

Abstract
The coronavirus outbreak was labeled a pandemic by the World Health Organization in 2020. Patients who require spine surgery should receive coronavirus disease 2019 (COVID-19) screening to prevent nosocomial cross-infection before surgery. However, spine fracture and spinal injury are critical and serious, and there are no standard protocols for management. This article aims to propose a treatment algorithm for the management of traumatic spine fracture during the COVID-19 pandemic.
Keywords: COVID-19, Traumatic spine fracture, Practice guideline, COVID-19 situation
Introduction
In Wuhan, China, a series of unexplained pneumonia cases was reported. This was identified as a new coronavirus in December 2019. With cases being exported to other countries, the World Health Organization (WHO) Director- General determined this “a public health emergency of international concern” on 30 January, 2020. The disease has been named coronavirus disease 2019 (COVID-19) [1]. Reverse transcription-polymerase chain reaction (PT-PCR) testing for the causative severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) includes methods that detect the presence of the virus and those that detect antibodies produced in response to infection. However, an earlier review shows a false-negative of RT-PCR and prolonged nucleic acid conversion in COVID-19 [2].
During the COVID-19 pandemic, it has been determined that all patients undergoing elective spine surgery should first receive COVID-19 screening to prevent nosocomial cross-infection. However, patients in emergency departments are more critical and serious, presenting with conditions including open fractures, multiple long bone fractures, and spinal fracture that require intermediate or emergency surgical intervention [3]. In this article, the authors describe their clinical practice guidelines for the management of COVID-19 in trauma patients with spine fractures.
The Nakornping Hospital Institutional Review Board provided approval to publish these details.
Management Principles
Surgical intervention or operative treatments may be required for patients with spinal displacement or compression, spinal cord injury, and progressive aggravation of weakness. Such patients may be routinely admitted to the hospital after the possibility of COVID-19 infection is excluded. However, orthopedic trauma patients with an indication for urgency and emergency operative procedures cannot be excluded from COVID-19 infection, since history may be unknown due to unconsciousness or patients who are borderline, unstable, or in a coma (extremis patient). These patients almost always need intubation or ventilator. The patients should be accompanied to a designated isolation room or area for the initial assessment. The surgeon must use full personal protective equipment (PPE) [4] and infection control measures for damage control orthopedics. The team should discuss with local designated COVID-19 teams the best place for care such as a separate ward or separate intensive care unit. Operative treatment with full PPE and infection control measures is very important when a patient is detected to have COVID- 19 by PCR testing.
In patients who are stable and fully conscious, we prefer to use screening criteria, including patient exposure to COVID-19, or symptoms of cough, fever ≥37.5° in WHO Phase 2 and ≥37.3° in WHO Phase 3, or risk of contact with COVID-19 in a pandemic area. If these symptoms or signs are present, the patient should wear a surgical face mask and be taken to a designated isolation room or area for an initial assessment. The team must use full PPE and infection control measures to be able to perform emergency operative procedures without waiting for the results of rapid tests or PCR for COVID-19 [5], and patients in this group can be tested using PCR after surgery. Patients without symptoms and at low risk of exposure to COVID-19 can be given a surgical face mask to prevent hospital-acquired infections. The operating room and treatment should be planned to allow standard infection control measures. During standard post-operative care, the patient should wear a surgical face mask.
The authors designed an algorithm to assess patients, presented in Fig.1. This is in contrast to the previous review, “Advice on standardized diagnosis and treatment for spinal diseases during the coronavirus disease 2019 pandemic,” which suggested that chest computed tomography and SARS-CoV-2 nucleic acid test should be performed three days before surgery [3,6]. Patients with confirmed COVID-19 should be transferred to the isolation ward for further treatment.
Fig. 1.
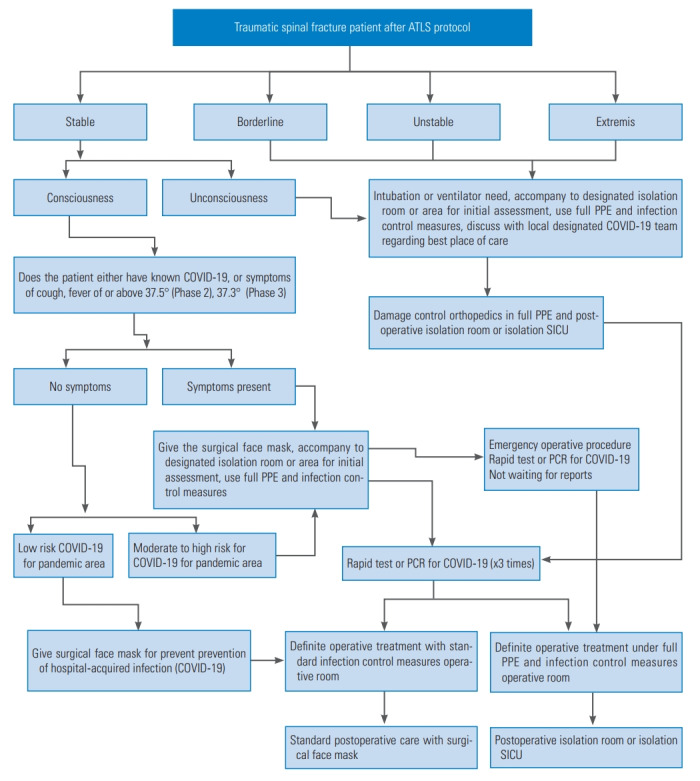
The authors preferred algorithm to assess COVID-19 risk in patients with a traumatic spine fracture. ATLS, Advanced Trauma Life Support; PPE, personal protective equipment; COVID-19, coronavirus disease 2019; SICU, surgical intensive care unit; PCR, polymerase chain reaction.
Conclusions
The authors conclude that this algorithm can help make decisions about surgical intervention for spine injury in patients at risk of COVID-19. This algorithm is an improvement to prevent surgeons and nurses from an infection of COVID-19. In the future, this algorithm should be revised according to updated knowledge of prevention, novel treatment, and laboratory testing technology for COVID-19.
Acknowledgments
Thank you to the Institutional Ethics Review Board at Nakornping Hospital.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.He F, Deng Y, Li W. Coronavirus disease 2019: what we know? J Med Virol. 2020 Mar 14; doi: 10.1002/jmv.25766. [Epub]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Xiao AT, Tong YX, Zhang S. False-negative of RTPCR and prolonged nucleic acid conversion in COVID- 19: rather than recurrence. J Med Virol. 2020 Apr 9; doi: 10.1002/jmv.25855. [Epub]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zou J, Yu H, Song D, Niu J, Yang H. Advice on standardized diagnosis and treatment for spinal diseases during the coronavirus disease 2019 Pandemic. Asian Spine J. 2020;14:258–63. doi: 10.31616/asj.2020.0122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rossi SL, Bortolosso H, Silva R, de Mello JM, Costella MF. Evaluation of the efficacy of personal protective equipment against occupational exposure to cold. Rev Bras Med Trab. 2020;17:136–44. doi: 10.5327/Z1679443520190326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wynants L, van Calster B, Bonten MM, et al. Prediction models for diagnosis and prognosis of covid-19 infection: systematic review and critical appraisal. BMJ. 2020;369:m1328. doi: 10.1136/bmj.m1328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tang YW, Schmitz JE, Persing DH, Stratton CW. The laboratory diagnosis of COVID-19 infection: current issues and challenges. J Clin Microbiol. 2020:JCM.00512-20. doi: 10.1128/JCM.00512-20. [DOI] [PMC free article] [PubMed] [Google Scholar]