

Abstract
Background
Postoperative pain is a major problem, especially in children, as their tolerance level is lower and several drugs are contraindicated in childhood. This study aimed to compare the effect of dexmedetomidine added to local infiltration of bupivacaine for postoperative pain relief in children undergoing inguinal herniorrhaphy.
Methods
This double-blind, randomized clinical trial included 60 children aged 6–72 months undergoing unilateral herniorrhaphy at selected hospitals in Shiraz, Iran, randomly allocated into two groups, 30 in each group. One group received 1 µg/kg dexmedetomidine plus local infiltration of 0.2 ml/kg bupivacaine 0.5% at the incision site before surgery (BD), and the other group received bupivacaine and normal saline (BO). Analgesic requirements, emergence time, and nausea/vomiting, postoperative pain and sedation scores were assessed for 4 h after the operation. Heart rate (HR), systolic blood pressure (SBP), and oxygen saturation (SaO2) were recorded at baseline, and at 10 and 20 min after injection.
Results
Eighty percent were boy in each group; mean age was 22.75 ± 18.63 months. SaO2 and SBP were not different between the groups, while HR was significantly lower in the Group BD at 10 and 20 min after injection (P < 0.05). Group BD had a lower pain score at 1 and 2 h after the operation, a higher sedation score at the first three time intervals, and longer emergence time than Group BO (all P < 0.001). Group BD had a lower pain score at 1 and 2 h after the operation (P < 0.001, P < 0.047 respectively).
Conclusions
Addition of dexmedetomidine to local infiltration of bupivacaine in children undergoing herniorrhaphy significantly reduced postoperative pain and increased sedation.
Keywords: Bupivacaine; Child; Dexmedetomidine; Herniorrhaphy; Pain, Postoperative; Vital signs
Introduction
Indirect inguinal hernia, caused by a patent processus vaginalis, is a common pathology in the first year of life, especially in low-birth weight male neonates [1]. Surgery (inguinal herniorrhaphy) is considered to be the first-line treatment, in which various techniques, such as open and laparoscopic procedures, have been proposed [2]. Nevertheless, despite the variety of techniques proposed for correction of inguinal hernia, herniorrhaphy is associated with severe adverse effects, such as recurrence, and persistent postoperative pain [3,4].
Among the postoperative adverse effects, pain has significant importance, especially in children, because uncontrolled acute pain may lead to chronic pain that can increase patient stress and negatively affect health-related quality of life. It can also increase the duration of hospital stay and total health costs [5]. Thus, researchers have investigated the efficacy of various analgesics, including bupivacaine, levobupivacaine, clonidine and naloxone, on post-herniorrhaphy pain in children administered at different times through various routes [6,7] such as caudal analgesia, inguinal nerve block, or local infiltration combined with a general anesthetic [8]. However, review studies have reported no significant differences among the various strategies [9].
Dexmedetomidine (DEX) is a highly selective α2-adrenergic agonist with a receptor affinity greater than clonidine, which acts through various mechanisms, such as increased hyperpolarization of action potential, causing hypnotic and analgesic effects [10]. Adding DEX as an adjuvant to bupivacaine has proven effectiveness for postoperative pain relief in various procedures such as cesarean section [11], abdominal hysterectomy [12], and knee arthroplasty [13]. Even a combination of DEX with bupivacaine has been proposed to be superior to bupivacaine alone or with tramadol in cholecystectomy procedures [14]. In children undergoing lower abdominal procedures, adding DEX to caudal bupivacaine increased analgesia without side-effects [15,16]. Recently, researchers reported the extended duration of postoperative pain relief and reduced response to hernial sac traction using 1 µg/kg DEX combined with bupivacaine in children undergoing hernia repair [17,18]. Higher doses of DEX has also been proposed as a feasible anesthetic in pediatric inguinal hernia repair [19]. Furthermore, premedication with sublingual DEX has been established to be more effective than sublingual midazolam in children < 12 years of age undergoing inguinal hernia repair [20].
