

Abstract
The COVID‐19 pandemic has plunged the world into a crisis. To contain this crisis, it is essential to build full cooperation between the government and the public. However, it is unclear which governmental and individual factors are determinants and how they interact with protective behaviors against COVID‐19. To resolve this issue, this study builds a multiple mediation model. Findings show that government emergency public information such as detailed pandemic information and positive risk communication had greater impact on protective behaviors than rumor refutation and supplies. Moreover, governmental factors may indirectly affect protective behaviors through individual factors such as perceived efficacy, positive emotions, and risk perception. These findings suggest that systematic intervention programs for governmental factors need to be integrated with individual factors to achieve effective prevention and control of COVID‐19 among the public.
The COVID‐19 pandemic has plunged the world into a crisis, and its effect on people's physical and mental health, economic development, and social stability cannot be underestimated (van Gelder et al. 2020). China is not only one of the first countries to experience the outbreak of COVID‐19 infection but also one of the few that have largely contained it. This cannot be separated from the strict governmental supervision and people's effective protective behaviors (Li, Chen, and Huang 2020). Therefore, drawing on China's experience in pandemic prevention and control can help accelerate the world's progress in defeating the disease.
The Protective Action Decision Model (PADM) was developed to explore people's actions in response to natural hazards and disaster events. According to the PADM, various sources of information cause people's attention, exploration, and comprehension to generate threat perceptions, protective action perceptions, and stakeholder perceptions, prompting them to form decisions about how to take self‐protective actions (Lindell 2018; Lindell and Perry 2012). Based on this framework, the current study proposes an information‐perception/consideration‐action mediation model to elucidate protective behaviors during a pandemic. In this model, government emergency public information is considered to be the source of information, and the individual's emotional and cognitive perception and consideration are considered to be an extension of perceptions in the PADM model. Additionally, protective behaviors, including preventive behaviors (i.e., wearing masks, disinfectants) (Kim et al. 2015), avoidant behaviors (i.e., stringent quarantine, avoiding public places) (Bayham et al. 2015), and management of disease behaviors (i.e., seeking professional protection or treatment information, paying for preventive and therapeutic drugs) (Hagan, Maguire, and Bopping 2008), are considered to be the actions (Bish and Michie 2010). One important issue that should be explored is how government emergency public information can persuade the public to adopt recommended protective behaviors to control the spread of COVID‐19.
Government emergency public information should enhance the public's courage and determination, raise their risk awareness, and prompt people to adopt effective protections to fight the pandemic (Paek et al. 2008). The Chinese government implemented several effective emergency public information measures through detailed pandemic information, positive risk communication, and rumor refutation (Chon and Park 2019; Li, Chen, and Huang 2020; Xu et al. 2020). Detailed pandemic information includes released statistical information, such as confirmed cases, dynamic suspected cases, recovered cases, and deaths, both in accumulative numbers and daily updates, as well as tracked information, including the travel history and trains or flights taken by specific confirmed or suspected patients. During the COVID‐19 pandemic, this kind of detailed information has become the foundation of current South Korean policy actions to combat COVID‐19 (Moon 2020).
Some researchers believe that detailed information can increase people's risk perception and promote protective behaviors (French 2011; Qazi et al. 2020). Positive risk communication conveying positive educational information can result in more appropriate manners (Fewtrell and Bartram 2001). According to the report China's Fight against COVID‐19 (China Daily 2020), the achievements in the fight against the virus and the stories of frontline medical workers and volunteers reported in the mainstream media could inspire people to participate in efforts to control the pandemic. Rumors increase the uncertainty of public information and trigger conspiracy theories and pseudoscientific claims (Dredze, Broniatowski, and Hilyard 2016; Sharma et al. 2017). One important challenge in controlling the Ebola hemorrhagic outbreak was numerous rumors (Lamunu et al. 2004). Timely refutation of rumors can help the government reduce public confusion, reduce perceived risk and panic, build trust, and promote proper protective behaviors (DiFonzo and Bordia 2007; Greenhill and Oppenheim 2017).
In addition, medical supplies during a pandemic are desperately needed (WHO 2015). For example, during the 2014 West Africa Ebola epidemic, evidence suggests that earlier supplies modestly reduced mortality (Walker and Whitty 2015). Efforts to add supplies such as lifesaving medicines and trained clinicians could increase public trust and encourage people to seek clinical care (WHO Ebola Response Team 2014). During this COVID‐19 pandemic, the rapid construction of Huoshenshan Hospital made people feel more concerned about the pandemic and feel that they had “warriors” in this battle (Allen 2020).
Perceived efficacy, positive emotions, and risk perception are important individual factors affecting protective behaviors (Prati, Pietrantoni, and Zani 2011). First, perceived efficacy plays a key role in positively predicting protective behaviors (Balkhy et al. 2010; Rubin et al. 2009; Seale et al. 2009). According to the protection‐motivation theory (Rippetoe and Rogers 1987), perceived efficacy is made up of self‐efficacy and response efficacy. Self‐efficacy refers to individuals’ confidence in their abilities to carry out protective behaviors, and response efficacy refers to individuals’ belief in the effectiveness of protective behaviors in coping with a health threat. People with higher perceived efficacy were more likely to take precautionary behaviors and seek control during the avian influenza pandemic (de Zwart et al. 2010). Conversely, people with low perceived efficacy felt less control and thus did little to change the outcomes of the swine flu pandemic (Lo, Wei, and Herng 2013).
Second, positive emotions play a crucial role in coping with crisis situations (Folkman and Moskowitz 2016; Fredrickson et al. 2003). Individuals who experience gratitude and hope can gain resilience and perceived efficacy to cope with the crisis more effectively (Emmons and Stern 2013; Ong, Edwards, and Bergeman 2006). A study conducted during the H1N1 influenza outbreak showed that these two positive emotions, gratitude and hope, mediated the relationship between crisis responsibility and disease management behaviors (Kim and Niederdeppe 2013). Furthermore, several studies have reported a positive correlation between risk perception and protective behaviors. Higher risk perception was associated with a higher likelihood of hand washing, personal hygiene, household disinfection, mask wearing, and avoidant behaviors during the H1N1, SARS, and the swine flu epidemics (Jones and Salathe 2009; Lau et al. 2004; Rubin et al. 2009; Wong and Tang 2005). In summary, it is crucial to identify the effects of perceived efficacy, positive emotions (such as gratitude and hope), and risk perception on anti‐pandemic behaviors.
