

Abstract
Introduction
Osteochondromas are the most common benign bone tumors (accounting for 20–50% of all benign bone tumors). They are developmental malformations rather than true neoplasms and are thought to originate within the periosteum. They usually affect bones that develop by enchondral ossification and rarely originate from bones that develop by intramembranous ossification such as the scapula, pubic rami, clavicle, and ribs.
Case Report
We present a case of a 24-year-old male, who came with a swelling in the right side inguinal region for 2 years which was diagnosed to be osteochondroma by trocar biopsy. The site and presentation are rare. The patient had no visceral or vascular involvement though the lesion was very near many vital structures on superior pubic ramus.
Conclusion
Osteochondroma arising from the pelvis is an unusual presentation which should be kept in mind as a differential diagnosis when evaluating mass in pelvis.
Keywords: Osteochondroma, exostosis, pubic ramus
Learning Point of the Article:
Pelvic osteochondroma is indeed a rare presentation and should be kept in mind while evaluating a pelvic mass.
Introduction
Osteochondromas are the most common benign bone tumors (accounting for 20–50% of all benign bone tumors). They are developmental malformations rather than true neoplasms and are thought to originate within the periosteum [1, 2]. Inheritance pattern is autosomal dominant which can cause multiple exostoses or isolated lesion [3]. They usually present during the period of rapid skeletal growth and cease to grow once maturity is reached [1, 3]. The patient usually complaints of swelling and cosmetic deformity [4]. They can present either as a pedunculated or a sessile mass (latter being more common)[1]. The lesion is typically mushroom-shaped affecting metaphysis of long bones such as femur and tibia [5]. It usually affects bones that develop by enchondral ossification and rarely originates from bones that develop by intramembranous ossification such as the scapula, pubic ramus, clavicle, and ribs [6]. We report a rare case of pedunculated variety of osteochondroma developing at an unusual site –superior pubic ramus.
Case Report
A 24-year-old healthy male student presented with complaints of a swelling in the right side inguinal region for 2 years. The swelling was insidious in onset, gradually progressive and was not associated with pain, but the patient complained of irritation and mass effect due to the swelling specially when wearing belt or tight clothing. On examination, there was a hard swelling of approximately 8 cm × 11cm size over the right inguinal region, medial to the mid-inguinal point. The swelling was non-tender, non-mobile, and fixed to underlying bone but not adherent to skin or overlying tissue. Cough impulse was absent.
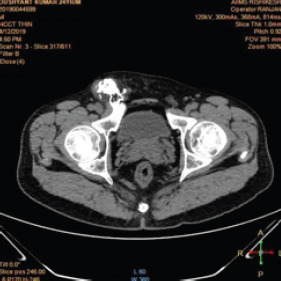
X-ray pelvis with both hips anteroposterior view and oblique views (Fig. 1) showed exostosis arising from superior pubic rami. Non-contrast helical computerized tomography (CT)pelvis with both hips (Fig. 2) showed a pedunculated round to oval lesion in continuity with cortex of superior pubic rami on the right side arising from outside surface. It had a cartilaginous cap. It measured 8 cm × 4.6 cm × 5cm in size. CT scan of pelvis confirmed the bony nature of swelling.
Figure 1.

Radiograph at presentation.
Figure 2.

Radiograph at presentation.
Trocar biopsy was taken first under C-arm guidance. Histopathological examination (Fig. 3) showed bony trabeculae along with cartilage with no evidence of dysplasia. Excisional biopsy of the tumor from the right superior pubic rami was performed using ilioinguinal approach. Intraoperatively, we noticed that tumor was in the plane between superficial abdominal wall and pubic ramus, and no need to open inguinal canal was felt. It was carefully operated using blunt and sharp dissection and excised from stalk. There was no infiltration into surrounding structure and tumor came out in toto. Macroscopically, it measured 90 cm × 60 cm × 20cm (Fig. 4). Outer surface had bosselated grayish-white appearance. The tumor involved midpart of superior pubic ramus with cap of mature cartilage covering the bone.
Figure 3.