Local infiltration of drugs into surgical wounds is considered to be an effective measure in reducing postoperative pain, and a safe method because it does not exert the hemodynamic effects of the drug when administered intravenously [21]. A combination of DEX with a local anesthetic, such as bupivacaine or ropivacaine, has been suggested as an appropriate method for postoperative pain relief in adult patients undergoing abdominal hysterectomy [22] and lower segment cesarean section [23]. However, to our knowledge, the effect of combining DEX with bupivacaine has not been described in the pediatric population. Thus, in the present study, we aimed to assess the combined effect of DEX and local infiltration of bupivacaine to improve postoperative pain relief in children undergoing inguinal herniorrhaphy.
Materials and Methods
Study design
This randomized clinical trial involved 60 children undergoing unilateral herniorrhaphy in Nemazee and Ghadir Hospitals, affiliated to Shiraz University of Medical Sciences, Shiraz, Iran. The study protocol was approved by the Research Ethics Committee of Shiraz University of Medical Sciences (Approval number: IR.SUMS.REC.1394.5.945) and was registered in the Iranian Registry of Clinical Trials (IRCT2016060314372N8). Before participant recruitment, the objectives of the study were explained to the parents of the children and written informed consent was obtained. The study adhered to the principles outlined in the Declaration of Helsinki.
Based on the calculated sample size, 60 children 6–72 months of age with unilateral inguinal hernia and American Society of Anesthesiologists (ASA) class I were included in the study. Children with developmental problems, intellectual disabilities, history of seizures, coagulopathies, sensitivity to DEX and bupivacaine, congenital heart disease, history of bleeding disorders, upper respiratory tract infection, liver or kidney failure, and neurological diseases were excluded from the study. A flow diagram illustrating patient recruitment is shown in Fig. 1.
Fig. 1.
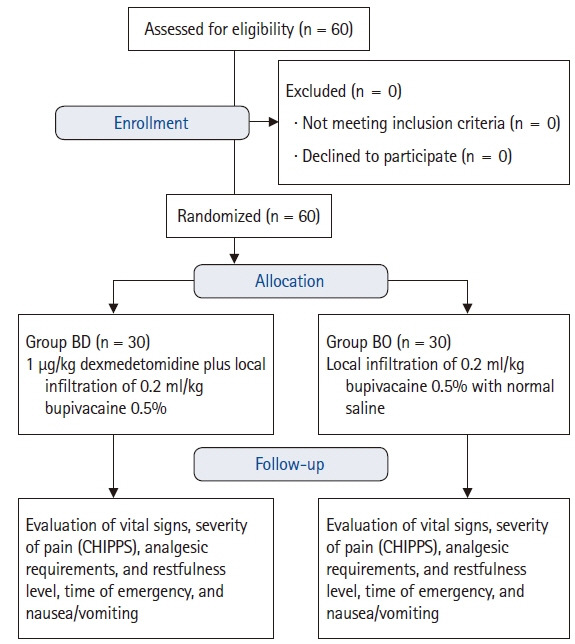
Flow diagram illustrating study enrollment. CHIPPS: Children and Infants Postoperative Pain Scale.
The included patients were randomly divided into two groups based on a computer-generated list: one group received 1 µg/kg DEX (Precedex, Pfizer Inc., USA) plus local infiltration of 0.2 ml/kg bupivacaine 0.5% (Group BD); and the other group received local infiltration of 0.2 ml/kg bupivacaine 0.5% with 1 mL normal saline (Group BO), which were prepared before surgery in similar syringes. The prepared drugs were injected at the surgical site immediately before incision.