Government emergency public information and individual factors are regarded as important contributors to protective behaviors during a pandemic (Chon and Park 2019). However, it remains unclear how these factors interact with each other and whether their interaction has an impact on protective behaviors. Therefore, the current study proposes a model with seven explanatory variables (see figure 1). Detailed pandemic information, positive risk communication, rumor refutation, and supplies are postulated as government emergency public information factors. Perceived efficacy, positive emotions, and risk perception are postulated as individual perception and consideration factors. Based on these hypotheses, this study tests two hypotheses. The first is that government emergency public information will encourage people to comply with protective behaviors directly. The second is that government emergency public information will contribute to protective behaviors by increasing people's perceived efficacy, positive emotions, and perceptions of risk.
Figure 1.
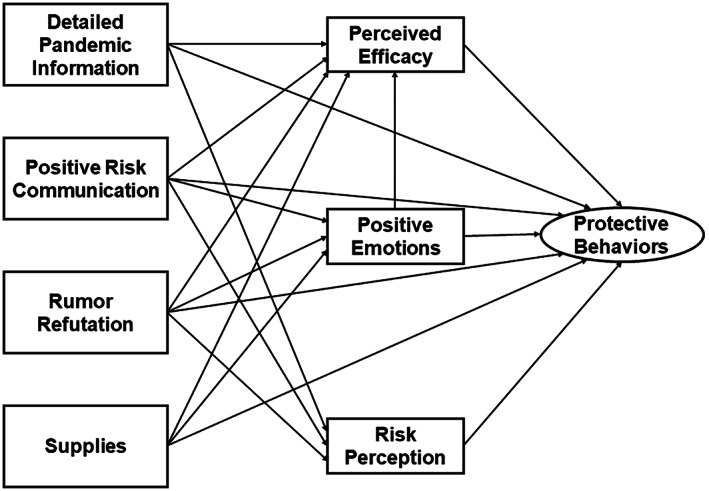
The Hypothesized Model for Predicting Protective Behaviors
Method
Participants and Data Collection
This cross‐sectional design research was approved by the Institutional Review Board of the Institute of Psychology, Chinese Academy of Sciences, and followed the Declaration of Helsinki. Data collection was conducted from February 24, 2020, to March 3, 2020. All the participants were recruited online from 33 provinces in China. After reading and signing the informed consent, we asked participants to rate government, personal, and behavior factors for 21 items on a 7‐point Likert scale (see table 1). The government factors measured detailed pandemic information (Cronbach's α = 0.67) with two items, positive risk communication and rumor refutation with a single item, and supplies (Cronbach's α = 0.84) with five items. The personal factors measured perceived efficacy (Cronbach's α = 0.67) with four items, positive emotions (Cronbach's α = 0.84) with two items, and risk perception with one item. The behavior factors measured protective behaviors (Cronbach's α = 0.65) with two preventive behavior items, one avoidant behavior item, and two management of disease behavior items. In the present study, these items were chosen to reflect the main components of these variables in the context of the COVID‐19 pandemic, and most of them had good or acceptable reliabilities.
Table 1.
Survey on COVID‐19
| Factors | Items |
|---|---|
| Governmental factors | |
| Detailed pandemic information | Suspected numbers, infected numbers, critically ill numbers, and death toll in different regions are officially announced every day. 1 (strongly disagree) to 7 (strongly agree) |
| Confirmed patient's recent movements are officially published as soon as possible. 1 (strongly disagree) to 7 (strongly agree) | |
| Positive risk communication | A lot of information about medical staff and supplies brought from other areas to the front line is officially announced. 1 (strongly disagree) to 7 (strongly agree) |
| Rumor refutation | Fake news is officially refuted in time. 1 (strongly disagree) to 7 (strongly agree) |
| Supplies | Medical staff are sufficient in your current country or region. 1 (strongly disagree) to 7 (strongly agree) |
| Medical supplies are sufficient in your current country or region. 1 (strongly disagree) to 7 (strongly agree) | |
| Living supplies are sufficient in your current country or region. 1 (strongly disagree) to 7 (strongly agree) | |
| Mental health support is sufficient in your current country or region. 1 (strongly disagree) to 7 (strongly agree) | |
| Patients are treated on time during the pandemic. 1 (strongly disagree) to 7 (strongly agree) | |
| Personal factors | |
| Perceived efficacy | I believe the pandemic will be fully controlled in the foreseeable future. 1 (strongly disagree) to 7 (strongly agree) |
| I am confident that the pandemic will be overcome. 1 (strongly disagree) to 7 (strongly agree) | |
| To cope with the pandemic, I can discriminate between true information and rumors about COVID‐19. 1 (strongly disagree) to 7 (strongly agree) | |
| To combat the pandemic, I do not post or forward any messages that have not been officially confirmed about COVID‐19. 1 (strongly disagree) to 7 (strongly agree) | |
| Positive emotions | In the last 10 days, what intensity of gratitude have you experienced? 1 (very low) to 7 (very high) |
| In the last 10 days, what intensity of hope have you experienced? 1 (very low) to 7 (very high) | |
| Risk perception | In your opinion, how contagious is COVID‐19? 1 (very low) to 7 (very high) |
| Protective behaviors | |
| Preventive | When I leave my home now, I usually wear a face mask. 1 (strongly disagree) to 7 (strongly agree) |
| When I return home from outside, I disinfect myself with alcohol spray or sanitizer. 1 (strongly disagree) to 7 (strongly agree) | |
| Avoidant | I will not go out until the pandemic is over unless I have to. 1 (strongly disagree) to 7 (strongly agree) |
| Management of illness | As soon as COVID‐19 preventive and treatment medications appear on the market, I will pay for them immediately. 1 (strongly disagree) to 7 (strongly agree) |
| I usually get medical information and prevention measures about COVID‐19. 1 (strongly disagree) to 7 (strongly agree) | |
A total of 1,131 participants finished the survey. Data from 1,022 participants (90.4 percent) entered the final statistical analyses after deleting the invalid data, in which participants gave a wrong response to a question used to detect whether they answered the questionnaire carefully. Participants’ demographic information is displayed in table 2. Comparison of the sample's demographic characteristics with the corresponding census data suggested that the sample overrepresented youth, higher education population, and students.
