

Abstract
Extramedullary (EM) disease in patients with acute myeloid leukemia (AML) is a known phenomenon. Since the prevalence of EM AML has so far only been clinically determined on examination, we performed a prospective study in patients with AML. The aim of the study was to determine the prevalence of metabolically active EM AML using total body 18Fluorodesoxy-glucose positron emission tomography/computed tomography (18FDG-PET/CT) imaging at diagnosis prior to initiation of therapy. In order to define the dynamics of EM AML throughout treatment, PET-positive patients underwent a second 18FDG-PET/CT imaging series during follow up by the time of remission assessment. A total of 93 patients with AML underwent 18FDG-PET/CT scans at diagnosis. The prevalence of PET-positive EM AML was 19% with a total of 65 EM AML manifestations and a median number of two EM manifestations per patient (range, 1-12), with a median maximum standardized uptake value of 6.1 (range, 2-51.4). When adding those three patients with histologically confirmed EM AML who were 18FDG-PET/CT negative in the 18FDG-PET/CT at diagnosis, the combined prevalence for EM AML was 22%, resulting in 77% sensitivity and 97% specificity. Importantly, 60% (6 of 10) patients with histologically confirmed EM AML still had active EM disease in their follow up 18FDG-PET/CT. 18FDG-PET/CT reveals a high prevalence of metabolically active EM disease in AML patients. Metabolic activity in EM AML may persist even beyond the time point of hematologic remission, a finding that merits further prospective investigation to explore its prognostic relevance. (Trial registered at clinicaltrials.gov identifier: 01278069.)
Introduction
Acute myeloid leukemia (AML) may present with either concomitant or isolated extramedullary (EM) AML, also termed myeloid sarcoma (MS). EM AML is defined by infiltrating AML blasts effacing normal tissue as demonstrated by histological evaluation.1 Data on the prevalence of EM AML are based on retrospective or clinical analyses, and they possibly under-estimate the true prevalence, since they rely on findings from physical examination only or on coincidental findings in standard imaging procedures. Others have performed retrospective analyses from autopsy series, which might over-estimate the prevalence of EM AML, since these series accumulate data on AML patients succumbing to their disease. So far, EM AML prevalence has been seen to range from 2.5% to 9.1%.2,3 Previous studies and AML treatment recommendations identified EM AML as an adverse prognostic factor in patients with AML.4 In contrast, a recent retrospective analysis based on clinical data from a large number of AML patients included in clinical trials revealed a high proportion of patients with EM AML (23.7%), but could not identify EM AML as an independent prognostic factor.5 Nevertheless, this analysis and others also included patients with, for example, hepatomegaly and/or splenomegaly, gingival hyperplasia based on clinical examination, suggesting these represent EM AML or leukemic meningitis. These findings per se do not fulfill the criteria for EM AML.5,6 However, without a precise assessment of EM AML, valid risk factor analyses cannot be performed. 18Fluorodesoxy-glucose positron emission tomography/computed tomography (18FDG-PET/CT) is able to detect highly metabolic tissue and has proven efficacy in imaging studies for various types of malignant diseases. We and others have demonstrated the utility of 18FDG-PET/CT imaging in AML patients with histologically proven EM AML.7–13 We were able to demonstrate a sensitivity of 90% using 18FDG-PET/CT imaging and found additional EM sites in 60% of the patients.8 Another study in ten unselected AML patients using 18Fluorodeoxythymidine-PET discovered EM AML in 4 of 10.14 Prospective studies to assess the prevalence of EM disease in AML in unselected patients have, so far, not been performed. The aim of this prospective, observational study was to use 18FDG-PET/CT to determine the prevalence of EM AML in patients prior to initiation of AML therapy.
