

Ibrexafungerp (formerly SCY-078) is a semisynthetic triterpenoid and potent (1→3)-β-d-glucan synthase inhibitor. We investigated the in vitro activity, pharmacokinetics, and in vivo efficacy of ibrexafungerp (SCY) alone and in combination with antimold triazole isavuconazole (ISA) against invasive pulmonary aspergillosis (IPA). The combination of ibrexafungerp and isavuconazole in in vitro studies resulted in additive and synergistic interactions against Aspergillus spp.
KEYWORDS: combination therapy, ibrexafungerp (SCY-078), isavuconazole, pulmonary aspergillosis, rabbits
ABSTRACT
Ibrexafungerp (formerly SCY-078) is a semisynthetic triterpenoid and potent (1→3)-β-d-glucan synthase inhibitor. We investigated the in vitro activity, pharmacokinetics, and in vivo efficacy of ibrexafungerp (SCY) alone and in combination with antimold triazole isavuconazole (ISA) against invasive pulmonary aspergillosis (IPA). The combination of ibrexafungerp and isavuconazole in in vitro studies resulted in additive and synergistic interactions against Aspergillus spp. Plasma concentration-time curves of ibrexafungerp were compatible with linear dose proportional profile. In vivo efficacy was studied in a well-established persistently neutropenic New Zealand White (NZW) rabbit model of experimental IPA. Treatment groups included untreated control (UC) rabbits and rabbits receiving ibrexafungerp at 2.5 (SCY2.5) and 7.5 (SCY7.5) mg/kg of body weight/day, isavuconazole at 40 (ISA40) mg/kg/day, or combinations of SCY2.5+ISA40 and SCY7.5+ISA40. The combination of SCY+ISA produced an in vitro synergistic interaction. There were significant in vivo reductions of residual fungal burden, lung weights, and pulmonary infarct scores in SCY2.5+ISA40, SCY7.5+ISA40, and ISA40 treatment groups versus those of the SCY2.5-treated, SCY7.5-treated, and UC (P < 0.01) groups. Rabbits treated with SCY2.5+ISA40 and SCY7.5+ISA40 had prolonged survival in comparison to that of the SCY2.5-, SCY7.5-, ISA40-treated, or UC (P < 0.05) groups. Serum galactomannan index (GMI) and (1→3)-β-d-glucan levels significantly declined in animals treated with the combination of SCY7.5+ISA40 in comparison to those of animals treated with SCY7.5 or ISA40 (P < 0.05). Ibrexafungerp and isavuconazole combination demonstrated prolonged survival, decreased pulmonary injury, reduced residual fungal burden, and lower GMI and (1→3)-β-d-glucan levels in comparison to those of single therapy for treatment of IPA. These findings provide an experimental foundation for clinical evaluation of the combination of ibrexafungerp and an antimold triazole for treatment of IPA.
INTRODUCTION
Invasive pulmonary aspergillosis (IPA) is a life-threatening infection in immunosuppressed patients, particularly in those with severe and prolonged neutropenia as a consequence of myelotoxic chemotherapy for the treatment of cancer and in those receiving immunosuppressive medication for rejection prophylaxis after organ transplantation or treatment of graft-versus-host disease (GVHD) in allogeneic bone marrow transplantation (1–5). Despite major advances in therapy with antifungal triazoles, mortality and morbidity from IPA remains unacceptably high. Clearly, new strategies are needed for more effective treatment of IPA.
The antifungal triazoles inhibit fungal cell membrane biosynthesis through inhibition of ergosterol formation at the level of lanosterol C14-demethylase. Isavuconazole (ISA), an antifungal triazole, with a potent and relatively broad-spectrum in vitro antifungal activity against medically important yeasts and filamentous fungi and with a favorable pharmacokinetic profile has the potential to become an important agent for the treatment of IPA.
Ibrexafungerp (formerly SCY-078) is a semisynthetic triterpenoid, a derivative of the natural product enfumafungin, and a potent inhibitor of fungal (1→3)-β-d-glucan synthases (6, 7). This compound is structurally different from the echinocandins and has the advantage of having high oral bioavailability. Its in vitro activity against Candida spp. and Aspergillus spp. was recently demonstrated (8–10). Even though there is some data on its activity in combination with antimold triazoles in vitro, little is known about ibrexafungerp efficacy in combination treatment against IPA in vivo (11, 12).
We hypothesized that simultaneous inhibition of the biosynthesis of (1→3)-β-d-glucan in the fungal cell wall by ibrexafungerp and ergosterol biosynthesis in the fungal cell membrane by an antifungal triazole in combination would result in a synergistic interaction in vivo. We, therefore, studied the in vitro activity, in vivo efficacy, and pharmacokinetics of ibrexafungerp in combination with isavuconazole in treatment of experimental IPA in persistently neutropenic rabbits.
RESULTS
In vitro activity studies.
In vitro combination of ibrexafungerp and isavuconazole (SCY+ISA) resulted in an additive interaction against Aspergillus fumigatus NIH-4215. The median in vitro fractional inhibitory concentration index (FICI) for SCY+ISA against A. fumigatus was 0.68 (0.38 to 1.06). The combination of SCY+ISA resulted in a synergistic interaction in A. fumigatus measured by Bliss independence drug interaction analysis. This synergistic interaction was observed for A. fumigatus (68.9 [23.7 to 115.3]) at 24 h (Fig. 1A) and (25.2 [11.5 to 50.7]) at 48 h (Fig. 1B).
FIG 1.

Interaction surfaces obtained from response surface analysis of Bliss independence drug interaction model for the in vitro combination of ibrexafungerp and isavuconazole against A. fumigatus after 24 h (A) and 48 h (B) of incubation. The x and y axis are the concentrations of ibrexafungerp and isavuconazole, respectively. The z axis is the ΔE in percentage. The 0 plane represent Bliss independent interactions, whereas the volumes above the 0 plane represent statistically significantly synergistic (positive ΔE) interactions. The magnitude of interactions is directly related to ΔE. The different tones in the three-dimensional plots represent different percentile bands of synergy. The mean ΔE ± SEM was 68.9 ± 12.3% after 24 h and 25.2 ± 3.8% after 48 h.
Plasma pharmacokinetics of ibrexafungerp.
The plasma concentration-time curves of ibrexafungerp at 7.5 (SCY7.5), 15, and 30 mg/kg of body weight/day after a single dose are depicted in Fig. 2. These data are compatible with linear dose-proportionality of the pharmacokinetic parameters depicted in Table 1.
FIG 2.
