

Abstract
Aim of study includes review on supra-auricular approach and its clearance of the tract including its branches and also its efficacy in reduction of recurrence when compared to standard technique. Prospective study in which 10 patients attending ENT opd with clinically diagnosed preauricular sinus undergoing supra-auricular approach under GA/LA, willing to participate in study were selected. An elliptical incision of the standard technique extended higher upward to pre- and supra-auricular temporal region. Plane of temporalis fascia was delineated. Skin, anterior to the sinus and tragus was separated. Soft tissue between the plane of temporalis fascia (deep limit) and the skin anterior to the sinus excised along with the piece of adjoining helical cartilage. This excised tissue contains the entire tract with its possible branches giving no room for recurrence. Patients were followed up for 6 months. 10 patient’s data was updated and analyzed. No recurrence observed in all 10 patients. Supra auricular approach is useful and helpful technique for preauricular sinus tract excision with no recurrence rate. However further studies are required with large sample size.
Keywords: Preauricular sinus, Surgical management, Supra auricular approach, Recurrence rate
Introduction
Preauricular sinus seen in 0.3–0.9% of the population, also common congenital malformation and is usually unilateral and occasionally bilateral. Most patients with preauricular sinus are asymptomatic. Classically a preauricular sinus presents as a small opening usually near the anterior limb of the ascending helix although most preauricular sinuses are found anterior to external auditory canal. Other sites that can be involved are posterior surface of helical crus, cymba concha, ear lobule and postauricular area. First described by Heusinger in 1864. This congenital abnormality is autosomal dominant type and might be due to defect in development of the first branchial arch during 6th week of gestation leading to incomplete fusion of hillocks of His. The course of this sinus tract is often tortuous and not constant and its bounded superiorly and laterally by parotid and cutaneous branches of facial nerve and deep limit is formed by temporalis fascia. Most of the times these sinuses are silent but at time, these can get infected, most common pathogen being staphylococcus aureus and present with clinical features as recurrent discharge, pain, swelling, headache and fever.
Various surgical technique have been described in literature with varied recurrence rate. The highest recurrence rate has been reported as 42% and lowest being 0%. Supra auricular approach involves en block resection of the sinus tract including its branches, removing all the subcutaneous tissue and leaving no room for recurrence.
Materials and Methods
This is a prospective study conducted in Tertiary Health care from July 2017 to January 2018. After institutional ethical committee clearance 10 patients of either sex, between 3 and 40 years, attending ENT opd with clinically diagnosed preauricular sinus undergoing supra auricular approach, willing to participate in study were selected. Patients who had active discharge were first medically treated and then were considered for surgery.
Informed, written consent were obtained from all patients and a note was made on patient’s demographics. Younger patients up to age of 17 were operated under general anesthesia and rest were operated under local anesthesia. Figure 1 showing preoperative picture of right preauricular sinus.
Fig. 1.

Right preauricular sinus
Under strict aseptic precautions, an elliptical incision is made around the sinus and incision is extended superiorly to supra auricular region. The incision is deepened till temporalis fascia is identified as deep limit or medial limit of dissection. The subcutaneous tissue between skin anterior to sinus and temporalis fascia removed along with piece of adjoining helical cartilage (Fig. 2). The entire tract with its possible branches excised, ensuring no room for recurrence en block dissection (Fig. 3). Thorough wash given. Wound closed in layers and dressing was done. The excised tract was sent for histopathological examination. All patients were put on antibiotics and analgesics. Sutures were removed on day 8th post operatively and followed up after 1 month for any wound site infection and after 6 months for recurrence.
Fig. 2.
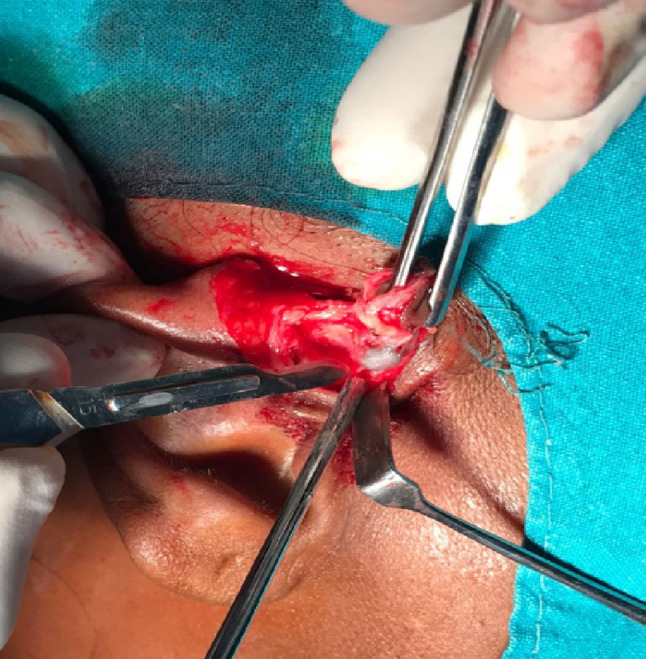
Tract removed along with subcutaneous tissue
Fig. 3.