Table 2.
Demographics of Participants
| Sample Size (N = 1,022) | Percent (%) | |
|---|---|---|
| Gender | ||
| Male | 409 | 40.0 |
| Female | 613 | 60.0 |
| Age | ||
| 18–25 | 458 | 44.8 |
| 26–35 | 279 | 27.3 |
| 36–45 | 152 | 14.9 |
| 46–61 | 120 | 11.7 |
| unknown | 13 | 1.3 |
| Education background | ||
| High school or lower | 136 | 13.3 |
| College/technical school | 81 | 7.9 |
| University bachelor's degree | 461 | 45.1 |
| Master's degree or higher | 344 | 33.7 |
| Career background | ||
| Student | 470 | 46.0 |
| Medical staff | 53 | 5.2 |
| Teacher/lawyer/civil servant | 181 | 17.7 |
| Manager/office clerk | 140 | 13.7 |
| Factory worker/agricultural worker | 53 | 5.2 |
| Subcontractor/service employee | 31 | 3.0 |
| Other | 94 | 9.2 |
Data Analysis
Data were analyzed using SPSS version 20.0, Amos version 23.0, and Mplus 7.0. T‐tests and one‐way analyses of variance (ANOVAs) were used to explore whether there were gender, age, and education differences in protective behaviors. Descriptive statistics were used to describe the sample characteristics of each factor. Pearson correlation analyses were performed to examine whether associations between factors conformed to the prerequisites for path analysis. Path analysis was conducted to test the model. The squared multiple regression correlation coefficient was estimated to identify the variance in protective behaviors that was explained by proposed factors. Bootstrap resampling was employed to test the significance of direct and indirect variable effects (MacKinnon, Lockwood, and Williams 2004).
Results
Impact of Demographic Features on Protective Behaviors
We analyzed how gender, age, and education background impact protective behaviors. A t‐test showed that gender had a significant effect on protective behaviors, t (1020) = 5.16, p < .001. Females showed more protective behaviors (M ± SD = 29.69 ± 3.87) than males (M ± SD = 28.23 ± 5.18). One‐way ANOVA showed that age had a significant effect on protective behaviors, F (3, 1,005) = 5.82, p < .001. A post hoc test indicated that participants from 18 to 25 years (M ± SD = 28.49 ± 4.36) showed significantly fewer protective behaviors than participants from 46 to 61 years (M ± SD = 30.13 ± 4.73), p < .01. No significant differences were found between other age groups, p > .05. One‐way ANOVA showed that education background had a significant effect on protective behaviors, F (3, 1,018) = 4.33, p < .01. A post hoc test indicated that participants with high school or lower education background (M ± SD = 30.08 ± 4.46) had significantly more protective behaviors than participants with university bachelor's degree (M ± SD = 28.81 ± 4.69), p < .05. No significant differences were found between other groups, p > .05.
Descriptive Statistics and Correlations
Means and standard deviations for the predictors of protective behaviors, as well as the correlation coefficients between them, are displayed in table 3. Only the association between risk perception and supplies was not significant (r = .03, p > .05). Associations between other factors and protective behaviors reached significance (p < .05). Furthermore, all the proposed governmental and individual factors were positively correlated with preventive, avoidant, and management of disease behaviors (p < .05). These three protective behaviors were also positively correlated with each other significantly (p < .05). Therefore, path analysis could be performed based on the current model.
Table 3.
Means, Standard Deviations, and Correlation Matrix of Predictive Factors
| Factors | M ± SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Detailed pandemic information | 12.44 ± 2.13 | 1 | |||||||||
| 2 Positive risk communication | 5.87 ± 1.32 | .32** | 1 | ||||||||
| 3 Rumor refutation | 5.24 ± 1.57 | .22** | .41** | 1 | |||||||
| 4 Supplies | 21.27 ± 6.38 | .08* | .30** | .41** | 1 | ||||||
| 5 Perceived efficacy | 23.22 ± 3.86 | .40** | .45** | .48** | .35** | 1 | |||||
| 6 Positive emotions | 10.50 ± 2.80 | .20** | .37** | .35** | .24** | .44** | 1 | ||||
| 7 Risk perception | 6.36 ± 1.04 | .26** | .17** | .11** | .03 | .17* | .19** | 1 | |||
| 8 Preventive behaviors | 12.61 ± 1.97 | .29** | .31** | .19** | .08** | .27** | .20** | .21** | 1 | ||
| 9 Avoidant behaviors | 5.76 ± 1.49 | .25** | .38** | .25** | .14** | .24** | .24** | .16** | .42** | 1 | |
| 10 Management of disease | 10.74 ± 2.31 | .24** | .28** | .24** | .19** | .29** | .24** | .15** | .48** | .29** | 1 |
*p < .05; **p < .01.
