

Abstract
Background
Several countries have imposed a mandatory 14‐day period of quarantine on individuals arriving from countries considered high‐risk for severe acute respiratory syndrome coronavirus‐2 (SARS‐CoV‐2) infection. However, it is not clear how long asymptomatic patients infected with SARS‐CoV‐2 can be an asymptomatic carrier.
Case Presentation
We experienced a case of an asymptomatic female patient infected with SARS‐CoV‐2 with abnormal chest computed tomography findings. She did not develop a fever during hospitalized isolation. She remained reverse transcription–polymerase chain reaction‐positive for 24 days.
Conclusion
An asymptomatic patient diagnosed with SARS‐CoV‐2 infection remained reverse transcription–polymerase chain reaction‐positive for 24 days, although she was quarantined in an isolation hospital. This finding suggests that an asymptomatic patient diagnosed with SARS‐CoV‐2 infection with abnormal chest computed tomography findings can be an asymptomatic carrier for more than 3 weeks.
Keywords: Coronavirus infection, COVID‐19, pandemic, pneumonia, reverse transcription–polymerase chain reaction, viral
Is it enough for potential severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) carriers to be required to self‐quarantine for 14 days to prevent the spread of coronavirus disease 2019 (COVID‐19)? In this case report, an asymptomatic female patient infected with SARS‐CoV‐2 who remained reverse transcription–polymerase chain reaction‐positive for 24 days although she was quarantined in an isolation hospital. Asymptomatic patients diagnosed with SARS‐CoV‐2 infection can be an asymptomatic carrier for more than 3 weeks.
![]()
Introduction
On 30 January 2020, the Cabinet of Japan classified coronavirus disease 2019 (COVID‐19) caused by severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) as a “designated infectious disease” that legally allows compulsory hospitalization. Additionally, on 14 February 2020, the Cabinet Orders (Cabinet Order Nos. 28 and 29 of 2020) allowed that the government could isolate an asymptomatic carrier with a positive SARS‐CoV‐2 test result by hospitalizing him/her in an entrusted medical institution designated for infectious diseases.
We report the case of an asymptomatic patient infected with SARS‐CoV‐2 with abnormal chest computed tomography (CT) findings who remained reverse transcription–polymerase chain reaction (RT‐PCR)‐positive for 24 days. She was quarantined in an isolation hospital.
Case Report
On 15 February 2020, a 64‐year‐old asymptomatic woman on board a cruise ship was tested for SARS‐CoV‐2 using RT‐PCR undertaken with a throat swab sample. Her husband was diagnosed with laboratory‐confirmed COVID‐19 and transferred to an isolation ward at a health‐care facility. Although she remained asymptomatic without fever on 20 February 2020, she was diagnosed with SARS‐CoV‐2 infection and was transferred to our hospital for quarantine.
The patient had been in her usual health without fever after her husband developed fever approximately 10 days before her current admission. Her medical history included hypertension. Her regular medications were amlodipine, candesartan, hydrochlorothiazide, and atenolol. On initial examination, her blood pressure, pulse rate, and body temperature were 108/57 mmHg, 57 b.p.m., and 36.6°C, respectively. While she was breathing ambient air, her respiratory rate and oxygen saturation were 18 breaths/min and 98%, respectively. Physical examination revealed the absence of cough and vesicular sound without crackles. Based on the patient’s laboratory test results, her white blood cell count and C‐reactive protein level were 7,300 cells/μL and 0.41 mg/dL, respectively (Table 1). Chest X‐ray showed no abnormal findings. Chest CT revealed patchy ground‐glass opacities in the peripheral areas under the pleura on the right lower lobe (Fig. 1).
Table 1.
Laboratory findings on admission of an asymptomatic 64‐year‐old woman infected with severe acute respiratory syndrome coronavirus‐2
| Hematology | Serum biochemistry | |||||||
| WBC | 7,300 | cells/μL | Na | 136 | mEq/dL | ALB | 4.7 | g/dL |
| Neut | 64.0 | % | K | 4.0 | mEq/dL | BUN | 10.9 | mg/dL |
| Lymph | 25.5 | % | Cl | 101 | mEq/dL | CRE | 0.56 | mg/dL |
| Mono | 10.0 | % | AST | 36 | U/L | CRP | 0.41 | mg/dL |
| Baso | 0.5 | % | ALT | 49 | U/L | Procalcitonin | 0.08 | ng/dL |
| Eos | 0 | % | LDH | 186 | U/L | Hemostasis | ||
| RBC | 486 × 104 | /μL | ALP | 420 | U/L | PT | 98 | % |
| Hb | 15.5 | g/dL | T‐Bil | 1.72 | mg/dL | PT‐INR | 1.01 | |
| Plt | 19.0 × 104 | /μL | CK | 47 | U/L | APTT | 34.3 | s |
ALB, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; Baso, basophil; BUN, blood urea nitrogen; CK, creatine kinase; CRE, creatinine; CRP, C‐reactive protein; Eos, eosinophil; Hb, hemoglobin; LDH, lactate dehydrogenase; Lymph, lymphocyte; Mono, monocyte; Neut, neutrophil; Plt, platelet; PT, prothrombin time; PT‐INR, prothrombin time – international normalized ratio; RBC, red blood cell; T‐Bil, total bilirubin; WBC, white blood cell.
