orthodontic investigation procedures as an adjunct procedure in individual identification.
Methods:
Fingerprints, lip prints, palatal rugae pattern and lateral cephalograms of 37 skeletal Class I patients were obtained using standardized procedures.
Results:
In Class I skeletal malocclusion, the maximum number of patients exhibited ulnar loop dermal pattern, Type 1 and Type 2 lip patterns and a wavy rugae pattern (Kapali et al. primary classification).
Conclusion:
Orthodontists prepare various antemortem records for diagnostic purposes, i.e., photographs, the impression of the teeth and palate, lateral cephalograms, orthopantomograms and hand-wrist radiographs. If orthodontists recorded additional data of finger and lip prints, the archives of an orthodontist would be of tremendous profit to forensic sciences in individual identification.
Keywords: Cheiloscopy, fingerprint, orthodontics, palatoscopy, sagittal jaw relation, skeletal Class I relationship
INTRODUCTION
Antemortem records are of enormous value in forensic sciences. The most commonly employed records for investigation purposes are dermatoglyphics, cheiloscopy, DNA analysis, dental comparison and palatoscopy.
The word dermatoglyphics stemmed from two Greek words derma (skin) and glyphs (carve), which was coined by Cummin and Midlo in 1962.[1,2,3] Fingerprints are commonly used for crime investigations and civil proceedings, as they save time, provide immediate and accurate results and are most importantly cost-effective.[3] The dermal ridges develop within the 6th–13th week of intrauterine life, and from then on, there is an increase only in size, with no other morphological changes.[4,5,6] Hence, due to its genetic basis, it is considered unique, reliable, imitable and classifiable.[2] Fingerprints have had good correlations with dental caries, oral cancer, bruxism, anomalies of teeth, cleft lip and palate, periodontal disease and dental fluorosis.[1] Recently, many studies have been confirming a strong association between malocclusion and fingerprint patterns. Tooth development starts as early as the 6th week of embryonic life,[1] which coincides with the development of dermal ridges; hence, researchers believe that there is a strong correlation between fingerprint and malocclusions.[1,2,4,5,6,7,8]
Lip prints consist of normal lines and fissures in the form of wrinkles and grooves present in the zone of transition of the human lip between the inner labial mucosa and outer skin, the study of which is referred to as cheiloscopy.[9,10,11,12,13] The lip formation completes within the 6th–9th week of intrauterine life.[13] The lip prints are unique to an individual except in monozygotic twins.[11] Lip prints and thumbprints have proven to be analogous.[9,10,11,12,13,14] Thumbprints and malocclusion have exhibited a parallel correlation in previous studies. Establishing a relationship between lip prints and malocclusions could help an orthodontist to determine the type of sagittal discrepancy and to provide additional information on personal identity.[9]
Morlang had stated that fingerprints have long been the standard for identification, but this form of identification is not possible if there are no antemortem records.[15] Practically speaking, postmortem fingerprints and lip prints are often unavailable, especially in cases involving fire, massive trauma and decomposition.[15] In such circumstances, palatal rugae play a productive role in individual identification. Palatal rugae are asymmetrical and irregular elevations of the mucosa in the anterior portion of the palate arranged in a transverse direction on each side of the median palatal raphae and behind the incisive papilla and sighted in the midsagittal plane. The hard connective tissue covering bone forms the palatal rugae in the 3rd month of intrauterine life.[15] The orientation of the pattern is formed by about 12th–14th week of prenatal life and remains stable until the oral mucosa degenerates after death.[15] Palatal rugae can be considered an important record for forensic investigation because they are protected from trauma by their internal position in the head and heat by the tongue and the buccal pad of fat,[15,16,17,18] hence proving to be unique, stable and postmortem resistant.[15,16,19] Sassouni stated that no two palates are similar in their configuration and are considered to be stable throughout life (following completion of growth), although there is considerable debate on this matter.[15,17] Studies have revealed that trauma, extreme finger sucking in infancy and persistent pressure with orthodontic treatment and dentures can contribute to changes in rugae patterns.[18] However, palatal rugae have found to be as reliable as fingerprints in forensic odontology.[17] The study of palatal rugae is known as palatoscopy or palatal rugoscopy.[15,17,18,20]
Fingerprints, palatal rugae and lip prints are permanent and unchangeable.[11] It has been formulated that fingers, palms, lip, alveolus and palate develop during the same embryonic period.[9] Since dermal patterns and craniofacial constitutions are firmly but not predominantly genetically governed structures, it may be hypothesized that hereditary and genetic factors causing variations in the lip, alveolus and palate may also cause peculiarities in fingerprint patterns.[1]
The main purpose of this study is to correlate cheiloscopy, dermatoglyphics and palatoscopy to Class I sagittal jaw relationship and to request orthodontists to include cheiloscopy, dermatoglyphics and palatoscopy in routine investigation procedures as an additional procedure, as this will aid and benefit the department of forensic odontology considerably.
