

Abstract
Background
Immunization is the process by which a person is made immune or resistant to an infectious disease, typically by the administration of vaccine. Vaccination coverage for other single vaccines ranged from 49.1% for PCV to 69.2% for BCG vaccine. The vaccination coverage for basic vaccinations was 39.7% in Ethiopia. There have been epidemiological studies available on immunization in Ethiopia. Yet, these studies revealed a wide variation over time and across geographical areas. This systematic review and Meta-analysis aim to estimate the overall immunization coverage among 12–23 months children in Ethiopia.
Methods
Cross-sectional studies that reported on immunization coverage from 2003 to August 2019 were systematically searched. Searches were conducted using PubMed, Google Scholar, Cochrane library, and gray literature. Information was extracted using a standardized form of Joanna Briggs Institute. The search was updated 20 Jan 2020 to decrease time-lag bias. The quality of studies assessed using Joanna Briggs Institute cross-sectional study quality assessment criteria. I-squared statistics applied to check the heterogeneity of studies. A funnel plot, Begg’s test, and Egger’s regression test was used to check for publication bias.
Results
Out of 206 studies, 30 studies with 21,672 children with mothers were included in the Meta-analysis. The pooled full immunization coverage using the random-effect model in Ethiopia was 58.92% (95% CI: 51.26–66.58%). The trend of immunization coverage was improved from time to time, but there were great disparities among different regions. Amhara region had the highest pooled fully immunized coverage, 72.48 (95%CI: 62.81–82.16). The I2 statistics was I2 = 99.4% (p = 0.0001). A subgroup meta-analysis showed that region and study years were not the sources of heterogeneity.
Conclusion
This review showed that full immunization coverage in Ethiopia was 58.92% (95% CI: 51.26–66.58%). The study suggests that the child routine immunization program needs to discuss this low immunization coverage and the current practice needs revision.
Keywords: Immunization-coverage, Vaccine, Children, Ethiopia, Systematic review, And meta-analysis
Background
Immunization is the process by which a person is made immune or resistant to an infectious disease, typically by the administration of a vaccine. A vaccine is a non-pathogenic antigen that stimulates the body’s immune system to produce an antibody to protect the person against later infection. It is the most cost-effective public health intervention that can control and end life-threatening infectious disease [1, 2].
Vaccination has lowered the burden of infectious diseases since the start of the Expanded Program on Immunization (EPI) by the World Health Organization (WHO) in 1974, reducing mortality, morbidity, and saving resources [3–6]. WHO has estimated that 29% of under-five deaths could be prevented with existing vaccines, averting between 2 to 3 million deaths each year globally [7]. Worldwide immunization coverage showed improvement in the past years; however, the validity of the data for measuring change over time has been questioned [8]. Therefore, accurate immunization information is essential for decision-makers of the Expanded Program on Immunization (EPI) to track and improve performance [9].
The Expanded Programmed for Immunization (EPI) in Ethiopia, launched in 1980, has been one of the core priorities in the past Health Sector Development Programmes (HSDPs) and the current Health Sector Transformation Plan (HSTP). The country has mobilized women’s development armies or volunteers, health extension workers, and health facilities to deliver its immunization services. Improved district planning and management were started in 2011 to reach every district. Stationary, outreach, and mobile are the three important services delivery platforms for vaccination. The aim of launching this program was to increase the coverage of immunization by 10% annually. However, the coverage in the first 20 years was very low, although during the 1990s good progress was observed through Universal Child Immunization (UCI). Reaching every district approach has been implemented in Ethiopia, since, 2004 in districts with poor immunization coverage and high dropout rates. As a result, the coverage showed marked improvement, but there was a variation in coverage among regions. Now, reaching every district strategic approach is recast to reaching every child/community strategic approach to deal with inequities within districts [10].
Ethiopia’s national coverage of the third dose of the pentavalent, combined diphtheria, pertussis, tetanus, hepatitis B, and Haemophilus influenza type B, vaccine (Penta) at 12–23 months of age is 37%; and the dropout rate between the first and third doses of this vaccine was reported as 43% in 2013 [11].
The routine immunization coverage in Ethiopia has never reached the targeted figures and planned goals. Sustainable improvements in service delivery is needed to protect Ethiopian children from unnecessary suffering and deaths [12]. Similarly, according to the EDHS 2011 report, the coverage of EPI in Somali Region was low, and it showed that only 16.6% of them were fully immunized while 35.4% were unimmunized. These figures are two times lower than similar figures from other regions [13]. The main reasons behind this very low coverage where include a pastoral lifestyle and programmatic level to infrastructure conditions of the region, little commitment at all levels, lack of resource allocation, personnel and shortage of functional health facilities were also mentioned [2]. Complete immunization coverage was 38.5% at the national level and 45.8% in the Amhara region [14, 15].
In the search for effective ways to discuss low and stagnating vaccination rates and improve access to and utilization of immunization services, increased attention is being paid to the role of communities and community engagement strategy [16]. It is argued that communities should not be viewed as passive recipients of immunization services; rather, they need to be actively involved in shaping vaccination program [17].
Objective and research question
The aim of this systemic review is synthesis and pooled level of full immunization coverage and its determinate factors among 12–23 months of children in Ethiopia. The research question is what is the level of full immunization coverage in Ethiopia?
Methods
Study settings
Ethiopia is one of the east African countries in the Horn of Africa. It covers an area of 1.104 million km2 and divided into 9 regions namely Tigray, Afar, Amhara, Oromia, Somali, Benishangul-Gumuz, Southern Nations Nationalities and People Region (SNNPR), Gambella, Harari, and two Administrative states (Addis Ababa city administration and Dire Dawa city administration).
Criteria for considering studies for the review
Inclusion criteria
Selection of studies
Cross-sectional studies were extracted and two reviewers (SS, AE) employed the predetermined inclusion criteria to screen for relevant full-text cross-sectional studies. Both reviewers were blinded to journal, authors, and results. There were no conflicts between the two reviewers in last choice decisions. Studies were included for data extraction and analyses.
Inclusion criteria
Articles were included in this systematic review if they fulfilled the following criteria, study type: full-text cross-sectional articles written in English which have been published (since 2003) in peer-reviewed journals, primary journals, be on human subjects and 12–23 months age group.
Type of studies
All published cross-sectional studies including government reports related to the coverage of immunization status was included.
Study participants
Mothers/ caretakers with children aged 12–23 months, and in which immunization status was reported by card and mother recalled method.