The patients were kept in a “nothing by mouth” state the night before surgery but could drink liquids up to 3 h before the procedure. Approximately 20 to 30 min before entering the operating theater, all patients received 0.5 mg/kg oral midazolam for sedation. After entering the operating theater, intravenous (IV) cannulation with a size 22–24 cannula was performed. Then, patients were infused with 6 ml/kg IV fluid (1/3 normal saline, 2/3 dextrose water). Anesthesia was induced by an anesthesiologist using 7 mg/kg sodium thiopental and continued with 2–3% sevoflurane, oxygen, and nitrous oxide through a facial mask. Vital signs, including heart rate (HR), blood pressure (BP), and oxygen saturation (SaO2) were recorded at three time points: baseline, and 10 and 20 min after injecting the study drugs. All procedures were performed by a surgical team using a similar method.
The drugs were prepared before surgery in similar syringes and provided to the surgeon, who was blinded to the group allocation. The drugs used in this study were prepared by an investigator who was not involved in the other parts of the study. The anesthesiologist, surgeon, and nurses were not aware of the content of the syringes. Monitoring during surgery included electrocardiography, pulse oximetry, and non-invasive blood pressure measurement. At the conclusion of the procedure, the patients were transferred to the post-anesthesia care unit, where their vital signs were monitored every 15 min by a nurse.
The sedation level and severity of pain (based on the Children’s and Infant’s Postoperative Pain Scale [CHIPPS]) were assessed by an expert nurse at 1, 2, 3, and 4 h after surgery. In cases for which CHIPPS score was ≥ 3, 15 mg/kg acetaminophen (Apotel, Uni-Pharma Kleon Tsetis Pharmaceutical Laboratories S.A., Greece) was infused and, in cases of nausea/vomiting, 0.15 mg/kg ondansetron was administered. Additionally, analgesic requirements, time of emergence, and nausea/vomiting were recorded for all participants by the same nurse. Sedation score was calculated as follows: 0 = patient is awake and alert; 1 = mild sedation, easy to rouse; 2 = asleep, easy to rouse; 3 = moderate sedation, inability to remain awake; and 4 = difficult to rouse [18]. Emergence time was defined as the time from the conclusion of surgery until eye opening following calling of the child’s name.
The primary endpoint of this study was postoperative analgesia; secondary endpoints included postoperative sedation, hemodynamic change, and emergence time.
Statistical analysis
The minimum sample size required for this study was calculated to be 23 in each group using the sample size estimation formula to compare mean values considering a confidence level of 95%, a power of 80%, standard deviation (SD) of 0.90 and 0.85, and difference of means between the groups at 0.75 (these figures were gathered from the study by Xiang et al. [18]). To address the possibility of drop out, 30 patients were included in each group, resulting in a total of 60 patients. Data are expressed as mean and SD for parametric, and median with range for non-parametric variables. The independent t- test was used to compare normally distributed variables, and the Mann-Whitney U test for pain and sedation score, emergence time, and duration of surgery between the groups. SPSS version 21.0 ((IBM Corp., USA) for Windows (Microsoft Corp., USA) was used for statistical analysis. Differences with P < 0.05 were considered to be statistically significant.
Results
A total of 60 patients were recruited for the study, with 30 patients (24 [80%] boys, 6 [20%] girls) in each group. The mean age of the participants was 22.75 ± 18.63 months (27.97 ± 20.78 months in the Group BD versus 17.53 ± 14.77 months in the Group BO). The age distribution of the participants in the two groups is summarized in Table 1, which shows that the highest frequency was the age category of < 12 months in both groups.
Table 1.
Age Distribution of Participants
| Age (yr) | Group BD | Group BO | P value |
|---|---|---|---|
| < 1 | 11 (33.7) | 18 (60) | 0.060 |
| 1–1.9 | 7 (23.3) | 6 (20) | 0.500 |
| 2–2.9 | 4 (13.3) | 2 (6.7) | 0.333 |
| 3–3.9 | 3 (10) | 3 (10) | 0.665 |
| 4–4.9 | 3 (10) | 1 (3.3) | 0.306 |
| 5–6 | 2 (6.7) | 0 (0) | 0.246 |
| Total | 30 (100) | 30 (100) | 0.100 |
Values are presented as number (%).
Group BD: bupivacaine + dexmedetomidine, Group BO: bupivacaine + normal saline.