Mediational Model
The model data fit was evaluated using χ2, χ2/df, root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), normed fit index (NFI), comparative fit index (CFI), and goodness of fit index (GFI). The RMSEA and SRMR should be less than .08. Regarding NFI, CFI, and GFI, values no less than .90 indicate a good model fit, whereas values above .95 indicate an excellent fit (Cohen et al. 2003). Because protective behaviors may be associated with a variety of demographic factors, the hypothesized model was performed adding gender, age, and education as control variables, which is a common statistics method considering the confounding effects of personal characteristics (e.g., Hew et al. 2018). Results of the initial hypothesized model (χ2 = 336.243, χ2/df = 7.005, RMSEA = .077, SRMR = .072, NFI = .867, CFI = .882, GFI = .950) showed that the fit of the model is suboptimal, while there were five nonsignificant pathways for age and protective behaviors (β = −.01, p = .693), education and protective behaviors (β = −.06, p = .074), rumor refutation and protective behaviors (β = .06, p = .157), supplies and protective behaviors (β = .01, p = .815), and rumor refutation and risk perception (β = .03, p = .374) in this model. After removing these five pathways, results of the measurement showed that the modified model fit the data excellently (χ2 = 114.423, χ2/df = 3.814, RMSEA = .052, SRMR = .036, NFI = .950, CFI = .962, GFI = .980). Pathway coefficients within factors are displayed in figure 2.
Figure 2.
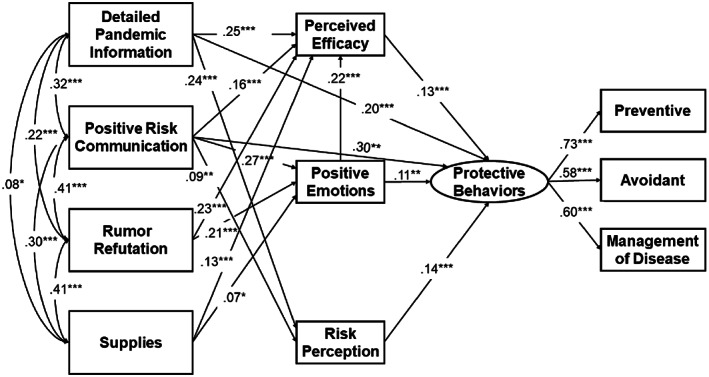
Standardized Estimates of the Predicting Model. *p < .05; **p < .01; ***p < .001.
Governmental and Individual Predictors of Protective Behaviors
To construct a model with a more reliable confidence interval (CI), this study set bootstrapping at 5,000 as recommended to yield a 95 percent CI (MacKinnon, Lockwood, and Williams 2004). The final model accounted for 39.6 percent of the total variance of protective behaviors. Gender was found to predict protective behaviors significantly negatively (β = −.22, p < .001), indicating that males adopted fewer protective behaviors than females. Detailed pandemic information (total effect [TE] = .268, p < .001) and positive risk communication (TE = .365, p < .001) were found to affect protective behaviors more than rumor refutation (TE = .058, p < .001) and supplies (TE = .027, p < .001). Besides, all governmental factors have significant indirect influences on protective behaviors. Statistical significance was approached by all the direct and indirect effects of government emergency public information on protective behaviors on the grounds of bootstrapping results (table 4).
Table 4.
Total, Direct, and Indirect Effects of Government Emergency Public Information on Protective Behaviors
| Effects of Predictors | β | Bias‐Correlated 95% CI |
|---|---|---|
| 1 Detailed pandemic information | ||
| TE | .268*** | [.189, .348] |
| DE | .202*** | [.119, .286] |
| IE | .066*** | [.037, .101] |
| 2 Positive risk communication | ||
| TE | .365*** | [.276, .455] |
| DE | .296*** | [.201, .394] |
| IE | .069*** | [.039, .104] |
| 3 Rumor refutation | ||
| TE | .058*** | [.032, .092] |
| DE | — | — |
| IE | .058*** | [.032, .092] |
| 4 Supplies | ||
| TE | .027*** | [.012, .048] |
| DE | — | — |
| IE | .027*** | [.012, .048] |
Notes: All the estimates provided in the table are standardized estimates. TE = total effect; DE = direct effect; IE = indirect effect; CI = confidence interval.
*p < .05; **p < .01; ***p < .001.
In addition, to further examine whether the mediating effect was significant, the indirect effects were computed using the bias‐corrected bootstrapping method; if the 95 percent CI did not include 0, the mediating effect was significant (MacKinnon, Lockwood, and Williams 2004). Table 5 displays the indirect effects of individual factors. Thus, with the exception of three multiple‐mediating effects of “Supplies → positive emotions → protective behaviors,” “Supplies → positive emotions → perceived efficacy → protective behaviors,” and “Positive risk communication → risk perception → protective behaviors,” the significant mediating roles of perceived efficacy, positive emotion, and risk perception were confirmed.
Table 5.
Standardized Indirect Effects and 95% Confidence Intervals
| Model Pathways | β | Bias‐Correlated 95% CI |
|---|---|---|
| Detailed pandemic information → perceived efficacy → protective behaviors | .033** | [.010, .056] |
| Positive risk communication → perceived efficacy → protective behaviors | .021** | [.005, .036] |
| Rumor refutation → perceived efficacy → protective behaviors | .030** | [.009, .051] |
| Supplies → perceived efficacy → protective behaviors | .017* | [.003, .032] |
| Positive risk communication → positive emotions→ protective behaviors | .028* | [.005, .052] |
| Rumor refutation → positive emotions → protective behaviors | .022* | [.002, .042] |
| Supplies → positive emotions → protective behaviors | .008 | [−.002, .017] |
| Positive risk communication → positive emotions → perceived efficacy → protective behaviors | .008** | [.002, .014] |
| Rumor refutation → positive emotions → perceived efficacy → protective behaviors | .006** | [.002, .011] |
| Supplies → positive emotions → perceived efficacy → protective behaviors | .002 | [0, .005] |
| Detailed pandemic information → risk perception → protective behaviors | .033** | [.010, .055] |
| Positive risk communication → risk perception → protective behaviors | .013 | [−.002, .027] |
Note: All the estimates provided in the table are standardized estimates.
*p < .05; **p < .01; ***p < .001.
