

1. INTRODUCTION
Transfusion safety is ever challenging as new diseases or risks appear from time to time. Despite the availability of modern sophisticated laboratory testing to better detect those important viral infections, there is still the inevitable limitation due to the possibility of a donor transmitting infection through blood in the window period of infection, when the blood contains infectious pathogens, but the biomarkers of infection are undetectable. Therefore, health history enquiry remains an important part of donor screening to exclude those donors who may be at risk to themselves or pose a risk to the blood supply. The health history enquiry covers a broad range of questions from personal health enquiry and travel history to evaluation of the risk of exposure to transmissible infections as a result of the donor's lifestyle. It becomes particularly important when a new disease appears with uncertain impact on blood safety and very limited knowledge of its biology.
In March 2003, Hong Kong faced an outbreak of atypical pneumonia of unknown aetiology. 1 , 2 Through many efforts, a new coronavirus was subsequently identified to be the causative agent. 3 , 4 , 5 As the infection was highly contagious through droplet transmission, the outbreak had a significant impact to society. The number of new cases increased exponentially between March and April 2003 before the infection was brought under control. Many health‐care workers were infected, causing much pressure in the provision of health‐care services. As a result, there was a significant change in the health‐care service and the demand for blood. In response to this, the blood transfusion service (BTS) introduced a number of changes during the SARS outbreak. Here, we review the changes implemented for the protection of donor and staff safety and for maintaining an adequate and safe blood supply. The review covers the time from the outbreak of the epidemic, when the World Health Organization (WHO) gave precautionary advice not to travel to Hong Kong, until the time when the epidemic was controlled, and Hong Kong was not an infected area anymore.
1.1. Donor and staff safety
As SARS is a highly contagious infection and is transmitted through droplets, stringent infection control measures were required to protect both donors and staff from contacting the virus. From the donor side, educational materials on SARS infection and prevention were put up at the entrance of the collection clinics to remind all prospective donors. All the donors were requested to wear face masks within the donation venue. Moreover, an alcohol‐based hand rinse was available to all donors so that they could disinfect their skin before handling their face masks. Body temperature checking was also introduced for every blood donor as part of donor eligibility criteria.
The staff were required to attend an infection control course on SARS and were constantly updated on the latest developments. Protective measures such as wearing face masks were mandatory within the donation venue and laboratory area. To protect the donor, staff were required to have their body temperature taken before reporting for duty every day.
Regarding facility management, the frequency of the cleaning schedule was increased over and above the normal routine to further reduce the risk of contamination.
1.2. Blood and recipient safety
As SARS was a newly identified viral infection, the understanding of its natural history was relatively limited. Based on the previous case histories, the incubation period was estimated to be between 2 and 10 days. Laboratory diagnostic evaluation was based on testing for the virus by Reverse Transcriptase Polymerase Chain Reaction from the secretions from upper respiratory tract and paired serological titres by immunofluorescence study. Therefore, the policy to combat SARS in blood safety had to be focused on donor deferral policy and a post‐donation call‐back system.
The BTS had implemented a donor deferral policy to temporarily defer prospective donors who had close contact history with patients who suffered from confirmed or suspected SARS. The initial policy was a 2‐week deferral followed by an enquiry into the donor's health status and risk exposure. It was then modified to a 4‐week deferral policy and was reassessed when the donor came again for blood donation. During this period, a total of 57 donors were deferred because of their contact history (Table 1).
TABLE 1.
Results of donor deferral policy on close contact history
| Numbers | |
|---|---|
| Total donors deferred | 57 |
| On follow up, number of donors did not develop SARS, and donors remain healthy and fit. Therefore, donor status can be reinstated. | 7 |
| Number of donors found to have ongoing risk of exposure (eg, working in hospitals, family members of SARS) | 50 |
Moreover, all the donors were reminded to report to the BTS if they experienced any SARS‐related symptoms within 1 month after their donations. Table 2 shows the number of post‐donation call backs during the period studied. It was found that there were more than double the number of call backs in the year 2003 compared to a similar period in 2002. The increase in call backs possibly reflected an increase in the awareness of the donors on their health concern and the BTS effort in donor education. Although some of the donations had been used for transfusion, there were no reports of any adverse reaction in the recipients when they were actively surveyed.
TABLE 2.
The number of post‐donation call backs with SARS‐related symptoms during the period studied
| 11 March 2003 to 23 May 2003 | 29 March 2002 to 22 June 2002 | |
|---|---|---|
| Total number of post‐donation calls with self‐exclusion | 100 | 68 |
| Number of post‐donation calls consistent with symptoms typical of SARS | 83 (83%) | 51 (75%) |
The BTS also followed the WHO recommendation to implement a donor deferral policy for those donors who recovered from confirmed or suspected SARS (http://www.who.int/csr/sars/guidelines/bloodsafety/en/) (accessed April 30, 2020), although very few donors belonging to this category came back to donate.