Chi-squared test (statistically significant at P < 0.05)
A comparison of vital signs between the groups at the three time points is shown in Table 2. There was no difference between the groups regarding SaO2 and SBP (P > 0.05), while HR was significantly lower in the Group BD at 10 and 20 min after injection (P < 0.004 and < 0.008, respectively). There was a significant time effect on HR (P < 0.001), and group × time interaction (P < 0.008). Additionally, time had a significant effect on SaO2; however, the trend in changes during time was not different between the groups (P = 0.5). Time did not have a significant effect on SBP (P = 0.08), and there was no difference between the groups in trends in changes in SBP during the study (P = 0.3).
Table 2.
Comparison of Heart Rate, Oxygen Saturation, and Systolic Blood Pressure at Three Different Time Points
| Parameter | Group BD | Group BO | P value |
|---|---|---|---|
| Heart rate (beats/min) | |||
| Baseline | 125.2 ± 14.3 | 133.5 ± 16.8 | 0.054 |
| 10 min post-injection | 122.5 ± 15.3 | 135.1 ± 15.9 | 0.004 |
| 20 min post-injection | 118.1 ± 13.1 | 128.3 ± 12.0 | 0.008 |
| Oxygen saturation (SaO2) (%) | |||
| Baseline | 97.1 ± 2.8 | 97.2 ± 2.6 | 0.858 |
| 10 min post-injection | 99.3 ± 0.6 | 99.1 ± 0.9 | 0.388 |
| 20 min post-injection | 99.3 ± 0.6 | 98.8 ± 1.6 | 0.251 |
| Systolic blood pressure (mmHg) | |||
| Baseline | 99.6 ± 12.8 | 94.1 ± 13.4 | 0.120 |
| 10 min post-injection | 94.9 ± 10.0 | 93.5 ± 13.9 | 0.668 |
| 20 min post-injection | 95.9 ± 11.3 | 92.3 ± 12.3 | 0.300 |
Values are presented as mean ± SD.
Results of independent t test.
Group BD: bupivacaine + dexmedetomidine, Group BO: bupivacaine + normal saline.
In the Group BD, the median pain score was significantly lower than in the Group BO at 1 h and 2 h after the operation (P < 0.001); however, there was no significant difference in median pain scores between the groups at 3 h and 4 h after the operation (Table 3). The effect of time was statistically significant in both groups (P < 0.001 and P < 0.003, respectively).
Table 3.
Comparison of Pain and Sedation Scores at Different Postoperative Intervals
| Pain/sedation | Postoperative interval |
P value | |||
|---|---|---|---|---|---|
| 1 h | 2 h | 3 h | 4 h | ||
| Pain score | |||||
| Group BD | 0 (0, 3) | 0 (0, 3) | 0 (0,1) | 0 (0, 0) | <0.001 |
| Group BO | 3 (2, 5) | 1 (0, 2) | 0 (0,1) | 0 (0, 0) | 0.003 |
| P value* | <0.001 | <0.047 | 0.765 | 1.000 | |
| Sedation score† | |||||
| Group BD | 2 (0, 4) | 1 (0, 2) | 0 (0, 1) | 0 (0, 0) | <0.001 |
| Group BO | 0 (0, 1) | 0 (0, 1) | 0 (0, 0) | 0 (0, 2) | 0.801 |
| P value | <0.001 | <0.001 | <0.001 | 0.283 | |
Values are presented as median (range). The pain score was assessed according to the Children and Infants Postoperative Pain Scale (CHIPPS).
Group BD: bupivacaine + dexmedetomidine, Group BO: bupivacaine + normal saline.
P value for Friedman test.
P value for Mann-Whitney U test.
The sedation score was significantly higher in the Group BD at the first three time points (1, 2, and 3 h after surgery) (P < 0.001). The effect of time was statistically significant in the Group BD (P < 0.001), but not in the Group BO (P = 0.8) (Table 3).