Exclusion criteria
Citations without abstracts and/or full text, commentaries, anonymous reports, letters, duplicate studies were excluded.
Search strategy and information sources
The database search had been structured using CoCoPop, where, Context (Ethiopia), condition (immunization coverage), Population (children aged 12–23 months). Notably, to fit the advanced PubMed database, the following search strategy applied: (Immunization OR Vaccination OR “Immunization Coverage” OR “Vaccination Coverage”) AND (Children OR “children aged 12-23 months”) AND (Determinant OR Determinants OR “Determinant factor” OR “Determinant factors” OR Factor OR Factors OR “Associated factor” OR “Associated factors”) AND (Ethiopia) AND full text [sb] AND (“2000/01/01”[PDat]: “2019/12/31”[PDat]) AND Humans [Mesh]. The presence of precursor systematic review and/or protocol on the topic of interest was checked on Cochrane database of a systematic review and Joanna Briggs Institute database of a systematic review. But, PROSPERO registration was not done.
An electronic database searches time was conducted using PubMed, Google Scholar, and Cochrane library and research gate from April 2019 to August 2019. To reduce time-lag bias, the search process was updated on 20 Jan 2020. The search focused on all published studies with epidemiological data of immunization coverage among children aged 12–23 months of children in Ethiopia. To find the relevant article, titles and abstracts of retrieved papers were exported to Endnote where duplicates were identified and removed by one investigator (SH). Full texts of peer-reviewed relevant articles were retrieved, assessed and their reference lists were hand-searched to show further relevant studies.
Quality assessment tool
Retrieved studies were exported to endnote version 7 to remove duplicate studies. A search strategy was done by two of the investigators (SS and AE). Both the reviewers were blinded to journal, authors, and results. There were no conflicts between the two reviewers in final choice decisions. The selections of identified studies were done in two stages. In the first stage, a selection of relevant studies based on titles and abstracts. In the second stage, studies that met the inclusion criteria and the full paper found for detailed assessment based on the inclusion criteria were considered.
Two reviewers (SS and AE) performed the study eligibility assessment independently by using JBI checklists. A critical appraisal checklist for cross-sectional studies adopted by JBI and used to assess the overall methodological quality and evaluated the risk of bias (additional file 1). The methodological components assessed include: addressing the target population; data was extracted from the included cross-sectional studies: outcome measures counted magnitude of immunization coverage, and region, and publication year, Antenatal care, and institutional delivery. These data were then compiled into a standard table (Table 1). The two reviewers (SS, AE), who selected the proper studies also extracted the data and evaluated the risk of bias.
Table 1.
Description of the included studies
| Authors | Study area | Sample size | Measurement of outcome interest | Immunization Coverage of Children aged 12–23 Months | Other Main findings | JBI-Quality score |
|---|---|---|---|---|---|---|
| Animaw et al., 2014 [18] | SNNPR, Arba Minch town and Arba Minch Zuria district | 630 | Card plus mother recall method | 461 (73.2%) were fully immunized | 128 (20.3%) were partially and Vaccinated, and 41 (6.5%) were unvaccinated | 88.9 |
| Facha, 2015 [19] | SNNPR, Arba Minch Zuriya Woreda | 210 | Card plus mother recall method | 112 (53.3%) were fully immunized | 90 (42.9%) were partially vaccinated, and 8 (3.8%) did not take any vaccine | 88.9 |
| Meleko et al., 2017 [20] | SNNR, Mizan Aman town | 322 | Card plus mother recall method | 136 (42.2%) were fully immunized | 159 (49.4%) were partially vaccinated, and 27 (8.4%) were unvaccinated. | 66.7 |
| Tefera et al., 2018 [21] | SNNPR-Worabe, a town | 484 | Card plus mother recall method | 297 (61.4%) were fully vaccinated. | 187 (38.6%) were not fully immunized | 66.7 |
| Ayano, 2015 [22] | SNNPR,Hosanna Town | 508 | Card plus mother recall method | 155 (30.51%) were fully vaccinated | 325 (63.98%) were partially vaccinated, and 28 (5.51) were unvaccinated | 66.7 |
| Fite and Hailu, 2019 [23] | SNNPR Areka Town, Sothern Ethiopia | 172 | Not specified. | 130 (75.6%) are fully vaccinated. | 25 (14.5) were partially vaccinated, and 17 (10.1%) were unvaccinated | 55.6 |
| Hailu et al., 2019 [24] | SNNPR, Wonago district in southern Ethiopia | 1116 | Card plus mother recall method | 585 (52.4%) were fully immunized | 333 (29.8%) were partially immunized, and 158 (14.2%) were not immunized | 100 |
| Michael Mesfin, 2015 [25] | SNNPR, Yirgalem Town | 473 | Card plus mother recall method | 367 (77.8) were fully immunized | 96 (20) were partially immunized, and 10 (2.1%) were not immunized | 77.8 |
| Mohammed et al. 2013 [26] | Oromia, Kombolcha Woreda | 694 | Card plus mother recall method | 159 (22.9%) completely immunized | -Of total 168 (24.2%) not immunized, and 367 (52.9%) partially immunized | 66.7 |
| Legesse and Dechasa, 2015 [27] | Oromia, Sinana district | 591 | Card plus mother recall method | - 454 (76.8%) were fully vaccinated | 122 (20.6%) were partiallyVaccinated, and 15 (2.5%) were unvaccinated. | 88.9 |
| Melese Girmaye, et al. 2019 [28] | Oromia, Wayu-Tuka District | 436 | Card plus mother recall method | Fully vaccination coverage was 73.9% | 109 (25%) were partially vaccinated, and (1.1%) were unvaccinated. | 66.7 |
| Sheka Shimelis, 2018 [29] | Oromia, in Serbo Town | 260 | Card plus mother recall method | 119 (48.8%) were fully immunized | −45.5% (126) were incompletely vaccinated and 5.7% (14) did not take any vaccination. | 88.9 |
| Udessa, 2018 [30] | Oromia, Wadera District | 440 | Card plus recall method | 184 (41.4%) were fully vaccinated | Among the total, 26 (5.9%) of the children were unvaccinated. | 66.7 |
| Etana and Deressa, 2012 [31] | Oromia, Ambo Woreda | 536 | Card plus mother recall method | 191 (35.6%) were fully vaccinated | 218 (40.6) were partially vaccinated, and 127 (23.7%) were unvaccinated. | 88.9 |
| Wado et al., 2014 [32] | Oromia southwestern Ethiopia | 889 | Immunization coverage by card | 329 (37%) were fully vaccinated | 361 (40.6%) were partially vaccinated, and 199 (22.4%) were unvaccinated. | 77.8 |
