

Abstract
[Purpose] We evaluated the reliability of the measurement function of the Honda Walking Assist Device and investigated the effect of the device on walking improvements, and foot and ankle function, in hemiplegic stroke patients. [Participants and Methods] We recruited 16 hemiplegic stroke patients who performed 10-meter walk tests, twice without assistance and once with device assistance. Based on the rate of change of velocity, we divided the participants into two groups and compared the walking parameters, the toe grip strength, the cross tests, and the maximum step width. Two examiners assessed the 10-meter walk test results, and the authors calculated the intraclass correlation coefficients for walking speed, stride length, cadence, flexion, extension, and scissor angles. [Results] The intraclass correlation coefficients were greater than 0.70 for all the walking parameters we measured. The device increased hip joint movement but did not alter the maximum walking speed of the stroke patients. The patients in the group with a greater change in velocity displayed lower toe grip strength and decreased maximum step width and used orthoses more commonly. [Conclusion] The walking measurement function of the device was reliable. The immediate effect of the device in stroke patients may be influenced by the level of paralysis and the presence of an orthosis.
Key words: Honda Walking Assist Device, Hemiplegic stroke, Foot and ankle function
INTRODUCTION
Among the sequelae of stroke, gait disorder has a major impact on daily life. Therefore, improving the ability to walk is one of the main purposes of rehabilitation1). The characteristics of walking in hemiplegic stroke patients include reduced walking speed, decreased stride length, and asymmetric movement of the lower limbs2, 3). The walking speed of hemiplegic stroke patients is related to activities of daily living, and those who walk faster live more actively than those who walk more slowly4). Therefore, gait training is important for improving the walking speed of these patients.
In recent years, many robotic technologies have been introduced to the field of rehabilitation. In the Japanese Guidelines for the Management of Stroke 2015, rehabilitation using robotics is recommended for patients with stroke-induced hemiplegia who cannot walk well. One of the wearable walking support robots in the rehabilitation field is the Honda Walking Assist Device (HWAD) developed by Honda Research & Development, Japan. The HWAD has the Stride Management Assist (SMA®) system that facilitates and measures hip joint movement while walking. The HWAD is light weight and easy to wear. Previous studies of the effects of robotic-assisted gait training (RAGT) with the SMA® system reported immediate improvement of walking efficiency in healthy people5), and improvement of walking speed in the elderly, after long-term use6). In addition, it was reported that walking speed was improved in stroke patients who received RAGT with the SMA® compared to conventional gait training7, 8). Furthermore, Arisue et al. reported that a greater improvement in the stride and walking speed was observed in the slower walking group of convalescent stroke patients compared to the faster walking group9). These results suggest that the effects of RAGT with the SMA® may be beneficial in stroke patients.
In biomechanical studies, Lelas et al. reported that the positive power peak values for the hip and ankle joints in the pre-swing and early swing phases were strongly correlated with increased walking speed in healthy individuals10). In hemiplegic patients, Olney et al. reported that the decrease in walking speed was correlated with the plantar flexors of the ankle, hip flexors, and hip extensors of the affected lower leg11, 12). The HWAD, however, only assists the hip joint. Therefore, it is possible that foot and ankle function may influence the improvement in walking speed observed with the HWAD. In addition, the HWAD measurement function that determines the effect and adjusts the assistance is used to evaluate hip joint movement. However, there have been no reports on the reliability of the measurement function itself. Therefore, the purpose of this study was to evaluate the reliability of the walking measurements of the HWAD and investigate the relationship between foot and ankle function as well as the HWAD-mediated improvement in walking in hemiplegic stroke patients.