Emergence time was significantly longer in the Group BD (20 min [range, 10–25 min]), compared with the Group BO (5 min (range, 3–20]) (P < 0.001); duration of surgery was not different between the two groups (P = 1.0). No episode of nausea or vomiting was recorded.
Discussion
The results of the present study showed no statistically significant differences in SaO2 and SBP between the two groups. HR in the Group BD was significantly lower compared with the Group BO at 10 and 20 min after infiltration of the drugs; however, there was no statistically significant change in HR in each group. Several studies have demonstrated the greater analgesic effect of DEX plus bupivacaine in caudal analgesia compared with bupivacaine alone in children undergoing lower abdominal procedures under sevoflurane anesthesia, without significant side effects, and have proposed similar adjuvant efficacy for DEX and clonidine [15,16]. These results are consistent with those of the present study, indicating the high analgesic and sedative effect of DEX when added to other anesthetics, although the type of anesthetic and administration method was different. In accordance with our study, Saadawy et al. [17] also confirmed significantly longer sedative and analgesic effects in the Group BD than Group BO in 60 children 1–6 years of age with ASA class I undergoing inguinal hernia repair. They concluded similar pain scores in the first 4 h between the BD and BO groups, which is inconsistent with our results, given that we observed lower pain scores in the Group BD 1 h and 2 h after surgery. This difference could be attributed to the different pain scale (objective pain scale) used in their study [17]. Xiang et al. [18] demonstrated that supplementation of 1 µg/kg DEX to caudal bupivacaine could extend the duration of postoperative pain relief and reduce the need for rescue analgesia. This is consistent with the results obtained in the present study, at 1 h postoperatively, 22 patients in the Group BD (73.3%) had a CHIPPS score of 0, while 24 (80%) in the Group BO had a CHIPPS score of 3 (P < 0.001). At 2 h postoperatively, 21 (70%) patients in the Group BD and 11 (36.6%) in the Group BO had CHIPPS scores of 0 (P < 0.006). However, they demonstrated no statistical difference in CHIPPS pain scores between the two groups until 4 h [18]. In their study, during the first 4 h, analgesia was adequate in all subjects of both groups. As the results of the study by Xiang et al. [18] demonstrated, adding DEX to caudal bupivacaine prolonged the duration of postoperative analgesia.
The results of our study investigating the analgesic effect of DEX administered as surgical site infiltration as an adjunct to bupivacaine are consistent with those of previous studies investigating adding DEX to other local anesthetics. Several studies have investigated the effect of adding DEX to ropivacaine, administered as an incisional infiltration, in different procedures, such as inguinal hernia [24], laparoscopic cholecystectomy [25], and lower segment cesarean section [23]. The results of these studies demonstrated significantly lower visual analogue scale (VAS) scores until 24 h after surgery in the DEX + ropivacaine group compared with ropivacaine alone, while nausea/vomiting or other complications were not different between the groups. Although the general results of these studies confirm the efficacy of adding DEX to local anesthetic, there were several differences between them and our study. First, the type of local anesthetic used was different (ropivacaine versus bupivacaine). Second, the study populations were different because they investigated adult populations, while we evaluated pediatric patients. In addition, in the current study, we used CHIPPS for assessment of postoperative pain, similar to the study by Xiang et al. [18], while other studies alternatively used other scales, such as the Face, Legs, Activity, Cry, Consolability Pain Scale [15], the OPS [17], and VAS [23–25]. Nevertheless, they all reported similar conclusions regarding the efficacy of adding DEX to bupivacaine and other local anesthetics in adults and children. Other studies have also indicated the efficacy of incisional infiltration of DEX on postoperative pain relief, supplemented with other anesthetics, such as levobupivacaine [26], lignocaine with adrenaline [27], suggesting that co-infiltration of local anesthetics can prolong their anesthetic and analgesic effect by peripheral action [28].