| Toyeb Yasine, 2015 [33] | Oromia, Tehulederie district | 639 | Immunization coverage by card | 531 (83.1) were fully vaccinated | 94 (14.7%) were partially vaccinated, and 14 (2.2%) were unvaccinated. | 77.8 |
| Kassahun et al., 2015 [34] | Amhar, Lay Armachiho District | 751 | Card plus mother recall method | 571 (76.03%) were fully vaccinated | 21.67 were partially vaccinated, and (2.3) not vaccinated at all | 88.9 |
| Gualu and Dilie, 2017 [35] | Amhara, Debre Markos Town | 288 | Not specified | 264 (91.7%) were fully vaccinated | 19 (6.6%) were partially vaccinated, and 5 (1.7%) were not vaccinated at all. | 55.6 |
| Mastewal Worku Lake et al., 2016 [36] | Amhara, Dessie Town,South Wollo Zone | 724 | Card plus mother recall method | 472 (65.2%) were fully vaccinated | 130 (17.9%) were partially vaccinated, and 252 (34.8%) never get vaccine | 77.8 |
| Ayal D, 2014 [37] | Amhara, Mecha district | 497 | Card plus mother recall method | 245 (49.3%) were fully vaccinated | 244 (49.1%) were partially vaccinated, and 8 (1.6%) have never been vaccinated. | 66.7 |
| Abebe et al., 2019 [38] | Amhara, Woldia Town | 389 | Card plus mother recall method | 343 (87.7%) children were fully immunized | 46 (11.8%) were partially vaccinated | 66.7 |
| Tadesse daget, 2018 [39] | Amhara, Bahirdar town | 846 | Card plus mother recall method | 494 (58.4%) were fully vaccinated | 144 (17%)were partially vaccinated and 208 (24.6%) were not vaccinated at all | 88.9 |
| Mekonnen et al., 2019 [40] | Minjar-Shenkora district | 566 | mother’s/caregivers’ report | 428 (75.6%) were fully vaccinated | 105 (18.5%) were partially vaccinated, and 33 (5.9%) were not vaccinated at all | 88.9 |
| Ayenew Engida, 2019 [41] | Amhara, Gondar city administration | 301 | Card plus mother recall method | 228 (75.7) were fully vaccinated | 73 (24.3%) were partially vaccinated | 77.8 |
| Girmay and Dadi, 2019 [42] | Tigria, Sekota Zuria district. | 620 | Card plus mother recall method | 480 (77.4%) of them were fully immunized | 15.5% (96/620) were partially immunized, and 44 (7.1%) did not received vaccin | 77.8 |
| Teklay Kidane, 2004 [43] | Tigria regional State | 110 | Card plus mother recall method | 83 (75.5%) were fully vaccinated | 27 (24.5%) were partially immunized | 77.8 |
| Mohamud et al., 2014 [44] | Somali National Regional State | 582 | Card plus mother recall method | 213 (36.6%) were fully vaccinated | 221 (37.9) were partially vaccinated, and 148 (25.4%) not vaccinated at all | 88.9 |
| Yihunie Lakew, 2015 [45] | National survey | 1927 | Card plus mother recall method | 468 (24.3%) were fully vaccinated | 1170 (60.7%) were partially vaccinated, and 289 (15%) were not vaccinated at all | 77.8 |
| Koku Sisay, 2019 [46] | National survey | 1909 | Card plus mother recall method | 38.3% are fully vaccinated | 61.7% were partially vaccinated. | 88.9 |
| Abebech Asmamaw, 2016 [47] | National survey | 4983 | Card plus mother recall method | 1296 (26%) are fully vaccinated | – | 88.9 |
Data extraction
A standardized data extraction form of JBI was used to extract the necessary data. The data extraction tool was piloted by considering the inclusion criteria to check consistency and to make sure that all the relevant information was captured. The extraction tool includes the title of the study, the first author’s name, and year of publication, study area (region) and all other important information. During the extraction process, data discrepancy among data extractors was resolved by referring back to the original study.
The third reviewer (SH) negotiated any discrepancy between the two authors. In other words, the papers were given to the third reviewer for consensus while a discrepancy in the decision process. The screening and selection process of the reviewed articles was summarized using the PRISMA flow chart (Fig. 1 [48]).
Fig. 1.

The PRISMA flow diagram of identification and selection of studies for the systematic review and meta-analysis
Outcome measures (fully immunizations/ immunization coverage)
Fully immunization coverage was the primary interest of this review, which was measured if the child took all recommended vaccines according to the Ethiopian EPI schedule. According to the WHO guideline “complete or full immunization” coverage is defined as a child has received a BCG vaccine, three doses of penta vaccine such as diphtheria, pertussis, tetanus, hepatitis B and Haemophilus influenza type B; at least three doses of polio vaccine, 3 doses of PCV vaccine, 2 doses of Rota vaccine and one dose of measles vaccine. It was assessed by vaccination card plus mothers recall [49].
Data synthesis and statistical analysis
Data was analyzed using the ‘meta’ packages of the Stata software (version 11.0). Unadjusted prevalence was recalculated based on crude numerators and denominators provided by each study and joined to calculate the pooled estimates. The quantitative data synthesis method was used to present extracted data from each study. Heterogeneity among the studies was evaluated using the χ2 test on Cochrane’s Q statistic [50], and I-square estimate greater than 75% was considered as indicative of moderate to high levels of heterogeneity [51]. Subgroup analysis was done to explore differences in outcomes according to a study area, study region, publication year. The funnel plot and Egger’s test were used to check the presence of publication bias [52]. A p-value < 0.05 on the Egger test was considered indicative of publication bias.
Results
Description of the included studies
The search strategy retrieved 206 studies from PubMed, Cochrane library, Google Scholar and gray literature. About 102 articles were excluded because of duplication matters and studies out of Ethiopia. After removing duplicates, a total of 74 articles were removed by reading title and abstract of the studies. Finally, 30 studies were screened for full-text review and used for quantitative analysis (Fig. 1).
Characteristics of included studies
Full-text cross-sectional articles written in English and published from 2003 to 2019 years were studied in a different part of Ethiopia. Of 30 studies, eight of them were done in Amhara region, eight in the Southern Nation Nationality People Region (SNNPR), eight in Oromia region, two in Tigray, three studies at national level study, and one in Somali National Regional State. In the included studies, the sample sizes were ranges from 172 to 3762. A total of 21,562 children aged 12–23 months were included in all studies. A summary of all relevant features and main findings of the including studies were presented in (Table 1).
