

Self-expandable metallic stent placement is a well-established treatment for malignant colonic obstruction.1, 2, 3 However, colonic stent placement for tumors close to the anal verge is challenging because of the likelihood of severe pain resulting from the close proximity to the dentate line.4 Precise deployment of a stent for tumors close to the anal verge is technically difficult.5
Herein, we describe the use of the newly developed proximal release–type colonic stent for malignant lower rectal obstruction close to the anal verge. This new stent is 22 mm in diameter, 70 mm in length, and mounted on a 16F delivery system. It has flares at both ends to prevent migration. The stent has a closed-cell design and is foreshortened by 30%. It is inserted with the over-the-wire technique (Figs. 1 and 2).
Figure 1.
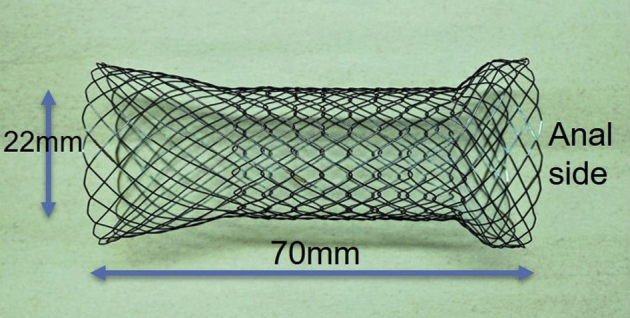
The newly developed proximal release–type colonic stent.
Figure 2.

The proximal release–type stent’s delivery system facilitates positioning of the stent at the anal side.
A 64-year-old man experiencing nausea and vomiting secondary to a malignant lower rectal obstruction caused by gastric cancer metastasis was referred to our center. A conventional colonic stent was technically difficult to deploy because the lesion was located 2 cm from the anal verge. To palliate this obstruction, we used the newly developed stent (Video 1, available online at www.VideoGIE.org).
We first examined the tumor using an ultraslim endoscope (Fig. 3). Gastrografin fluoroscopy revealed the stenosis length to be 4 cm (Fig. 4). The endoscope was then advanced through the stenosis to the oral side of the tumor, and a guidewire was placed across the stricture through the scope. The stent was inserted using the over-the-wire technique and released gently from the anal side while appropriate positioning was maintained under endoscopic view. The distal edge of the stent was kept at the distal tumor edge to facilitate positioning of the stent close to the anal verge. Finally, the stent was successfully deployed to the appropriate position (Fig. 5A and B). No adverse events, including pain, occurred, and oral intake was started 3 days after the procedure. The patient was discharged 8 days postprocedure.
Figure 3.
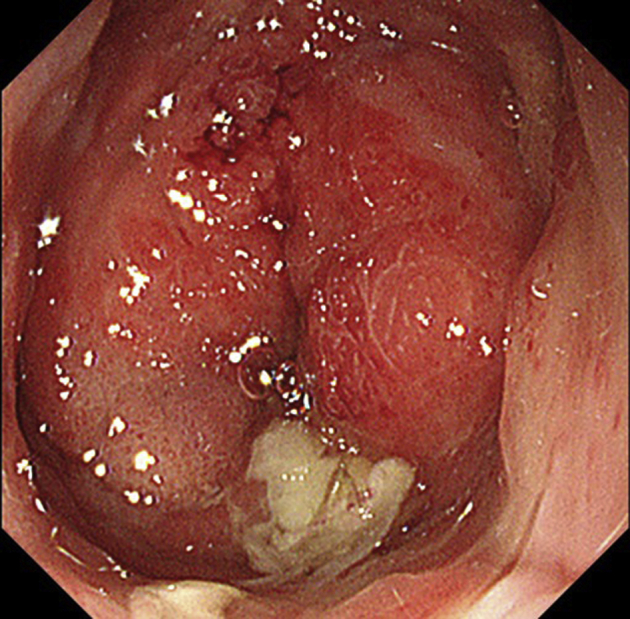
Colonoscopy indicated the tumor to be located 2 cm from the anal verge.
Figure 4.

Gastrografin fluoroscopy revealed the stenosis length to be 4 cm.
Figure 5.

A, B, Stent placement and bowel decompression were successful.
Disclosure
All authors disclosed no financial relationships relevant to this publication.
Supplementary data
The newly developed proximal release–type colonic stent was inserted using the over-the-wire technique and released gently from the anal side while appropriate positioning was maintained under endoscopic view. The distal edge of the stent was kept at the distal tumor edge to facilitate positioning of the stent close to the anal verge.
References
- 1.Saida Y. Current status of colonic stent for obstructive colorectal cancer in Japan; a review of the literature. J Anus Rectum Colon. 2019;3:99–105. doi: 10.23922/jarc.2019-009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Matsuzawa T., Ishida H., Yoshida S. A Japanese prospective multicenter study of self-expandable metal stent placement for malignant colorectal obstruction: short-term safety and efficacy within 7 days of stent procedure in 513 cases. Gastrointest Endosc. 2015;82:697–707.e1. doi: 10.1016/j.gie.2015.03.1978. [DOI] [PubMed] [Google Scholar]
- 3.Kuwai T., Sumida Y., Miura R. Use of a colonic stent to recover a biliary stent retained by malignant colonic obstruction. Endoscopy. 2019;51:E257–E258. doi: 10.1055/a-0891-0601. [DOI] [PubMed] [Google Scholar]
- 4.Song H.Y., Kim J.H., Kim K.R. Malignant rectal obstruction within 5 cm of the anal verge: is there a role for expandable metallic stent placement? Gastrointest Endosc. 2008;68:713–720. doi: 10.1016/j.gie.2007.12.051. [DOI] [PubMed] [Google Scholar]
- 5.van Hooft J.E., van Halsema E.E., Vanbiervliet G. Self-expandable metal stents for obstructing colonic and extracolonic cancer: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2014;46:990–1053. doi: 10.1055/s-0034-1390700. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The newly developed proximal release–type colonic stent was inserted using the over-the-wire technique and released gently from the anal side while appropriate positioning was maintained under endoscopic view. The distal edge of the stent was kept at the distal tumor edge to facilitate positioning of the stent close to the anal verge.