Another important finding of our study was significant higher sedation scores in the Group BD at the first three time points (i.e., 1, 2, and 3 h after surgery) as well as longer emergence time in this group, which indicate deeper sedation in Group BD, which is similar to the results reported by Xiang et al. [18] and others. In the study by Abdelnaim et al. [29], the researchers reported significantly higher Ramsay sedation scores in the Group BD compared with BO and DEX + magnesium groups, which confirms the results of our study. It has been previously indicated that IV administration and infiltration of DEX results in greater sedation compared with normal saline [30]. The sedative effects of DEX are mainly the result of the stimulation of α2-adrenoreceptors in the locus coeruleus [18]. Evaluation of the postoperative sedation scale in our study reveals more satisfactory sedation in the Group BD compared with the Group BO in the first three hours.
Strengths of the present study include the assessment of adjuvant efficacy of local infiltration of DEX in children undergoing inguinal hernia repair in a double-blind RCT. Nevertheless, the present study had some limitations, the first of which was the age difference between the two groups, despite the random allocation of participants and sufficient sample size, which may have affected the results of the study. Additionally, we evaluated patients for only 4 h after surgery; as such, longer follow-up periods may provide a wider spectrum for the best drug choice for researchers and physicians.
Local infiltration of DEX as supplementation to bupivacaine can significantly reduce postoperative pain in children undergoing herniorrhaphy, especially in the first postoperative hour, and can induce higher sedation after surgery without significant side effects on the hemodynamic status of pediatric patients. Thus, it is suggested that local infiltration of DEX be used as adjuvant therapy with bupivacaine after pediatric herniorrhaphy. Future studies with longer follow-up periods and larger populations may reveal the best anesthetic for children undergoing inguinal hernia repair.
Footnotes
Funding Statement
This study was financially supported by Shiraz University of Medical Sciences (Grants No. 8189).
Conflicts of Interest
No potential conflict of interest relevant to this article was reported.
Author Contributions
Simin Azemati (Conceptualization; Formal analysis; Funding acquisition; Writing – review & editing)
Anahita Pourali (Data curation; Formal analysis; Investigation; Writing – original draft; Writing – review & editing)
Sedigheh Aghazadeh (Data curation; Writing – review & editing)
References
- 1.Cusick RA. Pediatric inguinal hernias, hydroceles, and undescended testicles. Surg Clin North Am. 2012;92:487–504. doi: 10.1016/j.suc.2012.03.017. [DOI] [PubMed] [Google Scholar]
- 2.Bharathi RS, Arora M, Baskaran V. Pediatric inguinal hernia: laparoscopic versus open surgery. JSLS. 2008;12:277–81. [PMC free article] [PubMed] [Google Scholar]
- 3.Koning G, Wetterslev J, Van Laarhoven C, Keus F. The totally extraperitoneal method versus Lichtenstein's technique for inguinal hernia repair: a systematic review with meta-analyses and trial sequential analyses of randomized clinical trials. PloS one. 2013;8:e52599. doi: 10.1371/journal.pone.0052599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lange JF, Meyer VM, Voropai DA, Keus E, Wijsmuller AR, Ploeg RJ, et al. The role of surgical expertise with regard to chronic postoperative inguinal pain (CPIP) after Lichtenstein correction of inguinal hernia: a systematic review. Hernia. 2016;20:349–56. doi: 10.1007/s10029-016-1483-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287–98. doi: 10.2147/JPR.S144066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.She YJ, Xie GT, Tan YH, Kuang XH, Yu GF, Lian GH, et al. A prospective study comparing the onset and analgesic efficacy of different concentrations of levobupivacaine with/without dexmedetomidine in young children undergoing caudal blockade. J Clin Anesth. 2015;27:17–22. doi: 10.1016/j.jclinane.2014.09.005. [DOI] [PubMed] [Google Scholar]