PARTICIPANTS AND METHODS
Ten healthy young participants (4 males, 6 females, average age ± standard deviation (SD): 27.8 ± 3.2 years) were recruited to investigate the reliability of the walking measurement of the HWAD (Honda Motor Co., Ltd., Tokyo, Japan) (Fig. 1). Two examiners (Examiner A: HWAD usage history was 5 months; Examiner B: HWAD usage history was 1 month) measured an easy 10-meter walking test (10MWT) in random order. Examiner A measured twice and Examiner B measured once. The HWAD was removed and reattached between measurements. Additionally, the initial setting of HWAD was performed in a standing position between measurements. Intra-rater reliability (Examiner A-A) and inter-rater reliability (Examiner A-B) were determined as follows: the intraclass correlation coefficient (ICC) 1,1 (one-way random single measures) and ICC 2,1 (two-way random single measures), standard error of the measurement (SEM), and the minimal detectable change (MDC) were calculated for walking speed, stride length, cadence, hip flexion angle, extension angle, and scissor angle (flexion angle + contralateral extension angle). The SEM and MDC were calculated as follows13,14,15,16,17):
| SEM=SD ×√(1 − ICC); SD is standard deviation |
| MDC95=SEM×1.96×√2; MDC95 represents the MDC with a confidence interval of 95% |
Fig.1.
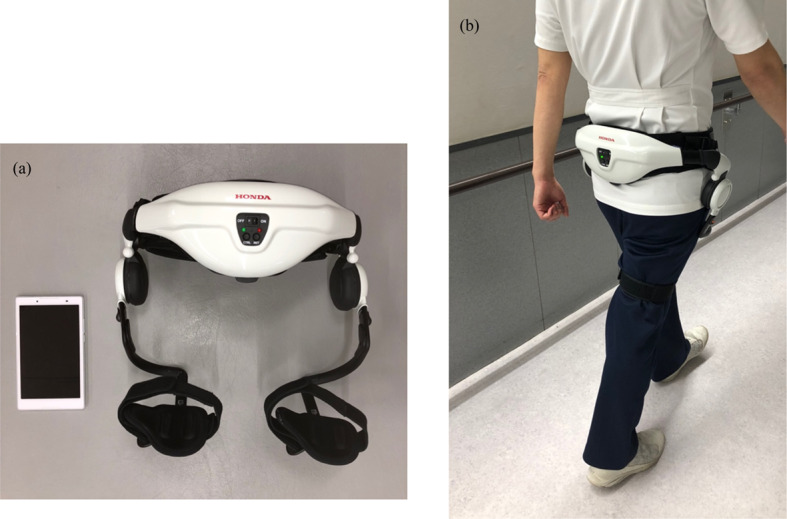
(a) The Honda Walking Assist Device and tablet. (b) How to attach the Honda Walking Assist Device.
The MDC indicates the smallest amount of detectable change in two repeated measurements that is not due to measurement error18).
Sixteen hemiplegic stroke patients (11 males, 5 females) were recruited to investigate the relationship between foot and ankle function and the immediate effects of the HWAD. The patients had the following characteristics: average age 54.2 ± 10.2 years, height 164.9 ± 8.0 cm, and body weight 64.7 ± 7.8 kg; 10 patients had hemiplegia on the right side and 6 on the left side; Brunnstrom recovery stages for the lower extremities were as follows: stage III: 2 patients, stage IV: 5 patients, stage V: 4 patients, and stage VI: 5 patients; nine of the patients were using ankle foot orthosis (AFO) and seven did not. We measured the maximum 10MWT, toe-grip strength (TGS), the cross test, and the one maximum step (OMS) width. The 10MWT was measured 3 times. We measured the first time without the HWAD (N1), the second time with the HWAD (A1), and the third time without the HWAD (N2). An assisted-walking exercise was performed for 3 minutes prior to the A1 test. The torque for the HWAD can be adjusted within a range of 0.0 (minimum)–4.0 N·m. The assisting torque was adjusted to 4.0 N·m for flexion and extension. We compared the walking speed, stride length, and hip joint angle (flexion, extension, scissors angle: flexion + contralateral extension angle) to the three 10MWT trials using repeated measures analysis of variance. Using these data, the participants were divided into two groups according to the median rate of change in velocity that was determined by calculating the ratio of A1/N1 (high change group: HCG ≥1.033, low change group: LCG <1.033). The TGS, cross test, OMS width, and walking parameters were compared using unpaired t-tests between the two groups. The presence or absence of orthosis was compared between the two groups using the Pearson’s χ2 test. IBM® SPSS Statistics for Windows, version 23 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses, and the significance level was set at p<0.05.