Fully immunization coverage among children 12–23 months in Ethiopia
In the included studies, full immunization coverage ranges from 22.9% [26] to 91.7% [35]. Among the total reviewed studies, in fifteenth studies, full immunization coverage was dominantly reported within the ranges of 22.9 to 58.4%. In 12, included individual studies, most children were fully immunized that reported within the range from 61.4 to 77.8%. In three, included studies, full immunization coverage was high which accounts for 87.7 to 91.7% (Table 1).
Partial-immunization coverage among children 12–23 months in Ethiopia
Partial immunizations were reported by 26 studies. The magnitude of partial immunization ranges from 63.98% at SNNPR, hosanna town to 6.6% at Amhara region, Debre Markos Town (Table 1).
Non-immunization coverage among children 12–23 months in Ethiopia
No immunizations were reported by 24 studies. The magnitude of never immunized children was range from 34.8% at Amhara Region, Dessie Town to (1.1%) at Oromia region, Wayu-Tuka District (Table 1).
Meta-analysis results
The drive of this meta-analysis was to estimate the pooled level fully immunization coverage among children 12–23 months in Ethiopia, by using proportions. A total of 30 studies met the inclusion criteria for meta-analysis.
Fully immunization coverage among children 12–23 months in Ethiopia
A total of 30 studies were included in this meta-analysis. The estimated overall pooled proportion of fully immunized children in Ethiopia were 58.92, (95%CI: 51.26–66.58) (Fig. 2).
Fig. 2.

Proportion of fully immunization coverage among children 12–23 months in Ethiopia from 2003 to 2019
In the regional subgroup analysis, Amhara region had the highest proportion of fully immunized children at 72.48(95%CI: 62.81–82.16), followed by SNNPR 58.30(46.42–70.18) and Oromia region 52.50 (95%CI; 35.08–69.91). The highest proportion of pooled fully immunization coverage was observed in the year 2019, 68.50, (95% CI: 59.17–77.83), but almost similar in the year 2016, 61.27, (95%CL: 41.43–81.08) and 2018, 62.39, (95% CL: 43.38–81.39) (Table 2 and Fig. 3).
Table 2.
Immunization coverage in Ethiopia among children age 12–23 months in Ethiopia from 2003 to 2019
| Variables | Coverage% (95% CI) | Heterogeneity | No. studies |
|---|---|---|---|
| Immunization coverage | |||
| Full immunization | 58.92 (51.26–66.58) | I2 = 99.4%, p = 0.000 | 30 |
| Partial immunization | 30.80 (23.91–37.65) | I2 = 99.1%, p = 0.000 | 25 |
| Non-immunization | 12.87 (9.77–15.96) | I2 = 98.5%, p = 0.000 | 24 |
| Regional status | |||
| Oromia region | 52.50 (35.08–69.91) | I2 = 99.4%, p = 0.000 | 8 |
| Amhara region | 72.48 (62.81–82.16) | I2 = 98.3%, p = 0.000 | 8 |
| SNNPR | 58.30 (46.42–70.18) | I2 = 98.4%, p = 0.000 | 8 |
| National level study | 37.54 (21.99–53.09) | I2 = 99.5%, p = 0.000 | 3 |
| Complete/full / Immunization | |||
| 2011 | 36.12 (33.30–38.93) | I2 = 0.001%, p = 0.728 | 2 |
| 2013 | 56.55 (28.16–84.94) | I2 = 99.6%, p = 0.000 | 4 |
| 2014 | 54.12 (29.03–79.21) | I2 = 99.4%, p = 0.000 | 3 |
| 2015 | 53.92 (21.19–86.66) | I2 = 99.8%, p = 0.000 | 4 |
| 2016 | 61.27 (41.43–81.08) | I2 = 99.6%, p = 0.000 | 4 |
| 2018 | 62.39 (43.38–81.39) | I2 = 99.0%, p = 0.000 | 4 |
| 2019 | 68.50 (59.17–77.83) | I2 = 97.3%, p = 0.000 | 7 |
| Partially immunization | |||
| 2011 | 39.21 (36.36–42.07) | I2 = 0.001%, p = 0.343 | 2 |
| 2013 | 31.25 (11.17–51.33) | I2 = 99.1%, p = 0.000 | 3 |
| 2014 | 37.07 (21.04–53.09) | I2 = 98.4%, p = 0.000 | 3 |
| 2015 | 39.84 (13.49–66.19) | I2 = 99.7%, p = 0.000 | 4 |
| 2016 | 12.25 (1.18–23.33) | I2 = 96.7%, p = 0.000 | 2 |
| 2018 | 26.94 (6.98–46.9) | I2 = 99.1%, p = 0.000 | 3 |
| 2019 | 24.51 (16.96–32.09) | I2 = 95.9%, p = 0.000 | 6 |
| Non-immunization | |||
| 2011 | 24.57 (22.04–27.09) | I2 = 0.001%, p = 0.509 | 2 |
| 2013 | 19.45 (7.80–31.10) | I2 = 99.1%, p = 0.000 | 3 |
| 2014 | 8.62 (0.57–16.67) | I2 = 99.0%, p = 0.000 | 3 |
| 2015 | 5.69 (0.09–11.29) | I2 = 98.5%, p = 0.000 | 4 |
| 2016 | 9.26 (5.64–24.15) | I2 = 98.9%, p = 0.000 | 2 |
| 2018 | 23.09 (4.77–41.42) | I2 = 95.9%, p = 0.000 | 3 |
| 2019 | 8.56 (5.02–12.11) | I2 = 90.6%, p = 0.000 | 6 |
Fig. 3.

Trend of immunization coverage among children 12–23 months in Ethiopia from 2003 to 2019
Partial and non-immunization coverage among children 12–23 months in Ethiopia
The pooled proportion of partially immunized children was 31.05% (95% CI: 24.00–38.10). The highest pooled proportion of partial immunization coverage was observed in the year 2015, 39.84 (95%CI; 13.49–66.19), but lower coverage was observed in the year 2019, 24.51, (95%CI; 16.96–32.09) (Table 1). The pooled proportion of non-immunization of children was 12.87(95%CI; 9.77–15.96) (Table 2 and Fig. 3).