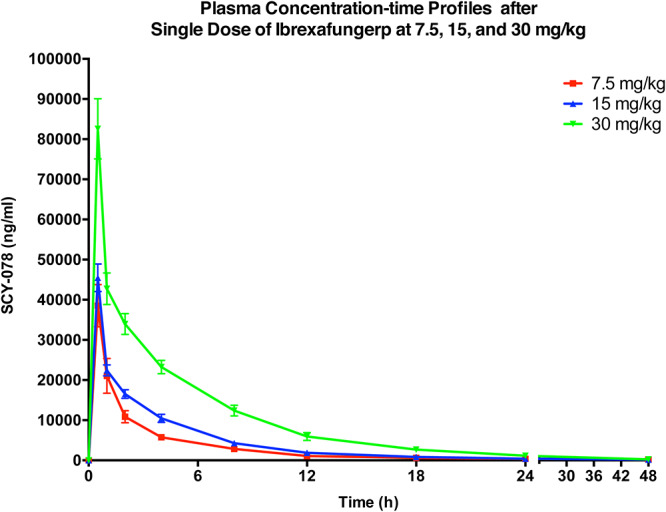
Plasma concentration-time curves after a single dose of ibrexafungerp at 7.5, 15, and 30 mg/kg administered to healthy New Zealand White rabbits. All values are presented as means from samples of four rabbits each ± SEM.
TABLE 1.
Pharmacokinetic parameters of ibrexafungerp after single-dose intravenous administration of 7.5, 15, and 30 mg/kg/day in healthy rabbits
| Dose of Ibrexafungerp (mg/kg) | AUC(0-24) (ng·h/ml) | Cmax (ng/ml) | CL (liters/h) | V (liters) |
|---|---|---|---|---|
| 7.5 | 90,338 ± 15,048 | 38,533 ± 5,282 | 0.28 ± 0.03 | 1.08 ± 0.12 |
| 15 | 128,563 ± 11,718 | 45,466 ± 3,443 | 0.38 ± 0.02 | 1.66 ± 0.07 |
| 30 | 292,629 ± 28,167 | 85,583 ± 7,478 | 0.34 ± 0.04 | 1.85 ± 0.13 |
The plasma concentration-time curves of ibrexafungerp at 2.5 (SCY2.5), 5, 7.5, 10, and 15 mg/kg/day on day 7 after repeated dosing are depicted in Fig. 3. The curves are compatible with a linear dose proportional profile, which is further depicted in Table 2, where dose proportionality is also reflected in the area under the curve from 0 to 24 h (AUC0–24), while volume of distribution (V) and clearance (CL) remain relatively constant across the range of dosages.
FIG 3.
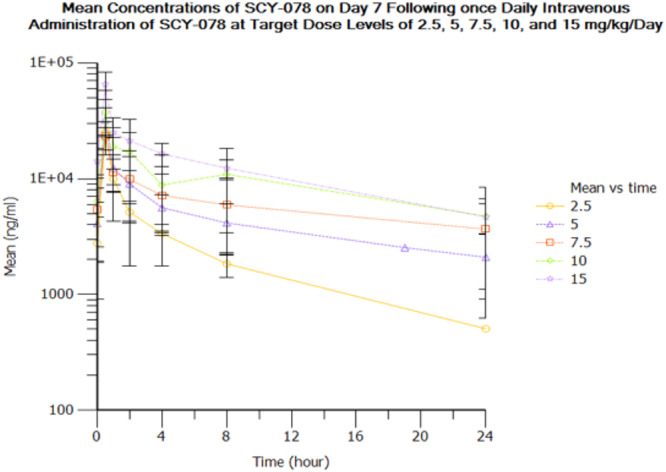
Plasma concentration-time curves after 7-day repeated dosing of ibrexafungerp at 2.5, 5, 7.5, 10, and 15 mg/kg/day to New Zealand White rabbits infected with Aspergillus fumigatus. All values are presented as means from samples of four rabbits each ± SEM.
TABLE 2.
Pharmacokinetic parameters of ibrexafungerp on day 7 after intravenous administration of 2.5, 5, 7.5, 10, and 15 mg/kg/day in infected rabbits
| Dose of Ibrexafungerp (mg/kg) | AUC(0-24) (ng·hr/ml) | Cmax (ng/ml) | CL (liters/h) | V (liters) |
|---|---|---|---|---|
| 2.5 | 50,384 ± 5,529 | 25,300 ± 1,700 | 0.12 ± 0.01 | 0.78 ± 0.17 |
| 5 | 98,548 ± 4,929 | 32,250 ± 4,307 | 0.13 ± 0.02 | 2.13 ± 0.63 |
| 7.5 | 137,421 ± 48,519 | 23,550 ± 3,761 | 0.19 ± 0.05 | 2.32 ± 0.23 |
| 10 | 162,869 ± 79,897 | 37,581 ± 9,962 | 0.35 ± 0.14 | 1.51 ± 0.28 |
| 15 | 260,041 ± 56,638 | 65,550 ± 8,689 | 0.18 ± 0.05 | 1.64 ± 0.23 |
Antifungal treatment of invasive pulmonary aspergillosis.
During the initial study, rabbits were treated with only ibrexafungerp at dosages of 2.5, 5, 7.5, 10, and 15 mg/kg/day. There were no significant differences in lung weights, pulmonary infarct score, and residual fungal burden. There was a trend in improved survival (see Fig. S1 in the supplemental material).
The dosages of 2.5 mg/kg and 7.5 mg/kg of ibrexafungerp were then selected to span the range of possible human exposures of combination therapy in the rabbit model of experimental invasive pulmonary aspergillosis. The combination of ibrexafungerp and isavuconazole at 40 (ISA40) mg/kg/day was chosen at dosages of SCY2.5+ISA40 and SCY7.5+ISA40 in the treatment of the IPA rabbit model.
Outcome variables. (i) Survival.
The survival in treated rabbits was significantly prolonged in the combinations of SCY2.5+ISA40 and SCY7.5+ISA40 in comparison to that of single therapies of SCY2.5, SCY7.5, or ISA40 (P < 0.05). In addition, significantly prolonged survival was achieved in the rabbits treated with SCY2.5+ISA40, SCY7.5+ISA40, and ISA40 alone in comparison to that of untreated control (UC) rabbits (P < 0.01) (Fig. 4).
FIG 4.