Fig. 1.
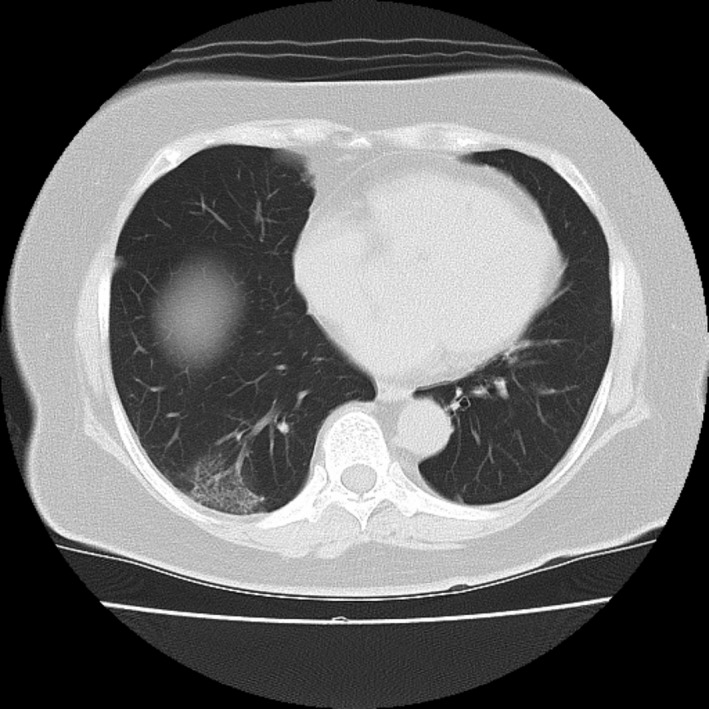
Chest computed tomography on admission of an asymptomatic 64‐year‐old woman infected with severe acute respiratory syndrome coronavirus‐2. Ground‐glass opacities were observed in the peripheral areas under the pleura on the right lower lobe (posterior basal).
The patient was quarantined in a single room with a bathroom. She was not allowed to move outside the room. She did not develop fever during her hospitalized isolation (Fig. 2). Follow‐up with chest X‐ray and chest CT was not carried out. Ten days after the first day of acquiring a positive RT‐PCR test result, RT‐PCR was undertaken on nasal swabs every few days following the instructions of the quarantine station.
Fig. 2.
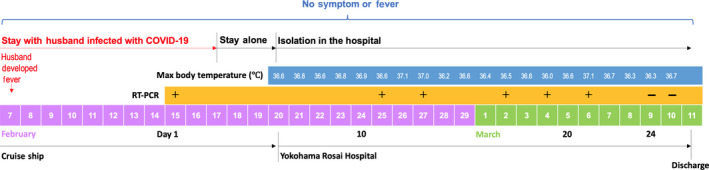
Symptoms and maximum body temperatures of a 64‐year‐old woman infected with severe acute respiratory syndrome coronavirus‐2, from the day her husband developed fever to the day of hospital discharge, 7 February to 11 March 2020. The patient did not develop fever and was asymptomatic during quarantine on a cruise ship and at Yokohama Rosai Hospital. RT‐PCR, reverse transcription–polymerase chain reaction.
The first day of continuous negative RT‐PCT test results was 9 March 2020. All the following criteria had to be met so that an asymptomatic patient infected with SARS‐CoV‐2 can be discharged from a hospital: (i) hospital isolation longer than 12.5 days, (ii) normal temperature lasting longer than 3 days, (iii) absence of respiratory symptoms, (iv) two consecutively negative RT‐PCR test results separated by at least 12 h. As the patient met the criteria for the discontinuation of quarantine in Japan on 10 March, she was discharged from our hospital on 11 March.
Discussion
The major finding of the present case indicated that an asymptomatic patient diagnosed with SARS‐CoV‐2 infection remained RT‐PCR‐positive for 24 days, and the potential communicable period was 24 days, although she was quarantined in an isolation hospital. This finding suggests that an asymptomatic patient diagnosed with SARS‐CoV‐2 infection can be an asymptomatic carrier for more than 3 weeks.
A previous study has shown that SARS‐CoV‐2 infection appears to have been transmitted during the incubation period of a patient who was diagnosed with COVID‐19. 1 However, it is still unclear whether asymptomatic individuals are potential sources of SARS‐CoV‐2 infection causing the current outbreak. Leekha et al. revealed that a patient with non‐enveloped virus infection who remained PCR‐positive was shedding virus as a carrier. 2 This case possibly suggests that asymptomatic patients diagnosed with SARS‐CoV‐2 infection continuously transmit SARS‐CoV‐2 for more than 3 weeks.