Discussion
This study proposed an information‐perception/consideration‐action framework and used a path analysis model to elucidate the relationship between government emergency public information and individual factors and their impact on protective behaviors during the COVID‐19 pandemic in China. The results showed that detailed pandemic information, positive risk communication, rumor refutation, and supplies positively predicted the protective behaviors. Meanwhile, perceived efficacy, positive emotions, and risk perception played a significant role in predicting protective behaviors. This study provides a reliable and instructive framework for governments to cope with the pandemic crisis.
In the final model, age and education background had no significant impacts on protective behaviors, except that males adopted fewer protective behaviors than females. This was consistent with a meta‐analysis of the association between gender and protective behaviors (Moran and Del Valle 2016) showing that females were about 50 percent more likely than males to adopt nonpharmaceutical behaviors (e.g., hand washing, face mask use, avoidance of the public). Results suggested that government risk communication should strengthen the protective behaviors of males.
Government emergency public information had a significant positive impact on protective behaviors. First, detailed pandemic information had a significant positive effect on protective behaviors. Consistent with previous research (Kass et al. 2014), when the public was more informed about the reality of the pandemic and what the government was doing about it, people were more likely to follow the government's recommendations. Detailed pandemic information may increase the public's trust in the government and make people more willing to implement recommended protective behaviors (Siegrist and Zingg 2014). On the contrary, people may distrust the government if information is concealed or misreported, which may cause negative or hostile actions (Driedger, Michelle, and Jardine 2018).
Second, positive risk communication showed a strong positive effect on protective behaviors. Information on the transport of medical staff and supplies may reduce the sense of insecurity and strengthen public cohesion, thus encouraging the public to actively participate in controlling the spread of the coronavirus (Stockmann and Gallagher 2011). Third, rumor refutation had a positive impact on protective behaviors. According to previous research (Barrelet et al. 2013), rumors may increase the public's distrust of government (Sharma et al. 2017). Rumor refutation is beneficial and crucial for the government to establish an image of integrity, to dispel conspiracy theories and the public's unnecessary fear, and to promote confidence and protective behaviors against the pandemic (DiFonzo and Bordia 2007; Greenhill and Oppenheim 2017).
Lastly, supplies predict protective behaviors indirectly. The government's efforts to provide supplies may affect the public's perceived efficacy and positive emotions to improve protective behaviors (Allen 2020; WHO Ebola Response Team 2014). Furthermore, detailed pandemic information and positive risk communication were more predictive than rumor refutation and supplies, because the first two variables had both direct and indirect effects, whereas the latter two only had indirect effects. This indicated that the government's active regulatory policies were more effective in improving people's protective behaviors than actual supplies such as medical treatments and material resources that were powerless to change by the government.
Government emergency public information influenced anti‐pandemic behaviors through the mediation of individual factors. First, consistent with previous research (Barnett et al. 2014), this study confirmed the mediating role of perceived efficacy on the relationships between four aspects of government emergency public information and protective behaviors. These government measures could strengthen individuals’ protective actions by increasing perceived efficacy, that is, their confidence in defeating the pandemic.
Second, positive emotions, including gratitude and hope, mediated the relationships of positive risk communication and rumor refutation with protective behaviors. The positive risk communication about frontline medical staff risking their lives to rescue patients filled people with gratitude and hope and increased their sense of social responsibility to comply with protective behaviors (Vaughan and Tinker 2009). Rumor refutation may decrease the level of public anxiety in uncertain situations, increase trust in the government, and promote proper anti‐pandemic behaviors (Greenhill and Oppenheim 2017). In addition, positive emotions may promote protective behaviors by enhancing individuals’ perceived efficacy. An interpretation of this may be that gratitude and hope increases one's resilience to perceive greater control over the crisis and stress (Abolghasemi and Varaniyab 2010; Emmons and Stern 2013; Ong, Edwards, and Bergeman 2006).
Third, risk perception played a mediating role in the prediction of protective behaviors from detailed pandemic information, which is consistent with previous research (Driedger, Michelle, and Jardine 2018; Siegrist and Zingg 2014). In the current study, the government information, including both statistical information on the overall outbreak and detailed information on the trajectory of confirmed cases, promoted individual protective behaviors. Overall, information made individuals aware of the severity of the pandemic, and detailed information strengthened individuals’ risk assessments. They both contributed to promote individual protective behaviors. Rumor refutation and supplies did not show significant negative effect on risk perception, possibly indicating that people had not let their guard down about the pandemic.
The current study has several limits and future directions. First, the sample in the current study is not representative of all demographic categories. A large number of participants were young college students with a bachelor's degree or higher, although age and education had no significant effects on protective behaviors. Thus, the applicability of the findings to other samples needs to be further explored. Second, previous studies have found that people's perceptions of authorities are different across countries and are correlated with their protective actions to pandemic (Wei et al. 2018). All participants in the current study were from China; a cross‐country comparative study is needed to expand the applicability of the current findings. Third, Cronbach's alpha coefficients for detailed pandemic information, perceived efficacy, and protective behaviors have acceptable reliabilities rather than good reliabilities in the present study, which may be caused by the limited number of items or the omission of important items (e.g., hand washing as an important protective behavior item). Future research should adopt questionnaire with more items or adding important items to improve their reliabilities.
Conclusion
To combat the COVID‐19 pandemic effectively, governments should take effective measures in combination with governmental and individual factors. First, governments are encouraged to prioritize improving the implementation of detailed pandemic information and the dissemination of positive risk communication to the public and to put forth effort to refute rumors and increase supplies. Second, individuals are encouraged to increase their perceived efficacy, positive emotions, and risk perception through government emergency public information to comply with anti‐pandemic behaviors. Lastly, it is highly recommended to intervene public behaviors from both governmental and individual levels to maximize the effect of intervention.