The study protocol adhered to the guidelines of the Declaration of Helsinki and was approved by the Tokyo Research Safety Ethics Committee of the Tokyo Metropolitan University (Approval No.16022) and Tokyo Metropolitan Rehabilitation Hospital (Approval No. 14, 2016), Tokyo, Japan. In addition, the study participants were fully informed of the content and purpose of the research, and the study procedures were carried out after obtaining written consent from the participants.
RESULTS
The results for the reliability of the walking measurements of the HWAD are shown in Table 1. In the comfortable 10MWT, three participants who had a change in walking time of 0.5 seconds or more were excluded due to changes in walking speeds. Therefore, data from 7 participants (14 lower limbs) were included in the determination of reliability.
Table 1. Reliability of the walking measurement for the HWAD in healthy participants.
| Average (SD) | ICC 1,1 (95% CI) | ICC 2,1 (95% CI) | SD (d) | SEM | MDC95 | |
| Walking speed (m/min) | 69.9 (13.3) | 0.962 (0.822 to 0.993) | 0.975 (0.874 to 0.996) | 3.92 | 0.764 | 2.12 |
| Step length (cm) | 62.6 (9.8) | 0.986 (0.932 to 0.998) | 0.980 (0.895 to 0.997) | 1.70 | 0.201 | 0.56 |
| Cadence (step/min) | 111.0 (6.5) | 0.901 (0.579 to 0.982) | 0.912 (0.566 to 0.984) | 3.00 | 0.944 | 2.62 |
| Flexion angle (°) | 33.0 (4.4) | 0.758 (0.414 to 0.914) | 0.799 (0.494 to 0.930) | 2.83 | 1.392 | 3.86 |
| Extension angle (°) | 6.5 (4.5) | 0.789 (0.476 to 0.926) | 0.706 (0.315 to 0.894) | 2.66 | 1.222 | 3.39 |
| Scissor angle (°) | 39.9 (3.4) | 0.893 (0.710 to 0.964) | 0.881 (0.677 to 0.960) | 1.68 | 0.550 | 1.52 |
ICC: intraclass correlation coefficient; 95%CI: 95% confidence interval; SD: standard deviation; SEM: standard error of measurement; MDC: minimal detectable change; MDC95: 95%CI of MDC; Scissor angle: includes flexion + contralateral extension angle.
The results of the relationship between foot and ankle function and the HWAD-facilitated improvement in gait function
are shown in Tables 2 and 3. For the three 10MWTs, the flexion and scissor angles on both the paralyzed and non-paralyzed sides and the extension angle on the paralyzed side were greater in A1 than in N1 and N2 tests (p<0.05, Table 2). There were no significant differences in the other gait parameters tested between the three 10MWTs. The comparison of the HCG and LCG groups showed that the HCG group had a significantly smaller OMS value on both the paralyzed and non-paralyzed sides compared to the LCG group (p<0.05, Table 3). The HCG group also had a smaller TGS value on the paralyzed side and significantly more participants using an orthosis compared to the LCG group (p<0.05). There were no significant differences in the cross test and walking parameters between the HCG and LCG groups.