Response of primary pulmonary aspergillosis in persistently neutropenic rabbits to antifungal therapy measured by survival, pulmonary infarct scores, lung weights, and mean pulmonary tissue residual fungal burden (log CFU/g) in untreated controls (UC) and rabbits receiving ibrexafungerp alone or in combination with oral isavuconazole. Values are given as means ± SEMs. For the measure of survival, the values on the y axis are probability of survival. Survival was plotted by Kaplan-Meier analysis. Differences in survival of treatment groups and UC were analyzed by log-rank test. P values are indicated as follows. Survival, ¶, P < 0.05, prolonged survival in SCY2.5+ISA40- and SCY7.5+ISA40-treated rabbits in comparison to that of single therapy with SCY2.5, SCY7.5, or ISA40; £, P < 0.01, prolonged survival of rabbits treated with SCY2.5+ISA40, SCY7.5+ISA40, and ISA40 alone in comparison to that of the UC. Pulmonary infarct scores, ¶, P < 0.01, decreased infarct scores in SCY2.5+ISA40- and SCY7.5+ISA40-treated rabbits in comparison to that of single therapy with SCY2.5, SCY7.5, or ISA40. Lung weights, *, P < 0.05, decreased lung weights in SCY2.5+ISA40- and SCY7.5+ISA40-treated rabbits in comparison to that of single therapy with SCY2.5, SCY7.5, or the UC. Mean pulmonary tissue residual fungal burden, †, P < 0.01, decreased residual fungal burden in SCY2.5+ISA40-, SCY7.5+ISA40-, and ISA40-treated rabbits in comparison to that of single therapy with SCY2.5, SCY7.5, or UC.
(ii) Pulmonary lesion scores, lung weights, and residual fungal burden.
The markers of fungal pathogen-mediated pulmonary injury (pulmonary infarct scores and lung weights) demonstrated a similar pattern of response. There was a significant decrease in pulmonary infarct scores in SCY2.5+ISA40- and SCY7.5+ISA40-treated rabbits in comparison to that of single therapy of SCY2.5, SCY7.5, or ISA40 (P < 0.01). Similarly, a significant decrease in lung weights was observed in SCY2.5+ISA40- and SCY7.5+ISA40-treated rabbits in comparison to that of single therapy of SCY2.5, SCY7.5, or UC (P < 0.05) (Fig. 4).
Residual fungal burden in lung tissues was significantly reduced in SCY2.5+ISA40-, SCY7.5+ISA40-, and ISA40-treated rabbits in comparison to that of single therapy of SCY2.5, SCY7.5, or UC (P < 0.01) (Fig. 4).
Galactomannan antigen.
Serum galactomannan antigenemia significantly declined in animals treated with the SCY7.5+ISA40 combination in comparison to those treated only with SCY7.5 or ISA40 (P < 0.05; Fig. 5A). By comparison, rabbits treated with the combination of SCY2.5+ISA40 did not have a significant decline in serum galactomannan antigen (Fig. 5B).
FIG 5.
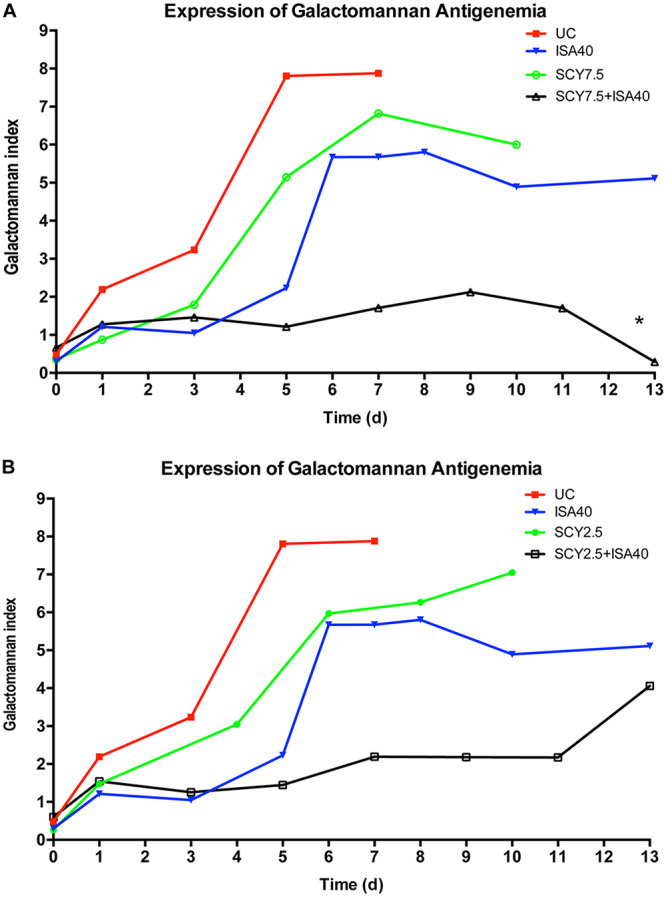
Expression of galactomannan antigenemia in persistently neutropenic rabbits with pulmonary aspergillosis in untreated controls (UC) and rabbits receiving ibrexafungerp alone or a combination of SCY7.5+ISA40 (A) or of SCY2.5+ ISA40 (B). Values are given as GMI means ± SEMs. P values are indicated as follows: *, P < 0.05; lower GMI in rabbits treated with combination regimen in comparison to that of single drug therapy.
Galactomannan index (GMI) in bronchoalveolar lavage (BAL) fluid in persistently neutropenic rabbits with pulmonary aspergillosis was significantly lower in rabbits treated with the SCY7.5+ISA40 combination or ISA40 alone than that of rabbits treated with SCY7.5 or UC (P < 0.05) (Fig. 6A). Residual fungal burden (log CFU/ml) in BAL fluid was lower in rabbits treated with combinations of SCY2.5+ISA40 and SCY7.5+ISA40 or ISA40 alone than that of the UC (P < 0.05) (Fig. 6B).
FIG 6.

Expression of galactomannan index (GMI) and residual fungal burden (log CFU/ml) in bronchoalveolar lavage (BAL) fluid in persistently neutropenic rabbits with pulmonary aspergillosis in untreated controls (UC) and rabbits receiving ibrexafungerp alone or in combination with oral isavuconazole. Values are given as GMI means ± SEMs. P values are indicated as follows. GMI, *, P < 0.05; lower GMI in BAL in rabbits treated with combination of SCY7.5+ISA40 or ISA40 alone in comparison to that of UC; †, P < 0.05; lower GMI in BAL in rabbits treated with combination of SCY7.5+ISA40 in comparison to that of single drug SCY7.5 therapy. Log CFU/ml, *, P < 0.05; lower log CFU/ml in BAL in rabbits treated with combination of SCY2.5+ISA40, SCY7.5+ISA40, or ISA40 alone in comparison to that of UC.
Serum (1→3)-β-d-glucan levels.
Serum (1→3)-β-d-glucan levels demonstrated a significant decline in rabbits treated with the combinations of SCY7.5+ISA40 (Fig. 7A) and SCY2.5+ISA40 (Fig. 7B) in comparison to those of rabbits treated with single drug therapy and UC (P < 0.05). However, the magnitude of the difference was less than that observed for serum galactomannan antigen.
FIG 7.