Methods
This open, prospective observational study was approved by the institutional review board (EK309102009) and registered at clinicaltrials.gov identifier: 01278069. Informed consent was collected prior to the first PET scan. Patients with AML aged 18-80 years underwent baseline total body 18FDG-PET/CT scans before initiation of therapy. Patients were included only if a delay of ≤5 days of initiation of treatment was clinically justifiable in order to perform the study.15 Hydroxyurea for disease control was admissible before the 18FDG-PET/CT. The primary objective of this study was to determine the prevalence of EM AML at diagnosis. The sample size was calculated such that the width of the 95% confidence interval (CI) would stay within 20%. Assuming a prevalence of 40% EM AML, 93 patients would need to be studied. The prevalence of 40% was based on the only data available at the time from a case series of ten unelected patients undergoing PET/CT scanning, demonstrating existence of EM AML in 4 of those 10 patients.14 This trial was not powered to compare survival differences in EM AML as compared to AML patients without EM. Since there is no evidence to indicate that the treatment of AML patients with EM manifestation of AML needs to be intensified or modified, the presence of EM AML was not part of the decision-making process for treatment of these patients.
In total, 106 patients were screened for the study between February 2011 and July 2013 in the Department of Haematology of the University Hospital Dresden. Of those, 13 patients were considered to be screening failures and were not considered for further analyses, such that the planned sample size of 93 patients was reached. Reasons for screening failure were: age >80 years or 18FDG-PET/CT not feasible due to the clinical condition of the patient (n = 7) or other (n=6). Interestingly, two of these 13 patients had EM AML (histologically confirmed diagnosis in one patient and clinical diagnosis in the other). Patients with PET-positive EM AML at baseline underwent a second 18FDG-PET/CT scan after therapy initiation either at the date of complete remission or until day 60 in case of not achieving CR. A complete diagram of screened and included patients is shown in Figure 1. Hybrid 18FDG-PET/CT scans were performed as recently published using a Siemens Sensation 16 as part of a bio-graph (Siemens, Knoxville, TN, USA) with intravenous application of 18FDG and 120 mL contrast media Ultravist 370 (Bayer Schering Pharma, Leverkusen, Germany).8 PET 3-dimensional emission scans were conducted with a median activity of 367 MBq (range, 223-433 Mbq), as recently published.8 For assessment of 18FDG-PET/CT imaging, no specific threshold or metabolic activity (e.g. maximum standardized uptake value, SUVmax) was applied. Instead, subtle correlation of any 18FDG-positive lesion with the fused CT images was performed to detect a corresponding tissue proliferation before suspecting an EM manifestation of AML. In cases in which no morphological correlate was apparent, 18FDG-positive lesions were declared to be unspecific. The estimated prevalence of EM AML was ascertained by calculating the specificity of baseline 18FDG-PET/CT positivity in relation to those EM AML lesions confirmed positive for EM AML upon histology. Thereafter, the total number of baseline 18FDG-PET/CT positive EM AML patients was multiplied by this specificity to derive an estimate for the prevalence in the total sample of 93. A CI with at least 95% coverage was derived by calculating the exact Clopper-Pearson-Confidence Intervals. Complete remission (CR) was defined according to the standard consensus criteria.16 The Mann-Whitney U-test was used to compare continuous variables between patient groups, while the χ2-test was applied to categorical variables. All statistical analyses were performed using SPSS version 25 (SPSS Inc., Chicago, IL, USA); two-sided tests were applied. P<0.05 was considered statistically significant.
Figure 1.

Modified CONSORT diagram demonstrating screening, patient selection and analysis for the complete patient cohort. PETAML: PET-CT in AML for Detection of Extramedullary AML Manifestations study; n: number; 18FDG-PET/CT: 18Fluorodesoxy-glucose positron emission tomography/computed tomography; EM: extramedullary; AML: acute myeloid leukemia.