- 7.Seyedhejazi M, Sheikhzadeh D, Adrang Z, Rashed FK. Comparing the analgesic effect of caudal and ilioinguinal iliohypogastric nerve blockade using bupivacaine-clonidine in inguinal surgeries in children 2-7 years old. Afr J Paediatr Surg. 2014;11:166–9. doi: 10.4103/0189-6725.132821. [DOI] [PubMed] [Google Scholar]
- 8.Shanthanna H, Singh B, Guyatt G. A systematic review and meta-analysis of caudal block as compared to noncaudal regional techniques for inguinal surgeries in children. Biomed Res Int. 2014;2014:890626. doi: 10.1155/2014/890626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Baird R, Guilbault M-P, Tessier R, Ansermino JM. A systematic review and meta-analysis of caudal blockade versus alternative analgesic strategies for pediatric inguinal hernia repair. J Pediatr Surg. 2013;48:1077–85. doi: 10.1016/j.jpedsurg.2013.02.030. [DOI] [PubMed] [Google Scholar]
- 10.Brummett CM, Hong EK, Janda AM, Amodeo FS, Lydic R. Perineural dexmedetomidine added to ropivacaine for sciatic nerve block in rats prolongs the duration of analgesia by blocking the hyperpolarization-activated cation current. Anesthesiology. 2011;115:836–43. doi: 10.1097/ALN.0b013e318221fcc9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Li Z, Tian M, Zhang CY, Li AZ, Huang AJ, Shi CX, et al. A randomised controlled trial to evaluate the effectiveness of intrathecal bupivacaine combined with different adjuvants (fentanyl, clonidine and dexmedetomidine) in caesarean section. Drug Res (Stuttg) 2015;65:581–6. doi: 10.1055/s-0034-1395614. [DOI] [PubMed] [Google Scholar]
- 12.Almarakbi WA, Kaki AM. Addition of dexmedetomidine to bupivacaine in transversus abdominis plane block potentiates post-operative pain relief among abdominal hysterectomy patients: a prospective randomized controlled trial. Saudi J Anaesth. 2014;8:161–6. doi: 10.4103/1658-354X.130683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sharma B, Rupal S, Swami AC, Lata S. Effect of addition of dexmedetomidine to ropivacaine 0.2% for femoral nerve block in patients undergoing unilateral total knee replacement: a randomised double-blind study. Indian J Anaesth. 2016;60:403–8. doi: 10.4103/0019-5049.183392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Shukla U, Prabhakar T, Malhotra K, Srivastava D, Malhotra K. Intraperitoneal bupivacaine alone or with dexmedetomidine or tramadol for post-operative analgesia following laparoscopic cholecystectomy: a comparative evaluation. Indian J Anaesth. 2015;59:234–9. doi: 10.4103/0019-5049.155001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.El-Hennawy A, Abd-Elwahab A, Abd-Elmaksoud A, El-Ozairy H, Boulis S. Addition of clonidine or dexmedetomidine to bupivacaine prolongs caudal analgesia in children. Br J Anaesth. 2009;103:268–74. doi: 10.1093/bja/aep159. [DOI] [PubMed] [Google Scholar]
- 16.Al-Zaben KR, Qudaisat IY, Abu-Halaweh SA, Al-Ghanem SM, Al-Mustafa MM, Alja'bari AN, et al. Comparison of caudal bupivacaine alone with bupivacaine plus two doses of dexmedetomidine for postoperative analgesia in pediatric patients undergoing infra-umbilical surgery: a randomized controlled double-blinded study. Paediatr Anaesth. 2015;25:883–90. doi: 10.1111/pan.12686. [DOI] [PubMed] [Google Scholar]