Factors associated with fully immunization coverage among children age 12–23 months
In this meta-analysis, urban residence OR:1.75; (95% CI: 1.42–2.17), maternal education OR:2.29;(95% CI:1.19–2.75), ANC follows ups OR: 2.38;(95% CI:2.06–2.76), delivery at health facilities OR:1.87;(95%CI:1.68–2.09), maternal TT vaccination OR:1.40;(95%CI:1.21–1.64), PNC follows OR:1.44;(95%CI:1.14–1.82), knowledge about immunization OR: 3.83;(95%CI: 2.88–5.10), mother knowing the schedule of vaccination OR:2.06;(95%CI:1.56–2.71), attitude towards immunization OR:1.86;(95%CI:1,04–5.33), mother who visited by HEW OR:2.23; (95%CI:1.63–3.04) were significantly associated with full immunization (Table 3).
Table 3.
factors associated with fully immunization coverage among children age 12–23 months in Ethiopia from 2003 to 2019
| Variables | OR, 95% CI | Heterogeneity | Number of studies |
|---|---|---|---|
| Educated mothers | 2.29 (1.19–2.75) | I2 = 68.4, p = 0.004 | 7 |
| Knowledgeable about immunization | 3.83 (2.88–5.10) | I2 = 64.1, p = 0.025 | 5 |
| Mother who had ANC visit | 2.38 (2.06–2.76) | I2 = 71.0, p = 0.0001 | 10 |
| Favorable attitude towards immunization | 1.86 (1,04–5.33) | I2 = 0.0, p = 0.445 | 3 |
| Mother who delivered at health institution | 1.87 (1.68–2.09) | I2 = 57.4, p = 0.002 | 17 |
| Mother who visited by HEW | 2.23 (1.63–3.04) | I2 = 0.0, p = 0.592 | 3 |
| Mother who lived at urban kebeles | 1.75 (1.42–2.17) | I2 = 0.0, p = 0.580 | 5 |
| Mother who taken TT vaccination | 1.40 (1.21–1.64) | I2 = 47.8, p = 0.105 | 5 |
| Mother who had PNC visit | 1.44 (1.14–1.82) | I2 = 46.1, p = 0.116 | 5 |
| Mother knowing the schedule of vaccination | 2.06 (1.56–2.71) | I2 = 0.0, p = 0.523 | 3 |
Evaluation for publication bias
The presence of heterogeneity among the studies was tested using I-squared statistics. I-squared (I2) statistics for full immunization coverage was (I2 = 99.4%) (p = < 0.0001), which indicates as there is high heterogeneity between studies. A p-value of < 0.0001, indicates the presence of significant heterogeneity among the included studies. The weights of the studies were reported from the random-effect model which ranged from 3.42 to 3.45% (Fig. 1).
We further conducted a subgroup meta-analysis to identify the source of this high heterogeneity using region and publication year. The I2 value for the region subgroup test was found to be 99.5% (p-value < 0.0001) which indicated the presence of heterogeneity between studies (Table 2).
The funnel plot is to be unsymmetrical and the distribution of studies indicates for the presence of heterogeneity. More studies are found on both sides of the funnel plot margin (Fig. 4). Egger’s test was performed, and the test showed there was a significant bias among studies (overall test: intercept = 3.92, 95% CI; 12.32–39.37and p-value = 0.001).
Fig. 4.
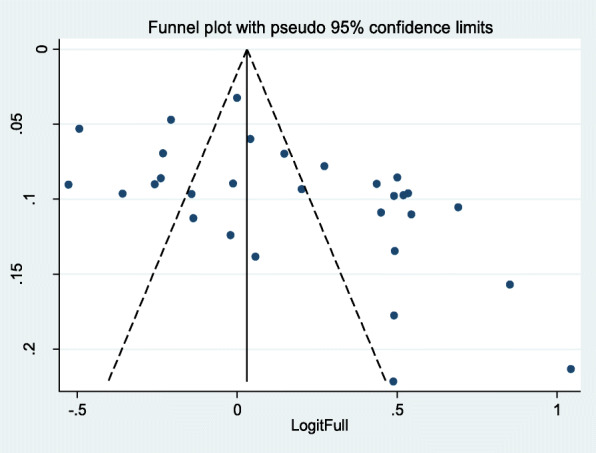
Funnel plot of effect estimates against standard error of log estimate
Sensitivity analysis has been performed to find the influence of each study on the estimates. The plot provides the omitted study on both sides of the margin that indicates there were studies that affect the estimates (Fig. 5).
Fig. 5.

Plot of sensitivity analysis to assessing the influence of individual study
Discussion
Immunization has been one of the most cost-effective health interventions worldwide, through which several serious childhood diseases have been successfully prevented or eliminated. However, vaccination could only become more effective if the child is given a chance to receive the full course of recommended vaccination doses [53].
In this meta-analysis, the proportion of pooled full immunization coverage among children in Ethiopia using the random-effect model was 58.92% (95%CI: 51.26–66.58%). The five consecutive Ethiopia Demographic health survey studies, immunization coverage’s were 14% in 2000, 20% in 2005, 24% in 2011, 39% in 2016 and 43% in 2019 [53, 54]. However, this pooled full immunization coverage indicates less promising to meet the 2020 health sector transformation plan of reaching immunization coverage to 95% in Ethiopia [55].
Understanding the barriers of immunization coverage was critical to formulating effective policies and programs. Lessons from different studies in Ethiopia revealed that fear of immunization side effects, lack of awareness about vaccination, take part negative attitude for the benefit of vaccination, child was sick, unavailability of vaccine, place of immunization too far, due to family health problem, absence of vaccinator, inconvenience vaccination schedule, far distance from health facility, wrong ideas about contraindications and religious, and custom restriction, were major causes for never vaccinated. Therefore, immunization programs should go beyond offering vaccination at health sectors [5] and strengthening collaboration to meet the coverage of all recommended basic vaccines in Ethiopia. Besides, reaching every community strategy (door to door immunization strategy) is an innovative approach that seeks to improve immunization coverage at health facilities [56]. The key goal of the immunization agenda by 2030 is to make vaccination available to everyone and everywhere [57].
This current proportion of pooled full immunization coverage was 58.92% (95%CI: 51.26–66.58%), other systematic review and meta-analysis in Nigeria showed that full immunization coverage was (34.4%) [58], and a national study conducted in Myanmar was (55.4%) [59], national health survey in Malaysia was (86.4%) [60]. In identified studies, forgetting the appointment date, lack of awareness about vaccination, absence of health worker on health facility, place and/or time of vaccination unknown, postponed until another time, fear of immunization side effect, mother too busy, long waiting time, child sick in the time of vaccination, far distance of immunization site, unaware of when to return 2nd or 3rd dose, don’t know next schedule and place, the experience of child sickness with earlier vaccination, disrespectful behavior of health professionals were major causes for incomplete immunization. Thus, the findings highlight that immunization coverage is not an exceptional problem of Ethiopia, it also a problem of other countries that demanding a strong immunization program.