Results
Patient population and safety
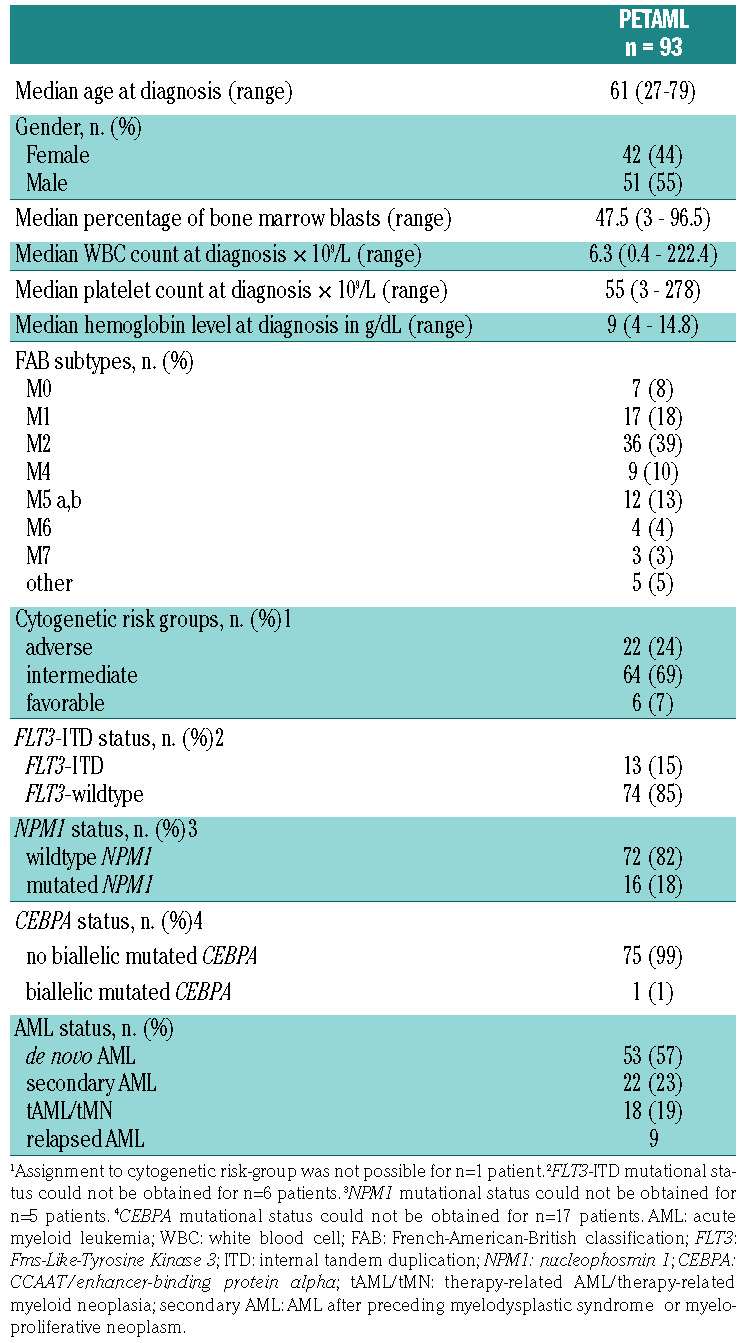
A total of 93 patients with AML (n=9 with relapsed AML) underwent total body 18FDG-PET/CT scans at diagnosis after giving informed consent. Median age of all patients was 61 years (range, 27-79 years). Clinical characteristics of the patient population are shown in Table 1. The majority were diagnosed with de novo AML (n=53, 57%) while 22 patients (23%) had secondary AML after preceding myelodysplastic syndrome (MDS)/myeloproliferative neoplasm (MPN), and n=18 (19%) patients had therapy-related AML (tAML)/therapy-related MPN (tMN). Median follow up of alive patients is 46 months (range, 5-60 months). There were no adverse reactions due to the application of intravenous 18FDG and intravenous contrast media. No deterioration in renal function, as determined by measurement of creatinine serum levels and estimation of GFR (eGFR) by Cockroft-Gault, was observed after 18FDG-PET/CT imaging.