Funding
This study was supported by grants from the National Natural Science Foundation of China (31571161 and 31500872), CAS Key Laboratory of Behavioral Science, Institute of Psychology (Y5CX052003), the Humanities and Social Science Research of the Ministry of Education of China (18YJC190002), the National Natural Science Foundation of China (71722004, 71572123), Tianjin Municipal Science and Technology Commission (17ZLZDZF00440), Tianjin Urban and Rural Construction Commission (2018‐soft10), and a CAS‐DAAD joint fellowship.
Acknowledgments
We thank all the participants for their commitment in the present study. We particularly thank Lux Li for his kindly help with proofreading and thank both reviewers for helping us improve the quality and clarity of our manuscripts.
Biographies
Bibing Dai is associate professor of psychology in the Department of Psychiatry and Psychology, School of Basic Medical Sciences, Tianjin Medical University. His research studies mental health and behavioral public administration, with an emphasis on psychological crisis management for societies, populations, groups, and individuals.
Email: daibibing@tmu.edu.cn
Di Fu holds a PhD in cognitive neuroscience from the Institute of Psychology, Chinese Academy of Sciences. Her research studies social decision‐making, empathy, and cognitive control.
Email: fud@psych.ac.cn
Guangteng Meng is a master's degree student in general psychology in the Institute of Psychology, Chinese Academy of Sciences. His research studies social decision‐making and empathy.
Email: menggt@psych.ac.cn
Bingsheng Liu is professor in the School of Public Affairs at Chongqing University, China. His research interests include public management, land acquisition, and group decision‐making.
Email: bluesea_boy_1979@163.com
Qi Li is associate professor of psychology in the Institute of Psychology, Chinese Academy of Sciences. Her research focuses on prosocial decision‐making, social public security, and psychological crisis management for societies, groups, and individuals. This research employs questionnaire, behavioral, EEG, and fMRI methods.
Email: liqi@psych.ac.cn
Xun Liu is full professor of cognitive neuroscience in the Institute of Psychology, Chinese Academy of Sciences. His research interests include empathy and social decision‐making, cognitive control, and conflict processing.
Email: liux@psych.ac.cn
References
- Abolghasemi, A. , and Taklavi Varaniyab S.. 2010. Resilience and Perceived Stress: Predictors of Life Satisfaction in the Students of Success and Failure. Procedia Social and Behavioral Sciences 5: 748–52. 10.1016/j.sbspro.2010.07.178. [DOI] [Google Scholar]
- Allen, Kerry . 2020. Coronavirus: Cement Mixers Become Celebrities in China Lockdown. BBC News, January 31. https://www.bbc.com/news/world‐asia‐china‐51315238 [accessed May 27, 2020].
- Balkhy, Hanan H. , Abolfotouh Mostafa A., Al‐Hathlool Rawabi H., and Al‐Jumah Mohammad A.. 2010. Awareness, Attitudes, and Practices Related to the Swine Influenza Pandemic among the Saudi Public. BMC Infectious Diseases 10: 42. 10.1186/1471-2334-10-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnett, Daniel J. , Thompson Carol B., Semon Natalie L., Errett Nicole A., Harrison Krista L., Anderson Marilyn K., Ferrell Justin L., et al. 2014. EPPM and Willingness to Respond: The Role of Risk and Efficacy Communication in Strengthening Public Health Emergency Response Systems. Health Communication 29(6): 598–609. 10.1080/10410236.2013.785474. [DOI] [PubMed] [Google Scholar]
- Barrelet, Clara , Bourrier Mathilde, Burton‐Jeangros Claudine, and Schindler Melinee. 2013. Unresolved Issues in Risk Communication Research: The Case of the H1N1 Pandemic (2009–2011). Influenza and Other Respiratory Viruses 7(Supplement 2): 114–9. 10.1111/irv.12090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bayham, Jude , Kuminoff Nicolai V., Gunn Quentin, and Fenichel Eli P.. 2015. Measured Voluntary Avoidance Behaviour during the 2009 A/H1N1 Epidemic. Proceedings of the Royal Society B: Biological Sciences 282(1818): 20150814. 10.1098/rspb.2015.0814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bish, Alison , and Michie Susan. 2010. Demographic and Attitudinal Determinants of Protective Behaviours during a Pandemic: A Review. British Journal of Health Psychology 15(Pt. 4): 797–824. 10.1348/135910710X485826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daily China. 2020. Report: China's Fight against COVID‐19. April 21. https://covid‐19.chinadaily.com.cn/a/202004/21/WS5e9e2c62a3105d50a3d17880.html [accessed May 27, 2020].