To achieve complete immunization coverage across all regions in Ethiopia, policymakers should design different interventions. For example, the success of immunization services is closely linked to the perceived quality of health services by the public. Health workers engaged in vaccination needed to be skilled in all aspects of vaccine administration, cold chain, and logistics. Regular training and supervision should emphasize these areas [5].
Understanding the determinants of immunization coverage is vital for the improvement of immunization status and identifies area that need to be focused by health care providers and policy-makers. In this meta-analysis, urban residence, maternal education, ANC follows ups, delivery at health facilities, maternal TT vaccination, PNC follows, knowledge about immunization, mother knowing the schedule of vaccination, attitude towards immunization, Mother who visited by HEW were significantly associated with full immunization.
Conclusions
The pooled proportion of immunization coverage in Ethiopia was 58.92% (95%CI: 51.26–66.58%). It was lower compared with 2020 governmental plan of immunization coverage to be 95%, but the proportion of pooled fully immunization coverage was improved from time to time. In this review, there were great disparities in immunization coverage among different regions in Ethiopia.
Implications for practice
Even though improving childhood vaccine coverage is a major priority health agenda in Ethiopia, immunization coverage remains a significant health problem [55]. In this review, the finding indicates that immunization coverage was improved from time to time, but the proportion of full immunization status still lower. In light of these challenges, the country needs to strengthen the implementation of the health extension program, implementation of reaching every district approach, strengthen the health development army in the community, and the government needs to work with the private sector and nongovernmental providers that will improve vaccination coverage in the country. Strategies are needed to make sure that private and public providers implement to reduce barriers and missed opportunities for vaccination [61].
The government needs to build capacity in their communities that emphasize the benefits of full immunization for their children. Individuals and communities should understand the benefits and participate in the decision-making, and delivery process. The community leaders should promote and collaborate closely with local health staff in outreach activities in the communities. However, the growing complexity of immunization programs increases the need for a well-trained, capable health workforce [62]. Children who received other health interventions were more likely to be fully immunized [63]. Therefore, immunization services should integrate with maternal health services in the actual service delivery setups that make it convenient for patients (mothers and their children) to receive vaccinations at primary healthcare settings in Ethiopia.
Lastly, understanding the determinants of immunization coverage is vital for the improvement of immunization status. And also the finding suggests that improved health education and service expansion to remote areas, strength the local specific health service and creating awareness of mothers to complete recommended doses of vaccination are necessary to step immunization access.
Supplementary information
Acknowledgements
We acknowledge the Authors of each article for reviewing their article. We would like to thank JBI for using their systemic review and meta-analysis guidance. We acknowledge also the academician who participated in the reviewing of this meta-analysis.
Abbreviations
- DPT
Diphtheria, Pertussis, and Tetanus
- EDHS
Ethiopia Demographic and Health Survey
- EPI
Expanded Program on Immunization
- HSTP
Health Sector Transformation Plan
- HTA
Health Technology Assessment
- CINAHL
Cumulative Index to Nursing and Allied Health Literature
- AMED
Allied and Complementary Medicine
- WHO
World Health Organization
- MeSH
Medical Subject Heading
- JBI-DSRIR
Joanna Briggs Institute Database of a Systematic Review and Implementation Reports
- PRISMA
Preferred Reporting Items for Systematic Review and Meta-Analysis
Authors’ contributions
AE: Design of the study, data extraction, analyze and interpretation of data and wrote the paper. SS: Data extraction, analyze and interpretation of data and wrote the paper. SH involved at the review of the draft manuscript. All authors read and approved the final manuscript.
Funding
This research did not receive any specific grant from any funding agencies.
Availability of data and materials
The authors confirm that all relevant data was included in the manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Akine Eshete, Email: akine.eshete@yahoo.com.
Sisay Shewasinad, Email: sisyehu@gmail.com.
Solomon Hailemeskel, Email: solomonhailemeskel9@gmail.com.
Supplementary information
Supplementary information accompanies this paper at 10.1186/s12887-020-02163-0.
References
- 1.Asmamaw A, Getachew T, Gelibo T, et al. Determinants of full valid vaccine dose administration among 12-32 months children in Ethiopia: evidence from the Ethiopian 2012 national immunization coverage survey. Ethiop J Health Dev. 2016;30(3):135–141. [Google Scholar]
- 2.Koumaré AK, Traore D, Haidara F, et al. Evaluation of immunization coverage within the expanded program on immunization in Kita circle, Mali: a cross-sectional survey. BMC Int Health Hum Rights. 2009;9(1):S13. doi: 10.1186/1472-698X-9-S1-S13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mwenda JM, Parashar UD, Cohen AL, Tate JE. Impact of rotavirus vaccines in sub-Saharan African countries. Vaccine. 2018;36(47):7119–7123. doi: 10.1016/j.vaccine.2018.06.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Fast SM, González MC, Markuzon N. Cost-effective control of infectious disease outbreaks accounting for a societal reaction. PLoS One. 2015;10(8):e0136059. doi: 10.1371/journal.pone.0136059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Machingaidze S, Wiysonge CS, Hussey GD. Strengthening the expanded program on immunization in Africa: looking beyond 2015. PLoS Med. 2013;10(3):e1001405. doi: 10.1371/journal.pmed.1001405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Johansson KA, Memirie ST, Pecenka C, Jamison DT, Verguet S. Health gains and financial protection from pneumococcal vaccination and pneumonia treatment in Ethiopia: results from extended cost-effectiveness analysis. PLoS One. 2015;10(12):e0142691. doi: 10.1371/journal.pone.0142691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Feldstein LR, Mariat S, Gacic-Dobo M, Diallo MS, Conklin LM, Wallace AS. Global routine vaccination coverage, 2016. MMWR Morb Mortal Wkly Rep. 2017;66(45):1252. doi: 10.15585/mmwr.mm6645a3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bryce J, Terreri N, Victora CG, et al. Countdown to 2015: tracking intervention coverage for child survival. Lancet. 2006;368(9541):1067–1076. doi: 10.1016/S0140-6736(06)69339-2. [DOI] [PubMed] [Google Scholar]
- 9.Negussie A, Kassahun W, Assegid S, Hagan AK. Factors associated with incomplete childhood immunization in Arbegona district, southern Ethiopia: a case-control study. BMC Public Health. 2015;16(1):27. doi: 10.1186/s12889-015-2678-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Berhane Y. Universal childhood immunization: a realistic yet not achieved goal. J Trop Med Hyg. 1993;96:139–145. [PubMed] [Google Scholar]
- 11.Alebachew A, Hatt L, Kukla M. Monitoring and evaluating progress towards universal health coverage in Ethiopia. PLoS Med. 2014;11(9):e1001696. doi: 10.1371/journal.pmed.1001696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Schieber GJ, Gottret P, Fleisher LK, Leive AA. Financing global health: mission unaccomplished. Health Aff. 2007;26(4):921–934. doi: 10.1377/hlthaff.26.4.921. [DOI] [PubMed] [Google Scholar]
- 13.Central Statistical Agency (CSA). Ethiopia Demographic and Health Surve. Ethiopia; 2011.