Table 1.
Patients’ characteristics at diagnosis.
Prevalence and sites
Total body 18FDG-PET/CT imaging detected highly metabolic manifestations suggestive of EM AML in 23% of the enrolled patients (n=21). Of these 18FDG-PET positive patients, 11 (52%) had de novo AML, while 7 (33%) had tAML and 3 (14%) secondary AML with preceding MDS/MPN. In total, 65 EM AML manifestations were identified with 18FDG-PET/CT in these 21 patients. The median SUVmax was 6.1 (range, 2-51.4). Patients with EM AML as per 18FDG-PET/CT had a median of two EM AML manifestations (range, 1-12) with only six patients having only one EM AML manifestation; exemplary 18FDG-PET/CT imaging is depicted in Figures 2A and B and 3A and 3B. Sites of EM AML as detected per 18FDG-PET/CT were connective tissue (n=4, one patient paravertebral, one paraaortic, one next to the jaw angle, and one at the base of the tongue), parenchymal tissues (n=8, with manifestations in adrenal glands, kidneys, liver, and spleen), and lymph nodes (n=15). A total of 9% of patients presented with clinically overt EM AML (n=8). Applying 18FDG-PET/CT, additional EM manifestations were detected in 62% (n=5) of these patients. In 12 of the 21 patients who were diagnosed with EM AML as per 18FDG-PET/CT, biopsies from EM sites were obtained in order to assess the provenance of the diagnosed tumor and to assess the sensitivity of 18FDG-PET/CT. In ten patients, histology review confirmed the occurrence of EM AML in these sites, indicating a sensitivity of 77% for 18FDG-PET/CT. Interestingly, in the two remaining patients in whom histology could not confirm EM AML, concomitant tumors were found (one patient with Castleman’s disease and one patient with a solid fibrous tumor). Extrapolating these results onto the entire cohort, and applying the positive predictive value of 83.3%, the prevalence of EM AML in our AML patient cohort was 17% (95%CI: 11-29%). When only analyzing patients with newly diagnosed AML, 16 (19%) patients were identified with EM AML as per 18FDG-PET/CT. Characteristics of patients with or without EM AML as per 18FDG-PET/CT and histological confirmation are shown in Online Supplementary Table S1. In comparison with PET-negative patients, those with PET-positive EM AML as per 18FDG-PET/CT had a higher percentage of bone marrow infiltrating blasts, higher white blood cell (WBC) count in the peripheral blood, and higher C-reactive protein serum levels. Furthermore, in the cohort of AML patients with EM disease, there were no patients with favorable cytogenetic risk and a higher fraction of patients with relapsed AML.
Figure 2.

Images of a 69-year old female patient with histologically confirmed extramedullary (EM), bilobular hepatic manifestations of acute myeloid leukemia (AML) (continuous arrows) who underwent intensive induction chemotherapy. (A) Maximum intensity projection (MIP) and (B) three representative slices of the fused multiplanar reconstructions (MPR) of the pre-therapeutic 18Fluorodesoxy-glucose positron emission tomography/computed tomography (18FDG-PET/CT). Maximum standardized uptake value (SUVmax) ranged from 5.2 to 7.4. (C) MIP of the post-therapeutic 18FDG-PET/CT confirming a complete metabolic remission of all hepatic lesions. Note the hypermetabolic focus (SUVmax 8.9) in the right thyroid lobe (dotted arrows, see also (A) at baseline) which does not reflect AML but rather a thyroid adenoma that was still present in the post-therapeutic scan (SUVmax 8.1).
Figure 3.