Table 2. Comparison of the three 10-meter walking tests conducted in hemiplegic stroke patients (n=16).
| N1 | A1 | N2 | ||
| Walking speed (m/min) | 69.1 ± 18.1 | 70.8 ± 17.5 | 72.3 ± 19.5 | |
| Step length (cm) | 60.4 ± 9.1 | 61.1 ± 8.6 | 60.5 ± 10.3 | |
| Cadence (steps/min) | 113.4 ± 16.5 | 114.6 ± 15.7 | 117.8 ± 16.0 | |
| Flexion angle – paralyzed side (°) | 29.3 ± 6.6 | 36.5 ± 6.5 | 29.3 ± 7.4 | *1*2 |
| Flexion angle – non-paralyzed side (°) | 35.0 ± 6.1 | 45.0 ± 6.9 | 36.4 ± 5.9 | *1*2 |
| Extension angle – paralyzed side (°) | 8.9 ± 4.3 | 12.7 ± 4.3 | 11.3 ± 4.8 | *1*3 |
| Extension angle – non-paralyzed side (°) | 11.9 ± 5.7 | 11.0 ± 8.7 | 12.9 ± 6.4 | |
| Scissor angle – paralyzed side (°) | 32.2 ± 6.9 | 40.4 ± 11.3 | 35.4 ± 8.0 | *1*2 |
| Scissor angle – non-paralyzed side (°) | 39.4 ± 5.6 | 55.8 ± 8.2 | 44.9 ± 6.5 | *1*2*3 |
Scissor angle: includes flexion angle + contralateral extension angle.
*p<0.05.
N1: without assist; A1: with assist; N2: without assist; *1: Significant differences between N1 and A1; *2: significant differences between A1 and N2; *3: significant differences between N1 and N2.
Table 3. Comparison between the HCG and LCG.
| HCG (n=8) | LCG (n=8) | |||
| Walking speed (m/min) | 61.6 ± 14.0 | 76.6 ± 19.4 | ||
| Step length (cm) | 56.8 ± 4.8 | 64.0 ± 11.1 | ||
| Cadence (steps/min) | 108.3 ± 18.6 | 118.5 ± 13.4 | ||
| Flexion angle - paralyzed side (°) | 27.7 ± 7.0 | 31.0 ± 6.2 | ||
| Flexion angle - non-paralyzed side (°) | 34.1 ± 6.5 | 36.0 ± 6.0 | ||
| Extension angle - paralyzed side (°) | 8.9 ± 4.0 | 9.0 ± 4.9 | ||
| Extension angle - non-paralyzed side (°) | 12.2 ± 7.0 | 11.6 ± 4.5 | ||
| Scissors angle - paralyzed side (°) | 42.5 ± 8.2 | 39.8 ± 12.7 | ||
| Scissors angle - non-paralyzed side (°) | 45.0 ± 7.7 | 43.0 ± 6.6 | ||
| Cross test | A-P (cm) | 11.8 ± 2.0 | 12.6 ± 1.7 | |
| L-R (cm) | 15.2 ± 2.6 | 18.8 ± 10.0 | ||
| Rectangular area (cm2) | 185.4 ± 59.8 | 244.0 ± 141.3 | ||
| OMS (/leg length) | Paralyzed side | 0.46 ± 0.12 | 0.70 ± 0.19 | * |
| Non-paralyzed side | 0.39 ± 0.16 | 0.78 ± 0.18 | * | |
| TGS (/weight) | Paralyzed side | 0.06 ± 0.05 | 0.15 ± 0.05 | * |
| Non-paralyzed side | 0.16 ± 0.05 | 0.17 ± 0.08 | ||
| Number of patients using AFO (paralyzed side) | 7 | 2 | * | |
*p<0.05.
A-P: anterior-posterior; L-R: left-right; OMS: one maximum step; TGS: toe grip strength;
HCG: high change group (walking speed A1/N1 ≥1.033); LCG: low change group (walking speed A1/N1 <1.033).
DISCUSSION
In this study, we evaluated the reliability of the measurement function for the HWAD in healthy young participants. In addition, we investigated the relationship between foot and ankle function and the walking improvement facilitated by the HWAD in hemiplegic stroke patients. Our findings revealed that both the intra-rater ICC (1,1) and inter-rater ICC (2,1) values for all the parameters tested were greater than 0.70. The HWAD changed the hip movement significantly, but did not change the maximum walking speed in the hemiplegic patients. The group of stroke participants with a greater change in velocity when using the HWAD (HCG) had smaller OMS on both sides and smaller TGS on the paralyzed side, and many of them used orthoses compared to the LCG participants.