- Chon, Myoung‐Gi , and Park Hyojung. 2019. Predicting Public Support for Government Actions in a Public Health Crisis: Testing Fear, Organization‐Public Relationship, and Behavioral Intention in the Framework of the Situational Theory of Problem Solving. Health Communication. Published online December 9. 10.1080/10410236.2019.1700439. [DOI] [PubMed]
- Cohen, Jacob , Cohen Patricia, West Stephen G., and Aiken Leona S.. 2003. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, 3rd ed. New York: Routledge. [Google Scholar]
- de Zwart, Onno , Veldhuijzen Irene K., Richardus Jan Hendrik, and Brug Johannes. 2010. Monitoring of Risk Perceptions and Correlates of Precautionary Behaviour Related to Human Avian Influenza during 2006–2007 in The Netherlands: Results of Seven Consecutive Surveys. BMC Infectious Diseases 10: 114. 10.1186/1471-2334-10-114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiFonzo, Nicholas , and Bordia Prashant. 2007. Rumors Influence: Toward a Dynamic Social Impact Theory of Rumor. In The Science of Social Influence: Advances and Future Progress, edited by Pratkanis Anthony R., 271–95. Philadelphia: Psychology Press. [Google Scholar]
- Dredze, Mark , Broniatowski David A., and Hilyard Karen M.. 2016. Zika Vaccine Misconceptions: A Social Media Analysis. Vaccine 34(30): 3441–2. 10.1016/j.vaccine.2016.05.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Driedger, S. Michelle, Ryan Maier , and Jardine Cindy. 2018. “Damned If You Do, and Damned If You Don't”: Communicating about Uncertainty and Evolving Science during the H1N1 Influenza Pandemic. Journal of Risk Research. Published online April 29. 10.1080/13669877.2018.1459793. [DOI] [Google Scholar]
- Emmons, Robert A. , and Stern Robin. 2013. Gratitude as a Psychotherapeutic Intervention. Journal of Clinical Psychology 69(8): 846–55. 10.1002/jclp.22020. [DOI] [PubMed] [Google Scholar]
- Fewtrell, Lorna , and Bartram Jamie, eds. 2001. Water Quality: Guidelines, Standards and Health: Assessment of Risk and Risk Management for Water‐Related Infectious Diseases. Geneva: World Health Organization. https://apps.who.int/iris/handle/10665/42442. [Google Scholar]
- Folkman, Susan , and Moskowitz Judith Tedlie. 2016. Stress, Positive Emotion, and Coping. Current Directions in Psychological Science 9(4): 115–8. 10.1111/1467-8721.00073. [DOI] [Google Scholar]
- Fredrickson, Barbara L. , Tugade Michele M., Waugh Christian E., and Larkin Gregory R.. 2003. What Good Are Positive Emotions in Crisis? A Prospective Study of Resilience and Emotions Following the Terrorist Attacks on the United States on September 11th, 2001. Journal of Personality and Social Psychology 84(2): 365–76. 10.1037/0022-3514.84.2.365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- French, P. Edward . 2011. Enhancing the Legitimacy of Local Government Pandemic Influenza Planning through Transparency and Public Engagement. Public Administration Review 71(2): 253–64. [Google Scholar]
- Greenhill, Kelly M. , and Oppenheim Ben. 2017. Rumor Has It: The Adoption of Unverified Information in Conflict Zones. International Studies Quarterly 61(3): 660–76. 10.1093/isq/sqx015. [DOI] [Google Scholar]
- Hagan, Patrick , Maguire Brigit, and Bopping Derek. 2008. Public Behaviour during a Pandemic. Australian Journal of Emergency Management 23(3): 35–40. [Google Scholar]
- Hew, Jun‐Jie , Lai‐Ying Leong, Wei‐Han Tan Garry, Voon‐Hsien Lee, and Keng‐Boon Ooi. 2018. Mobile Social Tourism Shopping: A Dual‐Stage Analysis of a Multi‐mediation Model. Tourism Management 66: 121–39. [Google Scholar]
- Jones, James Holland , and Salathe Marcel. 2009. Early Assessment of Anxiety and Behavioral Response to Novel Swine‐Origin Influenza A(H1N1). PLOS ONE 4(12): e8032. 10.1371/journal.pone.0008032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kass, Nancy , Hecht Kenneth, Paul Amy, and Birnbach Kerry. 2014. Ethics and Obesity Prevention: Ethical Considerations in 3 Approaches to Reducing Consumption of Sugar‐Sweetened Beverages. American Journal of Infection Control 104(5): 787–95. 10.2105/AJPH.2013.301708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim, Hye Kyung , and Niederdeppe Jeff. 2013. The Role of Emotional Response during an H1N1 Influenza Pandemic on a College Campus. Journal of Public Relations Research 25(1): 30–50. 10.1080/1062726x.2013.739100. [DOI] [Google Scholar]
- Kim, Yushim , Zhong Wei, Jehn Megan, and Walsh Lauren. 2015. Public Risk Perceptions and Preventive Behaviors during the 2009 H1N1 Influenza Pandemic. Disaster Medicine and Public Health Preparedness 9(2): 145–54. 10.1017/dmp.2014.87. [DOI] [PubMed] [Google Scholar]
- Lamunu, M. , Lutwama J.J., Kamugisha J., Opio A., Nambooze J., Ndayimirije N., and Okware S.. 2004. Containing a Haemorrhagic Fever Epidemic: The Ebola Experience in Uganda (October 2000–January 2001). International Journal of Infectious Diseases 8(1): 27–37. 10.1016/j.ijid.2003.04.001. [DOI] [PubMed] [Google Scholar]
- Lau, Joseph T.F. , Yang Xilin, Tsui H.Y., and Pang Ellie. 2004. SARS Related Preventive and Risk Behaviours Practised by Hong Kong‐Mainland China Cross Border Travellers during the Outbreak of the SARS Epidemic in Hong Kong. Journal of Epidemiology and Community Health 58(12): 988–96. 10.1136/jech.2003.017483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, Hao , Chen Xinguang, and Huang Hao. 2020. The Novel Coronavirus Outbreak: What Can be Learned from China in Public Reporting? Global Health Research and Policy 5: 9. 10.1186/s41256-020-00140-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindell, Michael K. 2018. Communicating Imminent Risk. In Handbook of Disaster Research, 2nd ed., edited by Rodriguez Havidán, Donner William, and Trainor Joseph E., 449–77. New York: Springer. [Google Scholar]
- Lindell, Michael K. , and Perry Ronald W.. 2012. The Protective Action Decision Model: Theoretical Modifications and Additional Evidence. Risk Analysis 32(4): 616–32. 10.1111/j.1539-6924.2011.01647.x. [DOI] [PubMed] [Google Scholar]