METHODS
G Power, version 3.0.1 (Franz Faul Universitat, Kiel, Germany) software was used to determine the sample size, and it provided a sample size result of 37 subjects. The randomized sample design method was used. In this study, male and female patients were included. The study was conducted at the Department of Orthodontics and Dentofacial Orthopedics, Vokkaligara Sangha Dental College and Hospital, Bengaluru.
For obtaining a fingerprint, Security Solutions Rectangle Inkless FingerPad was used. The patients were asked to dab the finger on the ink pad and then onto an A4 size sheet. The procedure was repeated for each finger, and each finger was labeled for the right and left hand, respectively. The fingerprints were then substantiated, and the whole procedure was repeated to ensure proper recording of the fingerprints. The fingerprints were classified based on patterns as whorls, loops and arches [Figure 1].[1]
Figure 1.
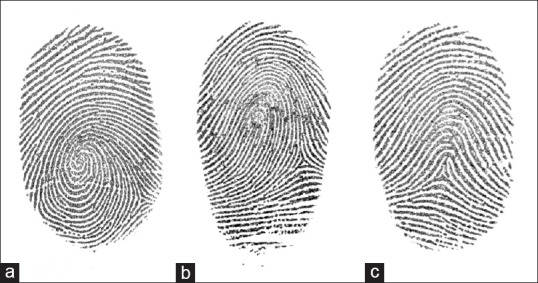
Finger print (a) ulnar loop (b) whorl (c) arch
For obtaining lip prints, seduction lipstick shade 2 (Las Vegas) was used. The lipstick was applied uniformly with one stroke on the upper and lower lips. The patients were asked to rub the upper and lower lip; an impression of the lips was made on a transparent self-adhesive tape having a width of 2 inches. The lip impression was immediately pasted on an A4 size white paper. Suzuki and Tsuchihashi's classification was employed for lip print identification [Figure 2].[9]
Figure 2.

Lip print
For obtaining palatal rugae, alginate impression of the upper arch was made for each patient, and the casts were poured and retrieved. The rugae were defined using a sharp graphite pencil under adequate light and magnification and were recorded according to the classification given by Kapali et al. primary classification [Figure 3].
Figure 3.

Rugae pattern
Lateral cephalograams of each patient were made and were classified into skeletal Class I malocclusions based on ANB value, Wits appraisal and beta angle [Figure 4].[1,3]
Figure 4.

Lateral cephalogram
RESULTS
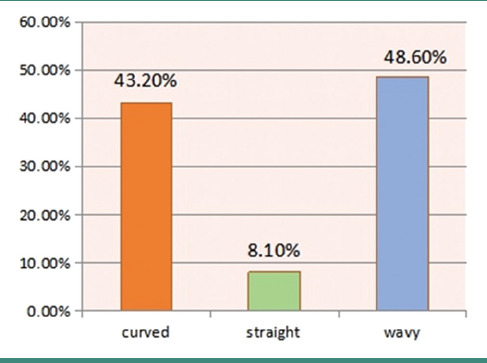
In this study, the results revealed that when skeletal Class I patients were investigated, the dermal pattern showed ulnar loop in 70.30% of the patients [Table 1], 48.60% exhibited Type 1 and Type 2 lip patterns [Table 2] and 48.60% exhibited wavy rugae pattern [Table 3].