- 14.Tilahun B, Teklu A, Mancuso A, Abebaw Z, Dessie K, Zegeye D. How can the use of data within the immunization program be increased to improve data quality and ensure greater accountability in the health system? A protocol for implementation science study. Health Res Policy Syst. 2018;16(1):37. doi: 10.1186/s12961-018-0312-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.World Health Organization . Achieving quality universal health coverage through better water, sanitation and hygiene services in health care facilities: a focus on Ethiopia. 2017. [Google Scholar]
- 16.Sabarwal S, Bhatia R, Dhody B, Perumal S, White H, Puri J. Engaging communities for increasing immunization coverage. What do we know? 2015. [Google Scholar]
- 17.World Health Organization . Global vaccine action plan 2011–2020. 2013. [Google Scholar]
- 18.Animaw W, Wondimagegn T, Behailu M, et al. Expanded program of immunization coverage and associated factors among children age 12 – 23 months in Arba Minch town and Zuria District, Southern Ethiopia, 2013. BMC Public Health. 2014;14:464. doi: 10.1186/1471-2458-14-464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Facha W. Vaccination coverage and associated factors among children aged 12 to 23 months in Arba Minch Zuriya Woreda, Southern Ethiopia. J Pharm Alternat Med. 2015;7.
- 20.Meleko A, Mesfin G, Frehiwot B. Assessment of child Immunization coverage and associated factors with full vaccination among children aged 12–23 months at Mizan Aman Town, Bench Maji Zone, Southwest Ethiopia. Int J Pediatr. 2017;2017:7976587. [DOI] [PMC free article] [PubMed]
- 21.Tefera Y, Abram W, Eyoel B. Predictors and barriers to full vaccination among children in Ethiopia. Vaccines. 2018;6:22. 10.3390/vaccines6020022. [DOI] [PMC free article] [PubMed]
- 22.Ayano B. Factors affecting fully Immunization status of children aged 12- 23 months in Hosanna Town, South Ethiopia. Preg Child Health. 2015;2:5. 10.4172/2376-127X.1000185.
- 23.Fite R, Hailu L. Immunization coverage of 12 to 23 months old children in Ethiopia. J Public Health Epidemiol. 2019;11(1):31–37. doi: 10.5897/JPHE2018.1071. [DOI] [Google Scholar]
- 24.Hailu S, Astatkie A, Johansson KA, Lindtjørn B. Low immunization coverage in Wonago district, southern Ethiopia: A community based crosssectional study. PLoS One. 2019;14(7):e0220144. doi: 10.1371/journal.pone.0220144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mesfin M. Incomplete vaccination and associated factors among children aged 12-23 months in Yirgalem Town. South Ethiopia: Addis Ababa University; 2015. [Google Scholar]
- 26.Mohammed H, Atomsa A. Assessment of child immunization coverage and associated factors in Oromia regional state, eastern Ethiopia. Sci Technol Arts Res J. 2013;2(1):36–41. [Google Scholar]
- 27.Legesse E, Dechasa W. An assessment of child immunization coverage and its determinants in Sinana District, Southeast Ethiopia. BMC Pediatr. 2015;15:31. doi: 10.1186/s12887-015-0345-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Melese G, Worku D, Mesfin K. Immunization incompletion among 12 - 23 months old children and associated factors in wayu-Tuka district, Western Ethiopia: a community based study. EC Paediatrics. 2019;8(2):114–27.
- 29.Sheka S, Workina A, Moga TT. Reason for incomplete vaccination and associated factors among children aged 12-23 months in Serbo Town, Jimma Zone, Oromia Region, Southwest Ethiopia. Adv Res J Multidiscip Discov. 2018;32(14):79–84.
- 30.Udessa G, Sena L. Berhanu S. Vaccination status and factors associated with It among children aged 12-23 months in Wadera District, South East Ethiopia Health Care Curr Rev. 2018; 6: 222. 10.4172/2375-4273.1000222.
- 31.Etana B, Deressa W. Factors associated with complete immunization coverage in children aged 12–23 months in Ambo Woreda, Central Ethiopia. BMC Public Health. 2012;12:566. doi: 10.1186/1471-2458-12-566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wado YD, Afework MF, Hindin MJ. Childhood vaccination in rural southwestern Ethiopia: the nexus with demographic factors and women’s autonomy. Pan Afr Med J. 2014;17(Supp 1):9. doi: 10.11694/pamj.supp.2014.17.1.3135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Yasine T, Beyene W. Childhood immunization coverage in Tehulederie district, Northeast of Ethiopia: A community based cross sectional study. Int J Curr Res. 2015;7(9):20234–20240. [Google Scholar]
- 34.Kassahun M, Gashaw A, Alemayehu S. Level of immunization coverage and associated factors among children aged 12–23 months in Lay Armachiho District, North Gondar Zone, and Northwest Ethiopia: a community based cross sectional study. BMC Res Notes. 2015;8:239. doi: 10.1186/s13104-015-1192-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Gualu T, Dilie A. Vaccination coverage and associated factors among children aged 12–23 months in Debre Markos Town, Amhara Regional State, Ethiopia. Adv Public Health. 2017;5352847:6. [Google Scholar]
- 36.Lake MW, Boulanger L, Wasswa P, et al. Factors for low routine immunization performance; a community based cross sectional study in Dessie Town, South Wollo Zone, Ethiopia, 2014. Adv Appl Sci. 2016;1(1):7–17. 10.11648/j.aas.20160101.12.