- 17.Saadawy I, Boker A, Elshahawy MA, Almazrooa A, Melibary S, Abdellatif AA, et al. Effect of dexmedetomidine on the characteristics of bupivacaine in a caudal block in pediatrics. Acta Anaesthesiol Scand. 2009;53:251–6. doi: 10.1111/j.1399-6576.2008.01818.x. [DOI] [PubMed] [Google Scholar]
- 18.Xiang Q, Huang DY, Zhao YL, Wang GH, Liu YX, Zhong L, et al. Caudal dexmedetomidine combined with bupivacaine inhibit the response to hernial sac traction in children undergoing inguinal hernia repair. Br J Anaesth. 2013;110:420–4. doi: 10.1093/bja/aes385. [DOI] [PubMed] [Google Scholar]
- 19.Bong CL, Yeo AS, Fabila T, Tan JS. A pilot study of dexmedetomidine sedation and caudal anesthesia for inguinal hernia repair in infants. Paediatr Anaesth. 2016;26:621–7. doi: 10.1111/pan.12907. [DOI] [PubMed] [Google Scholar]
- 20.Pant D, Sethi N, Sood J. Comparison of sublingual midazolam and dexmedetomidine for premedication in children. Minerva Anestesiol. 2014;80:167–75. [PubMed] [Google Scholar]
- 21.Gupta A. Wound infiltration with local anaesthetics in ambulatory surgery. Curr Opin Anaesthesiol. 2010;23:708–13. doi: 10.1097/ACO.0b013e32833f0dd7. [DOI] [PubMed] [Google Scholar]
- 22.Singh S, Prasad C. Post-operative analgesic effect of dexmedetomidine administration in wound infiltration for abdominal hysterectomy: a randomised control study. Indian J Anaesth. 2017;61:494–8. doi: 10.4103/ija.IJA_676_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bhardwaj S, Devgan S, Sood D, Katyal S. Comparison of local wound infiltration with ropivacaine alone or ropivacaine plus dexmedetomidine for postoperative pain relief after lower segment cesarean section. Anesth Essays Res. 2017;11:940–5. doi: 10.4103/aer.AER_14_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kang H. The effect of dexmedetomidine added to preemptive ropivacaine infiltration on post-operative pain after inguinal herniorrhaphy: a prospective, randomized, double-blind, placebo-controlled study. Eur Surg. 2012;44:274–80. [Google Scholar]
- 25.Yu JM, Sun H, Wu C, Dong CS, Lu Y, Zhang Y. The analgesic effect of ropivacaine combined with dexmedetomidine for incision infiltration after laparoscopic cholecystectomy. Surg Laparosc Endosc Percutan Tech. 2016;26:449–54. doi: 10.1097/SLE.0000000000000325. [DOI] [PubMed] [Google Scholar]
- 26.Jyothi B, Govindaraj K, Shaikh S. Comparison of analgesic efficacy of levobupivacaine, levobupivacaine and clonidine, and levobupivacaine and dexmedetomidine in wound infiltration technique for abdominal surgeries: a prospective randomized controlled study. Indian J Pain. 2017;31:127–32. [Google Scholar]
- 27.Mandal D, Das A, Chhaule S, Halder PS, Paul J, RoyBasunia S, et al. The effect of dexmedetomidine added to preemptive (2% lignocaine with adrenaline) infiltration on intraoperative hemodynamics and postoperative pain after ambulatory maxillofacial surgeries under general anesthesia. Anesth Essays Res. 2016;10:324–31. doi: 10.4103/0259-1162.167837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pratap JN, Shankar RK, Goroszeniuk T. Co-injection of clonidine prolongs the anesthetic effect of lidocaine skin infiltration by a peripheral action. Anesth Analg. 2007;104:982–3. doi: 10.1213/01.ane.0000257949.46444.a8. [DOI] [PubMed] [Google Scholar]
- 29.Abdelnaim HE, Mohamed NN, Saleh AH, Youssef AN. Comparison between bupivacaine-dexmedetomidine mixture and bupivacaine-magnesium mixture when used for wound infiltration before skin incision in surgeries for hernia repair regarding their intraoperative and postoperative analgesic effects. Ain-Shams J Anesthesiol. 2018;10:10. [Google Scholar]
- 30.Cheung CW, Ng KF, Choi WS, Chiu WK, Ying CL, Irwin MG. Evaluation of the analgesic efficacy of local dexmedetomidine application. Clin J Pain. 2011;27:377–82. doi: 10.1097/AJP.0b013e318208c8c5. [DOI] [PubMed] [Google Scholar]