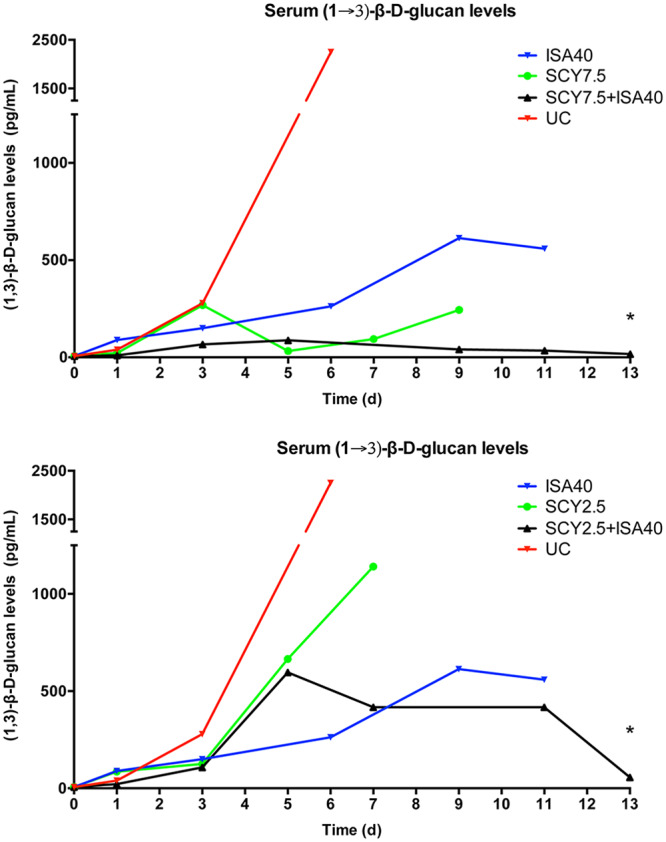
Serum (1→3)-β-d-glucan levels in persistently neutropenic rabbits with experimental pulmonary aspergillosis in untreated controls (UC) and rabbits receiving ibrexafungerp alone or a combination of SCY7.5+ISA40 (A) or SCY2.5+ISA40 (B). Values are given as (1→3)-β-d-glucan concentrations in picogram per milliliter. P values are indicated as follows. *, P < 0.05; decrease of serum (1→3)-β-d-glucan levels in rabbits treated with combination regimens in comparison to those of single drug therapy and UC.
Histopathology.
The histopathological features of aspergillosis were studied in the lungs of rabbits in all treatment groups. Each panel in Fig. 8 demonstrates a representative section of hyphal morphology in a corresponding treatment group. Abundant, slender, dichotomously branching, septate hyphae of A. fumigatus were present in lung tissues of UC rabbits (Fig. 8A). By comparison, hyphae in lung tissues of rabbits treated with SCY2.5 and SCY7.5 were truncated, distorted, and irregularly branched (Fig. 8B and C), while hyphae in lung tissues of rabbits treated with isavuconazole were aggregated, distorted, and devoid of dichotomous branching (Fig. 8D). Lung tissues of rabbits treated with the combination of SCY2.5+ISA40 revealed rare foci of fungal elements that consisted of two populations of structures, one of which appears only as faint shadow-like remnants of severely damaged hyphae and the other population as truncated, distorted, and minimally branching hyphal structures (Fig. 8E). There were no visible organisms in histological lung tissue samples of the SCY7.5+ISA40 treatment group.
FIG 8.

Effects of ibrexafungerp and isavuconazole alone or combination of ibrexafungerp plus isavuconazole in vivo on hyphal damage of A. fumigatus. (A) Abundant, slender, dichotomously branching, septate hyphae of A. fumigatus are present in lung tissues of untreated control animals. (B, C) Hyphae in lung tissues of rabbits treated with SCY2.5 and SCY7.5 were truncated, distorted, and irregularly branched. (D) Hyphae in lung tissues of rabbits treated with isavuconazole are aggregated, distorted, and devoid of dichotomous branching. (E) Lung tissues of rabbits treated with the combination of SCY2.5+ISA40 reveal rare foci of fungal elements that consist of two populations of structures, one of which appears only as faint shadow-like remnants of severely damaged hyphae and the other population as truncated, distorted, and minimally branching hyphal structures.
Safety.
There were no significant differences in serum creatinine, urea nitrogen transaminases, and bilirubin among the treatment groups (see Table S1 in the supplemental material).
DISCUSSION
This study found that the combination of ibrexafungerp and isavuconazole in dosages of SCY2.5+ISA40 and SCY7.5+ISA40 was more active than either agent alone as measured by increased survival, reduced fungal pathogen-mediated pulmonary injury, as well as decreased galactomannan antigenemia and serum (1→3)-β-d-glucan levels in treatment of experimental invasive pulmonary aspergillosis in persistently neutropenic rabbits. The improvement of survival correlated in parallel with a similar pattern of reductions of residual pulmonary fungal burden, pathogen-mediated pulmonary injury as reflected by decreased lung weights, and lower pulmonary infarct scores in comparison to those of animals treated with the single agents.
We hypothesized that ibrexafungerp would be synergistically active, possessing similar properties to that of echinocandins. As an inhibitor of the biosynthesis of cell wall (1→3)-β-d-glucan, ibrexafungerp has in vitro activity against Candida spp. and Aspergillus spp. (13, 14). Ibrexafungerp also has demonstrated in vivo activity against Candida spp., including echinocandin-resistant strains (15–17). Isavuconazole was selected as the preferred antifungal triazole in view of its clinical anti-Aspergillus activity comparable to that of voriconazole but with an improved safety profile, better tolerability, fewer drug-drug interactions, and more predictable plasma pharmacokinetics (18–20).
In vitro activity combination studies demonstrated that ibrexafungerp had synergistic to additive interaction with isavuconazole against several Aspergillus spp., including A. fumigatus, Aspergillus flavus, Aspergillus terreus, and Aspergillus niger by Lowe additivity and Bliss surface analysis (12, 21). In vitro activity combination studies for SCY+ISA by Lowe additivity analysis demonstrated additive activity (FICI = 0.68 [0.38 to 1.06]) for isolates of A. fumigatus. Conversely, when measured by Bliss independence response surface analysis, the SCY+ISA combination resulted in synergistic interaction against all other tested Aspergillus spp., including A. flavus, A. terreus, and A. niger. The greatest synergistic interaction was observed for A. fumigatus (21).
Consistent with these in vitro observations, the studies of experimental invasive pulmonary aspergillosis herein also demonstrated significantly greater antifungal efficacy of the combination of ibrexafungerp, at safely achievable plasma concentrations, and isavuconazole. The significantly greater survival is likely related to the synergistic antifungal activity and reduction of pathogen-medicated pulmonary injury.