Table 1.
Finger print distribution in Class I skeletal malocclusion
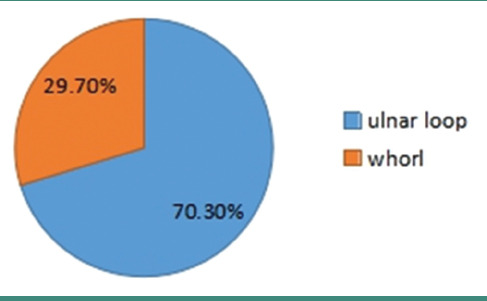
Table 2.
Lip print distribution in Class I skeletal malocclusion
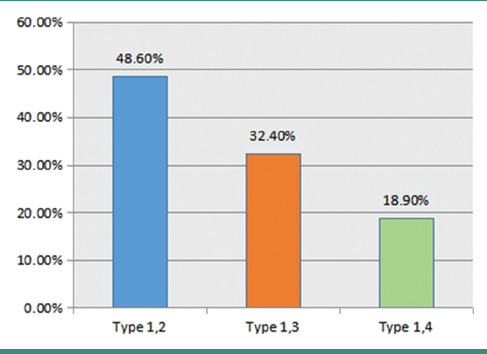
Table 3.
Rugal morphology distribution in Class I skeletal malocclusion
DISCUSSION
Our study is in accordance with Charles et al. and Kanematsu et al.'s study where there was an increase in loop pattern but was contrasting to the results obtained by Reddy et al., Jindal et al. and Trehan et al. “Proof of no change” was a rule put forth by Galton who stated that dermatoglyphics pattern remains unchanged throughout life.[1] By around the 5th month of gestation, the primary dermal ridges develop and the structure and configuration almost takes the final pattern until the 6th month of gestation when the secondary ridges are formed.[21] With improved research, epidermal ridges have been useful to determine hereditary diseases.[22,23] According to a study conducted by Pour-Jafari et al., fingerprint pattern was useful to detect even chromosomal abnormalities such as eczema, alopecia and psoriasis, and the three conditions had a maximum of ulnar loop and spiral whorl.[22] Dermatoglyphics play a major role in genetic counseling, especially for diseases such as vitiligo, alopecia, dermatoses, Darier's disease, psoriasis, ichthyosis, atopic dermatitis, anhidrotic ectodermal dysplasia, eczema and malignant acanthosis nigricans.[23] Considering that the dermal ridges and the tooth germ develop from the same ectoderm and also around the same period of time, a good correlation between the two has been established.[2]
A maximum of Type 1 and Type 2 lip patterns were observed in our study, which was in contrast to Kulkarni et al. who observed a maximum of Type 1 and Type 3 lip patterns in Class I skeletal malocclusion. The most commonly observed lip print pattern in human beings is Type I' according to a study conducted by Loganadan et al.[13] According to a study conducted by Raghav et al., when skeletal Class I malocclusion was assessed for lip print, the branched and reticular lip pattern was observed in males and branched lip pattern was observed in females.[12] Verghese et al., in Kerala, found that reticular lip pattern had the highest incidence. According to Tsuchihashi et al. study, in the Japanese population, intersected lip pattern was the most common. Vahanwala and Parekh, in their study on the North Indian population, found that vertical lip pattern was the most common. Sivapathasundharam, Prakash and Sivakumar studied the lip prints of Indo-Dravidian population and noted that intersected lip pattern was maximum in number. Due to the different lip print patterns observed in different regions of the world, lip prints have considered to have regional differences in their appearance.[12] Lip prints have far been the most commonly noticed latent prints in a crime scene. Irrespective of the application of lipstick, the lips have sebaceous glands and sweat glands around them which will leave marks that can be detected under magnification or using chemical powders.[9,10,11] Furthermore, from many studies, it has been concluded that there is no sexual dimorphism in lip print pattern.[12]
