

Dear Editor,
We have read with great interest the articles regarding cutaneous manifestations in coronavirus disease 2019 (COVID‐19) infection. Studies showed 20.4% of COVID‐19‐infected patients developed cutaneous manifestations and might be the only presenting symptom. 1 To date, previous cases reported urticaria as one of the cutaneous manifestations in COVID‐19. 1 , 2 , 3 , 4 This atypical symptom might lead to misdiagnosis, delayed diagnosis and virus transmission, especially in countries where cutaneous manifestation of COVID‐19 has not been reported widely such as in Indonesia. We would like to report a case of urticaria in COVID‐19‐positive non‐ICU hospitalized patient from Indonesia to bring awareness to its cutaneous manifestations.
A 51‐years‐old patient was admitted to our hospital on 12 April 2020 with presenting symptoms including fever, cough, dyspnoea and diarrhoea. His RT‐PCR for COVID was positive on 10 April 2020; therefore, he was diagnosed with COVID‐19. The patient has history of hypertension, diabetes, dyslipidemia and hyperuricemia on therapy. The vital signs were as follows: blood pressure 160/100 mmHg, pulse rate 106/min, respiratory rate 24/min, temperature 37.1°C and SpO2 97% on room air. The result of the examinations on admission is as follows: low haemoglobin (12.8 g/dL), red blood cell count (4.31 × 106/μL), pO2 (75 mmHg), HCO3 (19.8 mmol/L), total CO2 (20.8 mmol/L), base excess (−5 mmol/L) and high ESR (17 mm/h), LDH (300 U/L), CRP (6.9 mg/dL). Chest CT scan on April 12 showed fibrotic bands in both lungs with no ground‐glass opacity. Chest X‐ray on April 21 showed bilateral lung opacities predominantly in peripheral, lower zone (Fig. 1). The patient was treated with azithromycin, hydroxychloroquine, cefoperazone‐sulbactam, omeprazole and medicines for his comorbidities. On day 3 of hospitalization, suddenly, he developed pruritic urticaria involving the face (Fig. 2a,b) and without involvement of the rest of the skin. It appeared 5 days after the onset of symptoms. However, no urticaria triggers other than viral infection were found, as there was no history of food allergy, drug allergy, chronic urticaria, nor other allergies. There was no history of consuming new medicine in 15 days prior besides COVID‐19 treatment in hospital. Oral antihistamine loratadine was added to his treatment with improvement of symptom on the next day. The suspicion of urticaria caused by the medicines given in hospital could be eliminated by the fact his urticaria improved even the medicines continued to be given.
Figure 1.
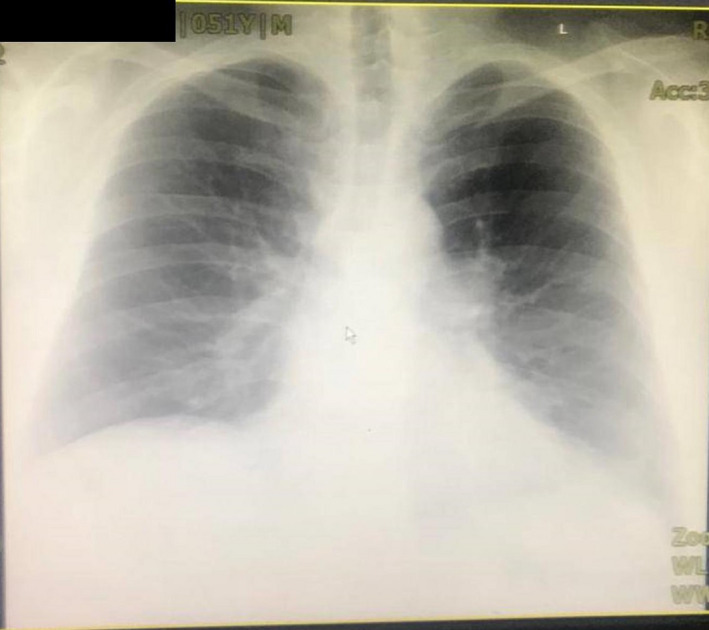
Chest X‐ray on April 21.
Figure 2.