- 37.Ayal D, Taye B. Assessment of fully vaccination coverage and associated factors among children aged 12-23 months in Mecha District, North West Ethiopia: a cross-sectional study. Sci J Public Health. 2014;2(4):342–8. 10.11648/j.sjph.20140204.26.
- 38.Abebe A, Mesfin W, Alemu B. Coverage, opportunity and challenges of expanded program on immunization among 12-23 months old children in Woldia Town, Northeast, Ethiopia, 2018: Mixed cross sectional study. Biomed Res Int. 2019;2019:5302307. 10.1155/2019/5302307. [DOI] [PMC free article] [PubMed]
- 39.Dagget T, Animaw W, Semachew A. Vaccination coverage and associated factors among children aged 12 – 23 months in Northwest Ethiopia. Hum Vacc Immunother. 2018;10:2348–2354. doi: 10.1080/21645515.2018.1502528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mekonnen A, Alebachew D, Esubalew T. Immunization coverage of 12–23 months old children and its associated factors in Minjar-Shenkora district, Ethiopia: a community-based study. BMC Pediatr. 2019;19:198. doi: 10.1186/s12887-019-1575-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Engida A, Tezera N, Habetie N, Shumet S. Incomplete childhood vaccination and associated factors among children aged 12–23 months in Gondar city administration, Northwest, Ethiopia 2018. BMC Res Notes. 2019;12:241. doi: 10.1186/s13104-019-4276-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Girmay A, Dadi A. Full Immunization Coverage and Associated Factors among Children Aged 12-23 Months in a Hard-to-Reach Areas of Ethiopia. Int J Pediatr. 2019;2019:1924941. doi: 10.1155/2019/1924941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kidane T. Factors influencing TT immunization coverage and protection at birth coverage in Tselemti District, Ethiopia. Ethiop J Health Dev. 2004;18(3):153–158. [Google Scholar]
- 44.Ab M, Amsalu F, Walelegn W, et al. Immunization coverage of 12–23 months old children and associated factors in Jigjiga District, Somali National Regional State, Ethiopia. BMC Public Health. 2014;14:865. doi: 10.1186/1471-2458-14-865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lakew Y, Bekele A, Biadgilign S. Factors influencing full immunization coverage among 12–23 months of age children in Ethiopia: evidence from the national demographic and health survey in 2011. BMC Public Health. 2015;15:728. doi: 10.1186/s12889-015-2078-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sisay K, Mequanent M. Full immunization coverage and its associated factors among children aged 12–23 months in Ethiopia: further analysis from the 2016 Ethiopia demographic and health survey. BMC Public Health. 2019;19:1019. doi: 10.1186/s12889-019-7356-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Asmamaw A, Getachew T, Gelibo T, et al. Determinants of full valid vaccine dose administration among 12-32 months children in Ethiopia: Evidence from the Ethiopian 2012 national immunization coverage survey. Ethiop J Health Dev. 2016;30(3):135–141. [Google Scholar]
- 48.Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. doi: 10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Stein CE, Birmingham M, Kurian M, Duclos P, Strebel P. The global burden of measles in the year 2000—a model that uses country-specific indicators. J Infect Dis. 2003;187(Supplement_1):S8–S14. doi: 10.1086/368114. [DOI] [PubMed] [Google Scholar]
- 50.Cochran WG. The combination of estimates from different experiments. Biometrics. 1954;10(1):101–129. [Google Scholar]
- 51.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 52.Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Central Statistical Agency (CSA) [Ethiopia] and ICF . Ethiopia Demographic and Health Survey 2016. Addis Ababa: CSA ICF; 2016. [Google Scholar]
- 54.Ethiopian Public Health Institute (EPHI) [Ethiopia] and ICF. Ethiopia Mini Demographic and Health Survey 2019: Key Indicators. Rockville: EPHI and ICF. p. 2019.
- 55.Ekström AM, Clark J, Byass P, et al. IN-DEPTH network: contributing to the data revolution. Lancet Diabetes Endocrinol. 2016;4(2):97. doi: 10.1016/S2213-8587(15)00495-7. [DOI] [PubMed] [Google Scholar]
- 56.Shikuku DN, Muganda M, Amunga SO, et al. Door–to–door immunization strategy for improving access and utilization of immunization services in hard-to-reach areas: a case of Migori County, Kenya BMC Public Health 2019;19(1):1–11. [DOI] [PMC free article] [PubMed]
- 57.Hogan DR, Stevens GA, Hosseinpoor AR, Boerma T. Monitoring universal health coverage within the sustainable development goals: development and baseline data for an index of essential health services. Lancet Glob Health. 2018;6(2):e152–e168. doi: 10.1016/S2214-109X(17)30472-2. [DOI] [PubMed] [Google Scholar]
- 58.Adeloye D, Jacobs W, Amuta AO, et al. Coverage and determinants of childhood immunization in Nigeria: a systematic review and meta-analysis. Vaccine. 2017;35(22):2871–2881. doi: 10.1016/j.vaccine.2017.04.034. [DOI] [PubMed] [Google Scholar]
- 59.Nozaki I, Hachiya M, Kitamura T. Factors influencing basic vaccination coverage in Myanmar: secondary analysis of 2015 Myanmar demographic and health survey data. BMC Public Health. 2019;19(1):242. doi: 10.1186/s12889-019-6548-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Lim K, Chan Y, Ani AN, Rohani J, Norfadhilah ZS, Santhi M. Complete immunization coverage and its determinants among children in Malaysia: findings from the National Health and morbidity survey (NHMS) 2016. Public Health. 2017;153:52–57. doi: 10.1016/j.puhe.2017.08.001. [DOI] [PubMed] [Google Scholar]
- 61.Olorunsaiye CZ, Langhamer MS, Wallace AS, Watkins ML. Missed opportunities and barriers for vaccination: a descriptive analysis of private and public health facilities in four African countries. Pan Afr Med J. 2017;27(Suppl 3):6. doi: 10.11604/pamj.supp.2017.27.3.12083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Shen AK, Fields R, McQuestion M. The future of routine immunization in the developing world: challenges and opportunities. Glob Health Sci Pract. 2014;2(4):381–394. doi: 10.9745/GHSP-D-14-00137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Restrepo-Méndez MC, Barros AJ, Wong KL, et al. Missed opportunities in full immunization coverage: findings from low-and lower-middle-income countries. Glob Health Action. 2016;9(1):30963. doi: 10.3402/gha.v9.30963. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The authors confirm that all relevant data was included in the manuscript.