In this study, the wavy rugae pattern was observed in large. In 1989, Hauser stated that the greater the palatal development, the greater the number of rugae.[19] Studies concluded that only Class III pattern had a distinct forking diverging pattern of rugae, but Class I and Class II exhibited wavy and curved patterns.[19] Palatal rugae are considered the most stable landmark in the oral cavity except if they have undergone expansion and orthodontic treatment or if they are denture wearers.[16] The rugae are formed by epithelial proliferation and below which fibroblasts orient themselves producing a particular pattern.[17] Rugae have seen to contribute a great role in swallowing, suction and in speech. Some studies concluded that rugae change their position when a tooth is extracted near the rugae, and sometimes, change patterns due to thumb-sucking habit.[18] However, even in times of injury, rugae are reproduced in the same site and form.[18] The population-specific pattern of the rugae makes it an exclusive tool for the investigation in forensic purposes.[17] Ranjan et al. from their study concluded that fingerprints, lip prints and rugae patterns are unique to an individual.[11]
Proficient diagnostic procedures and appropriate analysis of pertinent diagnostic data are the basis of a comprehensive plan of orthodontic therapy.[12] Malocclusion has always proven to have a genetic predisposition as one of its main etiological factors, and if the malocclusion is not treated, it has a major impact on the psychosocial life of the individual.[2] Further studies with a larger sample size are required to provide accurate and specific results for the malocclusion.
CONCLUSION
Skeletal Class I malocclusion revealed a wavy rugae pattern, ulnar loop dermal morphology and Type 1 and Type 2 lip patterns. Orthodontists prepare various antemortem records for diagnostic purposes, i.e., photographs, the impression of the teeth and palate, lateral cephalograms, orthopantomograms and handwrist radiographs. If orthodontists recorded additional data of finger and lip prints, the archives of an orthodontist would be of tremendous profit to forensic sciences.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Tikare S, Rajesh G, Prasad KW, Thippeswamy V, Javali SB. Dermatoglyphics-a marker for malocclusion? Int Dent J. 2010;60:300–4. [PubMed] [Google Scholar]
- 2.Taneja MB, Bhasin P, Singh A, Bhatia N, Akhilesh H. Shewale and natasha gambhir. Dermatoglyphics and malocclusion-a forensic link. Br Biotechno J. 2016;13:1–2. [Google Scholar]
- 3.Tandon A, Srivastava A, Jaiswal R, Patidar M, Khare A. Estimation of gender using cheiloscopy and dermatoglyphics. Natl J Maxillofac Surg. 2017;8:102–5. doi: 10.4103/njms.NJMS_2_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Charles A, Ramani P, Sherlin HJ, Dilip S, Srinivas S, Jayaraj G. Evaluation of dermatoglyphic patterns using digital scanner technique in skeletal malocclusion: A descriptive study. Indian J Dent Res. 2018;29:711–5. doi: 10.4103/ijdr.IJDR_137_18. [DOI] [PubMed] [Google Scholar]
- 5.Reddy BR, Sankar SG, Roy ET, Govulla S. A comparative study of dermatoglyphics in individuals with normal occlusions and malocclusions. J Clin Diagn Res. 2013;7:3060–5. doi: 10.7860/JCDR/2013/7663.3853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shetty SS, Mi Li GS, Babji NA, Liyana Yusof SB, Yang NN, Jun TD. Dermatoglyphics: A prediction tool for malocclusion. J Datta Meghe Inst Med Sci Univ. 2019;14:27–30. [Google Scholar]