Preauricular sinus with tract removed enblock
Results
10 patients were included who underwent supra auricular approach for preauricular sinus excision. Out of 10 patients 3 (30%) were males and 7 (70%) were females (Table 1).
Table 1.
Sex distribution (N = 10)
| Sex | Number | Percent |
|---|---|---|
| Males | 3 | 30 |
| Females | 7 | 70 |
| Total | 10 | 100 |
Among these patients, maximum affected were found to be in age group of 10–29 years. (Table 2). While comparing the laterality of disease both sides were equally affected in our case series (Table 3).
Table 2.
Age distribution (N = 10)
| Age (in years) | Frequency | Percent |
|---|---|---|
| 3–10 | 2 | 20.0 |
| 10–29 | 6 | 60.0 |
| 30–40 | 2 | 20.0 |
| Total | 10 | 100.0 |
Table 3.
Laterality of disease
| Side | Number | Percent |
|---|---|---|
| Right | 5 | 50 |
| Left | 5 | 50 |
3 cases had presented with first attack of acute infection and the rest 7 cases had previous history of recurrent ear discharge, pain.
The data analysis was done and average duration of surgery was calculated and found to be 26 min, hence proving shorter duration of surgery and better outcome with minimal recurrence.
In this case series, it has been observed that all 10 patients were followed up for 6 months and no recurrence was noted. The success rate was found to be 100%.
Discussion
Preauricular sinus is one of the most common congenital malformation seen in general population. Most of the cases are unilateral (80%), few found to be bilateral and vary from simple pit to complex branching sinus [1]. Most accepted theory for preauricular sinus is due to incomplete fusion of hillocks of His.
The recurrence of the pre auricular sinus is due to incomplete excision of sinus tract and presence of residual viable squamous epithelium, that usually occurs with conventional method. In supra auricular approach we identify the temporalis fascia as medial limit, cartilage of helix and auditory canal as lateral limit. En bloc removal of sinus with removal of subcutaneous tissue is done giving no room for recurrence.
Study on radical supra auricular approach with local excision conducted by Prasad et al. also gave similar results.
Study conducted by H Vijayendra in 2005 in 36 cases had no recurrence rate.
When compared with study conducted by Lam et al. where it was found that recurrence rate with classic sinusectomy technique was more than supra auricular approach (32% and 3.7%).
In our study females were more affected than males 70% and 30% respectively.
The advantages of this method is, it was simple, less time consuming, showed fewer difficulties and low scar formation when compared to standard conventional method.
Disadvantages of the study is rarely it can carry the risk of injury to superficial temporal artery causing bleeding, however it was not seen in our case series.
Conclusion
Supra auricular approach is a simple and effective technique and better than standard technique, giving negligible recurrence rate and accepted technique nowadays. No significant complications was noted and better cosmetically as it has low scar formation. It is better in recurrent cases and preauricular sinus associated with abscess. However further studies are required with larger sample size.
Acknowledgements
None.
Funding
None.
Compliance with Ethical Standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
Institutional ethical committee clearance obtained.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Reference
- 1.Vijayendra H, Sangeetha R, Chetty KR. A safe and reliable technique in the management of preauricular sinus. Indian J Otolaryngol Head Neck Surg. 2005;57(4):294–295. doi: 10.1007/BF02907690. [DOI] [PMC free article] [PubMed] [Google Scholar]