According to the criteria of Kuwabara et al., an ICC of >0.9 indicated great, >0.80 indicated good, 0.70–0.79 indicated normal, and <0.60 indicated poor reliability17). According to the criteria of Landis and Koch, an ICC of 0.81–1.00 indicated almost perfect, 0.61–0.80 indicated substantial, and 0.41–0.60 indicated normal reliability19). In our study, using the criteria described above, the ICCs of hip flexion and extension angle (0.706–0.799) can be classified as normal to substantial reliability, and the scissor angle ICCs (0.881–0.893) can be classified as good to almost perfect reliability. Therefore, we demonstrated that the HWAD measurement function for walking parameters was reliable. In this study, the reliability of the scissor angle measurements was higher than the reliability of the flexion and extension angle measurements. A possible explanation for this result could be attributed to the influence of the displacement of the baseline (0 degrees) of flexion-extension during detachment-attachment, and the small initial setting, as the scissor angle was the sum of the flexion angle and the contralateral extension angle. The reliability of the HWAD makes it a useful evaluation tool for measuring the walking parameters.
The results of our study support the concept that the HWAD, and possibly other robotic assistance devices, may not immediately offer a benefit for highly functional patients and the benefit may be dependent on the level of paralysis. Furthermore, it is possible that an immediate improvement of the walking speed was not observed because the HWAD assisted only the hip joint and not the ankle joint. Patients with more severe paralysis would have lower TGS and a greater need for orthoses. In order to increase the OMS on the paralyzed side, it is necessary for the patient to increase the swing of the paralyzed side. To increase the OMS on the non-paralyzed side, the lower limbs on the paralyzed side must be stabilized in the posture and the swing on the non-paralyzed side must be increased. Thus, paralysis would affect the bilateral OMS. The immediate effects of the HWAD in stroke patients may also be influenced by the use of AFO.
This study was limited in that the relationship was unclear between the hip and other lower limb joints (such as the knee and ankle), which is important for hemiplegic walking, because HWAD can only measure the hip joint. Therefore, future research would need to use 3-dimensional motion analysis during walking with HWAD. We recruited only healthy young participants in our reliability study and we did not examine the reliability of hemiplegic patients. A study of reliability in hemiplegic patients who can walk, with or without a walking aid, reported high reliability in walking speed and joint movement20). Therefore, examinations of hemiplegic patients wearing HWAD would be equally reliable. However, it is necessary to examine the reliability of HWAD in hemiplegic patients.
In conclusion, this study demonstrated for the first time that the HWAD measurements were reliable and may be useful as an evaluation tool in hemiplegic stroke patients, as well as other groups of patients with gait disorders. Furthermore, our study shows that the HWAD does not immediately affect walking speed and further research will be necessary to determine the long-term walking improvements afforded by this device. We propose that when using the HWAD, consideration should be given to the level of paralysis and the presence of orthoses to determine the efficacy of this device in hemiplegic stroke patients.
Funding
None.
Conflict of interest
The authors have no conflicts of interest directly relevant to the content of this article.