Both in vitro and in vivo studies of ibrexafungerp demonstrated damage to hyphal forms of A. fumigatus. Organisms treated in vivo revealed truncated, distorted, and irregularly branched hyphae in tissues of animals treated with single-agent ibrexafungerp at 2.5 mg/kg/day and 7.5 mg/kg/day. However, this damage in a profoundly neutropenic host did not translate into a clinically meaningful impact on outcome parameters of survival, residual fungal burden, pulmonary injury, or changes in serum galactomannan or serum (1→3)-β-d-glucan. By comparison, treatment with isavuconazole and ibrexafungerp affecting the cell membrane and cell wall, respectively, resulted in vitro and in vivo in sufficiently severe hyphal damage that translated into significantly improved survival, reduced residual fungal burden, decreased pulmonary injury, and decreased serum galactomannan and serum (1→3)-β-d-glucan. We have previously observed that this simultaneous inhibition of the biosynthesis of (1→3)-β-d-glucan in the fungal cell wall by echinocandins and ergosterol biosynthesis in the fungal cell membrane by an antifungal triazole in combination consistently resulted in a synergistic interaction in vivo.
The histopathologically documented damage to hyphal elements, especially in combination therapy, suggests a synergistic damage to both cell wall and cell membrane in vivo as evidenced by the paucity of fungal elements and the appearance of minimally staining remnants of nonbranching truncated hyphae. Such hyphal fragments were not found to involve blood vessels, resulting in lowered angioinvasion, reduced pathogen-mediated pulmonary injury, and improved survival.
This reduction in pathogen-mediated pulmonary injury and improved survival in rabbits treated with combination therapy was also paralleled by significant decline in serum galactomannan antigenemia and serum (1→3)-β-d-glucan levels. This decline in serum GMI and serum (1→3)-β-d-glucan levels in response to antifungal therapy of IPA may be useful as primary or secondary endpoints in a clinical trial of combination therapy.
The primary goal of this study was to evaluate the efficacy of ibrexafungerp and isavuconazole against experimental invasive pulmonary aspergillosis in a well-established and validated persistently neutropenic New Zealand White (NZW) rabbit model. Although these experiments used only one isolate of A. fumigatus, the in vitro activity of ibrexafungerp and isavuconazole against additional isolates of A. fumigatus demonstrated similar activity to those of the isolate used herein, suggesting the applicability of findings from this study. The isolate of A. fumigatus, which was used in our previous studies, has demonstrated consistent and reproducible experimental infection that has been predictive of therapeutic outcome in repeated clinical trials. Further in vivo studies using additional strains of A. fumigatus with high MICs could provide valuable insight into potential clinical utility of the combination of ibrexafungerp and isavuconazole against resistant A. fumigatus isolates.
The use of an orally bioavailable cell wall inhibitor of (1→3)-β-d-glucan synthesis, such as ibrexafungerp, in combination with an orally administered antifungal triazole has important implications for the management of invasive aspergillosis. Patients could be treated on an ambulatory basis with combination therapy initially, allowing early discharge from hospital and improved quality of life while receiving a synergistic combination.
These laboratory studies have established the foundation for a carefully designed phase II clinical trial (SCYNERGIA) to study the safety, tolerability, and antifungal efficacy of the combination of ibrexafungerp and voriconazole in targeted immunocompromised patients with IPA (ClinicalTrials registration number NCT03672292) (22). The data derived from such a clinical trial are critical to informing the design of a subsequent randomized phase III trial.
MATERIALS AND METHODS
Fungal isolate.
Aspergillus fumigatus isolate NIH-4215 (ATCC MYA-1163), as previously described (23), obtained from a patient with a fatal case of pulmonary aspergillosis, was used in this study. This isolate has been extensively used in previous studies for investigation of antifungal agents against invasive pulmonary aspergillosis for more than 2 decades. The MIC of isavuconazole and minimum effective concentration (MEC) of ibrexafungerp against A. fumigatus, determined according to CLSI standard (M38-A2) microdilution methods (24), were 1 μg/ml and 0.06 μg/ml, respectively.
Antifungal agents.
Ibrexafungerp (SCY-078; Scynexis, Inc., Jersey City, NJ) and isavuconazole (ISA; Astellas Pharma Global Development, Inc., Northbrook, IL) were used in this study. Ibrexafungerp and isavuconazole were provided in a lyophilized powder form in sterile vials and were prepared and preserved according to the manufacturer’s instructions. The intravenous infusion formulation of ibrexafungerp was used in studies. The oral solution of isavuconazole was used in the studies. The combination of ibrexafungerp with isavuconazole was investigated for pharmacokinetics, pharmacodynamics, and antifungal efficacy against pulmonary aspergillosis.
In vitro activity combination studies.
The combination of ibrexafungerp with isavuconazole was tested against A. fumigatus in triplicate with an in vitro broth microdilution checkerboard assay in 96-well flat bottom microtitration plates (Corning Incorporated, Corning, NY) based on the CLSI M-38A method as previously described (25). Two-fold serial dilutions of compounds were prepared in 50 μl of RPMI 1640 buffered at pH 7.0 with 0.165 M morpholinepropanesulfonic acid (MOPS). After inoculation with 100 μl of 4 × 104 CFU/ml prepared from 5- to 7-day-old cultures on potato dextrose agar, microtiter plates were incubated (Steri-Cult 200 incubator; DoveBid, Inc., CA) at 35°C for 48 h. Growth in each well was quantified spectrophotometrically at 405 nm using 16-scan points per well spectrophotometer (ELx808; BioTek Instruments, Winooski, VT). The percentage of growth inhibition in each well was calculated based on the following equation: 100% − (optical density at 405 nm [OD405]) of a well – background OD405)/(OD405 of the drug-free well – background OD405 of the drug-free well) × 100%. Background OD405 values were measured from a plate inoculated with a conidia-free inoculum and handled in the same way as the inoculated plates with the conidia-containing inoculum.
(i) Fractional inhibitory concentration index analysis.
The FIC index model expressed as ΣFIC = FICA + FICB = CAcomb/MICAalone + CBcomb/MICBalone, where MICAalone and MICBalone are the MICs of the drugs A and B when acting alone and CAcomb and CBcomb are concentrations of the drugs A and B at the isoeffective combinations, respectively. In order to capture both synergistic and antagonistic interactions among all fractional inhibitory concentrations (FICs) calculated for each checkerboard data set, the FICmin and the FICmax are determined as the lowest and highest FIC, respectively. Off-scale MICs are converted to the next highest or next lowest doubling concentration. Finally, the median and the range of FIC indices among the isolates of a given species are determined (21).
(ii) Pharmacodynamic Bliss independence-based drug interaction analysis.