Images of a 63-year old female patient with histologically confirmed extramedullary (EM) manifestation of acute myeloid leukemia (AML) in the oral cavity (dotted arrows) who underwent intensive induction chemotherapy. (A) Maximum intensity projection (MIP) and (B) fused multiplanar reconstruction (MPR) of the pre-therapeutic 18Fluorodesoxy-glucose positron emission tomography/computed tomography (18FDG-PET/CT). Maximum standardized uptake value (SUVmax) was 9.1. 18FDG-PET detected a further right iliac EM AML (SUVmax 5.6; continuous arrows). (C) MIP of the post-therapeutic follow up 18FDG-PET/CT confirming the slightly regressive EM AML of the oral cavity (SUVmax 7.4) but also the progressive right iliacal EM AML (SUVmax 8.1). (D) MPR of this scan. New bicervical EM AML (dashed arrows) was also detected (E), see also (C) (SUVmax up to 9.5).
In addition, in three patients of the 18FDG-PET/CT negative group (n=72), EM AML was identified on examination and diagnosed through histological confirmation after biopsy. Two of these patients had a skin manifestation (chloroma) while one patient developed cervical lymphadenopathy during induction chemotherapy and then underwent biopsy and an additional, unscheduled 18FDG-PET/CT, both confirming the diagnosis of EM AML. When these patients were added to our extrapolated prevalence of EM AML, the combined prevalence of EM AML in this study was 22%. Thus, the specificity for 18FDG-PET/CT to detect EM AML is 97%. An overview of patients undergoing biopsy for diagnosis in both cohorts is available in the Online Supplementary Table S2. When we analyzed only the largest subgroup of our study cohort of patients with newly diagnosed AML, the combined prevalence of EM AML was 17%.
A total of 18 patients (19%) in this study were treated with hydroxyurea prior to 18FDG-PET/CT and thus prior to initiation of chemotherapy. Four of the 21 patients (19%) who were diagnosed with EM AML as per 18FDG-PET/CT were treated with hydroxyurea prior to 18FDG-PET/CT imaging.
Follow-up 18FDG-PET/CT
Patients with EM diagnosed by 18FDG-PET/CT underwent a second 18FDG-PET/CT scan at confirmation of CR or, at the latest, until day 60 after initiation of therapy in case no CR was achieved. A total of 14 of 21 patients with EM AML as per baseline 18FDG-PET/CT at diagnosis underwent a second 18FDG-PET/CT. The remaining patients did not undergo a second 18FDG-PET/CT because of severe disease and intensive care treatment (n=3), mental distress (n=1), palliative care in a hospice (n=1), and withdrawal of study consent for the second 18FDG-PET/CT (n=2). When we analyzed only the follow up18FDG-PET/CT of those patients who were 18FDG-PET/CT positive and had a positive confirmatory biopsy (n=10 patients), 60% of these patients (n=6) were still positive for EM AML as diagnosed per the second 18FDG-PET/CT. Exemplary 18FDG-PET/CT imaging of a responding and a non-responding patient (who both underwent intensive induction chemotherapy) is available in Figures 2C and 3C-E. Interestingly, of the six patients who still had EM AML (as per 18FDG-PET/CT imaging) at the time of their second 18FDG-PET/CT, four patients with EM AML and AML bone marrow infiltration at diagnosis were in CR as determined by bone marrow cytomorphology at the time of second 18FDG-PET/CT. Of those four patients who still had EM AML in their second 18FDG-PET/CT, but who were in CR as per bone marrow cytomorphology, three patients subsequently relapsed. The other two (of the six patients with persistent metabolic disease) had isolated EM AML as per 18FDG-PET/CT: one patient had unchanged EM AML manifestations in the second 18FDG-PET/CT, while the other had a progression of EM AML manifestations in the second 18FDG-PET/CT. The metabolic and numerical dynamics of EM AML manifestations in patients with histologically confirmed EM AML from baseline to follow up 18FDG-PET/CT are shown in Online Supplementary Figure 1A and B.