Radiograph post-operative.
Figure 4.
Non-contrast helical computerized tomography scan.
Figure 5.

Gross specimen.
Figure 6.
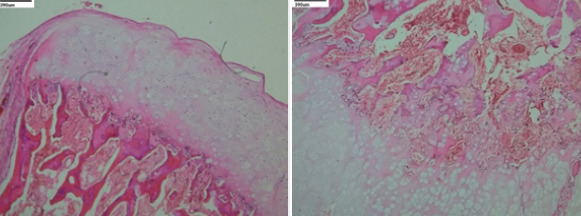
(a and b) Histopathological specimen showing bony trabeculae with bone intertrabecular tissue. The bone is covered by a cap of mature cartilage.
Discussion
The overall incidence of osteochondroma reported in literature is 35% of benign and 8% of all bone tumors [7]. Osteochondromas usually develop in bones that develop by enchondral ossification and rarely develop in bones developing by intramembranous ossification like pelvis [6]. Among the long bones, the most common site affected is distal femur [1]. Male predominance is seen with the ratio of 1.6–3.4:1 [8].Osteochondromas are usually seen in growing age group as they develop as cartilaginous overgrowth from physeal plate [1]. They have been reported to develop due to hematopoietic stem cell transplantation and due to surgery/radiation-induced injury [8]. Genetic etiology of the disease is well established with tumor suppressor gene EXT1 and EXT2 being the culprit for the disease [4, 9].
A thorough search of literature was made to find out the rarity of the case. PubMed and Google Scholar database were used to find out articles reporting osteochondroma arising from pubic rami. According to Rizzoli institution statistical data, only seven cases of osteochondroma arising from pubic rami were reported worldwide until 2009 [6]. Recently, Nekkanti et al. reported a case of sessile osteochondroma arising from iliac wing [4]. A cadaveric case report of osteochondroma arising from pubis was given by Nayak et al., in 2018 [10].
Osteochondromas cause symptoms only when they become large enough to cause a mass effect and compression of nearby structures. Review of recent literature shows that compression of lumbosacral nerve roots is common with pelvic osteochondromas [4,11,12]. Location of the tumor can be judged according to the symptoms of nerve compression. An iliac mass would cause lumbar nerve root compression, whereas an ischial mass would put pressure on sciatic nerves [4, 11, 12]. Urogenital structures can also be compressed by a large osteochondroma. The patient can have symptoms of bladder outlet obstruction due to compression of bladder neck and urethra [4, 9, 11, 13].
Osteochondroma is a benign neoplasm but has the potential of malignant transformation. About 1% incidence of chondrosarcoma developing from osteochondroma has been reported in literature [1, 4, 8, 11]. One case of chondrosarcoma development form pelvic osteochondroma has been published in the past [14]. Development of chondrosarcoma or neurovascular compromise is an absolute indication for tumor excision [1,4]. Our patient had no symptoms of any organ compression and complained only of a swelling in the right side pubic region causing irritation and pain on walking and squatting. We noticed that the tumor mass was present on ventral surface of the right superior pubic ramus. It was away from the hip joint, femoral neurovascular bundle and pubic viscera. The tumor was, therefore, excised enbloc. Ilioinguinal approach was used for the excision.
Conclusion
We report this case due to its unusual site of presentation. These tumors are usually asymptomatic but can cause pubic viscera compression or neurovascular compromise. These are usually operated due to cosmetic reasons with a very low incidence of recurrence. Pelvic osteochondromas should be kept in mind as differential of a bony hard pelvic mass.
Clinical Message.
Certain tumors present unusually at rare sites which make the diagnosis challenging for the surgeon. Although rare, osteochondroma can present in bones developing by intramembranous ossification. Detailed evaluation becomes necessary.
Biography


Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that Informed consent of the patient is taken for publication of this case report
References
- 1.Heck KR., Jr . Benign bone tumors and neoplastic conditions simulating bone tumors. In: Canale ST, Beaty JH, editors. Campbell's Operative Orthopaedics. 11th ed. Philadelphia, PA: Mobsy Elsevier; 2007. pp. 858–61. [Google Scholar]
- 2.Oljaca A, Hirzberger D, Bergovec M, Tiesenhausen K, Koter SH, Friesenbichler J, et al. Osteochondroma of the scapula associated with a subclavian artery pseudoaneurysm:Case report. SAGE Open Med Case Rep. 2019;7:2050313X18823089. doi: 10.1177/2050313X18823089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Taheriazam A, Saeidinia A. One-stage surgical excision of a huge bilateral multiple osteochondroma of the hip:A case report. Electron Physician. 2017;9:5310–7. doi: 10.19082/5310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nekkanti S, Savsani S, Reddy YC, Meka A, Mahtani A. A rare sessile variant of osteochondroma presenting at an unusual site of the iliac wing in a 15-year old boy. J Orthop Allied Sci. 2018;6:93–5. [Google Scholar]
- 5.Mohan M, Buch SA, Babu GS, Castelino RL, Rao S, Rao K. A rare clinical presentation of an osteochondroma of coronoid process of mandible. J Dent Shiraz Univ Med Sci. 2018;19:325–30. [PMC free article] [PubMed] [Google Scholar]
- 6.Gökkuş K, Atmaca H, Sağtaş E, Saylik M, Aydin AT. Osteochondromas originating from unusual locations complicating orthopedic discipline:Case series. EklemHastalikCerrahisi. 2015;26:100–9. doi: 10.5606/ehc.2015.21. [DOI] [PubMed] [Google Scholar]
- 7.Bovee JV, Wilpshaar TA. Bone:Osteochondroma. Atlas Genet Cytogenet Oncol Haematol. 2019;23:133–6. [Google Scholar]
- 8.Sharma S, Kalsotra SN, Gupta P, Wani I, Singh M, Singh D. Solitary osteochondroma of the ilium:A case report. Int J Orthop Surg. 2009;16:1 4. [Google Scholar]
- 9.Herode P, Shroff A, Patel P, Aggarwal P, Mandlewala V. A rare case of pubic ramus osteochondroma. J Orthop Case Rep. 2015;5:51–3. doi: 10.13107/jocr.2250-0685.307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nayak SB, Kumar N, Sirasanagandla SR, Srinivas SP, Pamidi N, Shetty SD, et al. Solitary osteochondroma in the body of the pubic bone:A cadaveric case report. Anat Cell Biol. 2018;51:136–8. doi: 10.5115/acb.2018.51.2.136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ali N, Bhat A, Bangroo FA, Dhanda MS, Maqsood M, Sharma SC, et al. Isolated osteochondroma of the ilium:Case report with review of the literature.Scholars J Appl Med Sci. 2014;2:1573–6. [Google Scholar]
- 12.Kim WJ, Kim KJ, Lee SK, Choy WS. Solitary pelvic osteochondroma causing L5 nerve root compression. Orthopedics. 2009;32:922. doi: 10.3928/01477447-20091020-25. [DOI] [PubMed] [Google Scholar]
- 13.Wang WY, Du LD, Lv WC, Tian Y, Shao Q, Zhang YH, et al. Osteochondroma of the symphysis pubis:A rare cause of bladder outlet obstruction. Am Surg. 2010;76:916–8. [PubMed] [Google Scholar]
- 14.Nystrom LM, DeYoung BR, Morcuende JA. Secondary chondrosarcoma of the pelvis arising from a solitary exostosis in an 11-year-old patient:A case report with 5-year follow-up. Iowa Orthop J. 2013;33:213–6. [PMC free article] [PubMed] [Google Scholar]