- Lo, Ven‐hwei , Wei Ran, and Herng Su.. 2013. Self‐Efficacy, Information‐Processing Strategies, and Acquisition of Health Knowledge. Asian Journal of Communication 23(1): 54–67. 10.1080/01292986.2012.725175. [DOI] [Google Scholar]
- Mackinnon, David P. , Lockwood Chondra M., and Williams Jason. 2004. Confidence Limits for the Indirect Effect: Distribution of the Product and Resampling Methods. Multivariate Behavioral Research 39(1): 99–128. 10.1207/s15327906mbr3901_4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moon, M. Jae . 2020. Fighting COVID‐19 with Agility, Transparency, and Participants: Wicked Policy Problems and New Governance Challenges. Public Administration Review 80(4): 651–56. 10.1111/puar.13214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moran, Kelly R. , and Del Valle Sara Y.. 2016. A Meta‐analysis of the Association between Gender and Protective Behaviors in Response to Respiratory Epidemics and Pandemics. PLOS ONE 11(10): e0164541. 10.1371/journal.pone.0164541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ong, Anthony D. , Edwards Lisa M., and Bergeman C.S.. 2006. Hope as a Source of Resilience in Later Adulthood. Personality and Individual Differences 41(7): 1263–73. 10.1016/j.paid.2006.03.028. [DOI] [Google Scholar]
- Paek, Hye‐Jin , Hilyard Karen, Freimuth Vicki S., Kevin Barge J., and Mindlin Michele. 2008. Public Support for Government Actions during a Flu Pandemic: Lessons Learned from a Statewide Survey. Health Promotion Practice 9(Supplement 4): 60S–72S. 10.1177/1524839908322114. [DOI] [PubMed] [Google Scholar]
- Prati, Gabriele , Pietrantoni Luca, and Zani Bruna. 2011. A Social‐Cognitive Model of Pandemic Influenza H1N1 Risk Perception and Recommended Behaviors in Italy. Risk Analysis 31(4): 645–56. 10.1111/j.1539-6924.2010.01529.x. [DOI] [PubMed] [Google Scholar]
- Qazi, Atika , Qazi Javaria, Naseer Khulla, Zeeshan Muhammad, Hardaker Glenn, Maitama Jaafar Zubairu, and Haruna Khalid. 2020. Analyzing Situational Awareness through Public Opinion to Predict Adoption of Social Distancing amid Pandemic Covid‐19. Journal of Medical Virology. Published online April 8. 10.1002/jmv.25840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rippetoe, Patricia A. , and Rogers Ronald W.. 1987. Effects of Components of Protection‐Motivation Theory on Adaptive and Maladaptive Coping with a Health Threat. Journal of Personality and Social Psychology 52(3): 596–604. 10.1037//0022-3514.52.3.596. [DOI] [PubMed] [Google Scholar]
- Rubin, G. James , Amlot Richard, Page Lisa, and Wessely Simon. 2009. Public Perceptions, Anxiety, and Behaviour Change in Relation to the Swine Flu Outbreak: Cross Sectional Telephone Survey. BMJ 339: b2651. 10.1136/bmj.b2651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seale, Holly , McLaws Mary‐Louise, Heywood Anita E., Ward Kirsten F., Lowbridge Chris P., Van Debbie, Gralton Jan, and MacIntyre C. Raina. 2009. The Community's Attitude Towards Swine Flu and Pandemic Influenza. Medical Journal of Australia 191(5): 267–9. 10.5694/j.1326-5377.2009.tb02781.x. [DOI] [PubMed] [Google Scholar]
- Sharma, Megha , Yadav Kapil, Yadav Nitika, and Ferdinand Keith C.. 2017. Zika Virus Pandemic‐Analysis of Facebook as a Social Media Health Information Platform. American Journal of Infection Control 45(3): 301–2. 10.1016/j.ajic.2016.08.022. [DOI] [PubMed] [Google Scholar]
- Siegrist, Michael , and Zingg Alexandra. 2014. The Role of Public Trust during Pandemics. European Psychologist 19(1): 23–32. 10.1027/1016-9040/a000169. [DOI] [Google Scholar]
- Stockmann, Daniela , and Gallagher Mary E.. 2011. Remote Control: How the Media Sustain Authoritarian Rule in China. Comparative Political Studies 44(4): 436–67. 10.1177/0010414010394773. [DOI] [Google Scholar]
- van Gelder, N. , Peterman A., Potts A., O'Donnell M., Thompson K., Shah N., and Oertelt‐Prigione S.. 2020. Covid‐19: Reducing the Risk of Infection Might Increase the Risk of Intimate Partner Violence. EClinical Medicine 94(1): 1–9. 10.1016/j.eclinm.2020.100348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vaughan, Elaine , and Tinker Timothy. 2009. Effective Health Risk Communication about Pandemic Influenza for Vulnerable Populations. American Journal of Infection Control 99(Supplement 2): S324–32. 10.2105/AJPH.2009.162537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker, Naomi F. , and Whitty Christopher J.M.. 2015. Tackling Emerging Infections: Clinical and Public Health Lessons from the West African Ebola Virus Disease Outbreak, 2014–2015. Clinical Medicine 15(5): 457–60. 10.7861/clinmedicine.15-5-457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wei, Hung‐Lung , Lindell Michael K., Prater Carla S., Wei Jiuchang, Wang Fei, and Ge Yue Gurt. 2018. Perceived Stakeholder Characteristics and Protective Action for Influenza Emergencies: A Comparative Study of Respondents in the United States and China. International Journal of Mass Emergencies and Disasters 36(1): 52–70. [Google Scholar]
- World Health Organization (WHO) . 2015. The WHO Model List of Essential Medicines, 19th ed. Geneva: World Health Organization. [Google Scholar]
- World Health Organization (WHO) Ebola Response Team . 2014. Ebola Virus Disease in West Africa—The First 9 Months of the Epidemic and Forward Projections. New England Journal of Medicine 371(16): 1481–995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wong, Chi‐Yan , and Tang Catherine So‐Kum. 2005. Practice of Habitual and Volitional Health Behaviors to Prevent Severe Acute Respiratory Syndrome among Chinese Adolescents in Hong Kong. Journal of Adolescent Health 36(3): 193–200. 10.1016/j.jadohealth.2004.02.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Xu, Bo , Gutierrez Bernardo, Mekaru Sumiko, Sewalk Kara, Goodwin Lauren, Loskill Alyssa, Cohn Emily L., et al. 2020. Epidemiological Data from the Covid‐19 Outbreak, Real‐Time Case Information. Scientific Data 7(1): 106. 10.1038/s41597-020-0448-0. [DOI] [PMC free article] [PubMed] [Google Scholar]