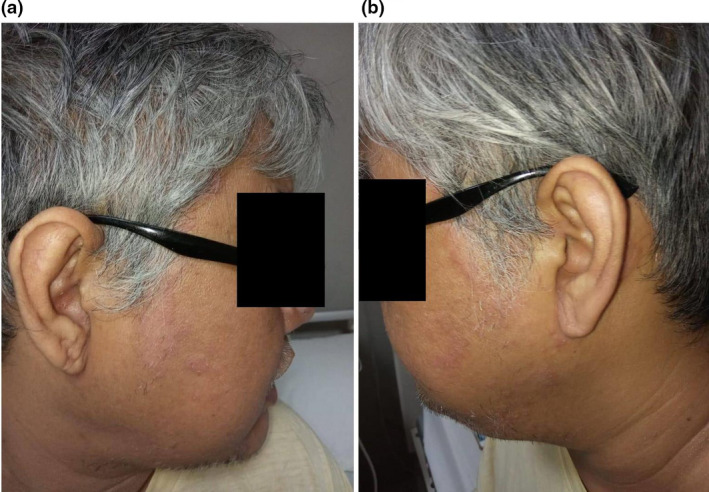
Urticaria involving face, on the right side (a) and left side of the face (b).
This report was consistent with previous studies, and treatment with oral antihistamines led to clinical improvement as well. A case in Spain reported urticaria in COVID‐19‐infected patient which biopsy revealed a perivascular infiltrate of lymphocytes, some eosinophils and upper dermal oedema. 4 However, biopsy was not done in this case because of the equipment limitation. The authors postulated the pathophysiology of urticaria in COVID‐19 might be described by three hypotheses. Firstly, it has widely known that viral infection causes nonimmunological urticaria by mast cell activation through complement activation. 5 Secondly, vasculitis might be the underlying cause as in pathophysiology in urticarial vasculitis. Angiotensin‐converting enzyme 2 (ACE2), the protein which SARS‐CoV‐2 uses to enter cells, was widely distributed in human’s body, particularly vascular endothelial. This might lead to formation of antibody‐antigen complex, which deposited at vascular wall, which is followed by complement activation and mast cell degranulation. 6 , 7 Thirdly, the urticaria might be associated with bradykinin in Kinin–kallikrein system in conjunction with ACE2. But more studies regarding BK‐mediated urticaria are needed. 8 , 9 , 10
Apparently, previous studies showed there was not any correlation of urticaria in COVID‐19 with disease’s severity, which is consistent with our case, because the patient was in stable condition and to date has fully recovered.
Acknowledgement
The patient in this manuscript has given written informed consent to the publication of their case details.
Funding source
none.
References
- 1. Recalcati S. Cutaneous manifestations in COVID‐19: a first perspective. J Eur Acad Dermatology Venereol 2020. 10.1111/jdv.16387. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 2. Wang D, Hu B, Hu C et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus‐infected pneumonia in Wuhan, China. JAMA 2020; 323: 1061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Henry D, Ackerman M, Sancelme E, Finon A, Esteve E. Urticarial eruption in COVID‐19 infection. J Eur Acad Dermatol Venereol 2020. 10.1111/jdv.16472 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Fernandez‐Nieto D, Ortega‐Quijano D, Segurado‐Miravalles G, Pindado‐Ortega C, Prieto‐Barrios M, Jimenez‐Cauhe J. Comment on: Cutaneous manifestations in COVID‐ 19: a first perspective. Safety concerns of clinical images and skin biopsies. J Eur Acad Dermatol Venereol 2020. 10.1016/j.sciaf.2019.e00146 [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Wedi B, Raap U, Wieczorek D, Kapp A. Urticaria and infections. Allergy Asthma Clin Immunol 2009; 5: 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Hamming I, Timens W, Bulthuis MLC, Lely AT, Navis GJ , van Goor H . Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol 2004; 203: 631–637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Mehregan DR. Pathophysiology of urticarial vasculitis. Arch Dermatol 1998; 134: 88–89. [DOI] [PubMed] [Google Scholar]
- 8. Tolouian R, Zununi Vahed S, Ghiyasvand S, Tolouian A, Ardalan M. COVID‐19 interactions with angiotensin‐converting enzyme 2 (ACE2) and the kinin system; looking at a potential treatment. J Ren Inj Prev J Ren Inj Prev [Internet] 2020; 9: 19. [Google Scholar]
- 9. Nishad AAN, Arulmoly K, Priyankara SAS, Abeysundara PK. A forgotten cause of allergy at ER that is still difficult to diagnose and treat at poor resource setting: angioedema after using angiotensin converting enzyme inhibitors for 4 years. Case Rep Immunol 2019; 2019: 1676391. 10.1155/2019/1676391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hofman ZLM, van den Elzen MT, Kuijpers J et al. Evidence for bradykinin release in chronic spontaneous urticaria. Clin Exp Allergy 2020; 50: 343–351. [DOI] [PubMed] [Google Scholar]