Discussion
Our study is the first to prospectively evaluate 18FDG-PET/CT imaging for the diagnosis of EM AML in patients with AML. Furthermore, this is the first prospective study combining 18FDG-PET/CT imaging, clinical findings, and histological examination after biopsy to systematically estimate EM AML. According to our results, 18FDG-PET/CT is a useful and safe tool to detect EM AML with a high sensitivity and specificity of 77% and 97%, respectively. While the prevalence of EM AML as per baseline 18FDG-PET/CT was 23%, we found an estimated prevalence of EM AML of 19% using 18FDG-PET/CT when including the sensitivity of 18FDG-PET/CT after histological examination of biopsied lesions. When also adding the three patients with histologically confirmed EM AML, who were initially 18FDG-PET/CT negative, the combined prevalence of the whole study cohort is 22%. An analysis of only patients with newly diagnosed AML led to a combined prevalence of EM AML of 17% in our study. This is 3-to 11-fold higher than previously reported2,3 but lower than in other reported studies.5,17,18 Some reports over-estimated the prevalence of EM AML since data were derived from autopsy studies, which have a natural selection in favor of relapsed and/or refractory patients, or because a positive selection in favor of myelomonocytic AML subtypes occurred, as these are known to have a higher likelihood of presenting with EM AML.17,18 Other studies under-estimate the prevalence of EM AML because they rely on the clinical findings of EM AML, which only represents the tip of the iceberg.3,5 Some reports also include EM AML sites in their calculation, such as gingival hyperplasia, splenomegaly or leukemic meningitis, which does not per se fulfill the World Health Organization (WHO) criteria for EM AML and therefore might over-estimate the prevalence of EM AML.5,6,17,19 A recent retrospective analysis by Ganzel et al. reported a clinical prevalence of 24% and argued that with a PET-based screening the rate of extramedullary AML would be even higher.5 The prevalence of EM AML in our study remains in that range; however, our study and the analysis by Ganzel et al. describe and discuss different EM AML characteristics. Whether leukemic meningitis, gingival hyperplasia, and splenomegaly fulfill the WHO criteria for extramedullary disease remains highly debatable. Disrupted tissue architecture by AML cells (or effaced tissue architecture) cannot be considered exclusively responsible for leukemic meningitis (but as rather resembling blood-brain-barrier migration), gingival hyperplasia (resembling indirect hyperplasia), and splenomegaly (resembling leukemic infiltration not effacing spleen architecture).1,20 Whether clinical assessment is sufficient, and whether it is necessary to biopsy EM AML, has been the subject of much discussion and controversy.5 However, our data show that a non-negligible proportion of AML patients with EM still harbor 18FDG-avid manifestations despite being in CR at the same time, as per bone marrow assessment. Since the definition of a CR of AML includes resolution of EM AML, this provides a further argument to perform sensitive 18FDG-PET/CT imaging in these patients. Furthermore, incidental findings of other hematologic malignancies such as multicentric Castleman’s disease at initial presentation of AML diagnosed in parallel in our study seem to argue for histological confirmation whenever possible. The observation that many patients with EM AML harbor more than one EM site has been suggested in our pilot study and others, and could be confirmed by this study.5,8 The phenomenon observed here that isolated EM AML of the skin (chloroma) is not necessarily 18FDG-PET-avid and thus cannot be visualized by 18FDG-PET/CT imaging has already been reported in our pilot study.8 For these patients 18FDG-PET/CT imaging might only be useful in identifying additional EM AML sites.