As previously reported (26), Bliss independence is described by the equation EIND = EA + EB − EA × EB, for a certain combination of x mg/liter of drug A and y mg/liter of drug B. EA is the percentage of fungal growth inhibition at x mg/liter of drug A alone, EB is the percentage of fungal growth inhibition at y mg/liter of drug B alone, and EIND is the expected percentage of fungal growth inhibition of a noninteractive (independent) theoretical combination of x mg/liter of drug A with y mg/liter of drug B. The difference (ΔE = EOBS − EIND) between the expected percentage of growth inhibition EIND and the experimentally observed percentage of growth inhibition EOBS describes the interaction of each combination of the concentrations of the two drugs. If ΔE and its 95% confidence interval (CI) were >0 (i.e., EOBS > EIND and hence more growth inhibition is observed than if the two drugs were acting independently), Bliss synergy is concluded for that particular combination. If ΔE and its 95% CI were <0 (i.e., EOBS < EIND and hence less growth inhibition is observed than if the two drugs were acting independently), Bliss antagonism is concluded for that particular combination. In any other case where the 95% CI of ΔE includes 0, the conclusion is Bliss independence.
Animals.
Healthy female New Zealand White rabbits (Covance Research Products, Inc., Denver, PA) weighing 2.6 to 3.5 kg at the time of endotracheal inoculation were used in replicate experiments. All rabbits were monitored under humane care and use of standards in facilities, accredited by the Association for Assessment and Accreditation of Laboratory Animal Care International, and according to the guidelines of the National Research Council (27) for the care and use of laboratory animals and under the approval of the Institutional Animal Care and Use Committee. Rabbits were individually housed and maintained with water and standard rabbit feed ad libitum. Atraumatic vascular access was established by modified surgical placement of a Silastic tunneled central venous catheter as previously described elsewhere (28). The Silastic catheter permitted nontraumatic venous access for administration of parental agents and for repeated blood sampling for studies of plasma pharmacokinetics, serum galactomannan antigen testing and serum (1→3)-β-d-glucan levels, biochemical, and hematological parameters.
Plasma pharmacokinetics of ibrexafungerp. (i) Single-dose pharmacokinetics.
Six healthy rabbits per dosage group received ibrexafungerp at 7.5, 15, and 30 mg/kg as intravenous (i.v.) infusion. Blood samples were drawn from each rabbit receiving ibrexafungerp at the following time points: baseline, 0.5 h, 1 h, 2 h, 4 h, 8 h, 12 h, 18 h, 24 h, and 48 h. Plasma was immediately separated by centrifugation and stored at –80°C until assayed.
(ii) Optimal sampling pharmacokinetics in infected rabbits.
The plasma pharmacokinetics of ibrexafungerp was investigated in four to six animals infected with A. fumigatus per each dosage cohort of 7.5, 15, and 30 mg/kg. Time points for sampling were determined by inspection of full plasma concentration profiles obtained in normal healthy rabbits following administration of similar dosages based upon previous plasma pharmacokinetic studies. Plasma sampling was performed on day 6 of antifungal therapy. Blood samples were drawn at baseline and at 0.5 h, 1 h, 2 h, 4 h, 8 h, and 24 h postdosing. Plasma was immediately separated by centrifugation and stored at –80°C until assayed.
Study groups of antifungal treatment.
Ibrexafungerp was administered i.v. at 2.5 (SCY2.5) and 7.5 (SCY7.5) mg/kg/day over 5 min. The prodrug isavuconazonium sulfate, which is equivalent to the active moiety isavuconazole (ISA), was administered orally (p.o.) at 40 mg/kg/day (ISA40). For combination groups of SCY2.5+ISA40 and SCY7.5+ISA40, ibrexafungerp was administered i.v. over approximately 5 min and then was followed by p.o. administration of isavuconazole. Antifungal treatment was started 24 h after endotracheal administration of the A. fumigatus inoculum and continued once daily for up to 12 days.
Inoculum and inoculation.
For each study, an inoculum of 1 × 108 to 1.25 × 108 conidia of A. fumigatus in a volume of 250 μl to 350 μl was prepared. Inoculation was performed on day 2 of the experiments while rabbits were under general anesthesia (0.5 to 0.6 ml of a 2:1 mixture [vol/vol] of ketamine 100 mg/ml and xylazine 20 mg/ml administered intravenously) as described previously (23).
Immunosuppression and maintenance of neutropenia.
Immunosuppression and profound persistent neutropenia (a neutrophil concentration of <100 neutrophils/μl) was established and maintained using cytarabine (Ara-C) (Cytarabine injection; Zydus Hospira Oncology Private Ltd., Gujarat, India, for Hospira, Inc., Lake Forest, IL) and methylprednisolone (Solu-Medrol; Pfizer for Pharmacia & Upjohn Co., Division of Pfizer Inc., New York, NY) as described previously (23). Antibiotics (ceftazidime, gentamicin, vancomycin) were used for prevention of opportunistic bacterial infections during neutropenia (23).
Outcome variables.
The following panel of outcome variables was used to assess antifungal efficacy: survival, pulmonary infarct scores, lung weights, and residual fungal burden (log CFU/g). The outcome variable panel was applied to all study rabbits when possible.
Survival.
The survival time in days postinoculation was recorded for each rabbit in each group. Following humane end points, rabbits were euthanized by intravenous administration of pentobarbital (65 mg of pentobarbital sodium/kg of body weight; Beuthanasia-D Special [euthanasia solution]; Schering-Plough Animal Health Corp., Union, NJ) on day 13 postinoculation, 24 h after the last dose of study drug (23).
Pulmonary lesion scores, lung weights, and residual fungal burden.
The lungs were carefully resected at autopsy. Pulmonary lesion scores and lung weights were assessed and calculated as previously described (23). Lung tissue from each rabbit was sampled and cultured by a standard excision of tissue from each lobe as previously described (23). The number of CFU of A. fumigatus was counted and recorded for each lobe, and CFU per gram was calculated.
Bronchoalveolar lavage.
BAL was performed, as described previously (29), on each lung preparation by the instillation of 10 ml of sterile normal saline into the clamped trachea with a sterile 12-ml syringe and subsequent withdrawal. The instillations repeated twice. The lavage was then centrifuged for 10 min at 400 × g. Part of the supernatant was discarded, leaving 2 ml of pellet with supernatant, which was then vortexed. An aliquot of 100 μl of this fluid and 100 μl of a dilution (101) of this fluid was cultured on 5% Sabouraud dextrose agar plates.
Detection of serum galactomannan antigen.
Serum samples from each rabbit were collected every other day and stored at –80°C before analysis. Galactomannan antigen, expressed as galactomannan index (GMI), was determined in serial serum samples and BAL fluid obtained postmortem by one-stage immunoenzymatic sandwich microplate assay method (30) (Platelia Aspergillus enzyme immunoassay [EIA]; Bio-Rad, Marnes la Coquette, France) according to the manufacturer’s instructions and as described elsewhere (29). Enzyme immunoassay data were expressed as a serum GMI plotted over time. The GMI for each test serum or BAL fluid sample was equal to the absorbance of a standard sample divided by the absorbance of a threshold serum provided by the manufacturer. A GMI of less than 0.5 was considered negative.