REFERENCES
- 1.Dobkin BH: Clinical practice. Rehabilitation after stroke. N Engl J Med, 2005, 352: 1677–1684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Olney SJ, Richards C: Hemiparetic gait following stroke. Part I: characteristics. Gait Posture, 1996, 4: 136–148. [Google Scholar]
- 3.Hsu AL, Tang PF, Jan MH: Analysis of impairments influencing gait velocity and asymmetry of hemiplegic patients after mild to moderate stroke. Arch Phys Med Rehabil, 2003, 84: 1185–1193. [DOI] [PubMed] [Google Scholar]
- 4.Sajiki N, Nakamura R, Hosokawa T: The relation between walking function and daily life activities of stroke patients at home. Jpn J Rehabil Med, 1991, 28: 541–548. [Google Scholar]
- 5.Kitatani R, Ohata K, Takahashi H, et al. : Reduction in energy expenditure during walking using an automated stride assistance device in healthy young adults. Arch Phys Med Rehabil, 2014, 95: 2128–2133. [DOI] [PubMed] [Google Scholar]
- 6.Shimada H, Hirata T, Kimura Y, et al. : Effects of a robotic walking exercise on walking performance in community-dwelling elderly adults. Geriatr Gerontol Int, 2009, 9: 372–381. [DOI] [PubMed] [Google Scholar]
- 7.Buesing C, Fisch G, O’Donnell M, et al. : Effects of a wearable exoskeleton stride management assist system (SMA®) on spatiotemporal gait characteristics in individuals after stroke: a randomized controlled trial. J Neuroeng Rehabil, 2015, 12: 69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tanaka N, Matsushita S, Sonoda Y, et al. : Effect of stride management assist gait training for poststroke hemiplegia: a single center, open-label, randomized controlled trial. J Stroke Cerebrovasc Dis, 2019, 28: 477–486. [DOI] [PubMed] [Google Scholar]
- 9.Arisue I, Tanaka N, Fujii Y, et al. : The influence of gait exercises using a walking assistance robot on the gait speed of stroke patients in the convalescent stage. Rigakuryoho Kagaku, 2015, 30: 119–123 (in Japanese). [Google Scholar]
- 10.Lelas JL, Merriman GJ, Riley PO, et al. : Predicting peak kinematic and kinetic parameters from gait speed. Gait Posture, 2003, 17: 106–112. [DOI] [PubMed] [Google Scholar]
- 11.Olney SJ, Griffin MP, McBride ID: Temporal, kinematic, and kinetic variables related to gait speed in subjects with hemiplegia: a regression approach. Phys Ther, 1994, 74: 872–885. [DOI] [PubMed] [Google Scholar]
- 12.Olney SJ, Griffin MP, Monga TN, et al. : Work and power in gait of stroke patients. Arch Phys Med Rehabil, 1991, 72: 309–314. [PubMed] [Google Scholar]
- 13.Ohya N, Yamada T, Satoh Y, et al. : Relative and absolute reliability of ultrasound measurements for the thickness of the soft tissue around the shoulder joint of young normal subjects. J Phys Ther Sci, 2017, 29: 754–759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ohya N, Yamada T, Satoh Y: Inter-rater reliability of ultrasound measurements of the thickness of the supraspinatus tendon, subacromial bursa and biceps tendon of young adults. Rigakuryoho Kagaku, 2017, 32: 603–607 (in Japanese). [Google Scholar]
- 15.Chuang LL, Wu CY, Lin KC, et al. : Relative and absolute reliability of a vertical numerical pain rating scale supplemented with a faces pain scale after stroke. Phys Ther, 2014, 94: 129–138. [DOI] [PubMed] [Google Scholar]
- 16.Takacs J, Garland SJ, Carpenter MG, et al. : Validity and reliability of the community balance and mobility scale in individuals with knee osteoarthritis. Phys Ther, 2014, 94: 866–874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kuwabara Y, Saito T, Inagaki Y: [Evaluation of intra- and inter-observer reliability]. Kokyu To Junkan, 1993, 41: 945–952 (in Japanese). [PubMed] [Google Scholar]
- 18.Shimoi T, Tani H: The absolute reliability of two different tandem gait tests with minimal detectable change. Rigakuryouho Kagaku, 2010, 25: 49–53 (in Japanese). [Google Scholar]
- 19.Landis JR, Koch GG: The measurement of observer agreement for categorical data. Biometrics, 1977, 33: 159–174. [PubMed] [Google Scholar]
- 20.Geiger M, Supiot A, Pradon D, et al. : Minimal detectable change of kinematic and spatiotemporal parameters in patients with chronic stroke across three sessions of gait analysis. Hum Mov Sci, 2019, 64: 101–107. [DOI] [PubMed] [Google Scholar]