However, all imaging methods have limitations. 18FDG-PET/CT is limited by the size of an EM AML mass required to emit an 18FDG-PET signal. Theoretically, a cluster of at least 106 FDG avid cells is needed to meet the spatial resolution of a commercially available human PET machine and to generate a detectable PET signal. Furthermore, an objective of this trial was to include a representative AML patient cohort, since it was designed to estimate the prevalence of EM AML, and not survival differences between patients with EM AML as compared to patients without EM AML. However, 3 of the 9 relapsed AML patients who were included in the trial harbored EM AML as per 18FDG-PET/CT. In spite of this, the National Comprehensive Cancer Network and others recommend 18FDG-PET/CT when EM AML is suspected in an AML patient, while the European LeukemiaNet provides no recommendations for doctors treating patients with EM AML.2,6,21,22
In summary, our study demonstrates a higher prevalence of EM AML than previously reported and assumed, while the clinical prevalence was in the range of previously published reports. We were able to demonstrate that18FDG-PET/CT is feasible and safe in patients with AML at diagnosis. Furthermore, we were able to confirm that, in most patients, more than one metabolically active EM AML manifestation could be detected with 18FDG-PET/CT. Interestingly, six patients who were PET-positive at baseline and who had histologically confirmed EM AML were in hematologic CR but still had detectable 18FDG-avid EM AML depicting heterogeneity after treatment (Online Supplementary Figure S1A). When analyzing those four patients who presented with EM AML at diagnosis (as per initial 18FDG-PET/CT) and frank bone marrow AML, all four were still positive for EM AML as per 18FDG-PET/CT but in a CR as per bone marrow aspirate; furthermore, three of these four patients eventually relapsed, despite consolidation therapy. The dynamics of PET-positivity with regard to concurrent bone marrow involvement, therefore, seem to be heterogeneous and the prognostic relevance of this has to be studied in further prospective trials. Hence, this study allows further trials to be designed and calculated for a prospective evaluation of the impact of EM AML using 18FDG-PET/CT.
Supplementary Material
Acknowledgments
We would like to thank Katrin Rosenow and Gabriele Kotzerke for co-ordinating the 18FDG-PET/CT procedures. We would like to thank Annett Engmann, Katrin Peschel, and Catrin Theuser for data management. We would like to thank the patients, nurses, and doctors who contributed to this study.
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/105/6/1552
Funding
This study was supported by the German Cancer Aid Foundation (109575 to FS, KZ, and MS). Open Access funding by the Publication Funds of the TU Dresden.
References
- 1.Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood. 2009; 114(5):937–951. [DOI] [PubMed] [Google Scholar]
- 2.Bakst RL, Tallman MS, Douer D, Yahalom J. How I treat extramedullary acute myeloid leukemia. Blood. 2011; 118(14):3785–3793. [DOI] [PubMed] [Google Scholar]
- 3.Avni B, Rund D, Levin M, et al. Clinical implications of acute myeloid leukemia presenting as myeloid sarcoma. Hematol Oncol. 2012; 30(1):34–40. [DOI] [PubMed] [Google Scholar]
- 4.Cornelissen JJ, Gratwohl A, Schlenk RF, et al. The European LeukemiaNet AML Working Party consensus statement on allogeneic HSCT for patients with AML in remission: an integrated-risk adapted approach. Nat Rev Clin Oncol. 2012; 9(10):579–590. [DOI] [PubMed] [Google Scholar]