Detection of (1→3)-β-d-glucan levels.
Serum from each rabbit was collected every other day for determination of (1→3)-β-d-glucan levels by using a colorimetric assay (Fungitell; Associates of Cape Cod, Inc.) read at 405 nm (with 490 nm background subtraction) based on para-nitroanilide absorption at that wavelength, performed according to the manufacturer’s instructions, and described in detail elsewhere (31). The (1→3)-β-d-glucan levels were determined by taking the mean optical density of the duplicate readings and comparing them with the standard curve of predetermined concentrations. Interpretation of (1→3)-β-d-glucan values, according to manufacturer’s instructions, was as follows: <60 pg/ml, negative; 60 to 79 pg/ml, indeterminate; ≥80 pg/ml, positive. The median correlation coefficient of the standard curves performed in these studies was an r of ≥0.9992 (range of 0.9982 to 0.9998).
Histopathology.
Pulmonary lesions were excised and fixed in 10% neutral buffered formalin. Paraffin-embedded tissue sections were then sectioned and stained with Grocott-Gomori methenamine-silver stain. Tissues were microscopically examined for pulmonary injury and structural changes in Aspergillus hyphae.
Statistical analysis.
Comparisons between the study groups were performed by Kruskal-Wallis test (nonparametric analysis of variance [ANOVA]) or the Mann-Whitney U-test, as appropriate. A two-tailed P value of ≤0.05 was considered to be statistically significant. Survival was plotted by Kaplan-Meier analysis. Differences in survival of treatment groups and untreated controls were analyzed by log rank test. Values were expressed as means ± standard error of the means (SEMs). Pharmacokinetic parameters were compared using ANOVA or Student's t test, as appropriate.
Supplementary Material
ACKNOWLEDGMENTS
This study was supported in part by an investigator-initiated grant from Scynexis, Inc. to Weill Cornell Medicine. T.J.W. is a Scholar of the Save our Sick Kids Foundation.
T.J.W. has received grants for experimental and clinical antimicrobial pharmacology and therapeutics to his institution from Scynexis, Inc., and served as a consultant to Astellas, ContraFect, Drais, iCo, Novartis, Pfizer, MethylGene, Sigma-Tau, and Trius. S.B, K.B.-E., N.A., and D.A. are employees of Scynexis, Inc. Other authors have no interests to declare.
Footnotes
Supplemental material is available online only.
REFERENCES
- 1.Kontoyiannis DP, Marr KA, Park BJ, Alexander BD, Anaissie EJ, Walsh TJ, Ito J, Andes DR, Baddley JW, Brown JM, Brumble LM, Freifeld AG, Hadley S, Herwaldt LA, Kauffman CA, Knapp K, Lyon GM, Morrison VA, Papanicolaou G, Patterson TF, Perl TM, Schuster MG, Walker R, Wannemuehler KA, Wingard JR, Chiller TM, Pappas PG. 2010. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) database. Clin Infect Dis 50:1091–1100. doi: 10.1086/651263. [DOI] [PubMed] [Google Scholar]
- 2.Kosmidis C, Denning DW. 2015. The clinical spectrum of pulmonary aspergillosis. Thorax 70:270–277. doi: 10.1136/thoraxjnl-2014-206291. [DOI] [PubMed] [Google Scholar]
- 3.Patterson TF. 2009. Risk stratification for invasive aspergillosis: early assessment of host susceptibility. Med Mycol 47(Suppl):S255–S260. doi: 10.1080/13693780902718339. [DOI] [PubMed] [Google Scholar]
- 4.Rubio PM, Sevilla J, González-Vicent M, Lassaletta A, Cuenca-Estrella M, Díaz MA, Riesco S, Madero L. 2009. Increasing incidence of invasive aspergillosis in pediatric hematology oncology patients over the last decade: a retrospective single centre study. J Pediatr Hematol Oncol 31:642–646. doi: 10.1097/MPH.0b013e3181acd956. [DOI] [PubMed] [Google Scholar]
- 5.Valdez JM, Scheinberg P, Young NS, Walsh TJ. 2009. Infections in patients with aplastic anemia. Semin Hematol 46:269–276. doi: 10.1053/j.seminhematol.2009.03.008. [DOI] [PubMed] [Google Scholar]
- 6.Ghannoum M, Long L, Isham N, Hager C, Wilson R, Borroto-Esoda K, Barat S, Angulo D. 2019. Activity of a novel 1,3-beta-d-glucan synthase inhibitor, ibrexafungerp (formerly SCY-078), against Candida glabrata. Antimicrob Agents Chemother 63:e01510-19. doi: 10.1128/AAC.01510-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.McCarthy MW, Walsh TJ. 2018. Candidemia in the cancer patient: diagnosis, treatment, and future directions. Expert Rev Anti Infect Ther 16:849–854. doi: 10.1080/14787210.2018.1536546. [DOI] [PubMed] [Google Scholar]
- 8.Jimenez-Ortigosa C, Paderu P, Motyl MR, Perlin DS. 2014. Enfumafungin derivative MK-3118 shows increased in vitro potency against clinical echinocandin-resistant Candida species and Aspergillus species isolates. Antimicrob Agents Chemother 58:1248–1251. doi: 10.1128/AAC.02145-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pfaller MA, Messer SA, Rhomberg PR, Borroto-Esoda K, Castanheira M. 2017. Differential activity of the oral glucan synthase inhibitor SCY-078 against wild-type and echinocandin-resistant strains of Candida species. Antimicrob Agents Chemother 61:e00161-17. doi: 10.1128/AAC.00161-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Schell WA, Jones AM, Borroto-Esoda K, Alexander BD. 2017. Antifungal activity of SCY-078 and standard antifungal agents against 178 clinical isolates of resistant and susceptible Candida species. Antimicrob Agents Chemother 61:e01102-17. doi: 10.1128/AAC.01102-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ledoux MP, Toussaint E, Denis J, Herbrecht R. 2017. New pharmacological opportunities for the treatment of invasive mould diseases. J Antimicrob Chemother 72:i48–i58. doi: 10.1093/jac/dkx033. [DOI] [PubMed] [Google Scholar]