A previous study has indicated that recovered COVID‐19 patients had positive RT‐PCR test results 5–13 days after the discontinuation of quarantine, although they met the criteria for hospital discharge, including the absence of clinical symptoms and radiological abnormalities with two negative RT‐PCR test results. 3 The following are the two possible reasons why recovered COVID‐19 patients still have positive RT‐PCR test results: the patient infects with another type of SARS‐CoV‐2 4 as the result of inadequate isolation at home, or false‐negative RT‐PCR test results are obtained regardless if continuous SARS‐CoV‐2 infection 5 is observed. As we strictly isolate our patients infected with SARS‐CoV‐2 with or without symptoms under the Quarantine Act and Cabinet Order of Japan in our hospital, the present case indicated that an asymptomatic patient diagnosed with SARS‐CoV‐2 infection could remain RT‐PCR‐positive for more than 3 weeks.
Hu et al. 6 reported that 20.8% and 50.0% of cases of asymptomatic patients infected with SARS‐CoV‐2 developed symptoms during hospitalization and showed typical CT images with ground‐glass opacities in the lung, respectively. In our case report, the patient did not develop fever, cough, or fatigue, and there were no abnormalities on chest X‐ray, but she had patchy ground‐glass opacities in the peripheral areas under the pleura on the right lower lobe. We defined the communicable period as the interval from the first day of a positive RT‐PCR test result to the first day of continuous negative test results. 6 The same study also revealed that the communicable period of SARS‐CoV‐2 infection ranged from 1 to 21 days (median, 9.5 days; interquartile range, 3.5–13.0 days) in the whole cases, and the communicable period was 4.0 days (interquartile range, 2.0–15.0) in patients who are asymptomatic with normal chest CT findings. 6 However, to the best of our knowledge, the communicable period in asymptomatic patients with abnormal chest CT findings was not mentioned in any studies. In our case report, the patient was asymptomatic with abnormal chest CT findings, and the communicable period was 24 days. This result suggests that abnormal chest CT findings would prolong the potential communicable period in asymptomatic patients infected with SARS‐CoV‐2.
Although several countries imposed a mandatory 14‐day period of quarantine on individuals arriving from countries considered high‐risk for SARS‐CoV‐2 infection, our findings suggest that prolonged period of quarantine might prevent the outbreak of COVID‐19. However, a previous study has revealed the negative association between COVID‐19 mortality and health‐care resource availability. 7 In general, asymptomatic patients infected with SARS‐CoV‐2 are identified only from systematic screening, which includes the assessment of their close contacts with COVID‐19 patients or COVID‐19‐suspected patients. By undertaking chest CT, the clinician could identify asymptomatic patients with abnormal chest CT findings as high risk for a prolonged potential communicable period.
Conclusion
The present finding shows that an asymptomatic patient infected with SARS‐CoV‐2 with abnormal chest CT findings remained RT‐PCR‐positive for 24 days, and the communicable period might be longer than 3 weeks. Disregarding health‐care resource availability, we could carry out a chest CT scan in order to identify the patient as high risk with a prolonged potential communicable period among asymptomatic patients. This finding suggests that a prolonged communicable period, even greater than expected in asymptomatic patients infected with SARS‐CoV‐2 with abnormal chest CT findings, might cause asymptomatic carrier transmission, suggesting that prolonged period of quarantine of at least 4 weeks might prevent the outbreak of COVID‐19.
Disclosure
Approval of the research protocol: N/A
Informed consent: Written informed consent was obtained.
Registry and the registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of Interest: None.
Acknowledgement
We would like to thank Editage for voluntary English language editing.
Funding information
No funding information provided.
References
- 1. Rothe C, Schunk M, Sothmann P et al Transmission of 2019‐nCoV infection from an asymptomatic contact in Germany. N. Engl. J. Med. 2020; 382: 970–1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Leekha S, Zitterkopf NL, Espy MJ, Smith TF, Thompson RL, Sampathkumar P. Duration of influenza A virus shedding in hospitalized patients and implications for infection control. Infect. Control Hosp. Epidemiol. 2007; 28: 1071–6. [DOI] [PubMed] [Google Scholar]
- 3. Lan L, Xu D, Ye G et al Positive RT‐PCR test results in patients recovered from COVID‐19. JAMA 2020; 323: 1502–3. 10.1001/jama.2020.2783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Tang X, Wu C, Li X et al On the origin and continuing evolution of SARS‐CoV‐2. Natl Sci. Rev. 2020. [Epub ahead of print]. 10.1093/nsr/nwaa036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Xie X, Zhong Z, Zhao W, Zheng C, Wang F, Liu J. Chest CT for typical 2019‐nCoV pneumonia: relationship to negative RT‐PCR testing. Radiology 2020; 200343 [Epub ahead of print]. 10.1148/radiol.2020200343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Hu Z, Song C, Xu C et al Clinical characteristics of 24 asymptomatic infections with COVID‐19 screened among close contacts in Nanjing, China. Sci. China Life Sci. 2020;63:706–11. 10.1007/s11427-020-1661-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ji Y, Ma Z, Peppelenbosch MP, Pan Q. Potential association between COVID‐19 mortality and health‐care resource availability. Lancet Glob. Health 2020; 8: e480. [DOI] [PMC free article] [PubMed] [Google Scholar]