- 5.Ganzel C, Manola J, Douer D, et al. Extramedullary Disease in Adult Acute Myeloid Leukemia Is Common but Lacks Independent Significance: Analysis of Patients in ECOG-ACRIN Cancer Research Group Trials, 1980-2008. J Clin Oncol. 2016; 34(29):3544–3553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dohner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017; 129(4):424–447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Karlin L, Itti E, Pautas C, et al. PET-imaging as a useful tool for early detection of the relapse site in the management of primary myeloid sarcoma. Haematologica. 2006; 91(12 Suppl):ECR54. [PubMed] [Google Scholar]
- 8.Stolzel F, Rollig C, Radke J, et al. (1)(8)F-FDG-PET/CT for detection of extramedullary acute myeloid leukemia. Haematologica. 2011; 96(10):1552–1556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Aschoff P, Hantschel M, Oksuz M, et al. Integrated FDG-PET/CT for detection, therapy monitoring and follow-up of granulocytic sarcoma. Initial results. Nuklearmedizin. 2009; 48(5):185–191. [DOI] [PubMed] [Google Scholar]
- 10.Kuenzle K, Taverna C, Steinert HC. Detection of extramedullary infiltrates in acute myelogenous leukemia with whole-body positron emission tomography and 2-deoxy-2-[18F]-fluoro-D-glucose. Mol Imaging Biol. 2002; 4(2):179–183. [DOI] [PubMed] [Google Scholar]
- 11.Makis W, Hickeson M, Derbekyan V. Myeloid sarcoma presenting as an anterior mediastinal mass invading the pericardium: Serial Imaging With F-18 FDG PET/CT. Clin Nucl Med. 2010; 35(9):706–709. [DOI] [PubMed] [Google Scholar]
- 12.Mantzarides M, Bonardel G, Fagot T, et al. Granulocytic sarcomas evaluated with F-18-fluorodeoxyglucose PET. Clin Nucl Med. 2008; 33(2):115–117. [DOI] [PubMed] [Google Scholar]
- 13.Ueda K, Ichikawa M, Takahashi M, Momose T, Ohtomo K, Kurokawa M. FDG-PET is effective in the detection of granulocytic sarcoma in patients with myeloid malignancy. Leukemia Res. 2010; 34(9):1239–1241. [DOI] [PubMed] [Google Scholar]
- 14.Buck AK, Bommer M, Juweid ME, et al. First demonstration of leukemia imaging with the proliferation marker 18F-fluo-rodeoxythymidine. J Nucl Med. 2008; 49(11):1756–1762. [DOI] [PubMed] [Google Scholar]
- 15.Sekeres MA, Elson P, Kalaycio ME, et al. Time from diagnosis to treatment initiation predicts survival in younger, but not older, acute myeloid leukemia patients. Blood. 2009; 113(1):28–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cheson BD, Bennett JM, Kopecky KJ, et al. Revised recommendations of the International Working Group for Diagnosis, Standardization of Response Criteria, Treatment Outcomes, and Reporting Standards for Therapeutic Trials in Acute Myeloid Leukemia. J Clin Oncol. 2003; 21(24):4642–4649. [DOI] [PubMed] [Google Scholar]
- 17.Cribe AS, Steenhof M, Marcher CW, Petersen H, Frederiksen H, Friis LS. Extramedullary disease in patients with acute myeloid leukemia assessed by 18F-FDG PET. Eur J Haematol. 2013; 90(4):273–278. [DOI] [PubMed] [Google Scholar]
- 18.Liu PI, Ishimaru T, McGregor DH, Okada H, Steer A. Autopsy study of granulocytic sarcoma (chloroma) in patients with myelogenous leukemia, Hiroshima-Nagasaki 1949-1969. Cancer. 1973; 31(4):948–955. [DOI] [PubMed] [Google Scholar]
- 19.Zhou WL, Wu HB, Wang LJ, Tian Y, Dong Y, Wang QS. Usefulness and pitfalls of F-18-FDG PET/CT for diagnosing extramedullary acute leukemia. Eur J Radiol. 2016; 85(1):205–210. [DOI] [PubMed] [Google Scholar]
- 20.Pileri SA, Ascani S, Cox MC, et al. Myeloid sarcoma: clinico-pathologic, phenotypic and cytogenetic analysis of 92 adult patients. Leukemia. 2007; 21(2):340–350. [DOI] [PubMed] [Google Scholar]
- 21.O’Donnell MR, Tallman MS, Abboud CN, et al. Acute Myeloid Leukemia, Version 3.2017, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Cancer Netw. 2017; 15(7):926–957. [DOI] [PubMed] [Google Scholar]
- 22.Cunningham I, Kohno B. 18 FDG-PET/CT: 21st century approach to leukemic tumors in 124 cases. Am J Hematol. 2016; 91(4):379–384. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.