- 7.Yang X, Xiaojun J, Yixuan Z, Hui L. Genetic rules for the dermatoglyphics of human fingertips and their role in spouse selection: A preliminary study. Springerplus. 2016;5:1396. doi: 10.1186/s40064-016-3072-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Achalli S, Patla M, Nayak U, Soans CR. Dermatoglyphics and orthodontics. Int J Orthod Rehabil. 2016;7:144–7. [Google Scholar]
- 9.Kulkarni N, Vasudevan S, Shah R, Rao P, Balappanavar AY. Cheiloscopy: A new role as a marker of sagittal jaw relation. J Forensic Dent Sci. 2012;4:6–12. doi: 10.4103/0975-1475.99152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mohanty B, Jadon AK, Rathore S, Bhatt P, Gupta S, Vaid S. Cheiloscopy as a means for personal identification in forensic dentistry: A study. Int J Prev Clin Dent Res. 2015;2:42–4. [Google Scholar]
- 11.Ranjan V, Sunil MK, Kumar R. Study of lip prints: A forensic study. J Indian Academy Oral Med Radiol. 2014;26:50–5. [Google Scholar]
- 12.Raghav P, Kumar N, Shingh S, Ahuja NK, Ghalaut P. Lip prints: The barcode of skeletal malocclusion. J Forensic Dent Sci. 2013;5:110–7. doi: 10.4103/0975-1475.119777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Loganadan S, Dardjan M, Murniati N, Oscandar F, Malinda Y, Zakiawati D. Preliminary Research: Description of Lip Print Patterns in Children and Their Parents among Deutero-Malay Population in Indonesia. Int J Dent. 2019;2019:7629146. doi: 10.1155/2019/7629146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Khanna S, Singh NN, Brave VR, Sreedhar G, Purwar A, Srivastava A. Training module for cheiloscopy and palatoscopy in forensic odontology. J Forensic Dent Sci. 2014;6:36–41. doi: 10.4103/0975-1475.127768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bansode SC, Kulkarni MM. Importance of palatal rugae in individual identification. J Forensic Dent Sci. 2009;1:77–81. [Google Scholar]
- 16.Shailaja AM, Romana IR, Narayanappa G, Smitha T, Gowda NC, Vedavathi HK. Assessment of palatal rugae pattern and its significance in orthodontics and forensic odontology. J Oral Maxillofac Pathol. 2018;22:430–5. doi: 10.4103/jomfp.JOMFP_190_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Nayak P, Acharya AB, Padmini AT, Kaveri H. Differences in the palatal rugae shape in two populations of India. Arch Oral Biol. 2007;52:977–82. doi: 10.1016/j.archoralbio.2007.04.006. [DOI] [PubMed] [Google Scholar]
- 18.Kesri R, Das G, Tote J, Thakur P. Rugoscopy-science of palatal rugae: A review. Int J Dent Med Res. 2014;1:103–7. [Google Scholar]
- 19.Kapoor P, Ragini, Kaur H. Rugoscopy: A diagnostic appurtenance for malocclusion or just a forensic aid? A pilot study. J Forensic Res. 2015;6:272. [Google Scholar]
- 20.Sabarigirinathan C, Vinayagavel K, Meenakshi A, Selvamani C, Sriramaprabu G, Sivasakthikumar S, et al. Palatal rugae in forensic odontology – A review. J Dent Med Sci. 14:83–7. [Google Scholar]
- 21.Miller JR. Dermatoglyphics. J Invest Dermatol. 1973;60:435–41. doi: 10.1111/1523-1747.ep12702906. [DOI] [PubMed] [Google Scholar]
- 22.Pour-Jafari H, Farhud DD, Yazdani A, Hashemzadeh Chaleshtori M. Dermatoglyphics in patients with eczema, psoriasis and alopecia areata. Skin Res Technol. 2003;9:240–4. doi: 10.1034/j.1600-0846.2003.00029.x. [DOI] [PubMed] [Google Scholar]
- 23.Kumar P, Gupta A. Dermatoglyphic patterns in psoriasis, vitiligo and alopecia areata. Indian J Dermatol Venereol Leprol. 2010;76:185–6. doi: 10.4103/0378-6323.60556. [DOI] [PubMed] [Google Scholar]