1.3. Impact on the blood supply
SARS had resulted in many significant changes in the health‐care service in Hong Kong. There was an influx of many SARS patients into hospitals in Hong Kong (eg, cases from Amoy Garden) and an outbreak of SARS infection in health‐care workers, 6 and therefore, a switch in the normal health‐care provision was made as the battle against SARS developed.
For the blood supply, the change in health care had resulted in a 12.8% reduction in the demand of blood (Figure 1). However, the impact of SARS on society, and hence the unwillingness to come forward for blood donation, was also significant. There was about a 16.9% reduction in the blood donation as a result of the decrease in donors attending blood donor centres and mobile sessions and cancellation of large numbers of scheduled mobile sessions (Figure 2). There was continued difficulty in scheduling new mobile sessions during this period because of the fear of SARS.
FIGURE 1.
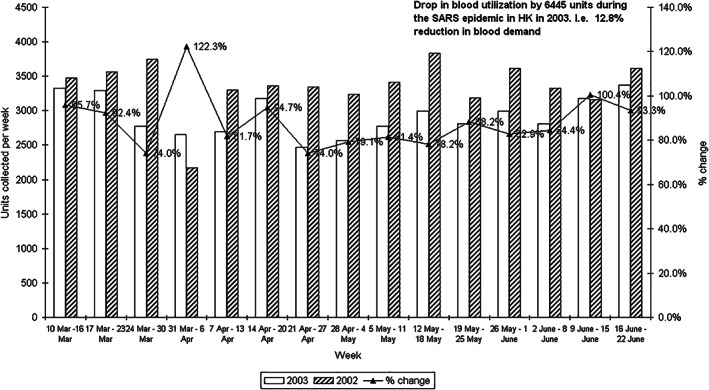
The change in blood utilisation during the period studied. The figure compares blood usage between March and June 2002 and March and June 2003. Overall, there was a drop in blood collection by 6445 units (or 12.8%) during the SARS epidemic in 2003
FIGURE 2.

The change in blood collection during the studied period. The figure compares blood collection between March and June 2002 and March and June 2003. Overall, there was a drop in blood collection by 9365 units (or 16.9%) during the SARS epidemic in 2003
2. DISCUSSION
The new coronavirus and SARS rapidly became a worldwide problem and resulted in a significant impact on the Hong Kong community and health‐care service. Although the BTS normally deals with healthy donors, it could not escape from the pressure of SARS. Many precautionary measures were adopted at the BTS to protect the donors', staff and recipients' safety in addition to its role in maintaining a stable supply of blood products to all the patients in need of transfusion in Hong Kong. It does not appear that SARS was transmitted by blood transfusion. The lessons learned during the epidemic may help prepare for the current global pandemic of COVID‐19 caused by SARS‐CoV‐2 and provide a basis for understanding the pathogenesis, laboratory diagnosis and role of coronaviruses in transfusion medicine. These are continuing problems as epidemics of coronavirus and other respiratory pathogens may recur with future impact on blood collection and blood donation screening.
ACKNOWLEDGMENTS
The authors acknowledge the staff and donors who continued to work to meet the transfusion demand of the patients at that time and are grateful for the valuable comments and advice given by Professor David Roberts.
REFERENCES
- 1. Lee N, Hui D, Wu A, et al. A major outbreak of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1986‐1994. [DOI] [PubMed] [Google Scholar]
- 2. Tsang KW, Ho PL, Ooi GC, et al. A cluster of cases of severe acute respiratory syndrome in Hong Kong. N Engl J Med. 2003;348:1977‐1985. [DOI] [PubMed] [Google Scholar]
- 3. Drosten C, Gunther S, et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348:1967‐1976. [DOI] [PubMed] [Google Scholar]
- 4. Ksiazek TG, Erdman D, Goldsmith CS, et al. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953‐1966. [DOI] [PubMed] [Google Scholar]
- 5. Leung GM, Hedley AJ, Ho LM, et al. The epidemiology of severe acute respiratory syndrome in the 2003 Hong Kong epidemic: an analysis of all 1755 patients. Ann Intern Med. 2004;141:662‐673. [DOI] [PubMed] [Google Scholar]
- 6. Peiris JS, Lai ST, Poon LL, et al. Coronavirus as a possible cause of severe acute respiratory syndrome. Lancet. 2003;361:1319‐1325. [DOI] [PMC free article] [PubMed] [Google Scholar]