- 12.Ghannoum M, Long L, Larkin EL, Isham N, Sherif R, Borroto-Esoda K, Barat S, Angulo D. 2018. Evaluation of the antifungal activity of the novel oral glucan synthase inhibitor SCY-078, singly and in combination, for the treatment of invasive aspergillosis. Antimicrob Agents Chemother 62:e00244-18. doi: 10.1128/AAC.00244-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pfaller MA, Messer SA, Motyl MR, Jones RN, Castanheira M. 2013. In vitro activity of a new oral glucan synthase inhibitor (MK-3118) tested against Aspergillus spp. by CLSI and EUCAST broth microdilution methods. Antimicrob Agents Chemother 57:1065–1068. doi: 10.1128/AAC.01588-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Pfaller MA, Messer SA, Motyl MR, Jones RN, Castanheira M. 2013. Activity of MK-3118, a new oral glucan synthase inhibitor, tested against Candida spp. by two international methods (CLSI and EUCAST). J Antimicrob Chemother 68:858–863. doi: 10.1093/jac/dks466. [DOI] [PubMed] [Google Scholar]
- 15.Lepak AJ, Marchillo K, Andes DR. 2015. Pharmacodynamic target evaluation of a novel oral glucan synthase inhibitor, SCY-078 (MK-3118), using an in vivo murine invasive candidiasis model. Antimicrob Agents Chemother 59:1265–1272. doi: 10.1128/AAC.04445-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wiederhold NP, Najvar LK, Jaramillo R, Olivo M, Pizzini J, Catano G, Patterson TF. 2018. Oral glucan synthase inhibitor SCY-078 is effective in an experimental murine model of invasive candidiasis caused by WT and echinocandin-resistant Candida glabrata. J Antimicrob Chemother 73:448–451. doi: 10.1093/jac/dkx422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Wring SA, Randolph R, Park S, Abruzzo G, Chen Q, Flattery A, Garrett G, Peel M, Outcalt R, Powell K, Trucksis M, Angulo D, Borroto-Esoda K. 2017. Preclinical pharmacokinetics and pharmacodynamic target of SCY-078, a first-in-class orally active antifungal glucan synthesis inhibitor, in murine models of disseminated candidiasis. Antimicrob Agents Chemother 61:e02068-16. doi: 10.1128/AAC.02068-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Andes D, Kovanda L, Desai A, Kitt T, Zhao M, Walsh TJ. 2018. Isavuconazole concentration in real-world practice: consistency with results from clinical trials. Antimicrob Agents Chemother 62:e00585-18. doi: 10.1128/AAC.00585-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kovanda LL, Kolamunnage-Dona R, Neely M, Maertens J, Lee M, Hope WW. 2017. Pharmacodynamics of isavuconazole for invasive mold disease: role of galactomannan for real-time monitoring of therapeutic response. Clin Infect Dis 64:1557–1563. doi: 10.1093/cid/cix198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Perfect JR, Cornely OA, Heep M, Ostrosky-Zeichner L, Mullane KM, Maher R, Croos-Dabrera R, Lademacher C, Engelhardt M, Chen C, Marty FM. 2018. Isavuconazole treatment for rare fungal diseases and for invasive aspergillosis in patients with renal impairment: challenges and lessons of the VITAL trial. Mycoses 61:420–429. doi: 10.1111/myc.12769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Petraitis V, Kavaliauskas P, Planciuniene R, Virgailis M, Petraitiene R, Barat S, Borroto-Esoda K, Angulo D, Walsh TJ. 2018. In vitro activity of SCY-078 in combination with isavuconazole or amphotericin B against medically important moulds, abstr 498. ASM Microbe 2018. ASM, Atlanta, GA. [Google Scholar]
- 22.Scynexis, Inc. 2019. Study to evaluate the safety and efficacy of the combination therapy of ibrexafungerp (SCY-078) with voriconazole in patients with invasive pulmonary aspergillosis (SCYNERGIA). ClinicalTrials registration no. NCT03672292. https://clinicaltrials.gov/ct2/show/NCT03672292.
- 23.Petraitis V, Petraitiene R, Sarafandi AA, Kelaher AM, Lyman CA, Casler HE, Sein T, Groll AH, Bacher J, Avila NA, Walsh TJ. 2003. Combination therapy in treatment of experimental pulmonary aspergillosis: synergistic interaction between an antifungal triazole and an echinocandin. J Infect Dis 187:1834–1843. doi: 10.1086/375420. [DOI] [PubMed] [Google Scholar]
- 24.Clinical and Laboratory Standards Institute. 2008. Reference method for broth dilution antifungal susceptibility testing of filamentous fungi; approved Standard—2nd ed. CLSI document M38-A2. Clinical and Laboratory Standards Institute, Wayne, PA. [Google Scholar]
- 25.Katragkou A, McCarthy M, Meletiadis J, Petraitis V, Moradi PW, Strauss GE, Fouant MM, Kovanda LL, Petraitiene R, Roilides E, Walsh TJ. 2014. In vitro combination of isavuconazole with micafungin or amphotericin B deoxycholate against medically important molds. Antimicrob Agents Chemother 58:6934–6937. doi: 10.1128/AAC.03261-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Meletiadis J, Mouton JW, Meis JF, Verweij PE. 2003. In vitro drug interaction modeling of combinations of azoles with terbinafine against clinical Scedosporium prolificans isolates. Antimicrob Agents Chemother 47:106–117. doi: 10.1128/aac.47.1.106-117.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.National Research Council. 2011. Guide for the care and use of laboratory animals, 8th ed National Academies Press, Washington, DC. [Google Scholar]
- 28.Walsh TJ, Bacher J, Pizzo PA. 1988. Chronic silastic central venous catheterization for induction, maintenance and support of persistent granulocytopenia in rabbits. Lab Anim Sci 38:467–471. [PubMed] [Google Scholar]
- 29.Petraitiene R, Petraitis V, Groll AH, Sein T, Piscitelli S, Candelario M, Field-Ridley A, Avila N, Bacher J, Walsh TJ. 2001. Antifungal activity and pharmacokinetics of posaconazole (SCH 56592) in treatment and prevention of experimental invasive pulmonary aspergillosis: correlation with galactomannan antigenemia. Antimicrob Agents Chemother 45:857–869. doi: 10.1128/AAC.45.3.857-869.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Stynen D, Sarfati J, Goris A, Prevost MC, Lesourd M, Kamphuis H, Darras V, Latge JP. 1992. Rat monoclonal antibodies against Aspergillus galactomannan. Infect Immun 60:2237–2245. doi: 10.1128/IAI.60.6.2237-2245.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Petraitiene R, Petraitis V, Hope WW, Mickiene D, Kelaher AM, Murray HA, Mya-San C, Hughes JE, Cotton MP, Bacher J, Walsh TJ. 2008. Cerebrospinal fluid and plasma (1→3)-beta-d-glucan as surrogate markers for detection and monitoring of therapeutic response in experimental hematogenous Candida meningoencephalitis. Antimicrob Agents Chemother 52:4121–4129. doi: 10.1128/AAC.00674-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.